
Abstract
Introduction
Adult females with International Federation of Gynecology and Obstetrics (FIGO) stage IIIC endometrial cancer are a heterogeneous group, accounting for 8-10% of all diagnosed cases. The FIGO 2009 staging system stratifies stage IIIC into IIIC1 (pelvic lymph node metastasis) and IIIC2 (para-aortic lymph node metastasis). 1 The prognosis of these patients is considerably worse than that of those with early stage disease.
Most patients with stage IIIC endometrial cancer are treated with a combination of chemotherapy and radiotherapy.2,3 Recent trials have sequenced radiotherapy with concurrent doxorubicin/cisplatin followed by combination chemotherapy for advanced endometrial cancer.4,5 An analysis of the adjuvant chemoradiotherapy versus radiotherapy alone in women with high-risk endometrial cancer (PORTEC-3) trial reported improved progression-free survival (PFS) and overall survival (OS) with the addition of chemotherapy during and after radiation compared with pelvic radiation therapy alone in those with stage III disease. 6 Interestingly, in an update of the GOG-258 trial, which recruited patients with stage I-II serous/clear cell and stage III-IVA endometrial cancer, the addition of external beam radiation therapy (EBRT) to chemotherapy was not associated with recurrence-free survival (RFS) and OS benefit. 4
Another important question is whether it is reasonable to recommend chemotherapy alone without pelvic ± extended-field radiotherapy in stage IIIC patients with favorable histological subtypes. Many prospective and retrospective analyses have combined multiple histologies, including patients with stage IIIA, IIIB, or IV disease, and mounting data suggest that there are prognostic, epidemiological, and genomic differences among the histological subtypes. 7
However, the optimal adjuvant therapy for adult females with stage IIIC endometrial cancer remains controversial. To date, no trial has directly compared adjuvant radiation plus chemotherapy in stage IIIC patients based on histology. As such, the present study analyzed data from the Surveillance, Epidemiology, and End Results (SEER) database to determine whether adjuvant radiation plus chemotherapy is associated with improved survival in adult females with stage IIIC endometrial cancer. Additionally, we sought to identify the preferred adjuvant therapy for different subgroups stratified according to histology, stage, and grade.
Materials and Methods
Data Source and Study Population
A retrospective cohort study was performed using the linked SEER registries, which cover approximately 34.6% of the United States population and contain approximately 97% of all incident cancer cases. Patients were identified using the International Classification of Diseases (ICD) O-3 primary tumor site codes (endometrium, C54.1) between 2010 and 2015. Histological types included in the analysis were endometrioid (8140, 8210, 8211, 8260-8263, 8380-8383, 8441, 8460, 8461, 8480, 8481, 8482, 8560, 8570), serous (8441, 8460, 8461), clear cell (8310, 8313), and carcinosarcoma (8950, 8951, 8980, 8981, 8982), according to ICD-O-3 morphological codes.
Given the retrospective design of the study and the use of anonymized data, requirements for informed consent were waived.
Study Variables and Outcomes
Study variables obtained directly from the SEER registry included age at diagnosis, race, histological type, tumor size, tumor grade, marital status, stage, year of diagnosis, and peritoneal cytology. Tumor grades were defined as I (well-differentiated), II (moderately differentiated), and III/IV (poorly differentiated or undifferentiated). A grade subtype variable was created using the following categories: low-grade (I and II endometrioid) and high-grade (III or IV endometrioid). For survival analyses, information regarding vital status records (study cut-off used) and survival months was collected. Adjuvant treatments included chemotherapy and radiation recovery. Radiation recodes include EBRT, vaginal brachytherapy (VBT), and a combination of beams and implants. Adjuvant therapy was further categorized as CT alone, CT+EBRT, CT+VBT, or CT+EBRT+VBT. The primary study outcome was OS, which was calculated as the time interval between the date of endometrial cancer diagnosis and the date of death from any cause or among adult females alive at the end of follow-up.
Statistical Analysis
First, the frequency distributions of demographics, treatment type, and clinical variables in the overall study population were examined using histology. Continuous variables are expressed as median with interquartile range (IQR). Descriptive analyses were performed using the chi-squared test for categorical variables and the Kruskal–Wallis test or one-way analysis of variance (ANOVA) test for continuous variables. Kaplan–Meier curves and log-rank tests were used to compare survival distributions according to treatment type in the overall study population and subgroups stratified according to histology (endometrioid, serous, carcinosarcoma, and clear cell), substage (IIIC1 vs IIIC2), or grade (low-grade vs high-grade). Cox regression models were used to estimate both the unadjusted and multivariate-adjusted relative hazard ratio (HRs) and corresponding 95% confidence interval (CI). All analyses were performed using R software version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). Differences with a two-sided P < 0.05 were considered to be statistically significant.
Results
Patient Demographic and Clinical Data
A total of 2138 cases were identified (Table 1). Overall, 1299 (60.8%) patients were stage IIIC1, 839 (39.2%) were stage IIIC2, 1172 (54.8%) were peritoneal cytology negative, and 363 (17.0%) were positive. The median patient age was 63 years (IQR 57-69 years). The most prevalent histology was endometrioid (n = 1368 [63.99%]), followed by serous (n = 471 [22.03%]), carcinosarcoma (n = 230 [10.76%]), and clear cell (n = 69 [3.23%]).
Characteristics of Women with Stage IIIC Endometrial Cancer by Histology.

Abbreviations: IQR, interquartile ranges; CT, chemotherapy; EBRT, external beam radiation therapy; VBT, vaginal brachytherapy.
Baseline characteristics differed according to histology. The proportion of serous cases increased in recent years (from 12.5% to 21.9%). Black females exhibited a greater proportion of carcinosarcoma (26.1%), serous (22.9%), and clear cell (20.3%) cases than females with endometrioids (7.9%). The median OS for all patients was 48 months (IQR 28-70 months). Histologically, the endometrioid subtype had the longest median OS (54 months [IQR 37-74 months]), followed by clear cell (42 months [IQR 23-59]) months, serous (39 months [IQR 21-58 months]), and carcinosarcoma (32 [IQR 14-52 months]). The median OS was 58 months (IQR 43-78 months) for low-grade patients and 44 months (IQR 24-39 months) for patients with high-grade disease.
Regarding adjuvant treatment, 40.5% of patients underwent chemotherapy alone. When radiation was used in addition to chemotherapy, it was most commonly in the form of chemotherapy with EBRT (35.5%); chemotherapy with EBRT+VBT (15.8%) was less common than chemotherapy with VBT (8.2%). When evaluated according to histology, the carcinosarcoma subtype had the greatest proportion of chemotherapy only (51.7%), whereas chemotherapy with EBRT+VBT was used in similar proportions across all histology types (13.0%-17.0%). Patients with low-grade disease were more likely to undergo chemotherapy with EBRT (39.5% vs 32.7%; P < 0.05) and less likely to undergo chemotherapy alone (34.6% vs 44.7%; P < 0.05) than those with high-grade disease.
Survival Outcomes
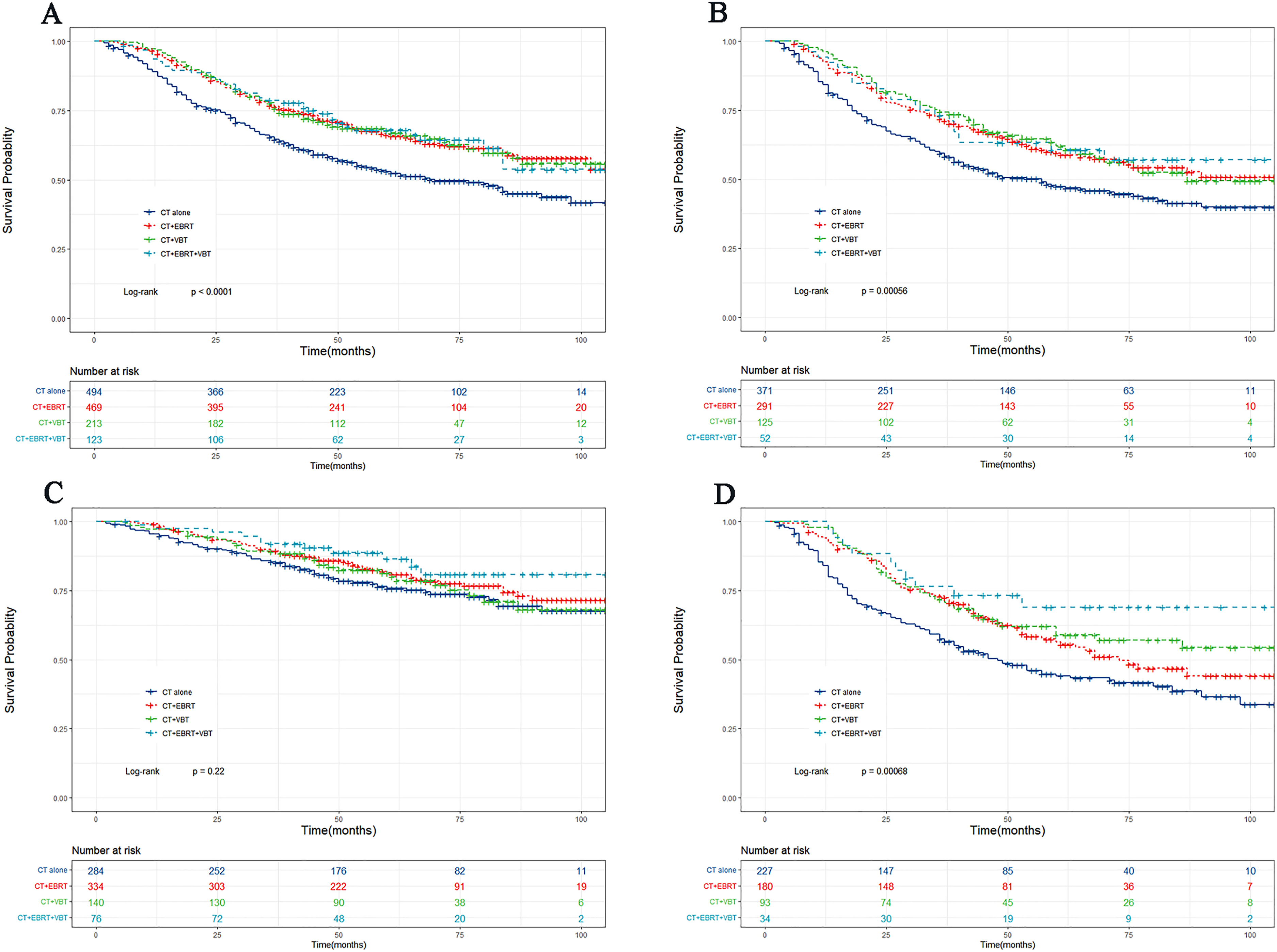
Overall, in the setting of chemotherapy alone as the reference group, patients treated with adjuvant radiotherapy exhibited a significantly reduced risk for death from endometrial cancer in both univariate and multivariate analyses (Table 2, Figure 1). OS also differed according to treatment arm when analyzing each histological subtype, and the use of radiation in addition to chemotherapy was associated with improved OS in endometrioid patients. However, combination therapy was no longer significantly different from chemotherapy alone for clear cell and carcinosarcoma. For serous cancers, chemotherapy + EBRT was associated with a survival benefit compared with chemotherapy alone (Table 2, Figure 2).

Kaplan–Meier curve of overall survival according to adjuvant treatment type in all stage IIIC endometrial cancer.

Kaplan–Meier curves of overall survival according to adjuvant treatment type in endometrioid (A); serous (B); carcinosarcoma (C); and clear cell (D) endometrial cancer patients.
Univariable- and Multivariable-Adjusted Cox Regression Analysis of Overall Survival in the Overall Stage III Patients and Stratified by Histology.
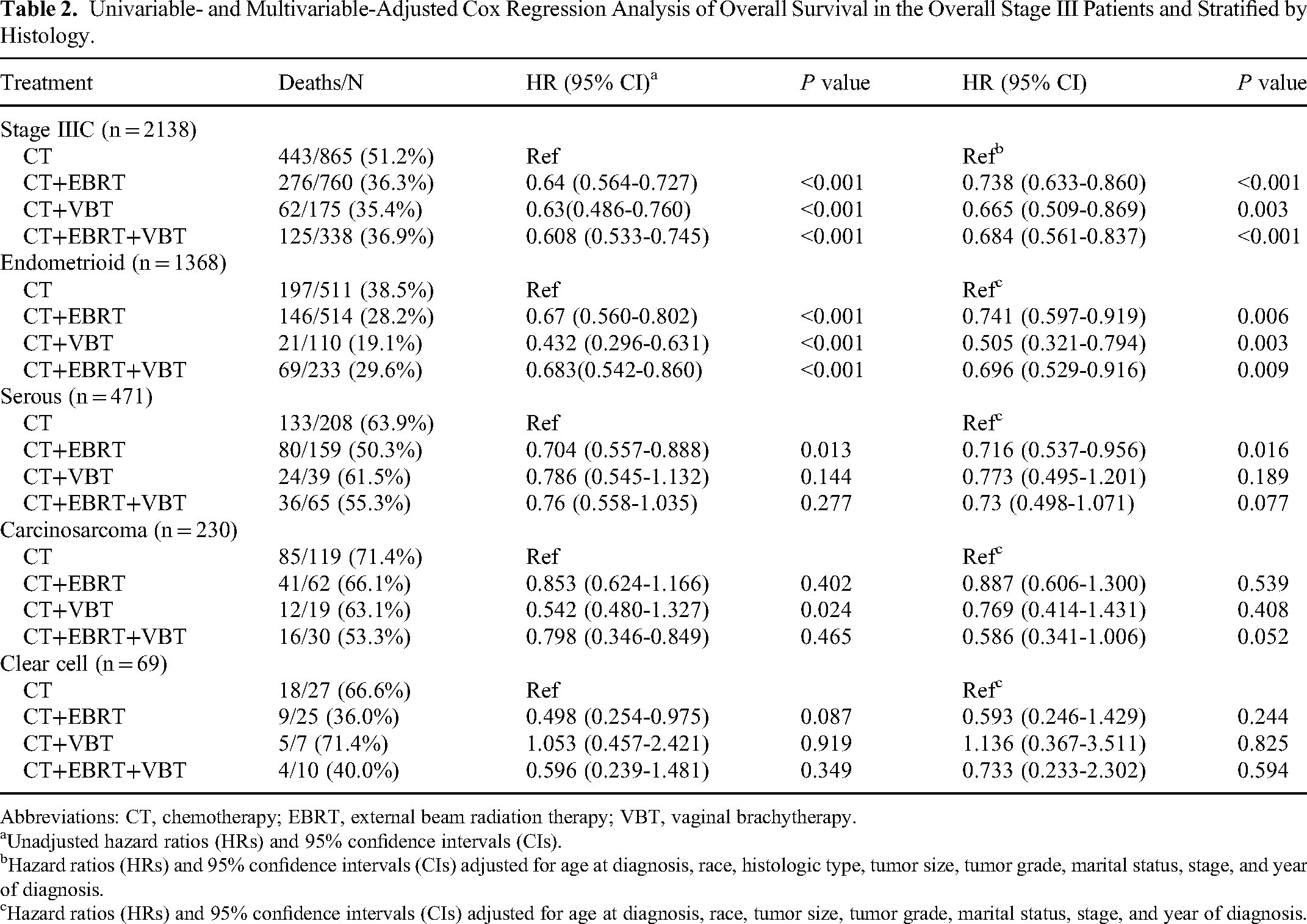
Abbreviations: CT, chemotherapy; EBRT, external beam radiation therapy; VBT, vaginal brachytherapy.
Unadjusted hazard ratios (HRs) and 95% confidence intervals (CIs).
Hazard ratios (HRs) and 95% confidence intervals (CIs) adjusted for age at diagnosis, race, histologic type, tumor size, tumor grade, marital status, stage, and year of diagnosis.
Hazard ratios (HRs) and 95% confidence intervals (CIs) adjusted for age at diagnosis, race, tumor size, tumor grade, marital status, stage, and year of diagnosis.
When examining the association between treatment type and OS stratified according to stage, the addition of radiation to chemotherapy was associated with improved OS in patients with IIIC1 and IIIC2 disease (Figure 3A and B). Similar associations were observed in patients with high-grade stage IIIC endometrioids. However, for low-grade tumors, combination therapy was no longer associated with a reduced risk for death compared with chemotherapy alone (Table 3, Figure 3C and D).
Kaplan–Meier curves of overall survival according to adjuvant treatment type in stage IIIC1 (A); stage IIIC2 (B); low-grade (C); and high-grade (D) endometrial cancer patients.
Univariable- and Multivariable-Adjusted Cox Regression Analysis of Overall Survival in Stage IIIC Patients Stratified by Substage and Grade.

Abbreviations: CT, chemotherapy; EBRT, external beam radiation therapy; VBT, vaginal brachytherapy.
Unadjusted hazard ratios (HRs) and 95% confidence intervals (CIs).
Hazard ratios (HRs) and 95% confidence intervals (CIs) adjusted for age at diagnosis, race, histologic type, tumor size, tumor grade, marital status, and year of diagnosis.
Hazard ratios (HRs) and 95% confidence intervals (CIs) adjusted for age at diagnosis, race, tumor size, marital status, stage, year of diagnosis.
Discussion
In patients with stage IIIC endometrial cancer, radiotherapy improves long-term local control but has a higher rate of distant metastases, whereas chemotherapy effectively reduces the risk for distant metastases but is associated with more frequent pelvic failure. 2 The National Comprehensive Cancer Network (NCCN) guidelines recommend cytoreductive surgery followed by systemic therapy with or without EBRT and/or VBT for patients with stages III and IV endometrial cancer. 8 However, patients with residual lymph node disease following surgery should be treated with either radiotherapy to the pelvis followed by chemotherapy or chemotherapy followed by radiotherapy to the pelvis ± para-aortic nodes according to the European Society of Gynaecological Oncology (ESGO)/European Society for Radiotherapy and Oncology (ESTRO)/European Society of Pathology (ESP) guidelines. 9 This was a large-scale national study of survival outcomes of adjuvant chemotherapy, EBRT, and VBT in 2138 patients with stage IIIC endometrial cancer, and we determined that adjuvant radiation plus chemotherapy was associated with improved OS. Furthermore, stratification according to histological subtype demonstrated the benefit of combined chemotherapy and radiation in high-grade endometrioid disease. However, for low-grade tumors, combination therapy was no longer associated with a reduced risk for death compared with chemotherapy alone. Additionally, for patients with clear-cell cancer and carcinosarcoma, we did not find a clear difference in survival between chemotherapy alone and concurrent regimens.
Several studies have suggested that combination chemoradiation therapy can provide superior long-term survival outcomes for locally advanced endometrial cancer compared with adjuvant monotherapy.5,6 Although the role of chemotherapy cannot be determined, the role of EBRT is yet to be determined. The GOG-258 trial did not demonstrate RFS benefit at 5 years with the addition of radiotherapy to chemotherapy, even after stratification according to disease stage, whereas patients who underwent EBRT alone exhibited higher rates of vaginal and pelvic recurrence. 4 A national cancer database study involving 9837 patients with stages III-IVA endometrial cancer found that the use of chemotherapy with radiation was associated with improved OS compared with radiation alone. 10 Our data demonstrated that stage IIIC endometrial cancer is a heterogeneous disease, and 40.5% of patients underwent chemotherapy only. Our results are consistent with those of other retrospective studies demonstrating that combination adjuvant treatment is superior to chemotherapy alone in patients with stage IIIC endometrial cancer.
Uterine serous carcinoma and clear cell carcinoma represent approximately 15% of all endometrial cancers but account for up to 40%-50% of endometrial cancer-related deaths. 11 In fact, serous and clear cell carcinomas are considered to be high-grade diseases, and both the NCCN and ESGO/ESTRO/ESP guidelines recommend more aggressive treatment for these histotypes.8,9 In the PORTEC-3 trial, serous and clear cell cancers in combination comprised 20%-25% of all patients enrolled. 6 Previous clinical trials1,3,6,7,10 grouped endometrioid and non-endometrioid tumors or included patients with stage IIIA, IIIB, or IV disease, limiting the ability to draw reliable conclusions for patients with stage IIIC serous carcinoma and clear cell carcinoma. Therefore, recommendations obtained from studies consisting mostly of endometrioid carcinoma may not be directly related to serous or clear cell histology.12–14 In a large SEER database analysis of 1789 patients (1437 serous, 352 clear cell), brachytherapy was associated with a significantly reduced risk for death in stage I-II patients, and both chemotherapy and brachytherapy appeared to confer a survival benefit in stage I-II patients with serous histology. 15 In stage III patients, chemotherapy is associated with improved survival outcomes, and EBRT may also benefit stage III patients with clear cell histology. 15 In another database analysis, there was no survival benefit with chemotherapy alone over combination therapy in the adjusted analyses of serous or carcinosarcoma histology. 7 Van Weelden et al 16 reported that chemotherapy + EBRT was associated with superior OS compared with chemotherapy, EBRT, or no adjuvant therapy in carcinosarcomas. Another population-based study reported that chemotherapy with or without radiotherapy had significant survival advantages among 3353 patients with stages III-IV carcinosarcomas. 17 In our cohort, combination therapy was no longer significantly different from chemotherapy alone for any histology (clear cell and carcinosarcoma), whereas EBRT remained significant, and VBT remained non-significant in the serous cohort. Our study provides additional insights into the optimal adjuvant management of serous and clear-cell cancers. Existing studies (both clinical trials and retrospective series) have been limited by sample size and patient heterogeneity and should be further investigated in future studies.
Patients with high-grade disease are most likely to benefit from combined modality treatment because grade 3 tumors have a higher propensity for distant metastasis. 18 Analysis of stage IIIC endometrial cancer stratified according to grade indicated that combination chemotherapy and radiotherapy remained superior to no treatment and chemotherapy alone in the G1-2 subgroup and remained superior to no treatment and radiotherapy alone in the G3 subgroup. 19 In the present study, OS was superior with chemoradiation therapy compared to chemotherapy alone in the high-grade subgroup. Combination chemoradiation therapy was found to be superior to radiotherapy alone in multivariate but not in univariate analysis in the low-grade subgroup. Therefore, radiotherapy may have a greater impact on survival in low-grade diseases, whereas chemotherapy improves the survival of patients with high-grade tumors. 20 Based on survival benefit, combined chemoradiation therapy should be the preferred modality for patients with stage IIIC disease who can tolerate this treatment; however, chemotherapy alone may be non-inferior in patients with low-grade disease, based on grade subgroup analysis.
The present study had several important limitations. First, although a substantial sample size was included in the large-scale database, some subgroups were limited to a small number of patients, which left the data underpowered to detect differences in outcomes in the subgroup analyses stratified according to histology. Second, the SEER database lacks important demographic and treatment variables, such as specific chemotherapeutic agents and number of cycles, radiotherapy details (fields, dose, and fractionation), toxicity of therapy, relapse and recurrence, toxicity data, lymphovascular space invasion, and molecular profiling. We were unable to distinguish between patients who underwent sequential, concurrent, or sandwich adjuvant chemotherapy and those who underwent radiotherapy. In addition, adjuvant treatment decisions for stage IIIC endometrial cancer may be optimized based on the four subgroups with distinct molecular characteristics and prognostic relevance as identified by The Cancer Genome Atlas. 21 Recently, various types of targeted therapies, including checkpoint inhibitors and DNA repair mechanisms, have been investigated in exploratory studies and clinical trials.22–24 Further research integrating molecular factors and new therapeutic targets to identify how this affects the adjuvant treatment of stage IIIC endometrial cancer is warranted.
Conclusion
Collectively, our results revealed that 40.5% of patients with stage IIIC endometrial cancer underwent chemotherapy alone, followed by 35.5% who underwent chemotherapy plus EBRT. Adjuvant chemotherapy plus radiation was associated with improved survival outcomes in stage IIIC patients, particularly those in the high-grade endometrioid subgroup. However, no survival benefit was found, and radiotherapy may be unnecessary in patients with low-grade endometrioids. In the histology-stratified analyses, no survival benefit was found for patients with clear cell and carcinosarcoma histology who underwent the addition of radiation to chemotherapy.
Footnotes
Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by The Youth Innovation Fund of The First Affiliated Hospital of Zhengzhou University and the Scientific and Technological Project of Henan Provine (LHGJ20210436).