
Abstract
Introduction
Locally advanced rectal cancer (LARC) remains a therapeutic challenge, with significant risks of both locoregional and distant relapse. Total neoadjuvant therapy (TNT), which combines induction chemotherapy and chemoradiotherapy (CRT) prior to surgery, has emerged as a potentially more effective strategy than traditional approaches, yet data from low- and middle-income countries (LMICs) remain limited. This study evaluates the efficacy and toxicity of induction FOLFIRINOX followed by concurrent CRT in Vietnamese patients with lower–middle LARC.
Methods
A retrospective analysis was conducted on adult patients (n = 72) with clinical stage T3–T4 M0 rectal adenocarcinoma. All patients received induction FOLFIRINOX for six cycles and preoperative CRT, followed by total meso-rectal excision (TME), and adjuvant chemotherapy as indicated. The primary endpoint was pathologic complete response (pCR, ypT0N0); secondary endpoints were 3-year disease-free survival (DFS) and safety. The study conforms to STROBE guidelines.
Results
Pathological complete response was achieved in 25.0% of patients. The 3-year DFS reached 90.6%. Treatment feasibility was high, with 93.06% completing all 6 induction cycles; hematologic adverse events, particularly leukopenia and neutropenia, were the most common toxicities but were generally manageable with supportive care, while nonhematological toxicities were predominantly mild. R0 resection rate was 100% and sphincter-preserving surgery was 86.1%.
Conclusion
In a LMIC setting, induction FOLFIRINOX followed by CRT shows promising efficacy and tolerable toxicity in LARC. These findings support early, intensified systemic therapy to enhance local control and mitigate metastatic spread.
Introduction
Background
Rectal cancer remains a significant global health concern, ranking among the leading causes of cancer-related morbidity and mortality worldwide. 1 In Vietnam, both registry and screening data indicate a rising rectal-cancer burden. In Ho Chi Minh City (1996-2015), the age-standardized CRC incidence increased from 10.5 to 17.9 per 100,000, with rectal cancer showing the fastest rise (AAPC 3.3%, 95% CI 1.0-5.7). 2 In Hanoi's first population-based program, FIT positivity was 6.1%, and among those scoped 3.5% had cancer and 17.8% had advanced adenomas. 3 Traditional management of locally advanced rectal cancer (LARC) has historically involved a combination of neoadjuvant chemoradiotherapy (CRT) followed by total meso-rectal excision (TME) and, when indicated, adjuvant chemotherapy. While this multimodal regimen has yielded improvements in local control and overall survival, a significant subset of patients still experience recurrence—particularly in the form of distant metastases. 4 Consequently, the sequencing and integration of chemotherapy and radiotherapy continue to evolve in pursuit of more robust systemic control, greater tumor downstaging, and reduced long-term toxicity.5–7
Rationale and Knowledge Gap
In recent years, total neoadjuvant therapy (TNT) has emerged as an innovative treatment paradigm for LARC. TNT typically involves administering systemic chemotherapy and chemoradiotherapy before surgical resection, thereby intensifying early systemic control of potential micro-metastases and increasing the likelihood of achieving pathological complete response (pCR). 8 One of the regimens at the forefront of this approach is FOLFIRINOX, a combination of leucovorin, fluorouracil, irinotecan, and oxaliplatin. Initially established in the treatment of advanced pancreatic cancer, FOLFIRINOX has demonstrated promising efficacy in rectal cancer, offering robust tumor shrinkage and favorable pathological responses when delivered as an induction regimen prior to CRT. 9
Concurrently, CRT continues to play an essential role in optimizing local tumor control by enhancing radiosensitivity and reducing tumor volume, which can potentially allow for sphincter-saving surgery in low rectal tumors.7,10 When employed as part of a TNT approach, concurrent CRT not only promotes maximal locoregional control but may also synergize with upfront systemic therapy to improve distant control. Early clinical trials have reported that TNT with an induction FOLFIRINOX regimen followed by concurrent CRT can facilitate higher rates of pCR and may ultimately translate into improved disease-free survival.8,9
Although TNT is increasingly adopted for LARC worldwide, implementation data from low- and middle-income countries (LMICs) remain limited. In Vietnam, to the best of our knowledge, there has been no study evaluating the efficacy and safety of an induction FOLFIRINOX-based total neoadjuvant therapy (TNT) strategy followed by concurrent chemoradiotherapy in patients with locally advanced rectal cancer.
Objective
Building on these promising findings, further investigation is needed to clarify the optimal sequencing of systemic therapy, radiotherapy, and surgery. The present study aims to evaluate the efficacy and safety of an induction FOLFIRINOX-based TNT strategy, followed by concurrent chemoradiotherapy, in Vietnamese patients with locally advanced rectal cancer to determine its impact on treatment outcomes and toxicity profile.
Methods
Patient Selection
This retrospective study was performed in hospitals in Vietnam from 2019 to 2025. Eligible patients were adults aged 18–75 years and had newly diagnosed, biopsy-proven, lower-middle rectal adenocarcinoma (Distal edge of tumour ≤ 10 cm from the anal verge) staged cT3 or cT4 M0, with a WHO performance status of 0–1 and no contraindications to chemotherapy, chemoradiation, and surgery. 11 Written informed consent was obtained from all participants before initiating treatment, and the study was approved by the Institutional Ethical Review Board of Hanoi Medical University (Approval No. 908/GCNHDDDNCYSH-DHYHN on 04/05/2023). All patient data were de-identified prior to analysis and no identifiable images or personal information are included. The reporting of this cohort conforms to the STROBE guidelines for observational studies. 12 We tried to minimize bias by enrolling consecutive eligible patients. The cohort represents a convenience sample of patients treated during the study window at participating hospitals. Finally, the study included 72 patients.
Clinical Data Collection
This study gathered baseline demographic and disease-related data from patients. The demographic data included gender, age. The disease-related data consisted of Eastern Cooperative Oncology Group performance status (ECOG PS) score, tumor location, tumor differentiation, T and N classification, meso-rectal fascia (MRF) status, and extramural vascular invasion (EMVI) status. Baseline comorbidities—including hypertension, diabetes mellitus, and coronary artery disease—were also recorded.
Treatment Procedure
Patients received induction chemotherapy with FOLFIRINOX (oxaliplatin 85 mg/m2, irinotecan 180 mg/m2, leucovorin 400 mg/m2, and fluorouracil 2400 mg/m2 intravenously every 14 days for 6 cycles), chemoradiation (50.4 Gy and 825 mg/m2 concurrent oral capecitabine twice daily for irradiation days), total meso-rectal excision, and adjuvant chemotherapy (3 months of modified FOLFOX6 [intravenous oxaliplatin 85 mg/m2 and leucovorin 400 mg/m2, followed by intravenous 400 mg/m2 fluorouracil bolus and then continuous infusion at a dose of 2400 mg/m2 over 46 h every 14 days for six cycles] or capecitabine [1250 mg/m2 orally twice daily on days 1-14 every 21 days]). Additional medications, such as granulocyte colony-stimulating factors (G-CSF), were administered if clinically indicated. Toxicities were graded using the National Cancer Institute's Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Chemoradiation will start within 2 to 4 weeks following the end of the last cycle of FOLFIRINOX. Radiation was delivered at 1.8 Gy per day, five days per week, in which, total pelvic irradiation dose of 45 Gy/25 fractions and 5.4 Gy/3 fractions boost to the tumor, using IMRT or 3D-CRT techniques, 6–15MV photons. Oral capecitabine 825 mg/m2 was administered twice daily on radiotherapy days, weekend off.
Fellow researchers may reproduce our methodology from the description.
Evaluation of Tumor Response
All patients were staged at baseline with pelvic MRI, CT chest/abdomen, digital rectal examination (DRE) and endoscopic evaluation. Repeat MRIs were performed before the start of CRT and again 4–6 weeks after its completion. Decisions on treatment sequencing were made in a multidisciplinary team (MDT) meeting. Surgery was scheduled 6–8 weeks after CRT.
Clinical and pathological responses after TNT were evaluated using RECIST 1.1 and Mandard tumor regression grade system (TRG), respectively. Complete response (CR) and partial response (PR) assessed by MRI were regarded as clinical response. For histopathology regression assessment, response was defined as Mandard TRG 1, 2, 3, in which, pCR is equivalent to Mandard TRG 1; and non-response as Mandard TRG 4, 5.
Circumferential resection margin (CRM) was recorded in millimeters; CRM positivity was defined as ≤1 mm. Pathology assessments were performed by institutional departments; central review was not performed.
Follow-up
All patients were contacted via telephone, and the final follow-up was on March 15th, 2025. Disease-free survival (DFS) was defined as the time from treatment initiation to documented occurrence of the first oncological event observed, such as local or metastatic recurrence, or death, irrespective of cause. Surveillance included chest x-ray, abdominal ultrasound, or CT chest/abdomen-pelvis every 3 months for 2 years then every 6 months, and colonoscopy annually.
Statistical Analyses
The primary endpoint of this study was pathologic complete response (pCR, ypT0N0); secondary endpoints were 3-year disease-free survival (DFS) and safety. The study conforms to STROBE guidelines.
Descriptive statistics summarized patient demographics, baseline tumor characteristics, treatment details, and observed toxicities. DFS were estimated using the Kaplan-Meier method. Statistical analyses were conducted using RStudio version 2023.03.0 + 386.
Results
Patient's Characteristics
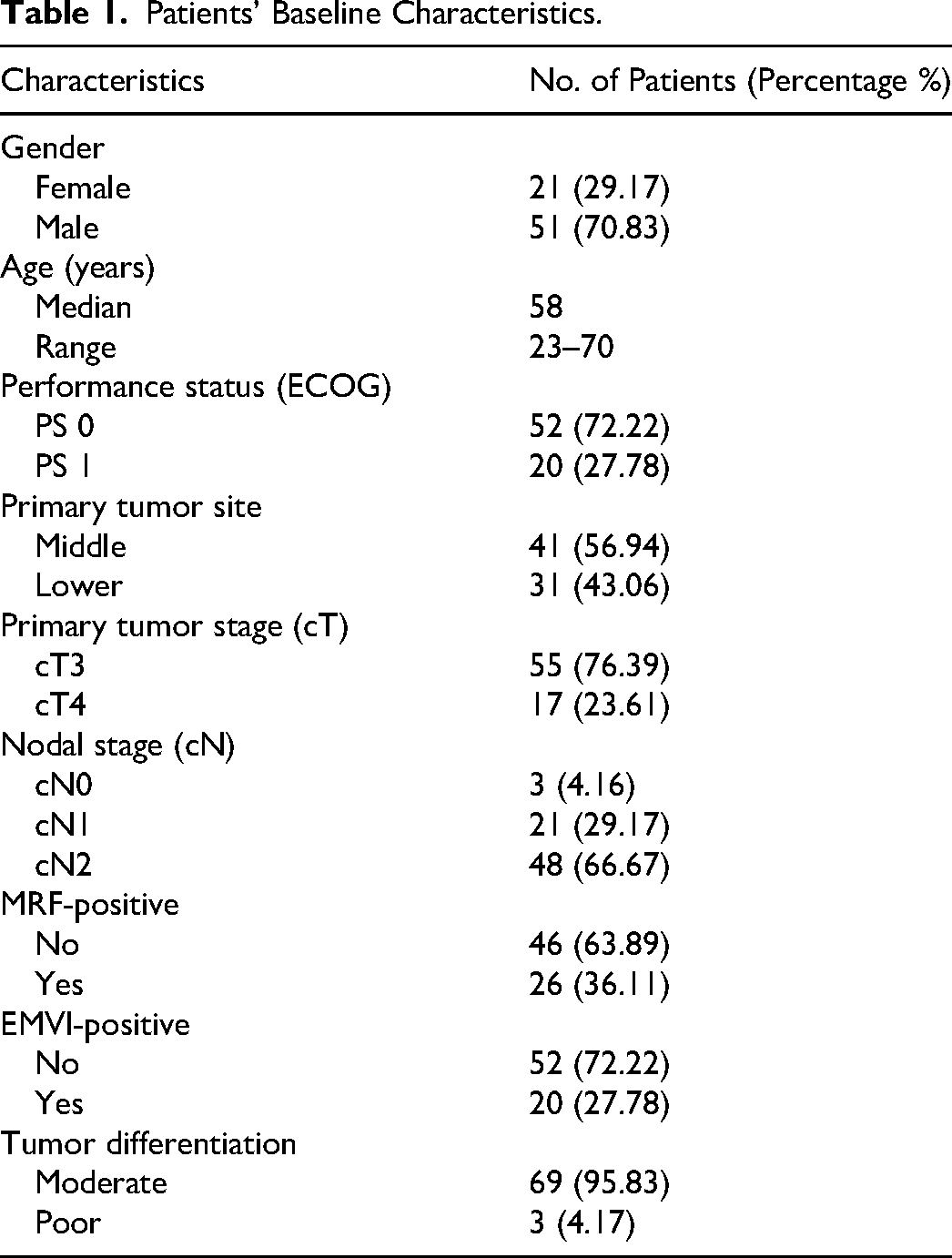
A total of 72 patients with LARC were included in the study. Patients’ characteristics were presented in Table 1. The median age was 58 years (range 23-70 years). 100% of patients had ECOG performance status was 0 and 1. T-stage distribution showed T3 in 55 patients (76.39%) and T4 in 17 patients (23.61%). Nodal involvement was N1 in 21 patients (29.17%) and N2 in 48 patients (66.67%) as shown in Table 1. All participants underwent TME surgery.
Patients’ Baseline Characteristics.
Treatment Results
Patients’ response to treatment was reported in Table 2. The overall response rate to the regimen (TRG 1-3) was 80.56%, with pCR in 18 patients (25.0%). The median duration of follow-up was 36 months (range 6.3 to 60.6 months). Disease-free survival curve of these patients was presented in Figure 1. The 3-year DFS was estimated as 90.6% (95% CI: 82-100%). During follow-up, five recurrences were recorded. Four patients (80%) developed isolated pulmonary spread, while one (20%) had locoregional relapse accompanied by lung involvement.

The 3-Year Disease-Free Survival.
Pathological Features After Surgery.

Toxicity
Toxicity of regimen was described in Table 3. In our study, 67 patients (93.06%) completed six cycles. Hematological toxicities were the most common adverse events. Leukopenia was observed in 22.80% of cycles (grade 1-3). Neutropenia occurred in 19.71% of cycles, including grade 3 in 2.14% and grade 4 in 0.71%. Anemia was reported in 18.76% of cycles. Non-hematological toxicities were mild and included elevated liver enzymes (AST and ALT) and increased creatinine. Diarrhea, nausea, and vomiting were infrequent and predominantly grade 1 and 2. At the patient level (worst grade per patient across induction), grade ≥ 3 events were uncommon. The most frequent was neutropenia in 9/72 (12.5%). Other hematologic ≥ grade 3 adverse events (AEs) included anemia 1/72 (1.4%), and thrombocytopenia 1/72 (1.4%). Non-hematologic ≥ grade 3 AEs were rare: diarrhea 3/72 (4.2%), nausea/vomiting 2/72 (2.8%), and elevated SGOT/SGPT 1/72 (1.4%).
Toxicity of FOLFIRINOX Regimen.

*presented as number (percentage %).
Discussion
Key findings
In this retrospective study of 72 patients with locally advanced lower–middle rectal cancer treated with TNT, induction FOLFIRINOX followed by concurrent CRT and subsequent TME yielded a pCR rate of 25.0%. Moreover, 3-year DFS reached 90.6%, indicating promising oncological outcomes in this Vietnamese cohort. Hematological toxicities were the most common adverse events but were generally manageable with supportive care, and most patients completed the planned six cycles of induction chemotherapy.
Strengths and limitations
This study provides valuable real-world data on the efficacy and safety of an induction FOLFIRINOX-based total neoadjuvant therapy (TNT) strategy in Vietnamese patients with locally advanced rectal cancer, a population for which limited data are available. By evaluating both oncological outcomes and treatment-related toxicities, this study contributes to optimizing treatment strategies and highlights the feasibility of intensive neoadjuvant regimens in a resource-limited setting. However, this study's retrospective design, modest sample size, and potential selection bias may limit the generalizability of our conclusions. Long-term endpoints such as 5-year OS remain under investigation, requiring extended follow-up. Additionally, variations in surgical techniques and supportive care across multiple institutions can introduce treatment heterogeneity.
Comparison with Similar Research
Different TNT regimens have been evaluated in randomized trials, such as short-course radiotherapy (5 × 5 Gy) combined with consolidation chemotherapy (RAPIDO) or induction chemotherapy followed by long-course CRT (PRODIGE 23).9,13 Updated analyses from these studies have consistently demonstrated improvements in pCR rates (up to ∼28%) and better control of distant metastases compared to conventional neoadjuvant CRT followed by surgery and adjuvant chemotherapy.4–6,9 Although direct cross-trial comparisons should be approached cautiously due to variations in patient selection and study design, our pCR rate of 25.0% is within the range reported by larger TNT trials (20-30%). Furthermore, our 3-year DFS of 90.6% is favorable relative to historical data from standard neoadjuvant protocols.5,9
Emerging data also suggest that short-course radiotherapy followed by multi-agent chemotherapy (eg, CAPOX or FOLFOX) can yield comparable pCR rates to long-course CRT plus combination chemotherapy—while potentially reducing the total treatment time. 6 The choice between induction or consolidation chemotherapy in TNT remains an area of active debate. Some studies indicate that induction chemotherapy may help control micro-metastases earlier and improve compliance with systemic therapy, 7 whereas consolidation chemotherapy maximizes tumor downstaging immediately prior to surgery.6,9,14 Our approach—induction FOLFIRINOX followed by CRT—aligns with reports indicating that delivering multi-drug therapy upfront can achieve robust tumor shrinkage and systemic control.9,15
Consistent with other FOLFIRINOX-based protocols, the most common adverse events in our cohort were hematologic, including leukopenia and neutropenia. Non-hematological toxicities—such as nausea, vomiting, and diarrhea—were predominantly mild. Over 90% of patients completed six cycles of chemotherapy, illustrating good tolerability when supportive care (eg, granulocyte colony-stimulating factor) is provided as needed. 9 This reflects findings from contemporary TNT studies that, with close monitoring and dose modifications, intensified chemotherapy can be delivered safely in a neoadjuvant setting.4,6,9
Our experience differs from most prior TNT reports. We adopted a front-loaded induction FOLFIRINOX (×6 cycles) followed by long-course chemoradiation (50.4 Gy with capecitabine) rather than consolidation sequences in a lower-middle–income health system with variable radiotherapy access and supportive-care capacity. Within this context, feasibility was high—93.1% of patients completed all six induction cycles, surgical quality was maintained (R0 100%), and sphincter-preserving procedures 86.1%, despite a higher-risk case-mix enriched for cN2 and T4 disease—suggesting that intensive induction TNT may be delivered safely and consistently outside high-income settings.
Explanations of Findings
The encouraging oncological outcomes in this study may be attributed to several factors. First, the use of induction FOLFIRINOX likely contributed to robust tumor shrinkage and early systemic control, reducing the likelihood of distant metastases. Additionally, CRT following induction chemotherapy may have enhanced radiosensitivity, further improving locoregional control.
The high DFS observed in this cohort suggests that intensive TNT strategies may be effective in Vietnamese patients, despite potential variations in supportive care and surgical techniques. While hematologic toxicities were frequent, their manageable nature suggests that, with appropriate monitoring, FOLFIRINOX-based TNT remains a viable treatment option.
Implications and Actions Needed
In LMIC networks with adequate chemotherapy delivery and radiotherapy planning, induction FOLFIRINOX followed by long-course CRT is a viable TNT option for carefully selected ECOG 0-patient with sufficient organ reserve. For frailer patients or where supportive care is limited, dose-attenuated induction or consolidation-first TNT may be more appropriate.
Prospective randomized studies with a larger patient population are necessary to definitively determine whether induction or consolidatiion chemotherapy is optimal, whether immunotherapy can be beneficial for non-dMMR tumors, and how best to sequence multimodal regimens. In the future, personalized treatment strategies guided by tumor biology and molecular markers (eg, dMMR, KRAS/NRAS status, circulating tumor DNA) may further optimize therapy. Novel approaches combining TNT with immunotherapy or targeted agents are already under exploration in clinical trials.4,16 These efforts aim to build on the encouraging short-term success of TNT, translating into improved long-term survival, organ preservation, and better quality of life.
Conclusions
Our findings support the growing body of evidence that total neoadjuvant therapy—specifically induction FOLFIRINOX followed by concurrent CRT—may yield favorable tumor downstaging, a high pCR rate, and encouraging short-term survival in locally advanced rectal cancer. Early systemic treatment appears to be a crucial element in improving both local and distant disease control.
Footnotes
Abbreviations
Acknowledgments
We sincerely thank the patients and their families for their trust and participation. Our gratitude also goes to the multidisciplinary teams—clinicians, nurses, coordinators, data managers, and administrators—whose dedicated support made this study possible.
Ethical Statement
This study was approved by the Institutional Review Board of Hanoi Medical University, and all procedures were conducted in accordance with ethical guidelines.
Written informed consent was obtained from all participants before initiating treatment, and the study was approved by the Institutional Ethical Review Board No. 908/GCNHDDDNCYSH-DHYHN on 04/05/2023.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.