
Abstract
Background:
Stereotactic body radiotherapy (SBRT) can emulate high dose rate brachytherapy (HDR-BRT) dose fractionation. We report our preliminary results using SBRT in monotherapy or pre-external-beam radiotherapy (EBRT) boost in patients with localized prostate cancer (LpC). The primary end point was the evaluation of both acute and late toxicities; secondary end point was the observation of prostate-specific antigen (PSA) nadir.
Patients and Methods:
Patients with LpC having prostate volume ≤90 cm3 were enrolled in the present study. Patients were treated with SBRT alone or in combined modality (SBRT + EBRT). SBRT was performed using a CyberKnife System (Accuray Incorporated, Sunnyvale, California) and fiducial tracking system.
Results:
From February 2008 to July 2013, 21 patients for monotherapy (38 Gy/4 fractions) and 5 for combined modality (9.5 Gy/2 fractions plus 46 Gy/23 fractions EBRT) were enrolled. Androgen deprivation therapy (ADT) was administered in 16 of the 26 patients. The median pretreatment PSA was 9.4 (range, 4.5-14.3) ng/mL. All patients completed the planned therapy. Acute Grade 1 toxicity was observed in 18 patients, genitourinary (GU) in 12 / 26 patients, and gastrointestinal (GI) in 6 / 26 patients. Acute Grade 2 GU toxicity was reported in 1 / 26 patients, and Grade 2 GI toxicity was observed in 2 / 26 patients. The median PSA nadir was 0.15 (range, 0.02 = 1.4) ng/mL. Late toxicities were observed in 5 / 26 patients: Grade 1 GU (3 of 26), Grade 2 GU (1 of 26), and Grade 1 GI (1 of 26). Median follow-up was 21.5 (range, 8-65) months.
Conclusions:
Our preliminary results of SBRT “simulating” HDR for LpC confirm a minimal toxicity and an optimal PSA response. The PSA nadirs appear comparable with HDR-BRT.
Introduction
Radiotherapy is an important treatment modality in the management of localized prostate cancer (LpC), but an optimal treatment regimen for LpC is yet to be determined. In recent years, the evidence for low a/ß value of the prostate cancer has changed the radiation approach in LpC. 1 -3 The use of large doses per fraction is the most efficient means of achieving dose escalation. Hypofractionation external-beam radiotherapy (EBRT) is a valid choice to treat LpC in terms of tumor control and toxicity. 4 -7 Until now, hypofractionation with high dose rate has been utilized by high dose rate brachytherapy (HDR-BRT), establishing itself as a viable and safe approach as monotherapy or boost after EBRT. 8 -15 The HDR-BRT has the advantage of better accuracy to the dose delivered and avoidance of complications secondary to organ movement compared to EBRT. In intermediate- and high-risk disease, HDR-BRT alone may not deliver adequate dose to periprostatic tissues. In this application, HDR-BRT may be used as a boost in combination with EBRT. 16,17 Using HDR-BRT boost with the EBRT may result in a substantial increase in biochemical relapse-free survival, reducing acute morbidity without an increase in late toxicity. 16 Data from a systematic review have emphasized the advantages of the combination of EBRT and HDR-BRT in terms of biochemical control and overall survival versus HDR-BRT or EBRT alone. 12 Data for LpC, published by Fuller et al, 18 suggest the validity of stereotactic body radiotherapy (SBRT) emulating dosimetry, dose, and fractionation of HDR-BRT. Another experience for LpC, 19 with SBRT as monotherapy and post-EBRT boost, has reported prostate-specific antigen (PSA) nadir comparable with HDR-BRT. The SBRT in our department is delivered using a CyberKnife system which permits to plan a heterogeneous dose distribution mimicking HDR-BRT’s target coverage; we used this system to treat LpC both in monotherapy and in pre-EBRT boost. The main purpose of this study is to evaluate feasibility, toxicity, and PSA outcome.
Patients and Methods
Patients with histologic diagnosis of prostate adenocarcinoma with Stage I-III, according to the VII edition of AJCC Manual for Staging of Cancer, 20 were considered to be eligible for this study. Thus, patients with LpC were eligible, but those with previous radiation therapy (RT), prostate surgery, or previous chemotherapy were excluded. Other requirements for eligibility were a Karnofsky Performance Status >70, a life expectancy >5 years, and a prostate volume ≤90 cm3, with absence of chronic inflammatory bowel diseases. The pretreatment evaluation included physical examination and complete blood count, anteroposterior and lateral chest X-ray, superior and inferior abdomen computed tomography (CT), and bone scan (in patients with a PSA value > 10 ng/mL). Other investigations were performed in presence of clinically suspected signs. Fully informed, written consent was required. One week before SBRT, 4 gold fiducials were placed in the prostate gland. The patient was positioned supine on the treatment couch and immobilized with a vacuum bag for SBRT treatment; for EBRT treatment, we used the Bellyboard Orfit prone immobilization system (PELVICAST™-Orfit® Industries America, New York) with pelvic custom-fitted thermoplastic cast. A Foley catheter was used in preplanning for urethral delineation and during the treatment to maintain the same urethral diameter and the same bladder volume of the simulation. For all patients, a multislice CT scanning (Siemens SOMATOM Sensation 16 - Siemens AG Medical Solutions, Germany) and magnetic resonance imaging (MRI; Siemens Magnetom 1.5-T - Siemens AG Medical Solutions, Germany) was performed. The CT protocol followed the CyberKnife-specific requirements, namely, acquisition 16 × 0.75 mm, Kv 120, effective mAs 320, rotation time 1 second, pitch 1.15, reconstruction slice 1.5 mm, reconstruction increment 1.5 mm, filter reconstruction H31 (smooth), and 512 × 512 matrix. The MRI was performed with the following parameters: matrix 512 × 512, flip angle 0°, effective thickness 0.88 mm, reconstruction slice 1.5 mm, and reconstruction increment 0 mm. The axial source images were transferred to the CyberKnife workstation for treatment planning (Multiplan® Treatment Planning System - Accuray Incorporated, Sunnyvale, California) for SBRT modality and to the Oncentra MasterPlan® (Nucletron BV, Veenendaal, the Netherlands) workstation for EBRT modality. The contouring of the tumor and critical volumes were defined with fusion MRI (T1 and T2 sequences) and CT imaging. For SBRT, the clinical tumor volume (CTV) included the prostate and proximal aspect of seminal vesicles (2 mm); the planning target volume (PTV) was obtained by an isotropic expansion of 2 mm for low-risk and 5 mm for intermediate- and high-risk prognoses in all directions except posteriorly where the prostate abutted the rectum. In this region, the margin expansion was reduced to 0 mm. The rectal mucosa was defined as a solid structure formed by a 3-mm contraction of the rectal wall. In EBRT modality, for high-risk patients, the CTV included the prostate, seminal vesicles, and lymph node areas (internal and external iliac, presacral, hypogastric, and obturator lymph nodes). The SBRT treatment planning was obtained with inverse planning algorithm using a nonisocentric technique. A heterogeneous dose distribution was generated to emulate HDR-BRT by observing the parameters proposed by Fuller et al. 18 For SBRT as monotherapy, a total dose of 38 Gy was delivered in 4 consecutive fractions (38 Gy/4 dd); for SBRT boost, the dose was 19 Gy in 2 fractions (19Gy/2 dd). The dose used for whole pelvic irradiation in 3D-conformal radiation therapy (3D-CRT) modality was 46 Gy in 23 fractions, 5 fractions per week. The SBRT dose was prescribed to 55% to 70% isodose line (Figure 1). The constraints of the maximum dose used were 37 Gy for rectum (D1-33 Gy), 30 Gy for rectal mucosa (D1-28 Gy), 39 Gy for urethra, 40 Gy for bladder, and 10 Gy for left and right femur head. In patients who performed 2 fractions, the maximum dose was halved. Three days before and for all days of treatment patients were prescribed diet free of slag; systemic cortisone was administered to all patients during treatment, and all patients were instructed to empty their rectum by self-administered enemas. In patients undergoing deprivation therapy, ADT was used as a scheme according to a long-term (2 years) or short-term (6 months) scheme through an anti-androgen and a luteinizing hormone (LHRH analogue). The prescription time limitation was made on the basis of risk classes. Patients were followed up every 3 months for PSA response, acute (within 12 weeks) or late (after 12 weeks). The peak toxicity was measured after 2 weeks posttreatment. Toxicities were recorded using common terminology criteria for adverse events v.3.

Stereotactic body radiotherapy (SBRT) treatment planning with inverse planning algorithm using a nonisocentric technique. The heterogeneous distribution dose was obtained to emulate high-dose-rate brachytherapy (HDR-BRT). In (a) and (b) an example of SBRT monotherapy plan (38 Gy in 4 fractions) is shown. In (c) and (d), a treatment plan of preboost (19 Gy in 2 fractions) 3D-conformal radiation therapy (46 Gy/23 fractions) is shown.
Statistical Analysis
Statistical analyses were performed using SAS version 9.2 (SAS Institute Inc, Cary, North Carolina) and SPSS version 20.0 (Chicago, Illinois). Exploratory analysis was carried out to determine the distribution of the demographic and clinical variables. Summary statistics, including mean (standard deviation) or median (interquartile range), as appropriate, were generated for continuous variables. Frequencies and percentages were determined for categorical variables. Patient characteristics across treatment groups were compared using chi-square test and Fisher exact test, as appropriate. Data normally distributed were compared using the student t test (two-group analyses) and the 1-way ANOVA (analysis of variance) with Bonferroni correction (multigroup analyses). Data not normally distributed were compared using the nonparametric Mann-Whitney U test (2-group analyses) and the Kruskal-Wallis test with Dunn correction (multigroup analyses). The linear relationship between continuous variables was evaluated using the Spearman correlation coefficient. To account for repeat measures, data were analyzed using the 2-way repeated measures ANOVA with Bonferroni correction. All hypothesis tests conducted were 2-tailed and a P value <.05 was considered significant.
Results
Description of Population
From February 2008 to July 2013, 26 patients with LpC were treated in SBRT modality using the CyberKnife System. Enrolled patients had a median age of 77 years (range, 62-89 years) and the median follow-up was 21.5 months, range 8 to 65 months (Table 1). Of the 26 patients with low or intermediate risk, 21 were treated with SBRT monotherapy using a total dose of 38 Gy (in our institution, patients with intermediate-risk cancers are not submitted to pelvic lymph node irradiation) and 5 patients were treated with preboost of 19 Gy in 2 fractions followed by 3D-CRT (46 Gy/23 fractions). One patient died 8 months after treatment due to unrelated cause. Of the 26 patients, 16 were treated with ADT; long-term ADT was used in 7 (58.3%) of the 12 intermediate-risk patients and 5 (100%) of the 5 high-risk patients. Short-term ADT was administered to 4 (33.3%) of the 12 intermediate-risk patients. The median initial PSA in all patients was 9.24 ng/mL (range, 4.4-20 ng/mL), 6.7 ng/mL (range, 4.36-9.95 ng/mL) in the monotherapy group with low risk, 11.7 ng/mL (range, 6.1-14.3 ng/mL) in the monotherapy group with intermediate risk, and finally 15.2 ng/mL (range, 6.8-20 ng/mL) in the high-risk group (preboost SBRT+3D-CRT).
Patients and Treatment Parameters.

Abbreviations: ADT, androgen deprivation therapy; pre-EBRT, pre-external-beam radiotherapy; PSA, prostate-specific antigen; SBRT, stereotactic body radiotherapy; GS, gleason sum.
Analysis of Acute and Late Toxicity
The SBRT monotherapy or boost for newly diagnosed LpC was well tolerated. Among patients studied, 57.69% developed complications and 46.67% of those had an acute adverse event. Most (60%) patients had a single low-grade complication. The incidence of late toxicity was not statistically different between patients treated with preboost SBRT+3D-CRT and those treated with monotherapy. However, patients treated with monotherapy had higher incidence of late toxicity (P = .026). Frequencies and percentages of specific complications are presented in Table 2. Late toxicity was observed in 5 (19%) of the 26 patients: grade 1 genitourinary (GU; 3 of 26, 11%), grade 2 GU (1 of 26, 4%), and grade 1 gastrointestinal (GI; 1 of 26, 4%; Table 2).
GU and GI Toxicity in Patients Treated with SBRT Monotherapy or Boost pre-EBRT (Common Terminology Criteria For Adverse Events v.3).a

Abbreviations: GI, gastrointestinal; GU, genitourinary; pre-EBRT, pre-external-beam radiotherapy; SBRT, stereotactic body radiotherapy.
a Data are n (%).
b Patients can develop more than 1 complication.
There was a significant difference in age between patients with and without complications (P = .0009), with patients who developed a complication tending to be younger than patients who did not experience toxicity (median 74 vs 80 years Figure 2). Toxicity was not associated with hormonal therapy, prescription, or prostate volume, although a trend toward increased number of complications in patients with larger prostate volume was seen (Figure 3). Patients with G2 late toxicity (dysuria) were treated with adrenergic-blocking agents.
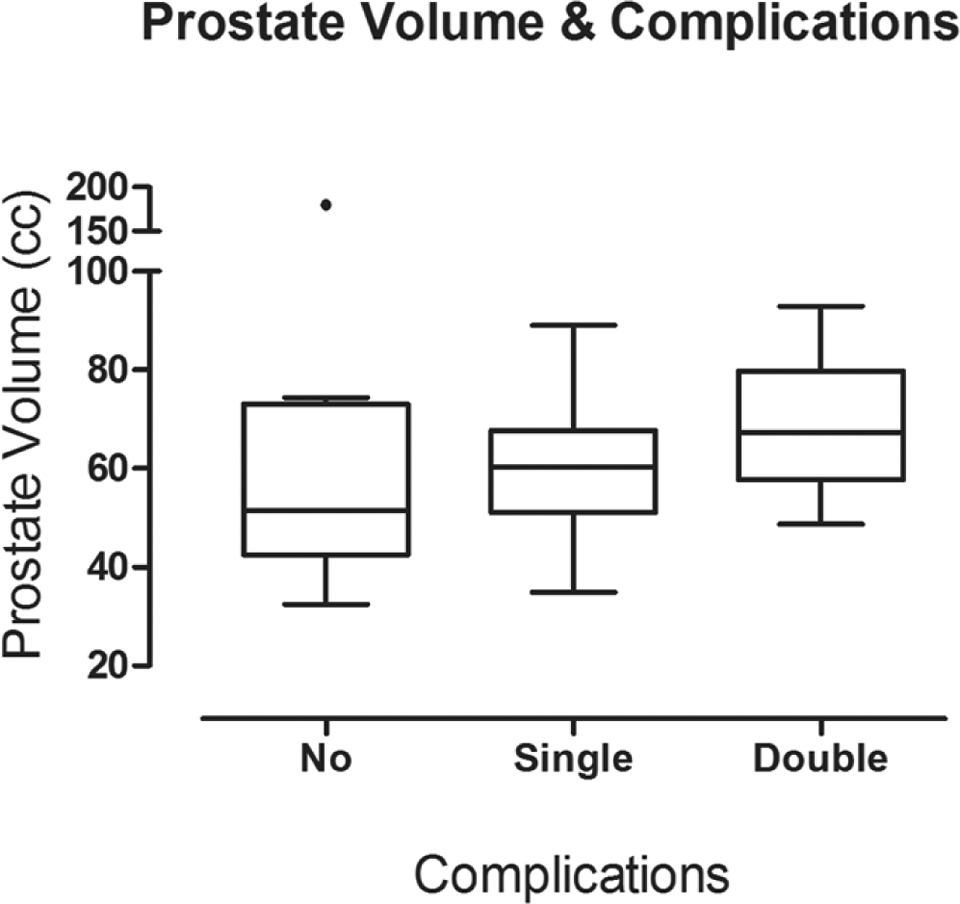
Prostate volume in patients with 1 (GU or GI) or 2 complications (GU and GI), and in patients without complications. GU indicates genitourinary; GI, gastrointestinal.
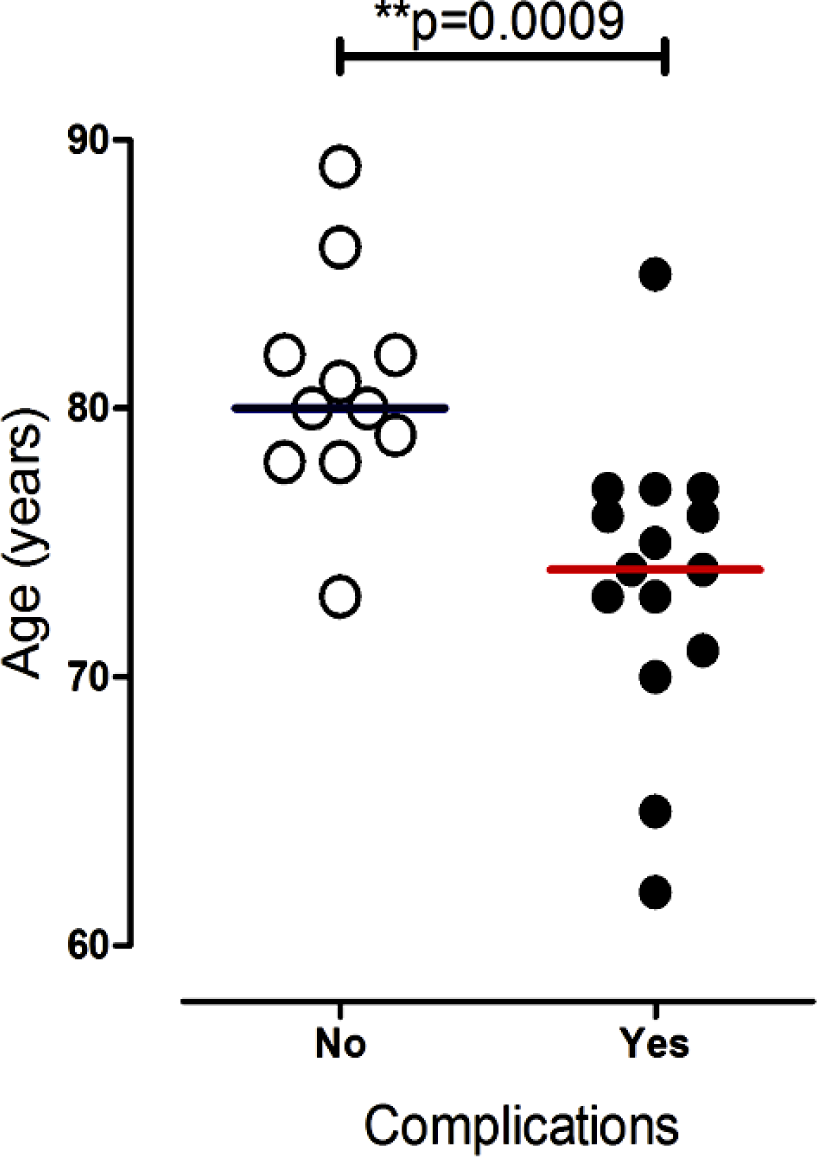
Dot plot demonstrating age in patients with and without complication.
Analysis of PSA Nadir
The treatment response was assessed by the value of PSA nadir after ADT treatment. The median nadir PSA value achieved was 0.21 ng/mL (range: 0.03-6.6 ng/mL). In the group treated with monotherapy for low-risk disease (median follow-up 28 months, range: 8-65 months), a PSA nadir of 0.11 (range: 0.03-2.3) was obtained. The monotherapy group with intermediate risk (median follow-up 29.5 months, range: 8-62 months) achieved a median PSA nadir of 0.19 ng/mL (range: 0.03-6.6 ng/mL). Finally, in the high-risk group (median follow-up 15 months, range: 8-17 months), a median PSA nadir of 0.7 ng/mL (range: 0.2-5.98 ng/mL) was reached. At latest follow-up, we had no evidence of rising PSA in 92% (24 of 26) of patients (Figures 4 and 5). An increased PSA value occurred in 1 patient treated with preboost SBRT+3D-CRT and in 1 patient treated with monotherapy and short-term ADT for 6 months.

Prostate-specific antigen profile in patients with and without added androgen suppression treatment.

Temporal prostate-specific antigen profile in patients treated with Cyberknife stereotactic body radiotherapy.
Discussion
The dose/fractionation scheme that was used in our study had been tested in a phase I/II HDR-BRT dose escalation study, 13,19 and optimal clinical outcomes were reported in an RTOG Phase II trial. 8,13 -15,19 It was our choice to treat the boost before EBRT for the following reasons; first at the start of SBRT, patients were naive from acute toxicities linked to EBRT; second at the start of the EBRT, prostate cancer cells were exposed at high radiation dose (BED2 109.25 Gy). Up to date, there is no larger studies on HDR-like prostate cancer treatment. Only Jabbari et al 19 report their experience on 20 patients with 18.3 months median follow-up. Larger data are reported using 5 fractions and total dose ranging from 35 to 50 Gy. In our patients, we delivered radiation using a heterogeneous dose distribution mimicking HDR-BRT’s target coverage and organ at risk (OAR) sparing (eg, bladder, rectum, penile bulb, etc). This heterogeneous SBRT planning permits to spare the intratarget OAR urethra; with a prescription dose between 55% and 75%, it allows to deliver higher doses to some regions within the target with higher heterogeneities (up to 45%) compared to modern HDR-BRT. The Cyberknife System permits to deliver this kind of dose distribution in different anatomic sites. 21 Patients treated in this study with SBRT for LpC with a minimum follow-up of 8 months present an optimal response in terms of PSA response (see Figures 4 and 5) with a median PSA nadir of 0.11 ng/mL. Although a longer follow-up is needed to confirm the results of SBRT in monotherapy or preboost modality for LpC, the data are encouraging and confirm the results obtained with HDR. 22,23 In another study, 19 a cohort of 38 patients with LpC, including 20 treated with SBRT monotherapy (38 Gy/4 fractions) and 18 with a post-EBRT boost (19 Gy/2 Fx) were described. The data observed were comparable to ours both in terms of toxicity and in terms of PSA control. However, among our 26 patients, PSA increase was observed in 2 patients. In 1 patient with high-risk disease, the rise corresponded to a pelvic and lumbar aortic lymph node metastasis, while in an intermediate-risk patient, the rise was due to a PSA bounce, which receded 6 months after the treatment. The question of PSA bounce with high-dose regimens is particularly interesting because benign rises in PSA may lead to unnecessary intervention. 24 This phenomenon has been examined in patients treated with BRT alone or BRT in combination with EBRT, EBRT alone, and SBRT. 25 -29 Recently, Caloglu and Ciezki 26 investigated various PSA bounce cutoff values in 820 patients who received I-125 BRT. By defining PSA bounce as a rise of 0.4 ng/mL with a subsequent return to nadir, 19.6% of patients experienced a bounce at a median of 16.3 months. A study with 975 patients has shown that the patients who have experienced a bounce have improved overall survival. 30 In our study, 16 patients were treated with ADT. It is unclear whether the use of ADT in intermediate- and high-risk patients who undergo BRT ± EBRT improves biochemical disease-free survival. No phase III trials evaluating the role of ADT in patients with locally advanced prostate cancer treated with EBRT and a BRT boost has been reported to date, although 2 trials are ongoing. 31 At 8 years, the addition of a course of ≤6 months of neoadjuvant/concurrent ADT to a very high radiation dose did not confer a therapeutic advantage but added side effects and cost. 32 Benefits of ADT in the setting of dose-escalated RT remain poorly defined. 33 Although our data show a low incidence of acute and late grade 2 to 3 toxicities, the data of the trials published on SBRT LpC have shown late grade 3 GI and GU toxicities within the 1% to 3% range. 18,25,34 -36 An exception was 1 SBRT trial 29 delivering 50 Gy in 5 fractions: In this study, 7% grade 3 GI and GU late toxicities were observed. Our data, of late toxicity, are, respectively, 1% for grade 2 GI toxicity and 4% for grade 2 GU toxicity. Longer follow-up for PSA control is needed before any definitive assessment of our data.
Conclusions
Our data on SBRT emulating HDR dose/fractionation for monotherapy or pre-EBRT boost for LpC confirm feasibility in a heterogeneous cohort of patients with prostate cancer having optimal PSA control and low acute and late toxicity. The SBRT appears to be an attractive option, although further long-term data and larger patient numbers are necessary; besides, the role of ADT used in our patients (16 of 26) with high-dose regimen remain poorly defined. Only 5 patients were treated with SBRT+EBRT, and then this is a very small number of patients to draw conclusions in terms of toxicity and PSA response. The extensive experience and practice of HDR-BRT support the use of SBRT dosimetry with added MRI-guided target volume delineation and intrafraction prostate motion tracking with real-time beam adjustment.
Footnotes
Abbreviations
Authors’ Note
All the authors contributed equally.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.