
Abstract
Background and Aims:
To evaluate long-term outcomes and prognostic factors of laparoscopic microwave ablation as a first-line treatment for hepatocellular carcinoma located at the liver surface not feasible for percutaneous ablation.
Methods:
51 consecutive patients receiving laparoscopic microwave ablation in our center between January 11, 2012, and July 31, 2014, were enrolled. Technique effectiveness (complete ablation or incomplete ablation) was evaluated 1 month postprocedure. Procedure-related complications were recorded. The influences of patients’ baseline characteristics on recurrence-free survival and overall survival were analyzed after a median follow-up of 34.0 (ranging 19.0-49.0) months.
Results:
Complete ablation was gained in 47 (92.2%) of the 51 patients. No patients died within 30 days of microwave ablation procedure. A total of 3 (5.9%) cases of complications were observed. Tumor progression/recurrence were observed in 40 patients (78.4%). The median recurrence-free survival and median overall survival of the total cohort was 11.0 months (95% confidence interval: 7.573-14.427) and 34.0 months (95% confidence interval: 27.244-40.756), respectively. Multivariate analysis identified alanine transaminase level and tumor number as independent significant prognosticators of recurrence-free survival whereas α-fetoprotein level as significant prognosticators of overall survival.
Conclusions:
As a first-line treatment, laparoscopic microwave ablation provides high technique effectiveness rate and is well tolerated in patients with hepatocellular carcinoma located at liver surface. Alanine transaminase and tumor number were significant predictors of recurrence-free survival, whereas α-fetoprotein level was significant predictor of overall survival. Laparoscopic microwave ablation might serve as a rational treatment option for patients with hepatocellular carcinoma with tumors at the liver surface, which merits validation in future perspective studies.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is the second leading cause of cancer death worldwide, with half of the mortalities being in China. 1 Hepatic resection and liver transplantation represent curative treatments for patients with HCC, 2,3 which, however, are applicable to only 10% to 25% of patients when diagnosed. 4 In recent years, thermal ablative therapies such as radiofrequency ablation (RFA) have emerged as a well-accepted alternative for patients with HCC of Barcelona Clinic Liver Cancer (BCLC) stage 0-A who are not eligible for hepatic resection and liver transplantation. 2 Microwave ablation (MWA) is another form of thermal ablation currently in use in many centers. Owing to its physical properties, MWA possesses several theoretical advantages over RFA, such as less-affected tissue charring during ablation and thus capable of producing larger ablation zone. 5 Recent studies suggest that MWA is less affected by heat sink effect 6 and might be more effective in treating large HCC 7,8 compared to RFA.
The MWA is mainly conducted through imaging-guided percutaneous approach by virtue of its minimally invasive nature. However, there are some tumor lesions located in areas that render percutaneous MWA unfeasible, such as ones protruding from liver surface and ones adhering to adjacent tissues/organs. These areas were referred to as “risk areas” in previous literatures, 9,10 and percutaneous MWA of lesions in these areas was technically challenging because it is hard to reach a balance between the need of complete ablation (CA) and the need of avoiding heat injury to adjacent tissues. These patients, however, might benefit from laparoscopic MWA, which guarantees a safer approach to liver tumors and enables intracorporeal ultrasound guidance and scrutiny. This study aimed at evaluating the technique effectiveness and long-term outcomes of laparoscopic MWA patients with HCC lesions not eligible for liver resection or percutaneous ablation.
Materials and Methods
Diagnosis and Treatment Allocation of HCC
Institutional Ethics Committee of Renji Hospital (Shanghai, China) approved this retrospective study. All HCC were diagnosed according to the guideline of the European Association for the Study of the Liver. 2 To be specific, the diagnosis was confirmed by biopsies in patients without cirrhosis and by typical features on 1 (for nodules of 1-2cm) or 2 (for nodules >2 cm) imaging technique(s) in patients with cirrhosis. Diagnosis was confirmed by biopsy in case of atypical radiological findings. The HCC were staged according to the BCLC staging system. 11
The clinicopathological characteristics of each patient were assessed for treatment allocation by the HCC expert team in Renji Hospital comprising hepatologists, liver surgeons, interventional radiologists, and oncologists.
Patients were allocated to local ablation therapies as an initial treatment for one of the following reasons: Patients within Milan criteria (single tumors ≤5 cm or 3 nodules ≤3 cm) but not eligible for liver resection and liver transplantation because of (a) refusing liver resection and liver transplantation for psychological/religious reasons; (b) contraindicated to liver transplantation and liver resection due to comorbidities (such as severe portal hypertension, impaired liver function, or compromised cardiopulmonary function); and (c) unable to receive liver transplantation due to lack of suitable transplant organ or economic reasons. Patients beyond Milan criteria but with tumors within 8 cm that could be clearly delineated under ultrasound and had a high likelihood to be completely ablated as assessed by our HCC expert team.
Subsequently, patients with tumors at the liver surface unfeasible for percutaneous approach were allocated to laparoscopic MWA, the scenario of which included (1) tumors protruding from liver surface; (2) tumors contacting or adhering to diaphragm or abdominal viscera (gastrointestinal tract and gallbladder) that could be displaced during laparoscopy; and (3) subphrenic tumors difficult to accurately target percutaneously, as confirmed by expert radiologists skilled in interventional procedures.
Patient Enrollment
The medical records of patients with HCC who received MWA in Renji Hospital (Shanghai, China) from January 11, 2012, to July 31, 2014, were reviewed and informed consents from patients to allow the review and analyses of their medical records were obtained. Patients were enrolled into this study according to preset criteria as shown in Figure 1.

Flowchart of patient’s enrollment.
Patients inclusion criteria were as follows: (1) treatment-naïve patients with HCC receiving laparoscopic MWA alone or in combination with percutaneous MWA in Renji Hospital (Shanghai, China) as an initial treatment from January 11, 2012, to July 31, 2014; (2) single lesion within 8 cm, or multiple (≦3) lesions with no more than 1 lesion beyond 5 cm; (3). Child-Pugh score A or B; and (4) adequate hematologic (platelet count >40 × 109/L, international normalized ratio <2.0) and renal (creatinine <2.0 mg/dL) functions.
Patients exclusion criteria were as follows: (1) patients who received other anticancer treatment before MWA, such as hepatic resection, sorafenib, RFA, or transcatheter arterial chemoembolization (TACE); (2) patients with vascular invasion, extrahepatic metastases, or malignancies of other tissue-of-origin; (3) patients with signs of decompensated cirrhosis such as clinical hepatic encephalopathy and refractory ascites; and (4) patients with compromised cardiopulmonary function who were unable to tolerate laparoscopic MWA.
Procedures of Laparoscopic Ultrasound Examination and Laparoscopic MWA
All laparoscopic ultrasound examination (LUS) and laparoscopic MWA procedures were performed under general anesthesia. Vital signs were monitored throughout the procedures. Abdominal access was obtained using a 12-mm optical trocar in the right upper quadrant (RUQ). Artificial pneumoperitoneum was developed through CO2 inflation to maintain a pneumoperitoneum pressure of about 12 to 14 mm Hg. Subsequently, another 12-mm trocar was placed in the RUQ. Diagnostic laparoscopy and LUS of the liver were performed by a surgeon trained in ultrasound techniques prior to each MWA. The LUS was carried out using a probe with either a rigid shaft (Aloka SSD 500, Sunbright, Shanghai, China [1996-1999]) or a flexible tip (50 cm in length; 10 mm in diameter). The tip of the shaft was side mounted by a 7.5 linear-array transducer, the length of whose surface was 38 mm, producing an image footprint of approximately 4 cm in length and 6 cm in depth.
Depending on the extent of tumor exposure, the extent of tumor adhesion, and the relative positions of tumor and its adjacent tissues under the laparoscopy, additional puncture tunnels would be developed under the xiphoid and/or next to the costal margin if deemed necessary, with an aim to separate adhesions and to expose tumors completely.
Laparoscopic MWA was performed with a 2450 MHz MTC-3C microwave generator (Vision Medical, Nanjing, China), which has a 25 cm cooled-shaft electrode probe (15-gauge) with a 1.5 cm expandable tip. The settings of power output were 80 to 100 W. The MWA was started once the electrode needles were placed into the tumors under laparoscopy or LUS. During ablation procedure, complete coverage of the tumor region by hyperechoic under real-time ultrasound was regarded as a measure of complete tumor ablation. At least 0.5 cm of the normal hepatic parenchyma surrounding the tumor was ablated as an ablative margin to achieve complete tumor destruction.
For each tumor, the most suitable ablation strategy was discussed and determined at an intradisciplinary meeting prior to each MWA procedure. The number of electrodes used and ablations needed were determined depending mainly on tumor characteristics and patient general conditions.
To treat the majority of tumors within 3 cm in diameter, single ablation with one electrode under laparoscopy or LUS was usually sufficient, but for those highly irregular ones, multiple ablations were applied so as to guarantee treatment efficacy. For tumors of 3 to 5 cm, multiple overlapping ablations under laparoscopy or LUS were harnessed. The electrode was inserted until the distal margin of the lesion and then was withdrawn every 1.0 to 1.5 cm to repeat the ablation.
Tumors larger than 5 cm were ablated by laparoscopic MWA combined with percutaneous MWA. In these cases, multielectrode and multiplanar ablation strategy was used, in which the intrahepatic part of the tumor was ablated by percutaneous MWA whereas the superficial part was ablated by laparoscopic MWA.
All procedures were performed by 1 of the 4 doctors (Z.B., W.T., S.W.H., C.J.C.) with at least 4 years of MWA experience. Laparoscopic cholecystectomy was performed in 7 cases where tumors adhered to the gallbladder. Detailed ablation parameters were shown in Supplementary Table 1.
After ablation, patients were monitored for a couple of hours in a recovery unit and then were sent back to the ward. A complete panel of blood chemistry, including liver and renal functions, was examined pre- and postablation.
Evaluation of Technique Effectiveness and Procedure-Related Complications
Technique effectiveness was assessed 1 month post-MWA by contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI). The ablation was considered complete (CA) if the ablation zone completely covered the tumor and no irregular enhancement existed at the ablation margin, which was regarded as technical effectiveness. Otherwise, the treatment was defined as incomplete ablation (IA).
According to the recommendations by the International Working Group on Image-Guided Tumor Ablation, 12 major procedure-related complications referred to those that lead to substantial morbidity and disability, increase the level of care, or result in hospital admission or substantially lengthens the hospital stay. All other complications were defined as minor.
Patients Follow-Up and Definition of Tumor Progression/Recurrence
Patients’ follow-up, including detailed history, physical examination, blood chemistry, and imaging (contrast-enhanced CT or MRI) evaluation, was performed 1 month postablation, every 3 months for the first year, and every 4 to 6 months thereafter.
Tumor progression/recurrence were defined according to the International Working Group on Image-Guided Tumor Ablation. 13 Briefly, in patients of CA, local tumor progression was defined as reappearance of enhancement within or contacting the ablation zone on follow-up imagines. Intrahepatic distant recurrence (IDR) was defined as the occurrence of tumor lesions within the liver but not contacting the ablation zone. Extrahepatic recurrence (ER) was defined as extrahepatic metastasis.
Recurrence-free survival (RFS) was calculated from the day of initial MWA to the day of tumor progression/recurrence or death or last follow-up. Overall survival (OS) was calculated from the day of initial MWA to the day of death (confirmed by medical records or by family members) or last follow-up.
Treatment Strategy After Tumor Progression/Recurrence
Treatment strategies after first tumor progression or recurrence included liver transplantation in 1 patient, hepatic resection in 2 patients, TACE in 27 patients, TACE plus sorafenib in 1 patients, Chinese traditional medicine in 2 patients, and MWA and/or RFA in 6 patients. Detailed treatment strategies after tumor progression or recurrence are shown in Figure 2.

Treatment strategies after recurrence in patients with primary or secondary technique effectiveness.
Statistical Analysis
The correlations between tumor characteristics and technique effectiveness were analyzed by χ2 test or Fisher exact test. Median OS (mOS) and median RFS (mRFS) were calculated using the Kaplan-Meier method and compared by the log-rank test. Variables with P values <.25 on univariate analyses were included in multivariate analysis (Cox proportional hazards model; Backward selection). All statistical analyses were conducted using SPSS 22.0 for Windows (SPSS, Chicago, Illinois). P < .05 was considered as statistically significant.
Results
3 Baseline Characteristics of Patients Included in This Study
According to the preset patient inclusion and exclusion criteria, a total of 51 patients were included in this study, and 27 of them had died by the last follow-up (January 31, 2016). The median follow-up was 34.0 months (ranging from 19.0 to 49.0 months). Patients’ baseline clinicopathologic features were shown in Table 1.
Preablation Clinicopathologic Characteristics of Patients Included in This Study.

Abbreviations: AFP, α-fetoprotein; ALT, alanine transaminase; AST, aspartate transaminase; CA199, carbohydrate antigen 199; CEA, carcinoembryonic antigen; HBV, hepatitis B virus; HCV, hepatitis C virus; TBil, total bilirubin.
Ablation Effectiveness, Complications, and Long-Term Outcomes
The CA was gained in 47 of the 51 patients, with CA rate being 92.2%. The CA rates of patients with largest tumors ≤3 cm, 3 to 5 cm, and >5 cm were 94.4% (17/18), 85.7% (18/21), and 100% (12/12), respectively. No patients died within 30 days of MWA procedure.
A total of 3 (5.9%) cases of complications (2 cases of acute renal deficiency and 1 case of hyperbilirubinemia) were observed during follow-up. All these 3 cases of complications subsided naturally or after medication.
Tumor progression/recurrence was observed in 40 (78.4%) patients by the last follow-up (January 31, 2016), of which 8 patients (15.7%) suffered from LTR, 31 (60.8%) from IDR, and the remaining 1 from ER. The mRFS and mOS of the total cohort was 11.0 months (95% confidence interval [CI], 7.573-14.427) and 34.0 months (95% CI, 27.244-40.756), respectively (Figure 3A and B).

Kaplan-Meier curves of patients’ recurrence-free survival (A) and overall survival in total cohort (B) and by level of AFP (C). AFP indicates α-fetoprotein.
Prognosticators of RFS and OS
The ALT ≤40 U/L was a significant favorable prognosticator of RFS compared with ALT >40 U/L on univariate analyses (P = .005, Table 2). Platelets count >100 × 109/L and CA also showed a favorable trend compared with platelets count ≤100 × 109/L (P = .052) and IA (P = .074), respectively, although without statistical significance. On multivariate analysis, ALT ≤40 U/L (hazard ratio [HR], 0.725; 95% CI, 0.502-0.923; P = .018) and 1 tumor lesion (HR, 0.288; 95% CI, 0.103-0.810; P = .018) were independent significant prognosticators of RFS compared with ALT >40 U/L and 3 lesions, respectively (Table 3).
Univariate Analyses of Prognosticators of Recurrence-Free Survival and Overall Survival.

Abbreviations: AFP, α-fetoprotein; ALK, alkaline phosphatase; ALT, alanine transaminase; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; CA1st, complete ablation at first microwave ablation (MWA); CA2nd, incomplete ablation at first MWA but complete ablation at second MWA; CLIP, Cancer of the Liver Italian Program; ER, extrahepatic recurrence; IA, remaining incomplete ablation after 2 sessions of MWA; IDR, interhepatic distant recurrence; INR, international normalized ratio; GGT, γ-glutamyl transpeptidase; HBV, hepatitis B virus; HCV, hepatitis C virus; LTR, local tumor recurrence; PT, prothrombin time; TBil, total bilirubin.
Multivariate Analysis of Recurrence-Free Survival.

Abbreviations: AFP, α-fetoprotein; ALT, alanine transaminase; CA199, carbohydrate antigen 199; CA, complete ablation; CEA, carcinoembryonic antigen; CI, confidence interval; HR, hazard ratio; IA, incomplete ablation; TBil, total bilirubin.
a Tumor number 1 vs 2; AFP ≤20 vs 20-400.
b Tumor number 2 vs 3; AFP 20-400 vs >400.
As for OS, α-fetoprotein (AFP) level was the only significant prognosticators on both univariate and multivariate analyses (Table 2). The mOS of patients with AFP ≤20 ng/mL, 20 to 400 ng/mL, and >400 ng/mL were 36 months (95% CI, 33.356-38.644), 34 months (95% CI, 25.105-42.896), and 23 months (95% CI, 8.708-37.929), respectively (P = .005; Figure 3C). Compared with AFP >400 ng/mL, AFP ≤20 ng/mL (HR, 0.177; 95% CI, 0.057-0.549; P = .003) and 20 to 400 ng/mL (HR, 0.306; 95% CI, 0.117-0.803; P = .016) were independent favorable prognosticators of OS (Table 4).
Multivariate Analysis of Overall Survival.
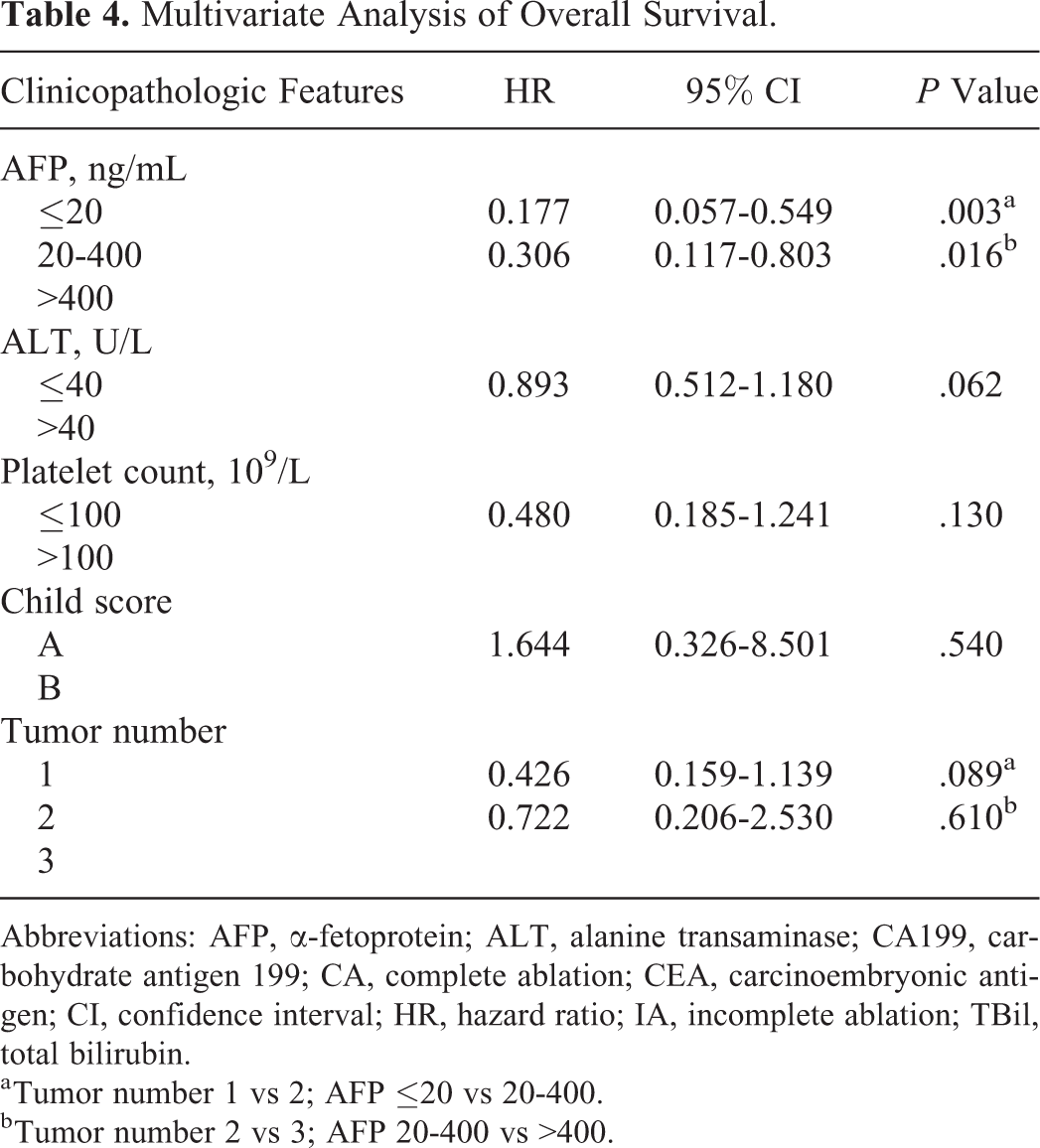
Abbreviations: AFP, α-fetoprotein; ALT, alanine transaminase; CA199, carbohydrate antigen 199; CA, complete ablation; CEA, carcinoembryonic antigen; CI, confidence interval; HR, hazard ratio; IA, incomplete ablation; TBil, total bilirubin.
a Tumor number 1 vs 2; AFP ≤20 vs 20-400.
b Tumor number 2 vs 3; AFP 20-400 vs >400.
Discussion
Thermal ablative therapies such as MWA have emerged as an alternative of hepatic resection and liver transplantation for early and very-early HCC. However, percutaneous RFA was unfeasible in about 25% to 55% of candidates 14 -16 due to unfavorable tumor locations. For example, the local recurrence rate is higher in tumors located at liver surface due to insufficient ablation than in tumors deep in the liver after percutaneous ablation. 12,13,17,18 Moreover, subphrenic tumors unable to be delineated clearly under percutaneous ultrasound are also unsuitable for percutaneous ablation. 14 -16
In these cases, laparoscopic ablation can serve as an alternative option because it possesses several advantages over percutaneous ablation while retaining the minimal invasiveness. First, it allows for improved tumor staging by intraoperative ultrasound and gross examination. 19 Second, it guarantees a safer approach to liver tumors whose locations render percutaneous approach unfeasible or extremely challenging. 20 Recent studies have shown that laparoscopic RFA provides safe treatment for HCC in unfavorable areas such as subcapsular lesions or lesions in close proximity to abdominal viscera. 20 -24 However, the safety and efficacy of laparoscopic MWA on HCC in areas unfeasible for percutaneous ablation remains largely unknown. In this study, we reported our experience of using laparoscopic MWA alone or in combination with percutaneous MWA to treat HCC in these unfavorable areas.
Using laparoscopic MWA on tumors ranging from 1 to 8 cm in areas unfeasible for percutaneous ablation, we gained an initial CA rate of 92.2%, which is higher than or at least comparable to the previous reported CA rates of percutaneous MWA of HCC. 9,25 Si et al, 25 for example, reported a complete response rate of only 42.4% in large (≥5 cm) treated with MWA followed by TACE. In tumors of 3 to 5 cm treated by percutaneous MWA, Zhang et al 9 reported an initial CA rate of 82.61%, and in HCC of 5 to 7 cm. Medhat et al 26 reported an initial CA rate of 73.1%. Given the importance of initial response in survival prediction of HCC as confirmed by multiple studies, 27,28 our results suggest that laparoscopic MWA is an effective strategy for patients with HCC with tumors in areas unfeasible for percutaneous approach.
In these 51 patients treated with laparoscopic MWA, only 3 (5.9%) cases of complications were observed, all of which subsided naturally or after medication. The complication rate in our study is lower than or at least similar to those reported in previous studies of percutaneous local ablative therapies in patients with HCC. In a large cohort study comprising 1305 patients spanning 10 years, 29 for example, the complication rate of patients with HCC following RFA as a first-line treatment was 8.3%. In our another study regarding percutaneous MWA of HCC in more than 200 patients, the complication rate was 10.4% (data submitted).
Patients with HCC >5 cm are not recommended for local ablative therapies in mainstream guidelines 2 with the notion that local ablative therapies are unable to provide CA for the majority of patients with large HCC. In our study, there were 12 patients with tumors >5 cm. These patients received MWA rather than TACE as an initial treatment because their tumors could be clearly delineated under ultrasound and hold a high likelihood to be completely ablated by laparoscopic MWA as assessed by our HCC expert team. Using special ablation techniques (multielectrode, multitract, and multiplanar ablation strategy) and a combination of laparoscopic MWA and percutaneous MWA, we gained a CA rate of 100% (12/12). However, due to the relatively small number of patients with large HCC in our study, future studies with larger patient cohort remain needed to validate our result.
In conclusion, although retrospective in nature, our study is the first to investigate the safety and efficacy of laparoscopic MWA on patients with HCC at liver surface unfeasible for percutaneous ablation. Our study revealed that laparoscopic MWA is well tolerated and effective in patients with HCC at liver surface and identified ALT and tumor number as independent predictors of RFS whereas AFP level as independent predictor of OS. The results of our study suggest that laparoscopic MWA might serve as a rational treatment option for patients with HCC with tumors at the liver surface unfeasible for percutaneous approach, which requires validation in future perspective studies.
Supplemental Material
Supplemental_PDF - Laparoscopic Microwave Ablation of Hepatocellular Carcinoma at Liver Surface: Technique Effectiveness and Long-Term Outcomes
Supplemental_PDF for Laparoscopic Microwave Ablation of Hepatocellular Carcinoma at Liver Surface: Technique Effectiveness and Long-Term Outcomes by Tao Wang, Xiao-Yu Zhang, Xiaojie Lu, and Bo Zhai in Technology in Cancer Research & Treatment
Footnotes
Authors' Note
Tao Wang and Xiao-Yu Zhang are co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.