
Abstract
Purpose
Numerous indicators can be used to predict tumor patients’ prognosis and tumor regression grade (TRG). The role of the neutrophil-lymphocyte ratio (NLR) among individuals with locally advanced rectal cancer (LARC) following neoadjuvant chemoradiotherapy (nCRT) hasn't been studied, nevertheless. This study aims to explore the predictive value of the NLR before nCRT (pre-NLR) in TRG and prognosis of LARC patients undergoing nCRT..
Methods
In this retrospective investigation, 326 LARC patients receiving nCRT in total were included. The link between the pre-NLR and TRG was examined using a logistic regression analysis. A Cox-based nomogram was created in the meanwhile to forecast overall survival (OS). With the use of calibration plots and receiver operating characteristic (ROC) curves, we evaluated the nomogram's predictive capabilities.
Results
The median pre-NLR across 326 patients was 2.2 (interquartile range, IQR: 1.7-2.7). In the logistic regression analysis, only the pre-NLR for TRG in LARC patients receiving nCRT was statistically significant (odds ratio, OR = 0.62, 95% CI: 0.47-0.80, P < 0.001). Pre-NLR, nCRT with surgery interval, ypTNM stage, TRG, vascular invasion, adjuvant chemotherapy, and carbohydrate antigen 19–9 before nCRT were revealed to be OS predictors in the Cox multivariate analysis. According to calibration plots and ROC curves, the predictive nomogram demonstrated high statistical performance on internal validation.
Conclusion
This study demonstrated that a lower pre-NLR was probably associated with a greater rate of TRG in LARC patients undergoing nCRT. Furthermore, the pre-NLR was credibly correlated with OS in LARC patients undergoing nCRT. Meanwhile, we constructed a nomogram for predicting the prognosis in LARC patients undergoing nCRT.
Keywords
Introduction
With approximately 1.9 million new cases along with more than 915 thousand deaths from cancer-related causes globally in 2020, colorectal tumors ranks as the third most frequent malignancy. 1 Among the patients with colorectal cancer, rectal cancer accounts for approximately two-fifths of these cases. Despite the overall declining trend of incidence and mortality from colorectal cancer, the incidence of rectal cancer in the young population has been increasing in the USA and Europe.2–4 Rectal cancer has been regarded as an important barrier to extending life span, and it places substantial physical and financial burdens on all patients with rectal cancer. For rectal cancer, appropriate treatment, including surgical treatment and multimodality therapy, can prevent recurrence and improve survival. In general, a transmural tumor or node-positive disease without distant metastases is referred to as local advanced rectal cancer (LARC). Currently, the recommended course of treatment for individuals with LARC is a combination of complete mesorectal excision (TME) surgery and neoadjuvant chemoradiotherapy (nCRT). 5 Studies have found that better local control and reduction of toxicity profiles could be achieved by combining nCRT and TME in comparison to postoperative chemoradiotherapy with similar survival outcomes.6,7 But not all patients benefited from nCRT, and there was a specific sensitivity of LARC patients to it. It is important to note that 20% to 46% of LARC individuals who had known postoperative pathology data had tumor cells that did not considerably or at all regress, and these individuals did not react to nCRT.8–10 Routine nCRT might result in overtreatment and additional toxicity for those patients. 11 Therefore, accurately identifying LARC patients who could benefit from nCRT is a key clinical problem that urgently needs to be addressed.
The neutrophil-lymphocyte ratio (NLR) is the ratio of neutrophil counts to lymphocyte counts as a measure of systemic inflammation. Its connection to tumor prognosis has been discovered in an increasing number of research. A high NLR is a sign of a bad prognosis in women with breast and colorectal cancer patients, according to certain research.12,13 The NLR's ability to predict tumor regression grade (TRG) and outcome of survival in LARC patients receiving nCRT is yet unknown. In this retrospective study, we sought to examine the predictive value of the NLR prior to nCRT (pre-NLR) in the TRG of LARC patients receiving nCRT. A statistical analysis of the clinicopathological information from LARC patients receiving nCRT was carried out in order to develop a nomogram depending on the pre-NLR that could predict the long-term outcome of patients.
Patient and Methods
Patient Population
In this study, 326 LARC patients who underwent nCRT at the Cancer Hospital (CHCAMS, Beijing, P.R. China) between November 1, 2012 and October 30, 2018, were consecutively retrospectively examined. For this study, all patient data has been de-identified. The following were the inclusion requirements: Colonoscopy-based pathological diagnosis of rectal adenocarcinoma, getting nCRT, imaging suggestive of stage II-III cTNM at the time of first diagnosis and no distant metastases, and completion of complete mesorectal excision (TME). The following were the exclusion requirements: 1) Lack of certain clinical feature data, 2) co-existing malignancies at other locations, and 3) preoperative imaging during or following nCRT therapy detecting new distant metastases. This study's reporting complies with STROBE criteria. 14
Clinical variables were all gathered by Hospital Information System. We select the Dworak standard for TRG. We classify TRG-1 and TRG-2 as poor responses to Dworak-TRG, and TRG-3 and TRG-4 as favorable responses. 15
Treatment
nCRT was administered to all patients at a median dosage was 50 Gy (range: 45-60 Gy). Volumetric modulated arc treatment (VMAT), intensity modulated radiation therapy (IMRT), and three-dimensional conformal radiation therapy (3D-CRT) are three types of concurrent radiotherapy. Capecitabine (X), X + bevacizumab, X + oxaliplatin, and raltitrexed were the concurrent chemotherapy regimens. Before receiving TME, all patients had received nCRT for at least 4 weeks.
Follow-up
Every 3 months for the first 2 years following surgery, and every 6 months for the next 3 to 5 years, all patients underwent hospital reviews. Physical examination, bloodstream tumor markers, chest, abdomen, pelvic, or whole-body PET-CT exams, if needed, are all included in the evaluation. The target for patient follow-up was August 31, 2021, during which time we checked in on patients at regular intervals. Overall survival (OS) was calculated as the time from the time of pathological diagnosis to the time of any cause of death or the last follow-up.
Statistical Analysis
To assess the odds ratio (OR) and 95% confidence interval (95% CI) of TRG, logistic regression analysis was used. The hazard ratio (HR) and 95% confidence interval (CI) of OS were assessed using Cox regression analysis. These statistically significant factors will be included in the multivariate model's univariate analysis. To predict the 3-year and 5-year OS, a nomogram was created based on significant features found by the multivariate analysis using the Cox regression model. With the use of calibration plots and receiver operating characteristic (ROC) curves, we evaluated the nomogram's predictive capabilities. R 4.1.0 was used to perform all statistical analyses. Statistical significance was defined as two-tailed P values that are below 0.05.
Results
Patient Characteristics
The study's inclusion criteria were satisfied by a total of 326 patients, 98 (30.1%) of whom were female and 228 (69.9%) were male patients. The median pre-NLR was 2.2 (IQR: 1.7-2.7). In addition, 42.0% (137/326) of patients reported ever drinking, 48.8% (159/326) of patients reported ever smoking, and 37.4% (122/326) of patients reported ever having a chronic illness. Among the patients, 59.2% (193/326) had a TRG score of 1–2. In terms of the radiation modality used prior to surgery, 289 (88.7%) patients underwent VMAT, 29 (8.9%) underwent IMRT, and 8 (2.5%) underwent 3D-CRT. 289 (88.7%) of the patients who underwent chemotherapy before surgery received the capecitabine regimen, 19 (5.8%) received capecitabine in combination with oxaliplatin, and 18 (5.5%) received other regimens. Table 1 displays the demographics and clinicopathological traits.
Clinical Features and Therapeutic Methods for Individuals with Locally Advanced Rectal Cancer

nCRT, neoadjuvant chemoradiotherapy; pre-NLR, neutrophil-lymphocyte ratio before nCRT; IQR, interquartile range; TRG, tumor regression grade; VMAT, volumetric modulated arc therapy; IMRT, intensity modulated radiation therapy; 3D-CRT, 3-dimensional conformal radiation therapy; pre-CEA, carcinoembryonic antigen before nCRT; pre-CA19-9, carbohydrate antigen 19-9 before nCRT.
Logistic Regression Analyses of Prognostic Factors for TRG
In order to estimate TRG in LARC patients undergoing nCRT, variables such as pre-NLR, age, sex, smoking history, drinking history, chronic disease history, cTNM stage, radiotherapy type before surgery, chemotherapy type before surgery, pre-CEA, and pre-CA19-9 were chosen. Only the pre-NLR (OR = 0.62, 95% CI: 0.47-0.80, P < 0.001) for TRG in LARC patients receiving nCRT and TME was statistically significant in the univariate analysis, while the other factors were not (Table 2). Subgroup analysis was performed by logistic regression to further assess the correlation of pre-NLR with TRG, and we found that most subgroups were statistically significant (Figure 1).
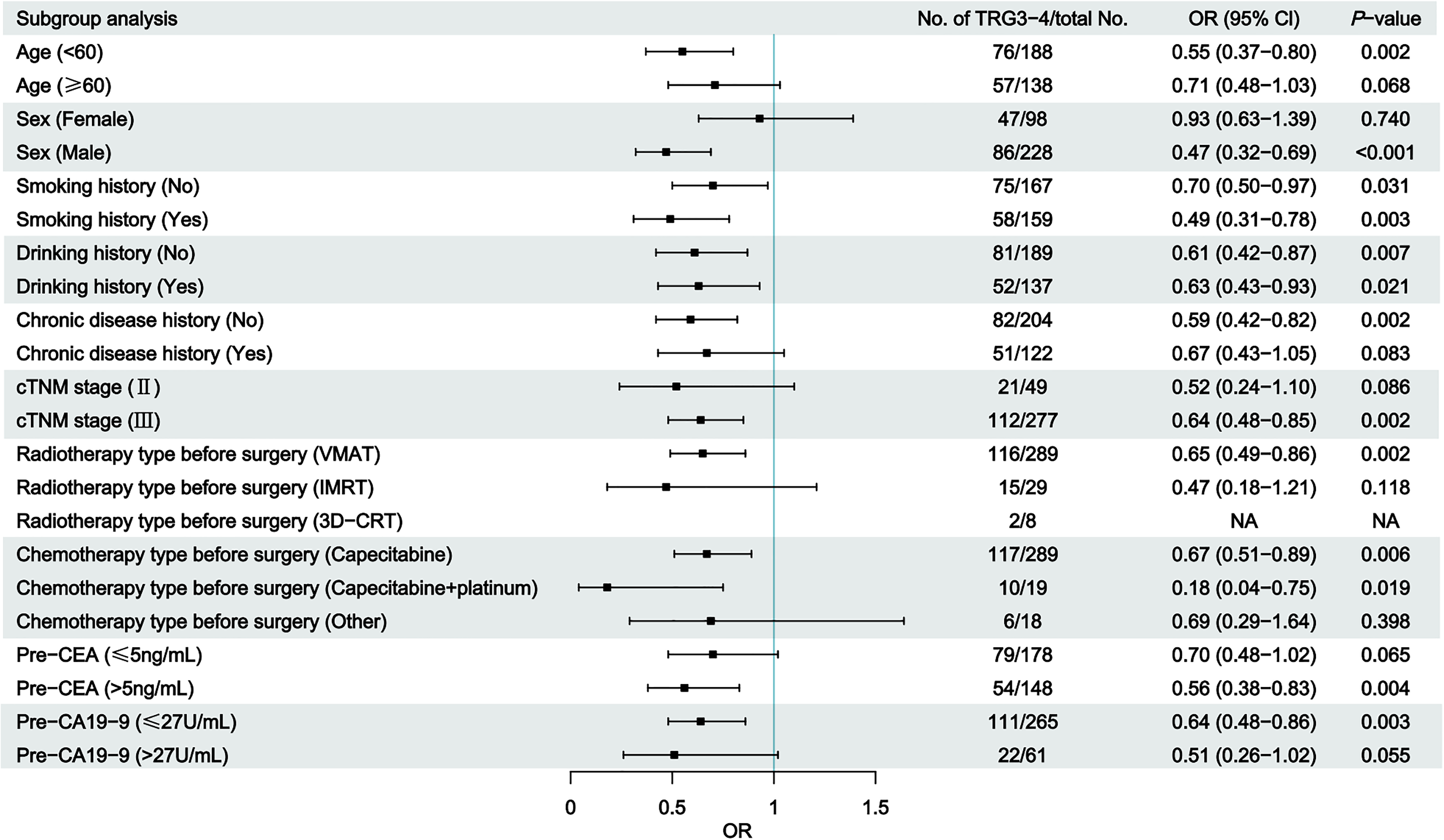
Subgroup analysis of logistic regression analyses of tumor regression grade factors.
Logistic Regression Analysis of Tumor Regression Grade Factors

nCRT, neoadjuvant chemoradiotherapy; pre-NLR, neutrophil-lymphocyte ratio before nCRT; VMAT, volumetric modulated arc therapy; IMRT, intensity modulated radiation therapy; 3D-CRT, 3-dimensional conformal radiation therapy; pre-CEA, carcinoembryonic antigen before nCRT; pre-CA19-9, carbohydrate antigen 19-9 before nCRT; OR, odds ratio; 95% CI, 95% confident interval.
Cox Regression Analysis of Prognostic Factors for OS
To estimate OS in LARC patients receiving nCRT and TME, all factors listed in Table 1 were chosen for univariate Cox regression analysis. Pre-NLR, smoking history, nCRT with surgical interval, ypTNM, TRG, vascular invasion, neural invasion, adjuvant chemotherapy, and pre-CA19–9 were variables in the univariate analysis that were independently linked with OS in LARC patients receiving nCRT and TME. The multivariate model incorporated the statistically significant factors from the univariate study. We found that pre-NLR (HR = 1.25, 1.02-1.54, P = 0.033), nCRT with surgery interval (2-3 mouths, HR = 0.52, 0.27-1.00, P = 0.049; > 3 mouths, HR = 0.25, 0.08-0.79, P = 0.019), ypTNM stage (stage III, HR = 21.81, 3.33-142.99, P = 0.001), TRG (TRG = 2, HR = 0.34, 0.17-0.70, P = 0.003; TRG = 3, HR = 0.29, 0.12-0.73, P = 0.008), vascular invasion (HR = 2.18, 1.00-4.75, P = 0.049), adjuvant chemotherapy (HR = 0.51, 0.30-0.86, P = 0.012) and Pre-CA19–9 (>27, HR = 2.12, 1.17-3.84, P = 0.014) were predictors of OS (Table 3).
Cox Regression Analysis of Prognostic Factors for Overall Survival

nCRT, neoadjuvant chemoradiotherapy; pre-NLR, neutrophil-lymphocyte ratio before nCRT; TRG, tumor regression grade; VMAT, volumetric modulated arc therapy; IMRT, intensity modulated radiation therapy; 3D-CRT, 3-dimensional conformal radiation therapy; pre-CEA, carcinoembryonic antigen before nCRT; pre-CA19-9, carbohydrate antigen 19-9 before nCRT; HR, hazard ratio; 95% CI, 95% confident interval.
Construction of a Nomogram to Predict OS
With the independent factors, a nomogram of 3-year and 5-year OS was created (Figure 2). In multivariate analysis, pre-NLR, nCRT with surgery interval, ypTNM stage, TRG, vascular invasion, adjuvant chemotherapy, and pre-CA19–9 were statistically significant for predicting OS. As a result, these factors were added to the nomogram. From these characteristics, a weighted total score is produced, which is used to predict the 3-year and 5-year OS for LARC patients who got nCRT. Patients with a lower pre-NLR had a higher overall survival.

Nomograms for predicting overall survival. nCRT, neoadjuvant chemoradiotherapy; pre-NLR, neutrophil-lymphocyte ratio before nCRT; TRG, tumor regression grade; pre-CA19-9, carbohydrate antigen 19-9 before nCRT; OS, overall survival.
Evaluation of the Nomogram
According to a multivariate model in the dataset, a nomogram to forecast 3-year and 5-year OS in LARC patients having nCRT was created. The model predicted OS with high accuracy, and calibration curves for the likelihood of OS showed strong concordance between what was observed and nomogram-predicted OS percentages in the cohort (Figure 3). The cohort's area under the ROC curve (AUC) was calculated, and the AUCs for 3-year and 5-year OS were 0.8343 and 0.8625, respectively (Figure 4).

Overall survival nomogram model calibration curves. (a) 3-year and (b) 5-year. OS, overall survival.

The receiver operating characteristic curve of the overall survival nomogram model. (a) 3-year and (b) 5-year.
Discussion
With improvements in surgical techniques, chemotherapy and radiotherapy, important advances have been made in the multimodality treatment of LARC in recent decades. Multiple randomized controlled studies reported that nCRT combined with TME exhibited an advantage in local tumor control for patients with LARC.16–19 Hence, nCRT with TME has been considered the standard of care for LARC. However, varied responses of patients with rectal cancer to nCRT have been reported. Bosset JF et al found that preoperative and postoperative chemotherapy could confer a remarkable benefit in terms of local control for patients with resectable rectal cancer, while preoperative radiotherapy failed to improve the prognosis of patients with resectable rectal cancer. 20 Thus, the prognosis of patients with LARC might be influenced by variable responses to nCRT. The existing technical methods cannot accurately identify these patients, which leads to patients suffering from additional chemoradiotherapy toxicity before surgery and delaying the surgery. After radiotherapy, intestinal canal edema becomes brittle, leading to an increased risk of perioperative complications.11,21 This results in a passive situation of wasted medical and economic resources and increased difficulty in follow-up treatment. Therefore, the predictor of response to nCRT could provide some reference value and improve individualized clinical decision-making regarding neoadjuvant treatment choice.
In this study, we collected clinical and pathological data of 326 LARC patients undergoing nCRT combined with TME and followed up each of them. First, we analyzed the effect of pre-NLR, age, sex, smoking history, drinking history, chronic disease history, cTNM stage, radiotherapy type before surgery, chemotherapy type before surgery, pre-CEA and pre-CA19-9 on TRG after nCRT and found that only pre-NLR was statistically significant. Our study showed that pre-NLR was negatively correlated with TRG, and the higher the pre-NLR, the less sensitive the patient was to nCRT, and the poorer the nCRT treatment effect, the lower the pre-NLR, the more sensitive the patient was to nCRT and the better the treatment effect. We demonstrated that the pre-NLR could be a predictor for nCRT response in patients with LARC. The potential mechanisms can be that the systemic inflammatory response might play a crucial role in facilitating tumor development by providing a favorable tumor microenvironment, and among different types of inflammatory cells infiltrating the tumor microenvironment, several tumor-promoting cytokines generated by neutrophils, including vascular endothelial growth factor, interleukin-18 and matrix metalloproteinases, could promote tumor progression.22–24 Moreover, elevated neutrophils restrain the anticancer activity of natural killer cells.25,26 On the other hand, the host anticancer response could be undermined owing to decreased lymphocytes. Neutrophils and lymphocytes may contribute to cancer metastasis by coordinating growth and angiogenesis.27–30 Thus, the balance between systemic inflammation and anticancer immunity could be reflected by NLR to some extent. 31 The high NLR indicates the breaking of the balance and the weakening of anticancer immunity, consequently leading to tumor progression and impaired therapeutic efficacy of nCRT.
In recent years, peripheral indicators of immunity/inflammation, including NLR, have been studied for possible correlations with survival outcomes in various types of cancers. Zheng Z et al found that NLR was a prognostic factor in patients with resectable esophageal squamous cell carcinoma, which was significantly associated with poor prognosis with respect to disease-free survival (DFS). 32 Qian C et al reported a positive relationship between a high NLR and shorter DFS and OS in patients with gastrointestinal cancer. 33 Hizal M et al also found that advanced renal cell carcinoma patients with an elevated pre-treatment NLR had a shorter median overall survival than patients with a lower NLR. 34 In addition to pre-treatment NLR, the combination of pre-treatment NLR and post-treatment NLR could be regarded as a prognostic factor with better accuracy in patients with hepatocellular carcinoma. 35 Furthermore, we conducted an analysis regarding the correlation between various inflammation-related biomarkers, such as C-reactive protein (CRP), C-reactive protein-albumin ratio (CAR), platelet-lymphocyte ratio (PLR), lymphocyte-monocyte ratio (LMR), systemic immune inflammation index (SII), and systemic inflammation response index (SIRI), with the TRG in LARC patients undergoing nCRT and TRG. These inflammation-related biomarkers were assessed within the dataset at our center. However, none of these biomarkers, including CRP (P = 0.539), CAR (P = 0.434), PLR (P = 0.079), LMR (P = 0.602), SII (P = 0.277), and SIRI (P = 0.304), exhibited statistically significant correlations with TRG. Similarly, no statistically significant associations were observed between these biomarkers and OS, namely, CRP (P = 0.185), CAR (P = 0.517), PLR (P = 0.294), LMR (P = 0.867), SII (P = 0.578), and SIRI (P = 0.112). Consequently, these biomarkers were not integrated into the predictive model.
The following are the benefits of our research. First, we discovered a link between pre-NLR and the therapeutic impact of LARC in patients who received nCRT, which may effectively discriminate the population sensitive/resistant to nCRT, paving the way for future clinical precision therapy and scientific study. Second, we conducted a Cox regression evaluation of the pre-NLR with common features and discovered that the pre-NLR was related to the OS of LARC patients receiving nCRT. We also built a nomogram that predicted the 5-year rate of survival. Third, we gathered clinical and pathological data of patients, as well as therapy information, hematological parameters, and social features, and examined more complete aspects. Our study, however, had certain drawbacks. For starters, this was a single-center study with a tiny sample size. The relevant results must be confirmed further by increasing the sample size. Second, our research cohort was gathered retrospectively over time.
Conclusion
This study demonstrates that a lower pre-NLR is probably associated with a greater rate of TRG in LARC undergoing nCRT. Furthermore, a low pre-NLR is credibly correlated with better OS in LARC undergoing nCRT. Meanwhile, we successfully constructed a nomogram based on available clinicopathologic and pathological factors for predicting the probability of 3-year and 5-year OS in LARC patients undergoing nCRT.
Footnotes
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding authors on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The National Key Research and Development Program of China, The CAMS Innovation Fund for Medical Sciences (CIFMS), (grant number 2020AAA0109501, 2021-I2M-1-015).
Ethics Approval
The retrospective study was approved by the Ethics Committee of the National Cancer Center/Cancer Hospital, the Chinese Academy of Medical Sciences and Peking Union Medical College (approval no. NCC2016JZ-06).