
Abstract
Background
Previous studies have failed to investigate the specific effects of advanced age on survival outcomes by considering the Charlson Comorbidity Index (CCI) and age permutation in patients with T1a renal cell carcinoma (T1a RCC) treated by microwave ablation (MWA). Notably, RCC guidelines recommended radiofrequency ablation (RFA) and active surveillance (AS) are both treatment options for elderly T1a RCC, but whether MWA is superior to AS in light of higher heating efficiency and larger ablation zone compared with RFA is not clear. This study aimed to investigate the specific effects of advanced age on survival outcomes of T1a RCC patients stratified by CCI score and indicate better intervention for elderly T1a RCC between MWA and AS.
Methods
This was a retrospective study. We retrospectively reviewed 237 patients with T1a RCC who had undergone MWA over the last 16 years. Data were analyzed by Cox regression and Landmark analysis. Interaction tests and propensity score matching were used to account for potential biases. We compared the overall survival (OS) and cancer-specific survival (CSS) rates of patients ≥75 years in our study with corresponding figures from 4251 counterparts undergoing AS in published articles.
Results
Using patients <75 years with a CCI ≤2 as a reference, the hazard ratio (HR) and 95% confidence interval (CI) of OS for patients<75 years with a CCI ≥3, patients ≥75 years with a CCI ≤2, and patients ≥75 years with CCI ≥3, were 2.954 (1.139-7.663), 3.48 (1.487-8.146), and 3.357 (1.162-9.698), respectively. The adverse effect of an age ≥75 years on OS was attenuated in patients with a CCI ≥3. The attenuation lasted for 62.5 months of follow-up (P = .017). Notably, advanced age exerted a protective effect on progression-free survival (PFS) in patients with a CCI ≥3, increasing the 8-year PFS from 67.8% to 100% (P = .049). Relative to 1-, 3-, 5-, and 8-year survival data for patients aged ≥75 undergoing AS, the OS rates for 5-year follow-up were always better in MWA. However, beyond 5 years, the OS rates dropped to levels that were similar to AS.
Conclusions
Advanced age exerts adverse effects and significantly protective effects on OS and PFS, respectively, in T1a RCC patients with a CCI ≥ 3. According to our study, elderly patients with T1a RCC underwent radical MWA may yield a better medium-term OS relative to AS.
Introduction
The incidental detection of renal masses has become increasingly common over the last two decades. 1 As life expectancy increases, a substantial number of diagnoses are made in the elderly population, often in the 7 or 8 decades of life 2 ; these diagnoses are often associated with significant comorbidities.
Previous studies reported that age and Charlson Comorbidity Index (CCI) score were the strongest predictors of overall survival (OS) for T1a renal cell carcinoma (RCC) patients 3 and that the benefits of OS from partial nephrectomy (PN) were both attenuated if a patient was older than 75 years.4,5 Mortalities are most likely caused by cardiovascular diseases (CVDs) arising due to the susceptible loss of renal function after surgery in elderly patients. 6 An age ≥60 years was previously identified as an independent adverse predictor for progression-free survival (PFS) due to age-related immunosenescence and immunosuppression following surgery. 7 Microwave ablation (MWA) as one of the TA techniques was developed by our team in China, and has been widely used depending on its excellent advantages such as higher heating efficiency, larger ablation zone, and antitumoral immunoactivation.8,9 Whether these theoretical advantages of MWA can be translated into tangible survival benefits for the elderly remain unknown. Our department as the largest MWA treatment center in China began to use MWA to treat T1a RCC in 2006. With the wide popularization and excellent efficiency of MWA in treating T1a RCC, international guidelines have recommended both MWA and active surveillance (AS) as alternatives for the management of a T1a RCC <3 cm in size for elderly patients.10,11 This creates confusion for clinicians with regard to whether TA can narrow the gap for OS, cancer-specific survival (CSS), and PFS between elderly and young patients. These guidelines also create confusion as to which modality (TA or AS) should be more strongly recommended for the treatment of T1a RCC in the elderly population.
In this study, we investigated the prognostic significance of age in T1a RCC patients undergoing TA and compared the survival rates between TA and AS.
Methods
Study Design and Patients
This was a retrospective study. The electronic clinical records system was consulted to retrieve data in all consecutive patients who underwent percutaneous MWA for cT1a RCC between April 27, 2006 and November 4, 2020 (n = 237). We have de-identified all patient details. Only those with histologic confirmation of RCC diagnosis and an RCC of 4 cm or smaller were included. The patient inclusion/exclusion criteria and the management protocol algorithm were shown in Figure 1. WHO defines people ≥75 years as elderly people, therefore, we adopt this criteria to define elderly patients by age 75. We compared the OS and CSS rates of patients ≥75 years in our study with corresponding figures from 4251 counterparts undergoing AS in published articles (data derived from the SEER, RESURGE, DISSRM databases, or a large institutional chart). None of AS patients were excluded due to delayed intervention during the follow-up period. The Ethics Committee of the Chinese PLA General Hospital (Beijing, China) approved the protocol (Approval No. S2023-186-01) on March 23, 2023. All patients provided written informed consent for treatment. The committee authorized the chart review. We have de-identified all patient details. The reporting of this study conforms to REMARK guidelines. 12
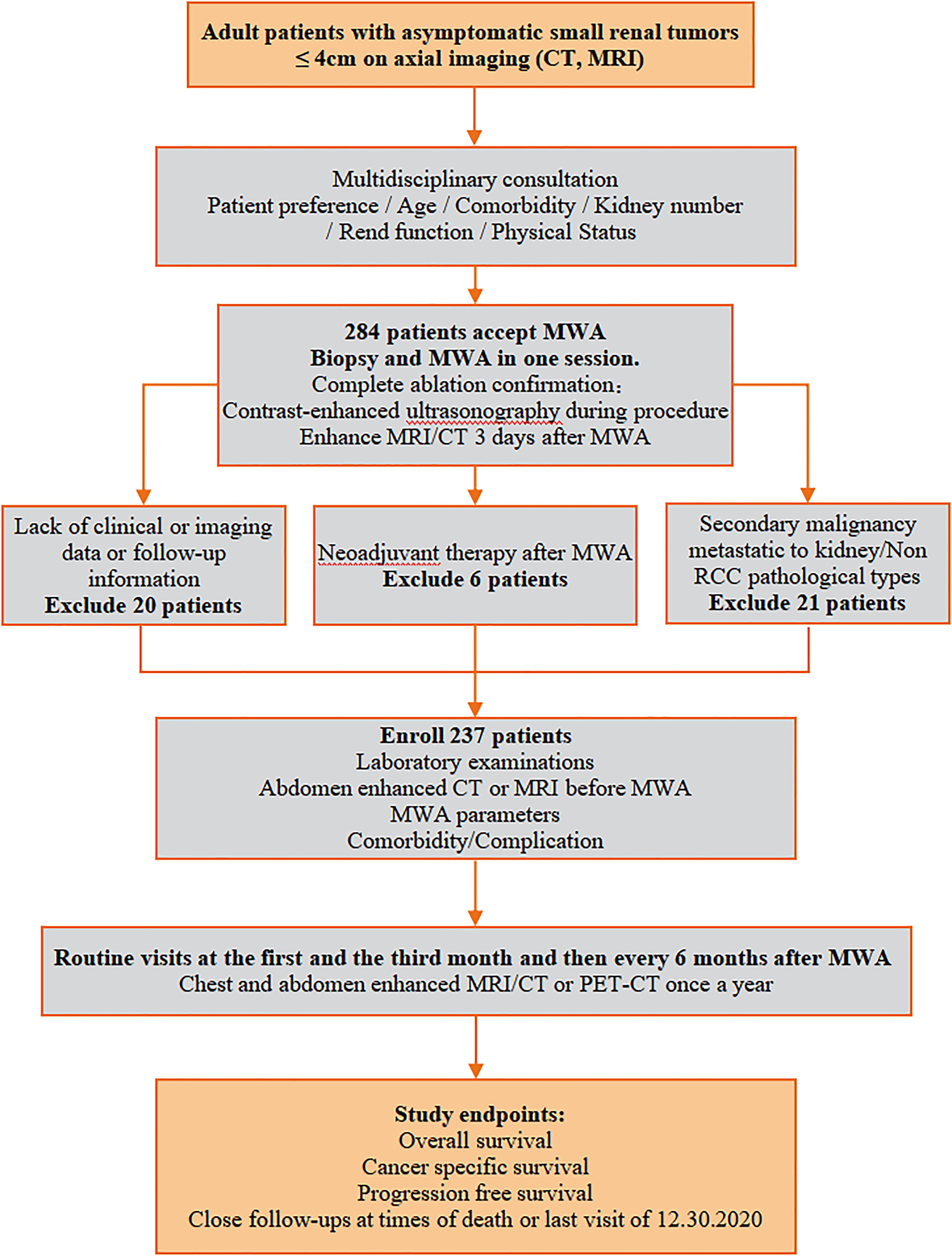
Inclusion and exclusion criteria and an algorithm for the management of T1a RCC patients who underwent MWA. Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging.
Follow-Up and Outcomes
Data provided by clinicians who fill up online standardized forms comprising patients’ age, sex, baseline eGFR, comorbidity, patient type, along with other disease characteristics such as tumor diameter, tumor adjacency, tumor pathology, and hydro-dissection technology were systematically sent to the electronic medical records system. After MWA treatment, complications within 30 days were recorded based on the classification of the Clavien–Dindo system. A major complication was defined as an event that led to substantial morbidity and disability (eg, resulted in the unexpected loss of an organ) and that increased the level of care, resulted in hospital admission, or substantially lengthened hospital stay (ie, ClavienDindo grades III-V complications). 13 Untreated fever, ascites, or elevated serum creatinine was not identified as complication. Routine visit was repeated at the first and the third month and then every 6 months. Besides routine visits, the life status and RCC outcomes were also recorded by telephone follow-up at the end of each year. After that, reason and date for death were measured and recorded. Tumor adjacent to the renal pelvis and bowel were defined as the distance between tumor margin and renal pelvis or bowel ≤5 mm as measured by ultrasound. 14 The indication for pyeloperfusion was the tumor protruding into renal pelvis.
Statistical Analysis
Statistical analyses were performed with SPSS 12.0 and R software. Cox proportional hazards model and time-dependent Cox regression analyses were performed to identify all possible predictors. Log-rank test and landmark analysis were used to compare the survival rates between groups. Propensity score matching was used to evaluate potential biases resulting from both measured and unmeasured confounders. Interaction tests were used to assess the independent role of age in predicting survival prognosis. Two-tailed P values of <.05 were considered statistically significant. Post hoc power calculation given the study's retrospective nature and absence of a predefined hypothesis, a priori sample size was not calculated. Post hoc power calculations were performed for the endpoints of OS in the PSM analysis. Data were analyzed using version 15.0 of PASS for the power analysis. Through statistical calculation, under the current sample size and significance level, the power calculated by OS at 120 months of follow-up is 0.99, and the power calculated by OS at 84 months of follow-up is 0.95.
Results
Baseline Characteristics
Table 1 shows the baseline characteristics of 237 patients with 245 tumors. The follow-up period was less than 6 months for 19 patients (8.0%), 6 months to 1 year for 11 patients (4.6%), 1-3 years for 53 patients (22.3%), 3-5 years for 50 patients (21%), 5-10 years for 83 patients (34.9%), and >10 years for 21 patients (8.9%). Detailed data before and after PSM for the total cohort and sub-cohorts are shown in Supplemental Figure 1.
Clinical Features of Patients and Tumors.

Lack of preoperative serum creatinine in 15 patients.
Data are means and standard deviation; data in parentheses are ranges.
Data in parentheses are percentages.
The Effect of Age on OS
Age was identified to be the only independent prognostic factor for OS for the total cohort (Table 2; Supplemental Table 1). The higher risk of overall mortality in patients ≥75 years was not significantly affected by gender, CCI, tumor diameter, pathology, tumor location, tumor adjacency, preoperative eGFR, or complications (Supplemental Table 2; P > .05 for all). After PSM, and using patients <75 years as a reference, the hazard ratio (HR) of overall mortality for patients ≥75 years was 2.703. Kaplan–Meier survival curves revealed significantly lower OS rates in patients ≥75 years, with 1-, 3-, 5-, 8-, and 10-year OS rates of 98.4%, 93.7%, 84.3%, 40.0%, and 27.6% versus 97.1%, 91.9%, 86.2%, 81.6%, and 71.2%, respectively, in patients<75 years (P = .008; Figure 2).

Kaplan–Meier curve and landmark analysis comparing OS, CSS, and PFS between T1a RCC patients aged ≥75 years and those <75 years after PSM across the entire cohort (A1, B1, C1), sub-cohort with a CCI ≤2 (A2, B2, C2), and a sub-cohort with a CCI ≥3 (A3, B3, C3). (A) OS: overall survival; (B) CSS: cancer-specific survival; (C) progression-free survival; 1: total cohort; 2: sub-cohort with a CCI ≤2; 3: sub-cohort with CCI ≥3.
Independent Prognostic Factors for OS, CSS and PFS.

Abbreviations: OS, overall survival; PFS, progression-free survival; CCI, Charlson Comorbidity Index; HR, hazard ratio; CI, confidence interval.
For the sub-cohort with a CCI ≤ 2, age and patient type were significantly associated with OS (Table 2; Supplemental Table 3). Using patients<75 years as a reference, the HR of overall mortality for patients ≥75 years was 4.686. Kaplan–Meier survival curves revealed significantly lower OS rates in patients ≥75 years, with 1-, 3-, 5-, 8-, and 10-year OS rates of 97.1%, 91.9%, 82.0%, 37.5%, and 37.5% versus 97.8%, 92.6%, 92.4%, 89.3%, and 68.5%, respectively, in patients<75 years (P = .004; Figure 2 and Supplemental Figure 2).
Notably, for the sub-cohort with a CCI ≥ 3, none of the variables were significantly associated with OS (Supplemental Table 4 shows data after PSM). However, Landmark analysis revealed significantly lower OS rates in patients ≥75 years after 62.5 months of follow-up, with 8- and 10-year OS rates of 33.8% and 18.4% versus 77.3%, and 77.3% in patients aged <75 years (P = .017; Figure 2).
The Effect of Age on CSS
Age was not significantly associated with CSS. When considering the total cohort, patient type, and nodule number were prognostic factors for CSS. Relative to incipient patients, or patients with single nodules, relapsed patients or patients with multiple nodules had an 8- or 18.401-fold higher risk of death from RCC (Table 2; Supplemental Table 5 shows data after PSM).
For the sub-cohort with a CCI ≤ 2, patient type and nodule number remained significantly associated with CSS (HR: 0.073, 95% CI [0.007-0.797], P = .032 for patient type; HR: 23.2, 95% CI [2.174-247.556], P = .009 for nodule number; Table 2; Supplemental Table 6). However, for patients with a CCI ≥3, none of the variables were associated with CSS (Supplemental Table 7).
The Effect of Age on PFS
Being a recurrent patient was the only predictor for poor PFS across the total cohort and sub-cohorts with a CCI ≤ 2. Relative to incipient patients, relapsed patients had a 4.5-fold higher risk of RCC progression (Table 2; Supplemental Tables 8-9). Advanced age exerted a protective effect on PFS in the sub-cohort with a CCI ≥ 3. Younger patients seemed more susceptible to RCC progression compared to their elderly counterparts (8/37 vs. 0/15). The 1-, 3-, 5-,8-, and 10-year PFS rates were 94.6%, 85.5%, 81.3%, 67.8%, and 67.8% in patients<75 years versus 100.0%, 100.0%, 100.0%, 100.0%, and 100.0% in patients ≥75 years (P = .049; Figure 2 and Supplementary Figure 2). This phenomenon was unexpected.
A Comparison of OS and CSS Between MWA and AS in Elderly T1a RCC Patients
Next, we compared the OS and CSS rates of patients ≥75 years in our study with corresponding figures from counterparts undergoing AS (data derived from the SEER, RESURGE, and DISSRM databases, and a large institutional chart; Supplemental Table 10). The 1-, 3-, and 5-year OS rates of patients undergoing AS were 88.1-93.0%, 63.3-73.0%, and 46.4-58.0%,6,15,16 lower than those in patients undergoing MWA, regardless of whether we considered the total cohort (98.4%, 93.7%, and 84.3%) or CCI-stratified sub-cohorts (97.1%, 91.9%, 82.0% for CCI ≤2; 100.0%, 100.0%, 86.3% for CCI ≥3). However, the 8-year OS rate for MWA modality dropped to a level that was similar to that of AS (33.8-40.0% vs. 31.3-46.2%).6,17 Unlike OS, the differences of the 1-, 3-, 5-, and 8-year CSS rates between MWA and AS were narrow: 97.5-100.0%, 92.4-100.0%, 92.4-100.0%, and 72.8-88.8% for MWA versus 95.9-97.0%, 89.4-94.0%, 82.5-94.0%, and 64.0-92.4% for AS.
Complications Between Patients Stratified by the Age of 75 Years
The incidence of Clavien–Dindo classified complications was not significant when compared between patients<75 years and those ≥75 years, irrespective of whether we considered the total cohort or the CCI-stratified sub-cohorts (all P>.5; Supplemental Table 11). Cox regression models also showed that complications were not an independent risk factor for OS, CSS, and PFS (Table 2 and Supplemental Tables 2-9).
Discussion
Accurate prognostic evaluation for patients with T1a RCC is a clinical dilemma. Previous studies indicated that the benefits (OS, CSS, and PFS) associated with curative PN were all attenuated if a patient was older than 75 years.4,5 Some scholars believe that this phenomenon was associated with immunosuppression and the increased risk of cardiovascular death in the elderly. 6
It is common knowledge that TA has less impact on renal function relative to PN and activates anti-tumor immunity. 18 However, previous studies did not determine whether the technical advantages of TA could be translated into clinical practice. In the absence of a randomized clinical trial, our findings are viewed as the best evidence from a long follow-up period (almost 16 years).
Several findings in the current study were noteworthy. Firstly, advanced age does not always play a negative role affecting survival outcomes. It can protect T1a RCC patients with a CCI ≥ 3 from RCC progression. Secondly, advanced age can not lead to a significantly worse OS in individuals with a CCI ≥ 3. Last but not least, MWA can further improve the short-medium term OS prognosis in patients aged ≥75 relative to counterparts who underwent AS.
Our study proved that as age increases, the OS benefit from MWA was attenuated. However, in patients with a CCI ≥ 3, the attenuation mainly occurred after 62.5 months of follow-up. Sub-cohort analyses with a CCI ≥ 3 showed that 33.3% of mortality was attributed to cardiovascular causes in patients<75 years, but this ratio increased to 80% in patients ≥ 75 years (P<.001). Outwardly, the wider disparity of cardiovascular mortality between patients ≥ 75 and patients<75 years should have highlighted the significant impact of advanced age on OS in patients with a CCI ≥ 3. In fact, there were great differences in the types of comorbidity when compared between elderly and young patients in this sub-cohort. Other systemic malignancies and advanced cirrhosis were common in patients<75 years (21/37, 56.8%) and CVDs were predominant in the elderly (12/15, 80.0%). Malignancy and advanced cirrhosis should be more lethal than a CVD over the short term. The development of CVD from the first diagnosis to death should take at least 5 years. 19 Therefore, the OS rates of elderly patients decreased substantially just after the 5-year follow-up, significantly lower than their younger counterparts. For relatively healthy patients (CCI ≤ 2), the higher overall mortality in the elderly represents the inherent biological nature of human beings.
In view of the reduced OS benefits in the elderly, we next investigated whether such patients should adopt AS instead of any form of radical treatment. We compared the survival rates of patients aged ≥75 years between MWA and AS and found that elderly T1a RCC patients were able to achieve better short- to medium-term OS outcomes from MWA relative to AS. However, from a long-term perspective, OS rates were comparable between the two modalities. The OS improvement for MWA over AS was 9.0%, 28.6%, and 37.9% at 1, 3, and 5 years, respectively, corresponding to the need to treat 11.1, 3.5, and 2.6 patients with MWA, respectively, to avoid 1 all-causes of death. This is inconsistent with conclusions from other recommendations stating that AS can be used as an option for the initial management of elderly T1a RCC whose diameter is less than 3 cm without invasive features.10,11 We believe that AS should not be recommended for most T1a RCC patients, unless the patient is facing the threat of death.
Age was not significantly associated with CSS. This finding was not consistent with previous studies involving PN.4,5 The tempered CSS benefit from PN or RN in elderly patients may be due to age-related immunosenescence and immunosuppression following surgery. 7 This can be reversed precisely by the activation of anti-tumor immunity depending on tumor antigen release after TA.20,21
PFS outcomes after PN are known to be controversial when considered by age.22,23 For TA, most studies reported that age was not associated with PFS in terms of cryoablation and radiofrequency ablation (RFA).24,25 However, our result is unique and has not been reported previously. We found that a younger age (<75 years) rather than an advanced age (≥ 75 years) worsened the PFS. We could not find any evidence to explain the phenomenon in the existing literature. We believe that this was related to comorbidity in the younger patients. Of the 37 progressive patients, 28 patients (75.7%) were aged under 75 years; 53.6% (15/28) had other systemic malignancies prior to the diagnosis of RCC. The corresponding figure in the elderly was just 22.2%. Younger patients are more likely to have a cancer-susceptible somatoplasm and cancer-aggressive behavior relative to their elderly counterparts.26,27 Cancer-susceptible somatoplasm refers to a poor genetic background that may form the fundamental mechanism for RCC recurrence or metastasis after curative treatment. 28 Previous researches hypothesized that gene polymorphism may explain the essentials of this phenomenon. 29
By comparing OS and CSS data between MWA and AS, we were led to consider why RCC ablation obviously improved OS more than CSS. We think these results are related to two different aspects: oncological behavior and the impact of cancer on CVD. 30 The indolent nature of small RCC leads to the majority of elderly T1a RCC patients dying from non-RCC causes before they develop poor oncological outcomes. More importantly, cancer could give rise to the onset or deterioration of CVD via specific mechanisms.31,32 Duarte et al used network methodologies to prove that cancer is an independent risk factor for CVD after adjustment for age, gender, and after correction for behavioral risk factors. 33 Therefore, the effective method with which to treat T1a RCC is to prevent the onset or deterioration of CVD and not just kill tumors.
The current study is not without limitations. First, the analyses are retrospective in nature; this comes with an unavoidable selection bias that is prevalent in all non-prospective, non-randomized studies. Second, it is essential to recognize that the current study only compromises single-center cohort. Prospective, randomized trial evaluating the influences of risk factors on survival benefits from TA based on multi-centers will represent the strongest level of evidence for clinical guidance. Moreover, the trial may be underpowered to detect a true survival difference between patients stratified by CCI and age permutation, because of the small available sample size in subgroups. Third, the database does not contain information on certain preoperative laboratory variables and pathological variables that have been shown to be independent prognostic factors for survival (eg, albumin, lactate dehydrogenase, Fuhrman grade et al). 34 Forth, we extracted patients at the time of MWA treatment. It is possible that some recurrent patients had undergone adjuvant anti-tumor therapy which was not exactly provided in the database, such as traditional Chinese medicine.
Conclusion
Advanced age significantly worsens OS of T1a RCC patients with CCI ≤ 2, but young age significantly worsens PFS of T1a RCC patients with CCI ≥ 3. MWA may bring out better medium-term OS and CSS outcomes to elderly patients relative to AS. Complications after MWA between patients aged <75 and ≥75 are not significant. Our study may help clinicians to deal with elderly T1a RCC patients more scientifically and reasonably.
Supplemental Material
sj-docx-1-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-1-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-3-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-3-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-4-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-4-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-5-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-5-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-6-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-6-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-7-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-7-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-8-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-8-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-9-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-9-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-10-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-10-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-11-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-11-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-12-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-12-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-13-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-13-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Supplemental Material
sj-docx-14-tct-10.1177_15330338231183585 - Supplemental material for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience
Supplemental material, sj-docx-14-tct-10.1177_15330338231183585 for Prognostic Significance of Advanced Age in Patients with T1a Renal Cell Carcinoma Treated by Microwave Ablation: A 16-Year Experience by Qidi Hou, Yaxi Wang, Dongyun Zhang, Yanchun Luo, Linan Dong, Mengjuan Mu, Jie Yu and Ping Liang in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the institutional review board of Chinese PLA General Hospital (Beijing, China), Approval No. S2023-186-01 (March 23, 2023). All patients provided written informed consent for treatment. The committee authorized the chart review.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Funds for PHD researchers of Guangdong Medical University in 2021 (No. 4SG21262G), Military health care project (No. 20BJZ42) and National Natural Science Foundation of China (No.12126607, No.82030047, No. 82030047).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.