
Abstract
Purpose
To compare the dosimetry and biological risk of volumetric modulated arc therapy (VMAT), helical tomotherapy (HT) and cyberKnife (CK) in the treatment of lung oligometastases.
Methods and materials
This retrospective study included a cohort of 21 lung oligometastasis patients, each with 2 or 3 lesions, who had previously undergone stereotactic body radiation therapy (SBRT). VMAT, HT and CK plans were made for each patient. The dose distribution of planning target volume (PTV) and organs at risk (OARs) were evaluated. Three biological risks were evaluated, namely radiation pneumonitis (RP), coronary artery disease (CAD) and congestive heart failure (CHF). Monitor Units (MUs) and beam-on-time were also recorded.
Results
All techniques were able to produce clinically deliverable plans. The expected biological risks for VMAT plans, CK plans, and HT plans were 6.69%, 5.05%, 5.88% for RP, 1.20%, 1.15%, and 1.17% for CAD, 1.26%, 1.19%, and 1.22% for CHF. The expected risks of RP were slightly lower in CK plans compared to VMAT and HT plans (p < 0.001), with VMAT plans showing the highest expected risks. For central lung cancer, the expected CAD risks of CK and HT plans were lower than those of VMAT plans (p < 0.05). The delivery efficiency of VMAT plans was significantly higher than that of CK plans and HT plans.
Conclusions
All three techniques, VMAT, HT, and CK, meet the therapeutic requirements for target coverage and dose constraints for OARs. Although there are statistical differences, the difference between the expected risk values of RP and CAD is very small, so the clinical manifestations may not show differences.
Keywords
Introduction
Stereotactic body radiation therapy (SBRT), also known as stereotactic ablative radiotherapy (SABR), has emerged as a viable therapeutic alternative for patients with early-stage lung cancer who are unsuitable or refusing surgery.1,2 Recently, SBRT has been increasingly used to treat multiple lung metastases. 3 Notably, SBRT has shown promising curative potential in patients presenting with pulmonary oligometastases, typically defined as fewer than five metastatic lesions.4–6 The technological advancements in SBRT delivery systems, coupled with more rigorous treatment planning requirements, have enabled highly precise targeting and conformal dose distributions. 7 Due to its excellent local control and an acceptable toxicity profile, SBRT is gradually being recognized as the a standard-of-care in the multidisciplinary management of patients with lung oligometastases. 8
Currently, the primary treatment technologies available for multi-target lung SBRT include linac-based SBRT, helical tomotherapy (HT), and CyberKnife (CK). As a linac-based SBRT irradiation technique, volumetric modulated arc therapy (VMAT) achieves complex dose distribution conformed to multiple targets by adjusting non-coplanar arcs (full arcs/ partial arcs), multileaf collimator (MLC) field shaping, six-dimensional couch and gantry rotation speeds, and dose rate. 9 HT offers fan-beam IMRT through continuous and synchronized gantry and couch movements during the irradiation process, enabling conformal high-dose irradiation to the targets. 10 CK is a linear accelerator mounted on a 6-axic robotic arm, equipped with tumor real-time tracking system. CK can deliver hundreds of noncoplanar and nonisocentric treatment beams for to achieve conformal irradiation. 11 Due to their distinct dose optimization algorithms and delivery techniques, multi-target lung SBRT using VMAT, HT, and CK causes varying planning dose distributions and radiation pneumonia risks.
So far, several studies have reported the dosimetric comparison of these techniques in single-target lung SBRT. Ding et al 12 and Shao et al 13 respectively compared the coplanar and non-coplanar radiation delivered by CK and linac-IMRT for single-target lung SBRT. Yu et al 14 evaluated the dosimetry and planning quality of CK and Varian knowledge-based-planning-VMAT for 13 single-target lung SBRT patients. Kannarunimit et al 15 and Okutan et al 16 compared the dosimetric characteristics and radiation pneumonitis risk associated with VMAT, HT, and CK in 9 patients with single-target central lung cancer and 15 patients with single-target peripheral lung cancer, respectively. However, there is limited comparison of these techniques in multi-target lung SBRT, except for a study by Li et al 17 comparing VMAT and HT in 21 patients with primary lung cancer/lung metastasis, which includes 6 dual-lesion patients. To our knowledge, there is currently no study comparing the physical dosimetry and biological advancements of VMAT, HT, and CK in multi-target lung SBRT.
The objective of this study was to compare the physical dosimetry and expected biological risks associated with VMAT, HT, and CK in the treatment of lung oligometastases. This study specifically focused on patients with 2–3 lung oligometastatic lesions, exploring the differences in physical and biological dose among various irradiation techniques for multi-target SBRT. We anticipated that the findings of this research will offer guidance and insights for selecting treatment technologies based on dosimetry, tumor control, and normal tissue protection.
Materials and Methods
Patient Data
A total of 21 patients were obtained by searching the database of our center from January 2018 to June 2022, with the search criteria being lung cancer oligometastatic patients and SBRT. All 21 patients were included in this retrospective study. All patients received SBRT for lung oligometastases during this period, which were stage IV. All patients were considered unfit for surgery or unwilling to undergo surgery. The ages of patient cohort ranged from 46 to 81 years (median age 67, mean age 68). The patient cohort consisted of 7 males and 14 females. The primary cancers included NSCLC (57.2%), esophageal cancer (19.0%) and thymic cancer (23.8%), of which 16 were Squamous cell carcinoma (SSC) and 5 were Adenocarcinoma (AC). Most patients had 2 lesions (85.7%), and the rest had 3 lesions (14.3%). 61.9% of the patients received 50 Gy in 5 fractions, and 38.1% of the patients received 50 Gy in 4 fractions. Patient and tumor characteristics are shown in Table 1.
The Clinical and Histopathological Characteristics of the 21 Patients.
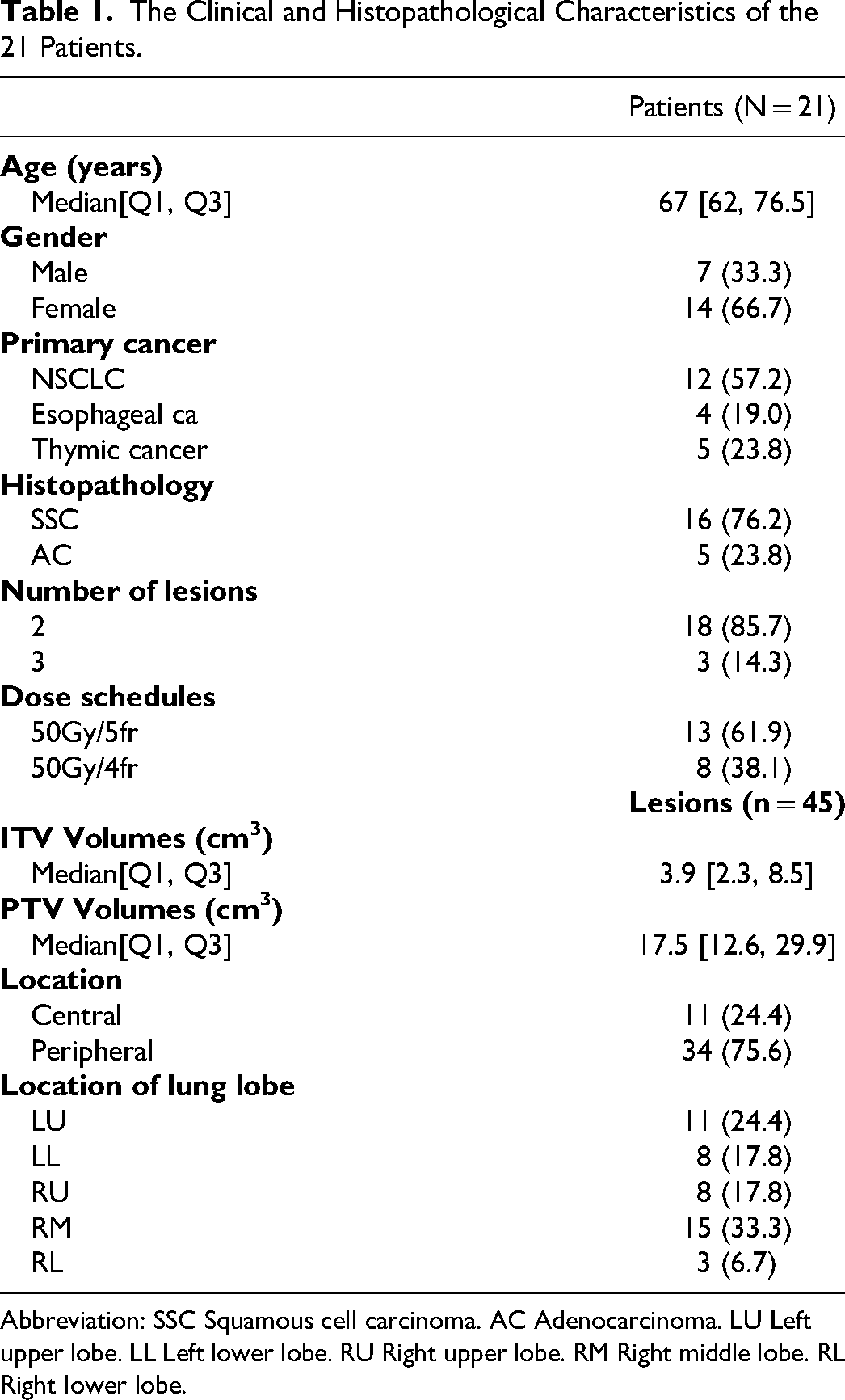
Abbreviation: SSC Squamous cell carcinoma. AC Adenocarcinoma. LU Left upper lobe. LL Left lower lobe. RU Right upper lobe. RM Right middle lobe. RL Right lower lobe.
Each patient was positioned in the supine position, and a head-neck-shoulder thermoplastic mask or vacuum pad was utilized to fix the body position. Siemens Somatom Definition AS CT was employed to scan all patients in the state of free breathing movement to obtain 4D CT images. Each 4D CT image containing 9 phases, with a slice thickness of 3 mm. Phase merging was performed on 4D CT images to generate maximum intensity projection (MIP) images. Planning target volume (PTV) was generated by adding a uniform 5 mm margin to interal target volume (ITV) to adapt to the uncertainty of patient positioning based on tumor size, location and synchronous movement. In addition, two experienced physicists evaluated the motion of the tumors to confirm that the synchronous motion of the tumors was less than 1 cm. Radiation oncologists described the OARs including lung, spinal cord, esophagus, trachea, great vessels, ribs, heart and major cardiac substructures [left atrium (LA), right atrium (RA), left ventricle (LV), right ventricle (RV), left anterior descending coronary artery (LAD)]. Our study was reported according to the STROBE checklist for cohort studies. 18
Planning Configuration
All plan were retrospectively made by three experienced planners for comparison in this study. All plans in this study were generated in accordance with our institutional planning standards. The three planners cross checked each other's plan to minimize differences between planners. 95% of the PTV is covered by the prescription dose and 99% of PTV is covered by 99% of the prescription dose, prescription isodose line is between 60% and 75%.
The VMAT plan was generated using the Pinnacle 9.10 (Philips radiation oncology systems, Fitchburg, WI, USA) planning system. Dose calculation was performed using the Collapsed Cone Convolution (CCC) Superposition with a 2 × 2 × 2 mm3 dose calculation grid. VMAT plans were implemented on 6 MV Edge linear accelerator (Varian, Palo Alto, CA, USA), which was equipped with 120 High definition multileaf collimator (MLC). The VMAT plans were single isocenter plans, and the isocenters were set near the centroid of all lesions. The plan used 2 coplanar full arcs. The collimator angle of all those arcs was selected so that when the gantry rotated around the patient, the MLC opening between tumors was minimized. The jaw tracking was used to further minimize the out-of-field leakage dose.
The HT plan was generated using the Accuracy Precision 1.1.1.1 (Accuray Inc., Sunnyvale, CA, USA) planning system of the fourth-generation 6 MV helical tomotherapy system (Radixact, Accuray Inc., Sunnyvale, CA, USA). The system equipped 64 binary aerodynamic MLC with a 6.25 mm projected leaf width at the isocenter. The HT plans adopted spiral rotary intensity modulation technology, with a 2.5 cm dynamic jaw opening, a modulation factor (MF) of 2.0–3.0 and a pitch factor of 0.215. The dose was calculated using the Convolution-Superposition algorithm, and the dose calculation mesh was 2.0 mm.
The CK plan was generated using Precision 1.0 software (Accuray Inc., Sunnyvale, CA, USA) of the M6 CK robotic system (Accuray Inc., Sunnyvale, CA, USA) with a 6 MV linear accelerator, using multiple nonisocentric 6 MV beams to target each metastasis. The dose was calculated with Monte-Carlo algorithm and using a 1-pixel high-resolution mesh. Two or three appropriate cone collimators (with circular fields of 5 to 60 mm) are selected for each case according to its size. In the premise of maintaining the clinical quality of the plan, beams and nodes were minimized to reduce treatment time to the extent possible.
Dosimetry and Plan Quality
VMAT, HT and CK plans were transferred to MIM Maestro 7.1.4 (MIM Software Inc., OH, USA) workstation respectively to compare the planning quality and physical dose.
For PTV, the target coverage (average of all PTVs) was obtained from the dose-volume histogram (DVH), which was used for the target dosimetry evaluation of three types of plan. In addition, the following parameters were collected and evaluated:
The conformity index (CI) was the product of the target coverage and the healthy tissue volume receiving dose equal to or greater than the reference dose, which measured the conformity of the size and shape of the radiation dose distribution volume and the targets. The CI was expressed as
19
: CI = VT,Rx2 / (VT × VRx), where VT,Rx was the PTV volume covered by prescription dose. VT is the PTV volume. VRx is the prescription dose volume. The gradient index (GI) was used to evaluate the dose fall-off of normal tissue around the target. The GI was reported in terms of 50% of prescription dose and was defined as by R50%.The GI was expressed as
20
: R50% = V50%Rx / VRx. Where V50%Rx refers to the volume covered by 50% of the prescription dose. Lower GI means that the better dose fall-off from PTV to normal tissue. D2cm was defined as the maximum dose at 2 cm from PTV in any direction.
For lung, the volume of lung receiving 5 Gy, 15 Gy, 20 Gy and 30 Gy (V5, V15, V20, V30) and the mean lung dose (MLD) for whole were recorded. Lung volume was defined as total lung volume minus ITV.
For heart, the mean and maximum dose (Dmean, Dmax) of the whole heart were collected. Recent studies have found that the whole heart dose was not enough to achieve precise heart protection.21–23 A previous study of our group also found that compared with the whole heart avoidance plan, the cardiac substructure avoidance plan showed new advantages, 24 so this study also collected the doses of the main substructure substructures. For cardiac substructures, Dmean of LA, RA, LV and RV and Dmax of LAD were collected.
For other OARs, Dmax of spinal cord, trachea, rib and esophagus, and great vessels were collected.
Biological Risk
The expected biological risk was calculated to predict the disease risk caused by side effects of radiotherapy. This study estimated the expected risk of radiation pneumonitis (RP), coronary artery disease (CAD) and congestive heart failure (CHF). All plans converted the tissue dose to the equivalent dose in 2Gy fractions (EQD2). The α ⁄ β ratio was 3Gy for RP, 2Gy for CAD and CHF.
For the estimation of RP risk, we adopted the Lyman Kutcher Burman (LKB) model 25 to calculate the normal tissue complication probability (NTCP) of ≥ grade 2 RP. The linear quadratic model and 3Gy of α ⁄ β ratio were used in the model. MATLAB r2016b (MathWorks, Natick, Massachusetts, USA) was used for calculating NTCP.
For the estimation of CAD risk, the risk model of van Nimwegen 26 and Darby 27 was adopted. The model showed that there was a linear dose-response relationship between the average dose of coronary artery and the CAD risk, and the relative risk of clinical events was 7.4% / Gy.
For the estimation of CHF risk, we adopted the risk model of van Nimwegen, 28 which showed the linear dose-response relationship between the average dose of LV and the CHF risk, and the relative risk of clinical events was 9.0% / Gy.
Treatment Efficiency
The Monitor Units (MUs) and beam-on-time of the three types of plan were collected and evaluated. The dose rates of VMAT, CK and HT were 1400 MU/min, 1000 MU/min and 850 MU/min, respectively. The beam-on-time did not include the time of imaging.
Statistical Method
SPSS 20.0 (IBM Crop., Armonk, NY, USA) statistical software was used for data analysis. Friedman test was used for comparison among VMAT, CK and HT plans. Wilcoxon signed rank test was used for pairwise comparison of VMAT, CK and HT plans. P value < 0.05 means that the statistical difference between the two groups is significant.
Result
Dosimetry and Plan Quality
All plan achieved the target and OARs dose constraints of RTOG and/or agreement of our center, details in Supplemental materials (Table S1&S2). According to the study design, the PTV target coverage of VMAT plans (average 95.59%), CK plans (average 95.56%) and HT plans (average 95.66%) met the clinical requirements. As shown in Figure 1, all three technologies achieved perfect dose coverage of the target, but there are differences in the low-dose areas outside the target (such as the lung).
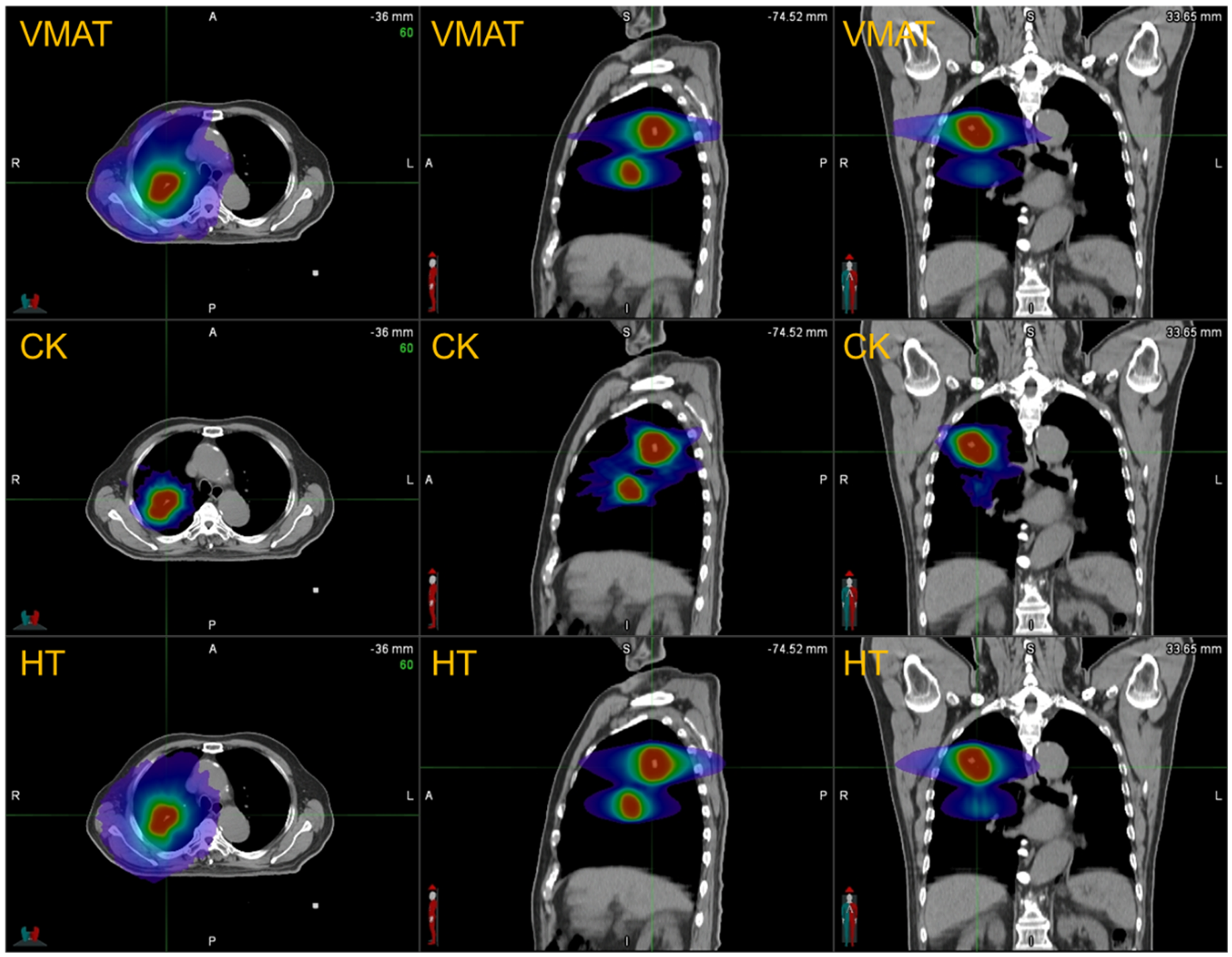
Comparison of typical dose distribution among VMAT, CK, and HT plans.
In Figure 2, the CI of VMAT plans and CK plans was better than that of HT plans (p < 0.001 for both comparisons), and VMAT plans achieved the best CI. The R50% and D2cm of CK plans were better than VMAT plans and HT plans (p < 0.001 for both comparisons), and the R50% and D2cm of HT plans were slightly better than VMAT plans (p < 0.001 for both comparisons). The details shown in Supplemental materials (Table S3).
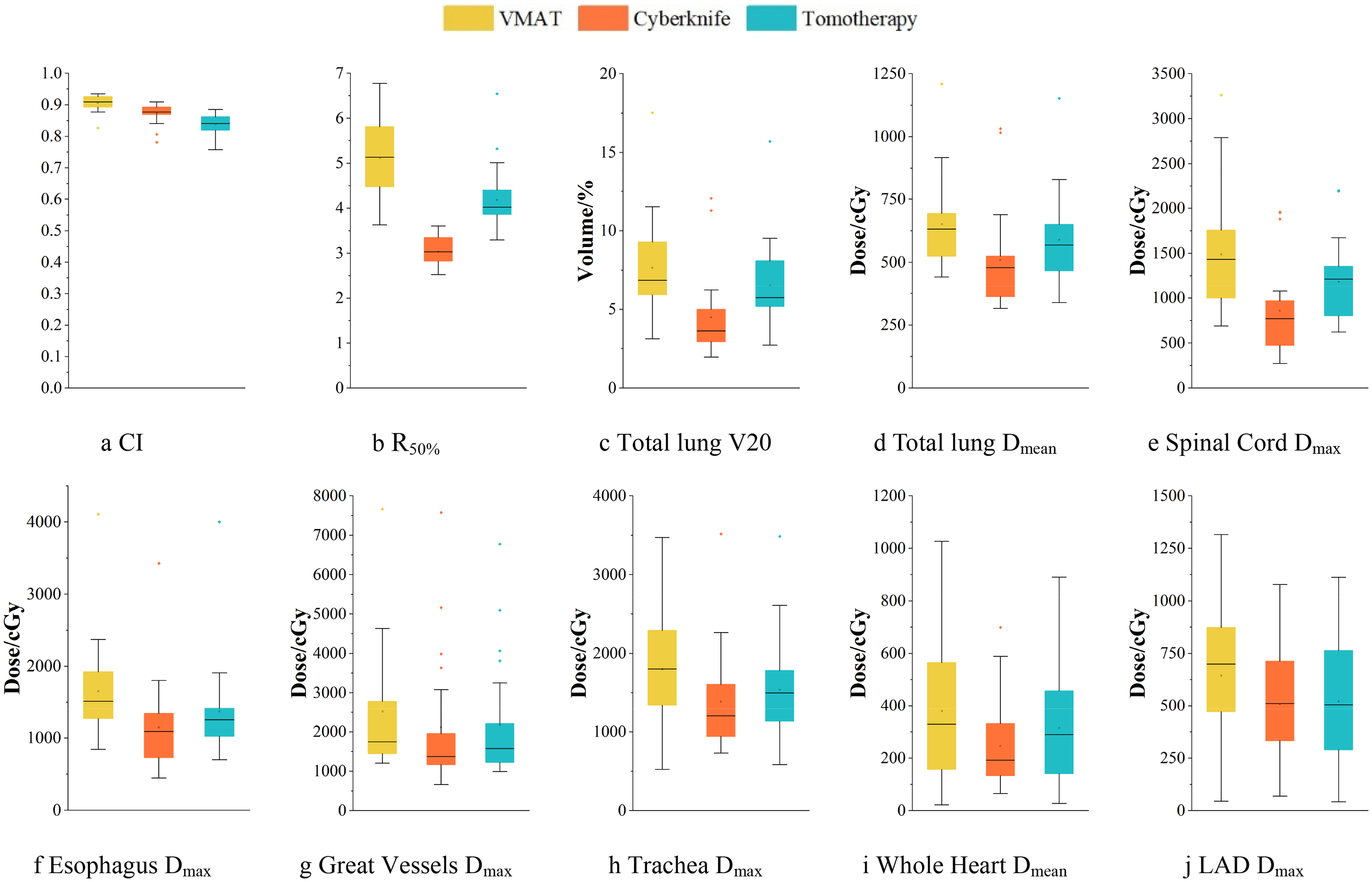
Comparison of major PTV and OARs dosimetric parameters among VMAT, CK, and HT plans.
For the whole lung, the V5, V10, V15, V20, V25, V30 and MLD of CK plans were better than those of VMAT plans and HT plans (p = 0.017 for V5 in CK vs HT, p < 0.001 for other comparisons). In addition, the lung dose metric of HT plans were better than those of VMAT plans (p = 0.011 for V30 in HT vs VMAT, p < 0.001 for other comparisons), which shown in Figure 2.
For serial OARs, the maximum doses of spinal cord, esophagus, trachea and great vessels in CK plans were significantly better than those in VMAT plans and HT plans (p = 0.002 for tracea in CK vs VMAT, p = 0.045 for trachea in CK vs HT, p < 0.001 for other comparisons, as shown in Figure 2), except that there was no significant difference between the great vessels maximum dose of CK plans and HT plans (p = 0.49). In addition, the maximum dose of HT plans in spinal cord, esophagus, trachea and great vessels was better than VMAT plans (p < 0.001 for all comparisons). The rib maximum dose of CK plans was better than that of VMAT plans and HT plans (p < 0.001 for CK vs VMAT, p = 0.002 for CK vs HT). The rib maximum dose of VMAT plans was higher than that of HT plans, but there was only a significant trend in the differences (p = 0.08).
For the heart and major cardiac substructures, there was no significant difference in all dose metrics between the CK plans and the HT plans, as shown in Figure 2. The average dose of the whole heart in the CK plans was better than that in the VMAT plans (p < 0.05). The maximum dose of the LAD, RV, LA and RA in the HT plans were better than those in the VMAT plans (p < 0.05 for all comparisons).
Biological Risk
As shown in Table 2, the expected RP risks for VMAT plans, CK plans, and HT plans were 6.69% ± 3.01%, 5.05% ± 2.81%, and 5.88% ± 2.73%, respectively. Compared to the CK and HT plans, the VMAT plans achieved the highest expected RP risk (p < 0.001 for both comparisons). The expected RP risk of CK plans was significantly lower than that of VMAT plans and HT plans (p < 0.001 for CK vs VMAT, p = 0.001 for CK vs HT)。
Expected Biological Risks of VMAT, CK, and HT Plans (mean ± SD).
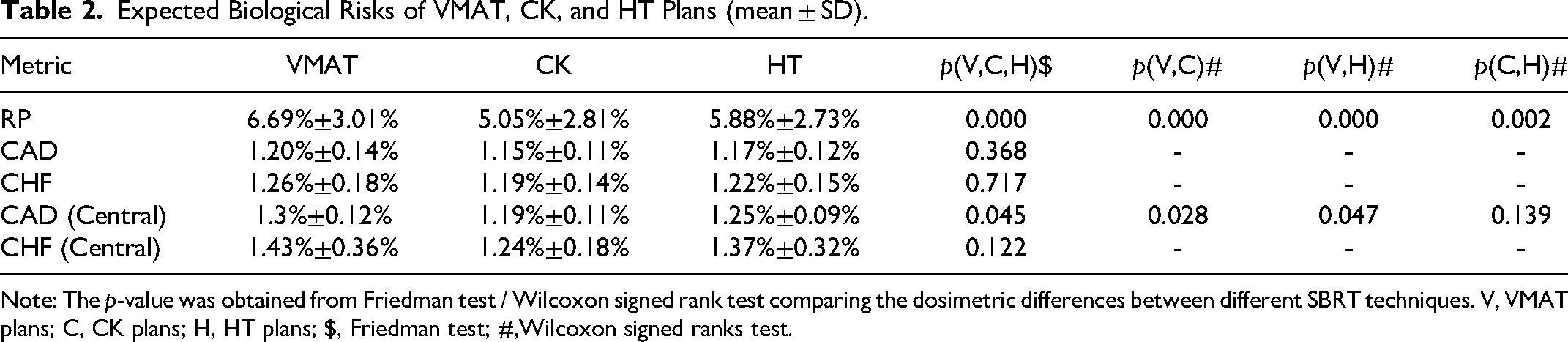
Note: The p-value was obtained from Friedman test / Wilcoxon signed rank test comparing the dosimetric differences between different SBRT techniques. V, VMAT plans; C, CK plans; H, HT plans; $, Friedman test; #,Wilcoxon signed ranks test.
The expected CAD risks for VMAT plans, CK plans, and HT plans were 1.20% ± 0.14%, 1.15% ± 0.11%, and 1.17% ± 0.12%, respectively. The expected CAD risk of CK plans was lower than that of VMAT plans and HT plans (shown in Figure 3), but there was no statistically significant difference (shown in Table 2). For central lung cancer, the expected CAD risks of CK and HT plans were lower than those of VMAT plans (p < 0.05 for both comparisons).

Comparison of expected biological risks among VMAT, CK, and HT plans.
The expected CHF risks for VMAT plans, CK plans, and HT plans are 1.26% ± 0.18%, 1.19% ± 0.14%, and 1.22% ± 0.15%, respectively. The expected CHF risk of CK was lower than that of VMAT plans and HT plans (shown in Figure 3), but there was no statistically significant difference (shown in Table 2), even in central lung cancer group.
Treatment Efficiency
As shown in Table 3, the MUs of VMAT plans were significantly lower than those of CK plans and HT plans (p < 0.001 for both comparisons). The beam-on-time of VMAT plans was significantly less than that of CK plans and HT plans (p < 0.001 for both comparisons). The beam-on-time of VMAT plans decreased by an average of 80.6% compared to CK plans and 88.3% compared to HT plans.
Treatment Efficiency of VMAT, CK, and HT Plans (mean ± SD).
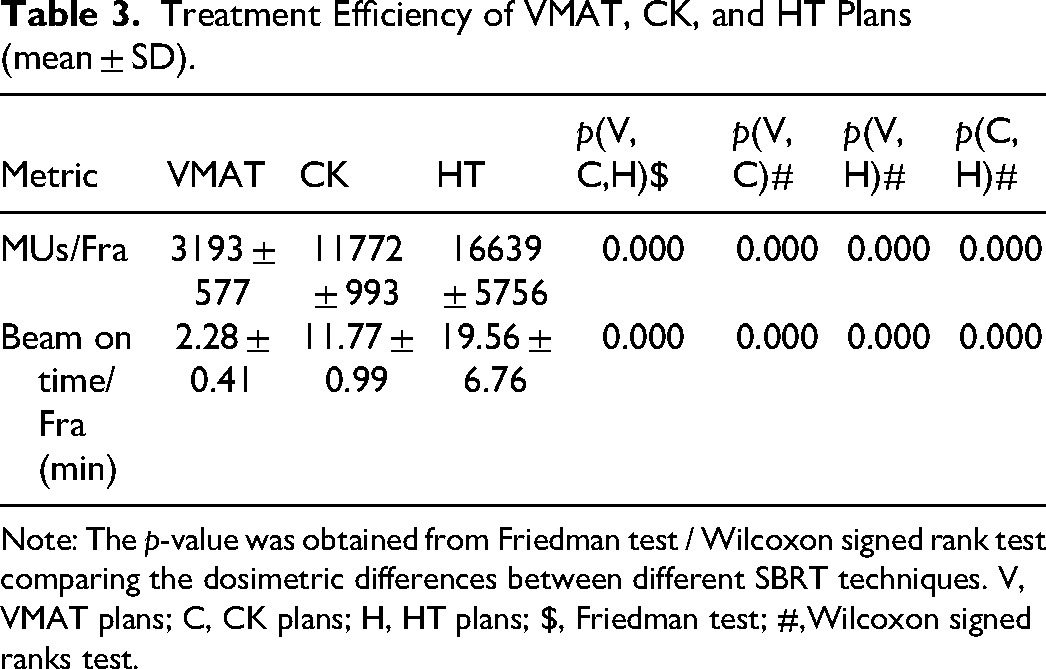
Note: The p-value was obtained from Friedman test / Wilcoxon signed rank test comparing the dosimetric differences between different SBRT techniques. V, VMAT plans; C, CK plans; H, HT plans; $, Friedman test; #,Wilcoxon signed ranks test.
Discussion
SBRT had gradually been widely used in the treatment of oligometastatic diseases. In this study, we presented the first direct comparison of three techniques — CK, HT, and VMAT — for the multiple lung metastases SBRT. Dosimetric parameters, expected biological risks, and delivery efficiency were employed for this systematic technique comparison. We found that all three techniques meet the dosimetric requirements outlined in the RTOG 0915. 29 For normal tissue protection, CK and HT had certain advantages in physical dose compared with VMAT, but the advantages in the expected biological risks were very small. Small differences in the expected biological risks might lead to less significant differences in clinical side effects.
All three techniques achieved similar target coverage, with the CI of the VMAT being slightly superior to that of the CK plans and HT plans. Notably, the CI of the VMAT plans was significantly better than that of the HT plans, which could be attributed to the finer MLC leaves of the linear accelerator (Edge: 32 pairs of 2.5 mm leaves in the center and 14 pairs of 5 mm leaves on the sides; Tomo Radixact: 64 leaves of 6.25 mm). The target coverage and conformity of the three technologies met the requirements of clinical guidelines, so their performance in local control was almost equivalent. Our results also indicated that the lung dose in CK plans was significantly lower than that in HT and VMAT plans. In this study, the VMAT plans utilized a single-isocenter technique. In our previous multi-target SBRT study, we observed that multi-isocenters plans resulted in a slightly lower MLD compared to single-isocenter plans (approximately 40 cGy). Obviously, the lung dose of multi-isocenters VMAT was still higher than that of CK plans. This might be due to the physical characteristics of CK with collimator in multiple directions, small source axis distance and non coplanar irradiation. As for other normal tissue, CK achieved lower doses compared to VMAT plans and HT plans, consistent with previous studies.12–17 Among them, Ding et al 12 found that CK may increase lung dose for posteriorly located tumors. There were fewer posteriorly located tumors in our cohort, and our dosimetric metrics were the average of all tumors in each patient, which might lead to different results. In addition, Yu et al 14 found that compared with CK, knowledge-based VMAT might produce equivalent or better dose distribution and produce more MUs than VMAT. In our study, we only compared VMAT and CK and did not include other advanced VMAT technologies. For the maximum dose to the spinal cord, esophagus, trachea, and ribs, CK plans were lower than HT plans. For great vessels, the whole heart, LAD, LV, and RV, CK and HT plans achieved similar dose distributions.
The expected risk of symptomatic RP for all three techniques was below 10%, with the CK plans exhibiting the lowest risk, approximately 86% of that of the HT plans and 75% of that of the VMAT plans. In published SBRT studies, total lung dose was widely recognized as an independent predictor of RP risk.30–32 Additionally, some studies have identified a correlation between unilateral lung dose and symptomatic RP, with Guckenberger et al 33 and Ong et al 34 noting that grade 2 or higher pneumonia is associated with the mean dose of the ipsilateral lung and the V5 of the contralateral lung respectively. Consequently, some research had employed both total lung and unilateral lung doses to estimate RP risk. 15 Given that some cases in our cohort had lesions in both lungs, we chose to use total lung volume parameters to estimate RP risk. We also found that CK and HT techniques provide better prevention of CAD and CHF in patients with central lung cancer compared to those with peripheral lung cancer, with CK demonstrating the most effective preventive results. Therefore, it seems better to use CK technology for SBRT in patients with ultra-central lung cancer or those with cardiac conditions that may not tolerate high doses (such as re-irradiation or pre-existing heart disease). Overall, there was no statistical difference in the expected biological risks among the three techniques. Even for central lung cancer, compared with VMAT, CK and VMAT might perform better in the expected risk of CAD. Although there are statistical differences, the numerical differences are small. Therefore, the three techniques might not show differences in the observation of clinical side effects, which might require further retrospective large cohort study or prospective research.
The delivery efficiency of single-isocenter VMAT was significantly superior to that of CK and HT, which was particularly beneficial for patients who pain or have difficulty lying still for extended periods. In comparison to previous studies, 15 the higher MU for HT in this study was attributed to our inclusion of more targets (≥2). In addition, the delivery efficiency in this study only considered the beam on time, while the delivery efficiency of CK also included the time spent on replacing the collimator and rotating multiple robot arms. For developing countries with a large population, economic benefits and treatment time were limited. Therefore, these clinics need to consider not only dosimetric and biological differences, but also treatment efficiency differences when selecting three radiotherapy techniques.
A limitation of this study was the lack of consideration for the differences in image-guided techniques across various platforms, such as the precision and robustness of these techniques. In this study, in order to more directly compare the differences among the CK, VMAT and HT, we chose the ITV method to make the CK plan. The M6 CK platform was equipped with a kV-X ray dynamic tumor tracking system, allowing for the use of smaller ITV margin or even no margin for SBRT/SRS. 35 Additionally, there may be differences in systematic errors between the MV helical computed tomography (CT) of HT and the kV Cone beam computed tomography (CBCT) of conventional accelerators. Another limitation was that our comparative study included differences between different technologies and TPS. We adopted different TPS equipped with CK and HT platforms to make plans. Different dose calculation algorithms might introduce “noise” to the results, especially in low-density tissues. In the future, we need to further compare in the same TPS to eliminate this “noise”. In addition, the sample size of patients in this study is relatively small, and further increase in sample size is needed in the future to reduce potential biases.
Conclusion
VMAT, Tomotherapy, and CyberKnife technologies can all meet the target treatment and OARs dose limit requirements for patients with oligometastatic lung disease. CK and HT protect normal tissues better in dosimetry and biology, and VMAT offers higher delivery efficiency. Although there are statistical differences, the difference between the expected risk values of RP and CAD is very small, so the clinical manifestations may not show differences. Therefore, it is recommended CK or HT for patients with low normal tissue tolerance, and VMAT for patients experiencing pain or difficulty lying down for extended periods.
Supplemental Material
sj-docx-1-tct-10.1177_15330338251330781 - Supplemental material for Comparative Dosimetry and Biological Risk Assessment of Lung Oligometastasis SBRT: VMAT, Helical Tomotherapy, and CyberKnife
Supplemental material, sj-docx-1-tct-10.1177_15330338251330781 for Comparative Dosimetry and Biological Risk Assessment of Lung Oligometastasis SBRT: VMAT, Helical Tomotherapy, and CyberKnife by Zhenjiong Shen, Mingyuan Pan, Lan Sun, Aihui Feng, Yanhua Duan, Hengle Gu, Yan Shao, Hua Chen, Hao Wang, Ying Huang and Zhiyong Xu in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Ethical Considerations
This study was approved by the Shanghai Chest Hospital Ethics Committee, Shanghai Jiao Tong University, Shanghai, China (Approval number: KS1863; Approval Date: August 29, 2018).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China [Grant/Award Numbers: 12375346], Shanghai Municipal Health Commission Health Industry Clinical Research Special Project [Grant/Award Numbers: 20244Y0035] and Research and Progress in Precision Radiotherapy for Cancer Research Project [Grant/Award Number: J202305E038A04].
Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.