
Abstract
Background
To analyze the relationship between the rotational and residual setup errors and the dose deviation on nasopharyngeal carcinoma (NPC) treated by helical tomotherapy (HT).
Methods
From 25 July 2017 to 20 August 2019, 16 treated NPC patients were enrolled in the study. These patients were scanned with full target range megavoltage computed tomography (MVCT) every other day. Adaptive radiotherapy function application software MIM7.1.3 were used to accumulate the actual dose. The dose deviation with the initial plan dose of the patients’ target and organs at risk (OAR) were compared, and the correlation between the dose change and the setup errors (rotational setup errors and neck residual setup error) was analyzed.
Results
Translational setup errors increased farther away from the head. Statistically significant difference among 3 groups was achieved in the directions of left-right (P < .001) and anteroposterior (P < .001) by analysis of variance test. Compared with the initial plan dose, the actual accumulated dose of the target area decreased with the actual exposure dose of the OAR increased. However, most of the dosimetric parameters differed by less than 5%. No correlation was found between dose deviation values and the translational setup errors of target. However, sagittal rotational setup errors (pitch) had a positive relationship (P < .05) with the avearge dose of PTVnd (L) (r = 0.885), PTVnd(R) (r = 0.547) PTV1(r = 0.633) and PTV2(r = 0.584). Transverse rotational setup errors (roll) had a positive relationship (P < .05) with the avearge dose of PTVnd(R) (r = 0.593), PTV1(r = 0.505) and PTV2(r = 0.662).
Conclusions
Dose deviation between the actual accumulated and initial plan is not negligible, but most indicators difference is less than 5%, NPC patients treated by HT with MVCT correction setup errors every other day did not need adaptive radiotherapy model unless got rapid tumor shrinkage or weight loss. Moreover, to minimize the dose deviation, more attention should be paid to the reduction of pitch, roll, and residual error of cervical vertebrae during body positioning.
Keywords
Background
Nasopharyngeal carcinoma (NPC) is a malignant tumor that occurs in the epithelial tissue of the nasopharynx. The distribution of NPC in the world is uneven, and it mainly occurs in East and Southeast Asia. The incidence and mortality of NPC in China are higher than the average in the world. 1 Radiation therapy is the most important treatment method. Compared with traditional 2-dimensional and 3-dimensional conformal radiotherapy technique, intensity modulated radiation therapy (IMRT) has become a major treatment modality for NPC. 2 It can generate fields of varied beam intensity which allows the higher radiation dose to be delivered to the tumor while minimizing exposure to the adjacent organs at risk (OAR).
Although the clinical benefits of IMRT for NPC treatment have been confirmed, it does put forward higher requirements for therapy precision related to dose conformity and setup errors. In previous studies, helical tomotherapy (HT) was proved to be the advanced IMRT technology, which provided the most favorable dose sparing of OARs than others.3,4 Moreover, image-guided radiotherapy (IGRT) is often used to verify the setup of isocenter in NPC patients. 5 Registration of cone-beam computed tomography (CBCT) and plan computed tomography (CT) can quantify the setup errors, and patient setup correction was executed by the movement of couch if necessary. It has already been demonstrated that megavolt-level computed tomography (MVCT) was better than CBCT with the superior image definition. 6 Therefore, HT combined with daily MVCT correction maybe the optimal solution to improve radiotherapy accuracy during the entire treatment process.
NPC radiotherapy is usually divided into 30 to 33 fractions, and with the accumulated dose, the shape and geometric centre of the tumor target area and surrounding organs will change significantly.
7
3-dimensional rigid image registration (RIR) method with setup errors to simulate the total dose distribution of head and neck carcinoma was reported
Deformable image registration (DIR) is a process that satisfies this requirement by locally registering image data sets into a reference image set. 10 DIR identifies the spatial correspondence to minimize the differences between 2 or among multiple sets of images. Hence, dose accumulation simulation based on DIR of daily MVCT images may be closer to the actual dose coverage. Thus the purpose of this study was to validate the feasibility of the scheme transmitting daily MVCT images to DIR via automatic positioning and cumulative dose function of MIM software to calculate the difference between the actual cumulative dose and the initial plan dose, and the relationship between rotational and neck residual error and dose deviation were also calculated for analysis.
Methods
Patient Selection
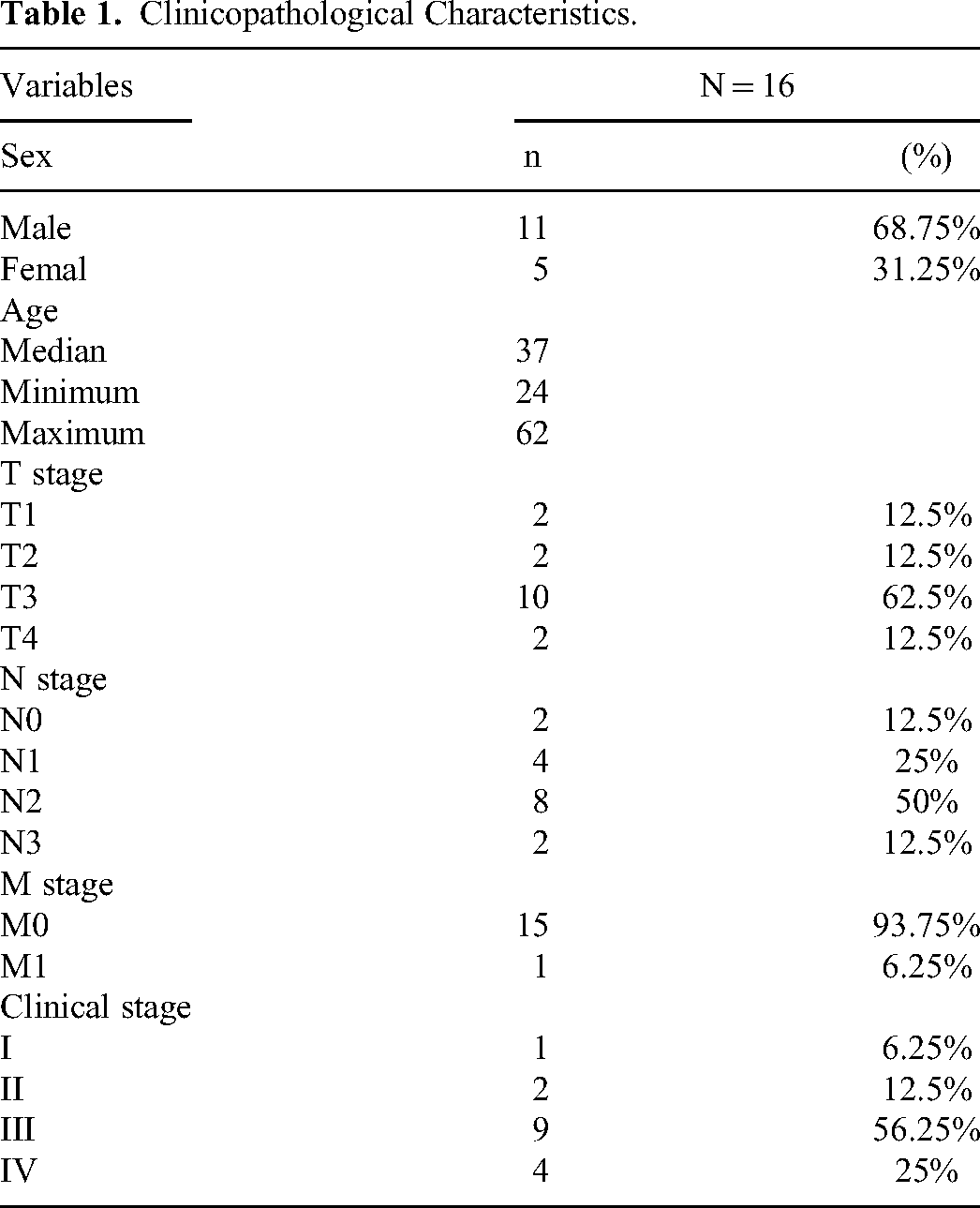
A total of 16 patients with NPC treated with HT in our hospital from 25 July 2017 to 20 August 2019 were enrolled in the study, The general information was shown in Table 1. All patients were confirmed with NPC by pathological examination.
Clinicopathological Characteristics.
Immobilization and Plan Design
All patients were immobilized with a head and neck thermoplastic mask (Klarity) combined with styrofoam (Fu Rui). The patients were scanned by BrillianceTM Big Bore CT (Philips) from frontal sinus upward 2 cm to subclavian 3 cm, and CT simulation was performed with 3 mm slice thickness and 3 mm slice spacing including the head and neck. The target areas and OAR were contoured by 2 or more senior physicians experienced in NPC, and the images and structures were then uploaded to planning system HiArt (version 5.0.6, Accuray, Sunnyvale) for HT plan design.
Acquisition of Setup Errors
MVCT was performed prior to treatment for all patients every other day. The scanning range was the same as CT. After scanning, MVCT images were registered with the planned CT images. The registration region was set as “nasopharynx region ± neck region,” and the registration algorithm is using “Bone and Tissue Technique” automatic registration method. The values of registration error were transmitted for the position correction of the treatment couch in the online calibration of IGRT. However, HT could only correct translational and transverse rotational setup errors (roll), it could not correct the sagittal rotational setup errors (pitch) and coronal rotational setup errors (yaw). In addition, the setup errors of the third cervical vertebra (C3) and sixth cervical vertebra (C6) were obtained separately, and the difference between 2 cervical vertebrae was also calculated. According to radiotherapy, technician's observation of external contour consistency between MVCT and plan-CT. If the deviation is less than the threshold value, start radiotherapy. Otherwise, manual body positioning adjustment and rescan were needed. During the course of treatment, patients were daily checked whether got rapid weight loss (≥ 35%), if so, replan was essential.
Acquisition of Accumulated Dose
Image fusion, dose deformation and accumulation were performed in the MIM (Version7.1.3, MIM Software). The dose on every MVCT image was calculated using corresponding machine record sinogram file. After setup correction, all the reconstructed actual radiation doses were obtained on the MVCT images, then they were fused with the original plan CT as reference images with deformable image registration, and the dose on MVCT image was deformed using the image deformation field. The dose on each MVCT was multiplied by 2 to represent the 2-day accumulated dose, considering that each MVCT image for dose calculation was scanned at every 2-fraction interval. Then, the total actually accumulated delivered dose was obtained by summing each deformed dose multiplied by 2. Dose deviation between the actual accumulated and initial plan was calculated for analysis.
Statistical Analysis
One-way analysis of variance (ANOVA) was performed for setup errors comparison of whole target range. Rank correlation analysis was applied to test the relationship between the average value of setup errors and dosimetric change which is expressed by percentage. All statistical analyses were performed using SPSS software (version 24, SPSS Inc.). The statistically significant level was set as .05.
Results
Translational and Rotational Setup Errors
As shown in Table 2, the translational setup errors were varying due to the different region of interest (ROI) selected for image registration. Compared to the full target area, the translational setup errors values of cervical vertebrae as ROI increased farther away from the head (Figure 1). Statistically significant difference among 3 groups was achieved in the directions of left-right (LR) (P < .001) and anteroposterior (AP) (P < .001) by ANOVA test. When the third cervical vertebra and sixth cervical vertebra are respectively selected as ROI, compared to the full target area, the residual set-up errors (ΔC3 and ΔC6) was shown in Table 3. When the full target area is selected as ROI, the rotational errors in the 3 directions of the patients were obtained using the automatic registration function of HT: pitch (0.41 ± 0.46°), Roll (0.43 ± 0.61°) and Yaw (0.33 ± 0.45°). The average rotation setup errors in the 3 directions are all less than 1°.

Comparison of translational setup errors for different regions of interest (A: LP; B: SI; C: AP). Abbreviations: AP, anteroposterior; LR, left-right; SI, superior-inferior
Comparison of Translational Setup Errors in Different Regions of Interest (mm).
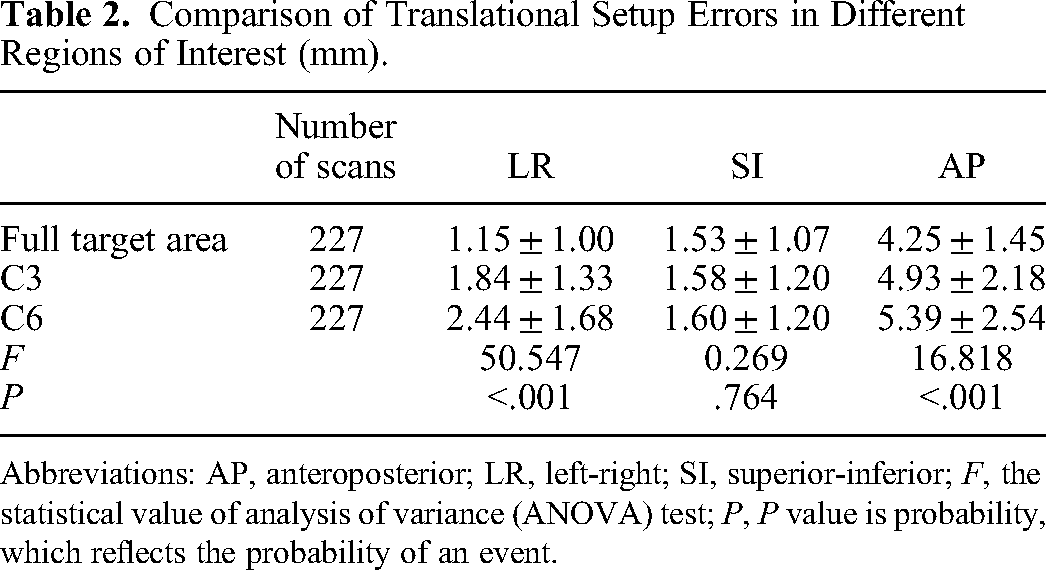
Abbreviations: AP, anteroposterior; LR, left-right; SI, superior-inferior; F, the statistical value of analysis of variance (ANOVA) test; P, P value is probability, which reflects the probability of an event.
Residual Neck Translational Setup Errors (mm).

Abbreviations: AP, anteroposterior; LR, left-right; SI, superior-inferior.
Accumulated Dose Deviation
Average values of deviation percentage in actual irradiation dose and planned dose for the target volume and OAR were as followed: PTVnx-mean ( − 0.17%), PTVnx-V100 ( − 2.8%), PTVnd(L)-mean (0.01%), PTVnd(L)-V100 ( − 3.27%), PTVnd(R)-mean ( − 0.12%), PTVnd(R)-V100 ( − 3.44%), PTV1-mean ( − 0.25%), PTV1-V100 ( − 1.56%), PTV2-mean (0.05%), PTV2-V100 ( − 1.56%), SCMax (3.21%), BSMax (2.59%), parotid(L)-mean (2.43%), parotid(R)-mean (5.67%), TP(L)-V60 (0.12%), TP(R)-V60 (0.45%), ON(L)Max (3.22%), ON(R)Max (3.58%) and OCMax (6.40%). Compared with the initial plan dose, the actual accumulated dose of the target area decreased with the actual exposure dose of the OAR increased (Figure 2). However, most of the dosimetric parameters differed by less than 5% except for right parotid and optic chiasma.

Average dose change percentage of targets and organs at risk.
As shown in Figure 3, the most sensitive dose index was target coverage. A total of 8 out of 16 patients got more than 5% dose deviation of V100 including PTVnx (25%), PTVnd(L) (37.5%), PTVnd(R)(25%), PTV1(6.3%), and PTV2(6.3%), respectively. For OAR, the most sensitive dose index was the hot dose. More than 5% accumulated hot dose deviation of series organs among 16 patients were as followed: SCMax (37.5%), BSMax (18.8%), ON(L)Max (43.8%), ON(R)Max (25%) and OCMax (56.3%).

Percentage change of the actual radiation dose in the target and organs at risk dose.
Correlation Between Setup Errors and Dose Deviation
No correlation was found between the dose change percentage and the translational setup errors of the whole target area. Some dose index deviations were positively correlated with rotation setup errors in pitch and roll (Table 4). Pitch and PTVnd(L)-mean (r = 0.885), PTVnd(L)-V100 (r = 0.868), PTVnd(R)-mean (r = 0.547), PTVnd(R)-V100 (r = 0.612), PTV1-mean (r = 0.633), PTV1-V100 (r = 0.604), PTV2-mean (r = 0.584), and PTV2-V100 (r = 0.735) had a positive relationship (P < .05). Roll and PTVnd(L)-V100 (r = 0.498) PTVnd(R)-mean (r = 0.593), PTV1-mean (r = 0.505) and PTV2-mean (r = 0.662) had a positive relationship (P < .05). The residual setup errors in the AP direction of the third and sixth cervical vertebrae (AP (ΔC3) and AP (ΔC6)) were positively correlated with SCMax (r = 0.647, r = 0.624, P < .05) (Table 5).
Correlation Between Setup Errors and Percent Change in Dosimetric Parameters.

Note: * marked as P < .05, ** marked as P < .01, with statistical significance. Abbreviations: AP, anteroposterior; LR, left-right; SI, superior-inferior.
Correlation Between Residual Neck Translational Setup Error (Anteroposterior [AP]) and SCMax.

Discussion
Previously published studies have revealed that HT achieved significantly better dose conformity to target in the treatment of NPC.11,12 Hence the accuracy of treatment implementation is particularly important. The target areas for NPC radiotherapy include the original nasopharyngeal tumor area and the lymphatic drainage area of the neck. The cervical spine has many joints and can move in multiple directions, so the reproducible positioning of the neck is difficult to maintain. Setup errors in the different cervical vertebra may lead to a significant increase in the SCMax. 13 In this study, a head-neck shoulder mask combined with a styrofoam head-neck pad was used for postural immobilization of patients instead of standardized resin headrests, to fix the NPC body position and neck fixation and combined head, neck and shoulder masks for body position fixation, thereby improving the repeatability of neck fixation. However, the fixation effect of the mask on the neck and chest position is not as good as that of the head, it was found that the setup error of the full target area was statistically significant difference from that of the third and sixth cervical vertebrae in LR and AP directions (P < .001). This observation was consistent with previously published studies.14,15 With the increasing orientation error trend of head to foot, the residual error of the neck can affect the actual dose change. It was shown that a total of 4 out of 16 patients got more than 15% dose deviation of SCMax compared to the initial plan, consistent with Yao et al 16 Correlation analysis revealed the residual error of the third and sixth cervical vertebrae and OAR, and a moderate correlation was noted between residual error and SCMax. Therefore, improving the fixation effect of neck to spare spinal cord in the radiotherapy of NPC remains the direction that needs to be pursued.
In the actual radiation therapy process, translational or rotation errors can affect the actual exposed dose of the target and OAR. Qi et al 17 quantified the translational and rotational errors of patients, and the PTV minimum dose error has an average reduction of 4.4% and 6% in translation and rotation, respectively, and a reduction of 7% in combination. Muurholm et al 18 proved that correcting rotation error by 6-dimensional couch in prostate radiotherapy got better dose distribution than before (3.1%). Our study examined the effects of rotation error on the actual dose deviation of target and OARs in the absence of 6-dimensional couch. Due to mechanical limitations of HT, we only partially corrected translational errors and the transverse rotational setup errors (roll). The sagittal rotational setup errors have a greater impact on the actual dose deviation of the target area far from the central axis, especially for targets with symmetrical distribution of left and right, such as bilateral cervical lymph node target area PTVnd(L) and PTVnd(R), as well as the PTV1 and PTV2 including bilateral lymph node target areas. And, the max dose of the spinal cord, optic chaism, and optic nerves were sensitive to setup errors (Figure 3). Therefore, the manual on-line adjustment requirements for clinical patient positioning should be increased. Otherwise, expanding the margin for bilateral target and serial organs may be an alternative.
A routinely used image registration method for IGRT is RIR, which is highly effective to correct setup errors when no anatomical changes are expected. However, during the entire treatment process of radiation therapy for NPC, the anatomical changes, such as respiration, weight loss, tumor shrinkage and changes in the shape of OAR, are prone to occur during this process and caused intrafractional and interfractional organ movement, 9 which cannot be corrected only by RIR. The intrafractional organ motion is less significant in NPC because there is no organ-in-motion such as lungs and bowel there, and fixed with an individualized immobilization. however, the interfractional organ motion in the head and neck can not be ignored in the actual treatment process. Daily dose accumulation based on DIR of scan-CT with the kV plan-CT maybe a novel strategy. 19 Poon et al 20 proposed an efficient tool to registrar CBCT with planning CT by DIR to stimulate the actual accumulated dose distributions. The greatest percentage difference in observed dose parameters of target was less than 5%. But larger dose deviations were found in OARs such as spinal cord (Dmax: 56.70%) in comparison with target volumes. Esteyrie et al 21 proposed that a daily MVCT offered an efficient workflow for plan adaptation if neccessary. Our study combined MVCT images and DIR, providing an improved tool for the actual and planned dose deviation check. The accumulated dose deviation showed a trend of lower dose in the target area and higher dose in the OARs. However, the dose difference is random in different directions. Most of the target dose index difference was less than 5%, similar to Lu's study. 22 But dose deviation of OARs was almost smaller, except for SC, OC, and ON.
Adaptive radiotherapy (ART) would be particularly useful for some complicated disease sites.23,24 It has several important advantages, including a lower risk of late adverse effects and a potential improvement in disease-free survival, but it is necessary to spend considerable time and energy to explore the appropriate time of ART in NPC radiotherapy. Our results confirmed that most deviations in the calculation of the actual exposure dose to the target area and OARs of NPC patients are less than 5%,which is acceptable for most clinicians. As followed up, the 3-year overall survival rate of 16 enrolled patients was 93.8%, including 1 case with distant metastasis and 1 case with residual lymph nodes. In addition, except for 1 patient with left-side radiation encephalopathy, all the other patients reported only 1–2 grade toxicity. It should be noted that the majority of NPC patients treated by HT with MVCT correction setup errors every other day, didn’t need the ART model unless got rapid tumor shrinkage or weight loss. 25
Conclusions
This study has provided evidence that dose deviation between the actual accumulated and initial plan is not negligible, but most of the indicators difference is less than 5%, NPC patients treated by HT with MVCT correction setup errors every other day didn’t need ART model unless got rapid tumor shrinkage or weight loss. Moreover,to minimize the dose deviation, more attention should be paid to the reduction of pitch, roll, and the residual error of cervical vertebrae during manual body positioning.
Footnotes
Acknowledgements
Many people have offered us valuable help in our study. We would like to give our sincere gratitude to Dr Zhang and Prof. Xia, who gave us great help by providing clinical materials. Moreover, we are pleased to acknowledge Mr Hu for his invaluable assistantance in statistical analysis.
Authors’ Contributions
Senkui Xu designed and supervised the study. Wenyan Yao, Jiang Hu, Peixun Xu, and Mengxue He collected and analyzed the data. Yongwen Fang, Mingzhi Liu, Zongtai Li, Huilang He, Hui Liu, and Xuanguang Chen provided technical assistance for the study. Wenzhao Sun and Senkui Xu wrote the manuscript. All co-authors have reviewed and approved this version of the manuscript.
Availability of Data and Materials
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article. This research was funded by the Medical Science and Technology Research Fundation of Guangdong Province, No.A2020621, the Medical Science and Technology Research Fundation of Guangdong Province, No.A2017613.
Ethical Approval
Our study was reviewed and approved by the Institutional Review Board of Sun Yat-Sen University Cancer Center, with the approval number GYX2020-011.
Informed Consent
Written informed consent for publication of their clinical details and clinical images was obtained from the patient/parent/guardian relative of the patient.