
Abstract
Non-subungual glomus tumor in the fingers is very rare. To explore the insights gained from diagnosing and treating non-subungual glomus tumors in the finger, we collected 19 cases in the last ten years, which were only reported as isolated cases in the previous literature. This was a retrospective study of 19 surgical patients between May 2012 and January 2022 with preoperative MRI, ultrasound, and their final pathological diagnosis is glomus tumor, while the lesions were located not under the nail bed. Immunohistochemistry indicated that SMA(+)100%, CD34(+)89.5%, Ki-67(+1∼3%)68.4%, CD31(vessel+)26.3%, Desmin(+)21%, Calponin(+) 10.5%, Vimentin(+)5.2%, Caldesmon(+)5.2%. The sensitivity of preoperative MRI was 100%, while the sensitivity of ultrasound was 63.2%. And the diagnosing accuracy rate of preoperative MRI was 36.8%. Preoperative MRI is helpful in the diagnosis of non-subungual glomus tumor in fingers. Ultrasound can be used as a supplemental examination technique, and the results depend on the operator and tumor location. Surgical excision is an effective therapy for non-subungual GT in the fingers.
Introduction
Glomus tumor (GT) usually occurs under the fingernail or toenail, so this type of GT is called subungual GT. Patients with GT usually present with characteristic clinical symptoms, such as pink or purple vascular papules or nodules, paroxysmal pain especially when the lesion is under the nail, cold sensitivity, and localized tenderness. 1 In most cases, the diagnosis of GT is usually made in a clinical setting, and the radiological examinations and clinical tests help with the localization of GTs. Still, a biopsy of the excised tumor tissue sample is necessary for confirming the diagnosis. However, since the hardness and thickness of the nail, as while as the abundant sensory nerve endings at the fingertips, GT in or around the nail unit cannot be ascertained simply by ocular inspection or palpation, and misdiagnosis sometimes occurred. Another phenomenon sometimes encountered is that no GT is found after removing the nail plate, this kind of occurrence may lead to an unnecessary deformation of the nail plate. Meanwhile, even if the clinical diagnosis of a subungual GT is correct, conducting a surgical operation without exact knowledge of the site and size of the tumor may result in incomplete excision, thereby leading to recurrence. It is because of these above-mentioned reasons that when it comes to GTs, it's not just enough to arrive at the right diagnosis, but it's also essential to pinpoint the exact location and accurately estimate the size of the tumor preoperatively.
Meanwhile, GT can also occur elsewhere, in the palm, wrist, arm/legs, and trunk, so this type of GT is collectively called non-subungual GT. Due to the extremely low incidence of non-subungual glomus tumors and their nonspecific symptoms, they are easily overlooked during clinical physical examinations, presenting significant challenges for their clinical diagnosis. 2 Therefore, enhancing clinicians’ ability to accurately diagnose and treat non-subungual GT is crucial for improving patients’ quality of life. A practical approach to resolving this challenge is by utilizing imaging modalities. However, apart from scattered case reports, there are currently no systematic studies on the use of preoperative Magnetic Resonance Imaging (MRI) and ultrasound for diagnosing non-subungual GT. We analyzed non-subungual GT in the fingers with preoperative MRI and ultrasound in our hospital, the significance of the clinical application of MRI and ultrasound was discussed. Surgical treatment and outcomes were also discussed.
Methods
This was a retrospective study with patients presenting as pain in fingertip between May 2012 and January 2022. The recruiting criteria: Patients who underwent preoperative MRI and ultrasound, and were all confirmed by pathology to have GT located in the non-subungual parts of the fingers. The same outpatient doctor noted the clinical diagnosis of GT and the location of stabbing pain before the exam of MRI. The machine we used was Philips Achieva 1.5 T (Netherlands). Contrast-enhanced MRI was contributory to diagnose GT before the operation (Figure 1 and 2). Ultrasound is operated by different outpatient doctors (Figure 3). All surgeries were performed by the same surgeon. Under general or nerve block anesthesia, incisions were planned preoperatively based on ultrasound and MRI localization. A brachial tourniquet was used, and the procedure was carried out with surgical loupes (Figure 4). The tumors were completely excised and subjected to pathological examination and immunohistochemical analysis. Postoperative histologic findings were GT in all cases.

The image showed a 35 years old female with pinpoint pain in her medial little finger pulp, no lesions can be touch.

(A) T1-weighted MRI image shows hypo-intense signal; (B) T2-weighted MRI image shows hyper-intense signal (C) contrast enhanced MRI shows the images increased significantly.

Ultrasound shows low echo nodules.

This image shows complete resection of lesion was achieved in operation.
All patient follow-ups were conducted by the medical staff at the outpatient clinic where the authors of this study are based. Written informed consent for publication of patients’ clinical details and clinical images were obtained from the patients. The patient data used in the article does not reveal any patient privacy. Authors didn’t have access to information that could identify individual participants during or after data collection and conducted this study from June 2022 to December 2022.
Statistical Analyses
Statistical analysis was performed using SPSS 18.0 for Windows (SPSS Inc., Chicago, IL, USA). For the comparison of the maximum tumor diameter under imaging and under gross observation, matched t-test was performed. The differences were considered statistically significant at P < .05.
Results
There was a total of 153 patients with GTs in ten years, among them 19 patients with non-subungual GT were included in this study (Table 1). This series was all female patients with an average age of 39.16 years, ranging from 23 to 66 years. Seven of 19 patients were involved in the middle finger, seven involved the thumb, three involved in the little finger, and two involved in the ring finger. Meanwhile, the non-subungual GT of 17 cases were in the finger pulp and two cases were near by the phalangette.
Patient Data.
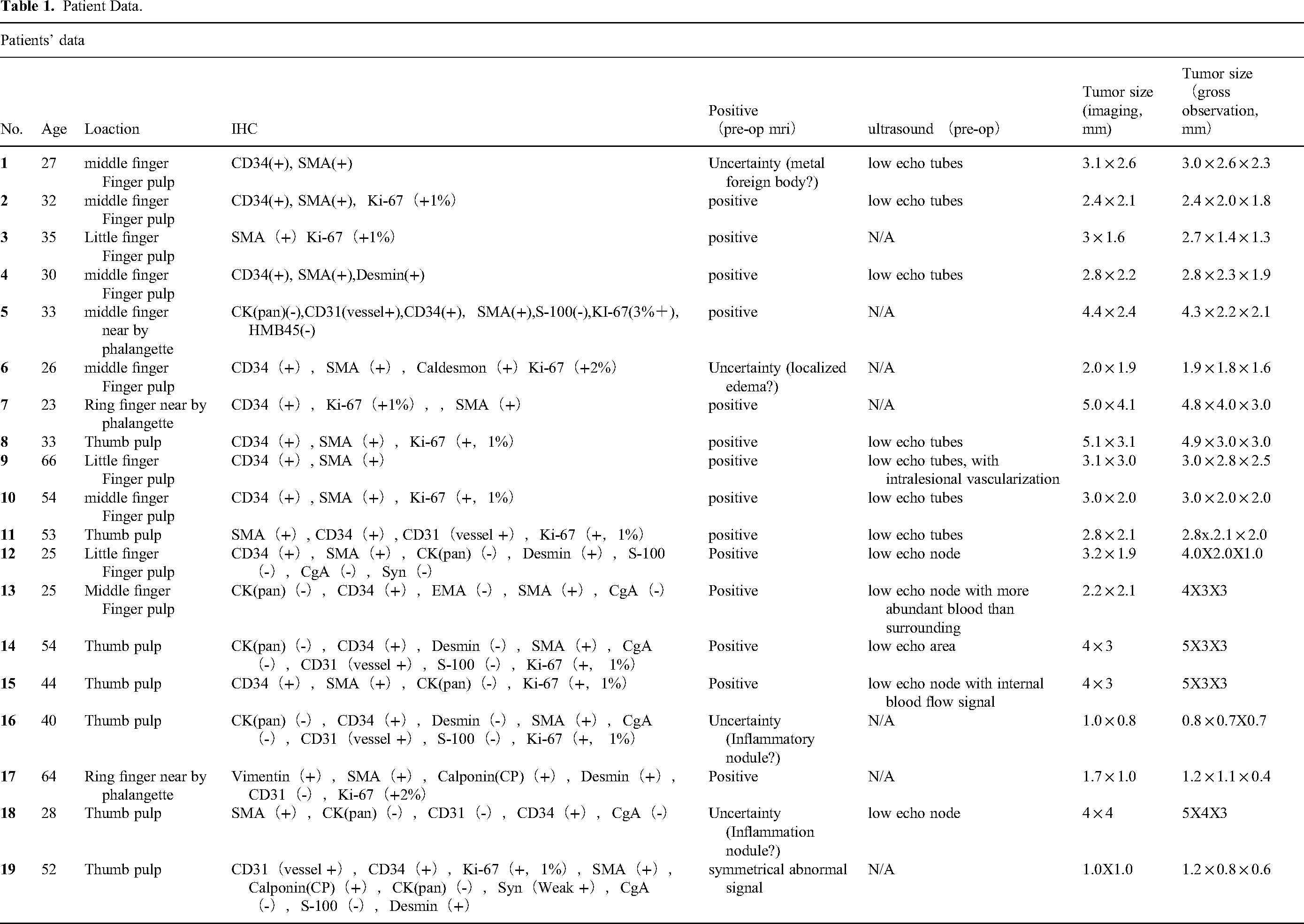
MRI demonstrated the maximum diameter of the lesions were from 1.0 mm-5.1 mm with the average of 4.37 mm. In pre-operation MRI, seven patients were reported GT. One was reported metal foreign body and nine were reported localized edema. The sensitivity was 100%, and the accuracy rate was 36.8%. In pre-operation ultrasound, 12 patients were reported low echo nodules. The sensitivity of ultrasound was 63.2%. Immunohistochemistry indicated that SMA(+)100%, CD34(+)89.5%, Ki-67(+1∼3%)68.4%, CD31(vessel+)26.3%, Desmin (+)21%, Calponin(+)10.5%, Vimentin(+)5.2%, Caldesmon(+)5.2%. Grossly, the maximum diameter of the lesions was from 0.8 mm-5.0 mm, and the average diameter was 3.25 mm. Based on the maximum tumor diameter of tumor sizes under gross observation, the mean absolute percentage error of maximum tumor diameter was 12.7%. The results of the paired sample t-test indicate that there is no significant difference between the maximum tumor diameter under imaging and under gross observation.
None of the patients developed postoperative infections. All the wounds were primary healing, and no painful scar was experienced. All patients were treated with 200 milligrams of Celebrex (celecoxib, 200 mg bid, Pfizer Manufacturing Deutschland GmbH), twice a day for one week after surgery. 16 patients relieved the pain symptom after the operation. But, the improvement of three patients was not obvious, they were treated with Lyrica (pregabalin,150 mg bid, Pfizer Manufacturing Deutschland GmbH) for one month, then the patients gained a functional recovery. Postoperative follow-up indicated no tumor recurrence within one year for all patients.
Discussion
Accurate diagnosis and preoperative localization of the tumor's position and size for non-subungual GT are crucial, and the use of imaging modalities is highly beneficial in this regard. A wide variety of imaging modalities can be utilized to detect GT, including x-rays, ultrasound, CT and MRI. The plain radiograph usually shows erosion or thinning of the underlying bones, especially when the tumors are sizeable. But this finding is not ubiquitous and is only noted in 30% to 60% of cases. 3 Ultrasonography can be exploited to observe GT but has a limited value in this endeavor. This imaging technology is quite subjective and the imaging findings are more dependent on the expertise of the sonologist owing to the small size of these kinds of tumors. MRI is the most useful imaging modality for preoperative localization of GTs and can be used to help diagnose when a GT is suspected. GT on MRI appears hypointense on T1 and hyperintense on T2 images, and most glomus tumors had a strong enhancement after injection of contrast agents such as gadolinium. 4 Furthermore, it can distinguish tumors from normal tissue with high accuracy. Concerning the diagnosis of GT, MRI reaches very high sensitivity and an equally high positive predictive value, which are 90%, and 97% respectively. 5
But the value of preoperative MRI in diagnosing GT in the fingers is controversial. Ham et al indicated that only high-resolution MRI can tell the details of GT, 6 the standard MRI achieves the diagnostic value, as MRI with high-resolution can distinguish tumors as small as 2 millimeters in diameter. 7 In our study, the minimum size of non-subungual GT was 2.0 × 1.9 mm in the pulp of the middle finger measured by MRI, but this report of MRI was uncertain due to its consideration of the lesion as localized edema. Intraoperatively, the real size of the lesion was 1.9 × 1.8 × 1.6 mm, closely to the diameter measured by MRI, which proved that the MRI was clinically practicable in our case series for non-subungual GT. None of the multiple lesions was diagnosed in our case series. But to Al-Qattan et al, 5 the specificity of MR imaging was low, with a specificity of 50%, a negative predictive value of 20%, and false negative images may also occur frequently. They think the diagnosis of typical GT can be made by clinical history and physical examination.
However, dark bluish discoloration or nail ridges are typically not observed in non-subungual GT. 8 Compared with classic GT, it is more difficult to diagnose non-subungual GT. The X-ray may present bone erosion of the subadjacent distal tuft of the finger. But none of the bone erosion was found in our case series. The color Doppler is particularly used in the diagnosis of non-subungual GT, 1 mm lesions were also identified. 9 But the quality of the instrument and the doctors’ skill is important. Even though we marked the location of pinpoint pain before the exam of Ultrasonography in our department, to help ultrasound doctors better position. In our group of cases, the sensitivity of ultrasound diagnosis was lower than that of MRI. For instance, in two patients in our study, hypoechoic nodules 3 × 4 mm in size were detected on ultrasound, but the blood flow signal within the lesions was not significant on color Doppler, thus ultimately, ultrasound only reported hypoechoic nodules in the fatty layer of the fingers. These two cases, in turn, were considered as GT on MRI. We consider the following issues that may have contributed to this result: First, the rareness of the disease itself, the operating doctor was not familiar with the disease; Second, the tumor was close to the phalanx, and the high echo affects the diagnosis; Last, the results of ultrasound vary widely among different doctors. In our hospital, some patients had numerous visits to different hospitals in the past, with multiple different diagnoses including neuroma, neuritis, Raynaud's disease, and menopausal syndrome. And some radiologists reported a typical GT patient by MR as “foreign body”. We think there may be differences in GT knowledge among hand surgery, orthopedics, general surgery surgeons, and radiologist. So, education should be strengthened to improve clinical medical staff medical professional knowledge. We encountered patients whose non-subungual GT ruptured ultimately due to misdiagnosis. 10 If pre-operation MRI could confirm the diagnosis, it is beneficial for doctor-patient communication, especially in China.
Coming to treatment modalities, surgical excision is not only the best mode of treatment but currently, but also the only effective method for treating this condition. MRI can be a helpful tool to decide surgical approach. 11 The surgical excision of GTs is generally completed under local anesthesia with or without sedation. Small (<5 mm), GTs of the fingers typically possess a pseudo capsule, which makes the excision relatively easy. GTs often lead to shallow erosions or cystic changes of the underlying bone, and therefore require bony curettage to reduce the risk of recurrence. 12 Initial recurrence may happen within weeks or months after the surgical procedure and recurrence usually indicate that the excision was incomplete. 13 Sometimes, recurrence may be seen after longer durations of time, ie, a few years after surgery, this phenomenon is presumably the result of the development of a new tumor. 12
In our case series, we do the minimally invasive incision according to MRI and to accurately localize the GTs. The endothelial suture was used for reducing the scars. None of the patients had the complication of a painful scar. The combination of pre-operation imaging and complete resection in surgery is performed to reduce tumor recurrence. The reports and images of pre-operation MRI were well agreed with the tumor's location and size observed during surgery. Pre-operation MRI is quite helpful for initial imaging, primarily to rule out felon or other soft tissue tumors in the distal finger.14–17 Although the overall study sample size is small, it is already the longest and largest follow-up study. It is hoped that multi-center and prospective research will be carried out in the future.
Due to the extremely low incidence of non-subungual GT, our study was unable to collect a sufficient number of contemporaneous samples and establish a control group for a cohort study, necessitating a descriptive retrospective study instead. Additionally, to provide high-quality medical care, clinicians require comprehensive imaging information to aid in diagnosis and surgical treatment, resulting in all samples undergoing imaging examinations and the absence of a control group. Nevertheless, compared to previous studies on non-subungual GT, which were predominantly isolated case reports, our study holds significant reference value.
Conclusion
Our study, featuring the largest sample of patients with rare non-subungual GT in China, is the first systematic investigation in the country to explore the use of MRI and ultrasound for the diagnosis and treatment of non-subungual GT. We found that MRI and ultrasound are highly beneficial for the accurate diagnosis and preoperative localization of the tumor's position and size.
Footnotes
Level of Evidence: Level IV
Acknowledgements
This work was supported by Alibaba Cloud.
Authors’ Contributions
Hui Lu designed the study, Haoyu Wang, Jiahang Han, and Haiying Zhou performed the data collection, Haoyu Wan, Zewei Wang and AHMAD ALHASKAWI performed the analysis, Haoyu Wang and Yanzhao, Dong drafted the manuscript. All authors read and approved the final manuscript.
Availability of Data and Materials Section
The dataset supporting the conclusions of this article is included within the article.
Consent for Publication
Written informed consent for publication of clinical details and clinical images was obtained from patients. Upon request, copies of the consent form are available for review by the Editor of this journal.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zhejiang Provincial Natural Science Foundation of China, Alibaba Youth Studio Project, (grant number LS21H060001, ZJU-032).
Ethics Approval and Consent to Participate
Written informed consent for publication of clinical details and clinical images was obtained from patients. This research had been approved by the medical ethics committee of the First Affiliated Hospital, College of Medicine, Zhejiang University (IRB NO.2021224).