
Abstract
Breast cancer (BC) is the most frequently diagnosed malignancy among women. In the past two decades, new technologies and BC screening have led to the diagnosis of smaller and earlier-stage BC (ESBC). Therefore, percutaneous minimally invasive techniques (PMIT) were adopted to treat patients unfit for surgery, women who refuse it, or elderly patients with comorbidities that could make surgery a difficult and life-threatening treatment. The target of PMIT is small-size ESBC with the scope of obtaining similar efficacy as surgery. Minimally invasive treatments are convenient alternatives with promising effectiveness, lower morbidity, less cost, less scarring and pain, and more satisfying cosmetic results. Ablative techniques used in BC are cryoablation, radiofrequency ablation, microwave ablation, high-intensity focused ultrasound (US), and laser ablation. The aim of our study is to discuss the current status of percutaneous management of BC, evaluate the clinical outcomes of PMIT in BC, and analyze future perspectives regarding ablation therapy in BC.
Keywords
Introduction
Breast cancer (BC) is the most frequently diagnosed malignancy among women, accounting for 28.8% of all cancer diagnoses, and is the second most diagnosed cancer in the world.1,2 Due to increasingly widespread screening campaigns and improved imaging detection rates, the diagnosis of BC occurs in almost half of all cases at earlier stages, when the tumor size does not yet exceed 2 cm. 3 Nevertheless, even for small and low-risk tumors, the gold standard for the treatment of BC is conservative surgery. According to the National Comprehensive Cancer Network 2022 guidelines, the standard treatment for early-stage invasive ductal carcinoma (ICD), involves lumpectomy with sentinel lymph node (SLN) detection followed by adjuvant therapies according to the biology of the tumor. 4 The prognosis after conservative surgical treatment is excellent, and the 5-year survival rate ranges from 98% to 99%. 3
Elderly women with BC are more brittle, have a poor performance status, and tend to preferer conservative therapy instead of surgery. Moreover, in elderly patients, surgery is riskier due to patients’ comorbidities. 4 Furthermore, surgery is associated with complications such as postoperative hemorrhages or infections and results in poor cosmetic outcomes.5,6 Therefore, in the last decades, in parallel to the increasing age of patients with a diagnosis of BC, percutaneous minimally invasive techniques (PMIT) were developed and adopted to either treat patients unfit for surgery or women who refuse it. Minimally invasive techniques used in the treatment of BC are cryoablation (CYA), radiofrequency ablation (RFA), microwave ablation (MWA), high-intensity focused ultrasound (HIFU), and laser ablation (LA). 7 The general advantages of PMIT are lower employment of general anesthesia, lower rates of infectious and hemorrhagic complications, shorter recovery time that would promote an earlier initiation of adjuvant therapies, and better cosmetic results. 8 The aim of our study was to discuss the current status of percutaneous management of BC, evaluate clinical outcomes of PMIT in BC, and analyze future perspectives regarding ablation therapy in BC.
Ablative Therapies in Breast Cancer
The employment of ablative techniques in the treatment of BC is receiving growing scientific evidence, but it still needs more prospective studies and technological advancements to be mentioned in indications for BC treatment. 7 Nowadays, the Food and Drug Administration (FDA) and the American Society of Breast Surgeons (ASBrS) approved for use in clinical practice (level A of evidence) the sole CYA in the setting of benign tumors, such as fibroadenoma. 9 As of today, the indications for these types of treatments take into account patient-related factors (such as performance status, comorbidities, and age) and tumor-related factors, mainly its size, but in some cases its histotype or tumoral component around the lesion have also been considered. 10 Several studies outlined a likely cutoff for the ablative treatment with curative intent of BC: the best results have been obtained when treating small tumors (≤2 cm).8,11 The ablative treatments require a minimum safe distance from the skin surface, which ranges from 0.5 mm during CYA 12 to 1 cm during RFA or MWA 13 and 2 cm during HIFU, 14 in order to avoid skin or muscle burns, the most common complications related to these procedures.
Radiofrequency Ablation in Breast Cancer
Radiofrequency is a widely used local ablative technique that is utilized for the treatment and palliation of different primary and secondary tumors, particularly in the treatment of early stage HCC, and it is still considered the main ablative therapy for HCC lesions smaller than 5 cm in diameter.8,15,16 Its mechanism relies on the administration of radiofrequency after the imaging-guided positioning of one or more electrodes in the whereabouts of the lesion. These electrodes generate radiofrequency waves in the context of an electrical circuit. The circuit is completed with the positioning of grounding pads onto the patient's lower limbs. The generated current induces attrition between ions, increasing tissues’ temperature to an optimal value of 60° to 100°. The resulting thermal energy causes a highly targeted necrotic area, focused on the malignant tissue. 16
In consideration of the pain that may result from the procedure, RFA is mostly performed under moderate sedation or general anesthesia, even though several studies explored the possibility to execute it with local anesthesia,17,18 with minimal discomfort for the patients and an inferior anesthesiologic risk.
In early 2000, several studies demonstrated the feasibility and safety of RFA for the treatment of BC, with low reported complication rates and good technical outcomes. For instance, Burak et al 18 conducted one of the first pilot studies on the subject with the aim of assessing the immediate post-ablation tumor response. Out of 10 tumors ≤2 cm, a pre-treatment MRI scan showed 9 enhancing lesions, 8 of whom showed no residual enhancement at the post-procedural MRI, signaling a good therapeutical response. RFA has been mainly studied in the context of early BC lesions because the ablation of bigger target lesions could lead to either complications derived from an increased radiofrequency administration or to less satisfactory safe-ablation margins, that in feasibility studies were mostly achieved when treating tumors less than 2 to 3 cm. 19 Current treatment strategies for stage I BC include conservative surgical treatments, such as quadrantectomy or localized resections, in fact, RFA has mainly been evaluated in combination with immediate or delayed conservative surgical interventions. In some cases, though, such as in populations of inoperable patients, RFA has been tested without successive surgical excision. Susini et al 20 studied the effects of RFA on 3 elderly high-risk surgical patients, evaluating the discomfort generated by the procedure and the achievement of post-procedural tumor necrosis assessed by both radiological and histopathological examinations. No radiological recurrence was shown 18 months after the treatment. Nevertheless, the treatment of small BC with just RFA raises concerns about the possibility of fully eradicating the tumor. Yamamoto et al 21 conducted a study aimed to further confirmation of RFA's efficacy by performing post-operative MR scans and acquiring multiple vacuum-assisted tissue samples to assess the achievement of safe ablation margins (approximately 1 to 2 cm around ablated BC) histologically free of disease. Twenty-nine patients with ≤2 cm IDC and no signs of extensive duct invasion represented the target population. MRI showed effectively ablated zones in 100% of cases while histological analyses confirmed no viable tumoral tissue in 27 of 29 patients. Albeit no definite cut-off has already been outlined for an RFA treatment of BC, pilot studies showed that full ablation might not be reached in tumors bigger than 3 cm. 22 Two recent meta-analyses have been focusing on lesions ≤2 cm treated with ablative treatments. Xia et al 23 evaluated patients with a BC ≤ 2 cm who underwent RFA, the majority of whom received either tumor resection or radical surgery (65.4%) after treatment; the remaining 34.26% received just RFA. The reported success rate, defined as the correct technical execution of ablation treatment with good patient cooperation, ranges from 86.67% to 100%. Assessment of the ablation rate with MRI and biopsies was performed, with an overall complete ablation rate of 96%. The local recurrence rate was assessed in 232 of 406 cases based on both clinical and imaging evaluations: no events of local recurrence after a median follow-up of 27.29 months were reported, despite undergoing surgical resection following RFA or not. The overall complication rate was 6.80%, confirming the safety of the procedure. No life-threatening complications were reported, the most common ones being relative to skin burns, pneumothorax, and pectoral muscle burns. Van de Voort et al 3 compared the different ablation techniques for the treatment of BC ≤ 2 cm; RFA yielded the highest complete ablation rate (92%), monitored with margin biopsy and MRI. Albeit very high, in both meta-analyses, complete ablation rate with RFA was not achieved consistently: respectively 90% to 94% 3 and 96%. 23 The most common reasons for incomplete ablation account for technical failures (eg, probe placement, inaccurate ultrasound guidance), uncollaborative patients, or operators’ misjudgements (eg, underestimation of tumor size, poor pre-procedural planning) more than linked to limitations of the technique. Data after median follow-ups of 15 to 61 months and 9 to 81 months are encouraging, showing low (up to 0.3% of the analyzed population) rates of local recurrence, evaluated on the basis of clinical and radiological features. Immediate cosmetic outcomes were also satisfactory, but many studies did not report data about aesthetics. 24 These results confirm the promising nature of RFA to treat tumors ≤2 cm with satisfying cosmetic results, few complications, and good local tumor control. Reported studies have been summarized in Table 1.
Ablation Modality, Lesion Type, Lesion Size, Anesthesia, Complications, and Recurrence of BC.

Abbreviations: RFA, radiofrequency ablation; IDC, invasive ductal carcinoma; DCIS, ductal carcinoma in situ; ILC, invasive lobular carcinoma.
MWA in Breast Cancer
MWA is a local hyperthermic ablative technique used to treat different malignancies (liver, lung, kidney, and bone tumors). To date, some studies evaluated the MWA's role in the treatment of BC.27,30 Throughout the years MWA has gained a lot of interest, proving to be an efficacious technique, equal or even superior to RFA in some cases.31,34 Indeed, plenty of studies demonstrated that MWA ablation may offer some advantages over RFA: shorter treatment time, higher intratumoral temperatures, and a larger area of necrosis.7,35,36 MWA heat-generating capabilities depend upon electromagnetic radiation (EMR), which causes a fast-switching rotation at atomic or molecular levels of electric dipoles, mostly water, generating heat by dielectric hysteresis obtained by the friction of water molecules. 37 It follows that MWA is especially effective in tissues with high water concentration; in the context of breast ablation, it is thought that tumor cells are preferentially destroyed, with a relative sparing of normal fatty breast tissue that has a lower water content. 38 MWA is usually more painful than RFA and CYA. It can be performed under local or general anesthesia, or under local anesthesia with intravenous administration of drugs, to achieve a state of sedation. There are no consensus guidelines for the type of anesthesia and each center chooses independently in accordance with its experience.7,39,40 Although there is no state-of-the-art literature on MWA BC ablations, there are some studies that evaluate the efficacy and safety of MWA in the treatment of BC (Table 2). 30 Yu et al published a retrospective cohort study that enrolled 64 patients (21 in the MWA group and 43 in the surgery group) to compare nipple-sparing mastectomy (NSM) and MWA ablation for the treatment of IDC ≤ 5 cm with no direct tumor involvement of the nipple, areola, skin, and pectoralis, and no extensive vascular carcinoma thrombus. 41 Median follow-up was 26.7 months (range, 14.6-62.5 months) and showed one local tumor progression and one ipsilateral breast recurrence, that occurred respectively at 42 and 28 months after MWA, and one ipsilateral breast recurrence and two bone metastases at 31.2, 34, and 30.5 months after NSM. The two groups had no significant difference in tumor progression. No participants in both groups incurred in cancer-related death or major complications. Compared with NSM, MWA achieved similar short-term effects for BC control, better cosmetic satisfaction, and provided an adequate option for elderly patients unfit for surgery. Moreover, Zhou et al published a multicenter clinical study to determine the local effect and antitumor immune response of MWA in the treatment of early-stage BC. 42 They enrolled 35 patients who underwent MWA, and 13 patients diagnosed with invasive BC with similar clinical stages, who only underwent surgery. After MWA patients either underwent surgery or a 1-month follow-up with breast MRI, according to their wishes or medical conditions. After a median follow-up of 36 months (range 13-47 months), complete ablation was confirmed by radiological and anatomopathological examinations in 91.4% of patients. Furthermore, the study shows that compared with surgery, MWA induced significantly increased levels of inducible co-stimulator (ICOS)+ activated CD4+ T cells and serum IFN-γ, indicating a shift in the Th1/Th2 balance toward Th1. In addition, this study shows that MWA could be a trigger of antitumor immunity for BC although the long-term immune response and the effect of this response on clinical outcomes are still unknown.
Ablation Modality, Lesion Type, Lesion Size, Anesthesia, Complications, Recurrence of BC, and Overall Survival.

Abbreviations: MWA, microwave ablation; IDC, invasive ductal carcinoma; DCIS, ductal carcinoma in situ; IBC, invasive breast cancer.
CYA in Breast Cancer
CYA causes cellular death by alternating freezing and thawing cycles via circulating liquid nitrogen or rapid decompression of argon gas. 43 The freezing process starts with the activation of one or more cryoprobes appropriately placed at the center of the tumor through its longest axis to optimize the maximal ice ball length along the cryoprobe, often with intraoperative US guidance. 43
CYA needs a first freeze cycle, followed by a passive thaw, and then a second freeze cycle. The freeze-thaw duration depends on the device, the characteristics of the lesion (such as the size), and the desired ablation margin. 34 In the first freeze, extracellular water freezes earlier because of a higher intracellular osmolarity, causing compensatory extravasation of water from the intracellular to the extracellular environment, which leads to cell dehydration. 44 The osmotic gradient is reversed during the passive thaw, resulting in the swelling and rupture of the cell. A longer thaw after the first cryoablation freeze is believed to be important in maximizing cell damage. 44
CYA has proven to be a feasible treatment modality for benign symptomatic fibroadenomas and IDC in selected cases (Table 3).7,45,46
Ablation Modality, Lesion Type, Lesion Size, Anesthesia, Complications, Recurrence of BC, and Overall Survival.

Abbreviations: CYA, cryoablation; IDC, invasive ductal carcinoma; IBC, invasive breast cancer.
Patients with DCIS and IDC with a notable intraductal component have largely been excluded from studies because of the frequent absence of precise US correlation and the augmented risk of extension outside of the US-targeted ablation zone. 48
The perfect candidate for BC CYA is a low-grade IDC smaller than 1.5 cm without significant intraductal component, hormone receptor-positive, and HER2-negative because those tumors tend to be biologically less aggressive, less likely to be multifocal and multicentric. Moreover, tumors best suited for CYA are located at least 5 mm from the skin (to avoid skin necrosis) and are well visualized on ultrasound. 7
Since the procedure is done percutaneously through a small needle, there is no need for incision or suture and no scars are detected in most of the cases, with good to excellent cosmetic outcomes. 3 To accomplish a complete CYA the expected result is to create a 1 cm margin of ice on all sides of the lesion. 45
In a systematic review and meta-analysis, Mauri et al evaluated studies on the percutaneous ablation of BC with any of the most common techniques. 49 The pooled rate of CYA technical success, defined as the rate of patients in whom the operator was able to technically complete the ablation procedure, was 95% (CI: 90%, 98%); the pooled rate of CYA technical efficacy, defined as the rate of completely ablated lesions, was 75% (51-90%). 49
The American College of Surgeons Oncology Group ACOSOG (Alliance) Z1072 is a phase II, nonrandomized study evaluating the success of CYA in the treatment of invasive ≤2 cm BC, with ≤25% intraductal component and tumor enhancement on MRI. Pathologic review revealed successful CYA in 75.9% of cancers and residual IBC and/or DCIS in 24.1% of patients. Furthermore, if non-multicentric tumors alone had been taken into account, the success rate of target lesion ablation would have been 92%, achieving complete ablation in 80 out of 87 cancers. 47
Habrawi et al made a prospective longitudinal study to evaluate the feasibility of CYA for the treatment of early-stage low-risk BC without tumor resection. 4 They enrolled 11 patients ≥ 50 years old, with early-stage hormone receptor-positive and HER2-negative, unifocal IDC ≤ 15 mm in size without extensive in situ component that was visible at US. All follow-up imaging modalities showed complete ablation of the target zone in 11/11 patients at a median follow-up of 28.5 months (all patients had at least 6 months of follow-up). Four patients (33.3%) have been followed up for ≥ 2 years with no local or residual disease.
In a recent metanalysis, van de Voort et al examined the complete ablation rate for BC ≤ 2 cm using the most common ablation modalities, for CYA complete ablation was reported in 85% (CI: 82%, 89%) of patients. 3
An important ongoing study on the safety and efficacy of CYA on breast cancer is the ICE3 trial, which is a prospective, multicentric, single-arm, non-randomized study including women aged ≥ 60 years old with unifocal IDC, visible on US, ≤1.5 cm in size, classified as low to intermediate grade HR-positive and HER2 negative. The primary outcome is ipsilateral breast tumor recurrence (IBTR) at 5 years. A 3-year mid-term analysis was performed to evaluate the outcomes at an intermediate follow-up period. It was found that with a mean follow-up of 34.83 ± 17.96 months (range, 0.07-67.55 months), the overall IBTR rate was 2.06% (4/194 patients; 95% CI: 0.56, 5.19), without reporting severe device-related adverse events. Satisfactory cosmetic results were achieved according to the 95% of the patients and 98% of the physicians. Promising data on local disease control were also obtained; in this population appear to be similar to that of surgery but with fewer complications related to the operation, better cosmetic results, and shorter recovery time. 50
The specific advantages of CYA are that often it only needs local anesthesia because the freezing provides additional analgesia, its minimal invasiveness, and short post-procedural hospitalization times.
Disadvantages are the cost, particularly when multiple probes are used, and the fact that procedures can take more time than other methods (average time of 45 min).43,51
Among complications, the most feared is skin necrosis, which is an uncommon potential issue with experienced operators and can be mitigated by a hydro-dissection between tumor and skin. Other possible complications are infection, bleeding, and injuries to the chest wall. 7
Interestingly, recent studies suggest that CYA may augment the expression and immunogenicity of tumor neoantigens, which could increase the ability of the immune system to recognize and kill cancer cells at both local and distant sites. 52
HIFU in Breast Cancer
HIFU is a noninvasive technique, performed without any skin opening, used in both nononcological and oncological settings for many cancers (prostate, bone, kidney, liver, pancreas, etc) including BC. HIFU converges the thermal energy of high-intensity focused US (1-7 MHz) delivered by a piezoelectric transducer into a small volume of tissue (0.8 × 0.2 × 0.2 mm3), defined as the “focal zone,” resulting in a rapid (1-2 s) rise in temperature to 50 °C to 95 °C, causing coagulative necrosis. 11 Indeed, depending on temperature, HIFU can generate thermal effects and mechanical effects respectively reaching <55 °C hyperthermia that hence increases capillary permeability, facilitating the passage of carrier molecules (sonoporation), useful for drug delivery; on the other hand, temperatures >55 °C cause irreversible cell death. 53 The targeted area is mapped by diagnostic US or, preferably, by MRI. The accuracy of targeting is verified in real-time with US, as the focal area becomes hyperechoic, while with MRI, thermosensitive sequences are acquired at a later time. 11 The patient is positioned in prone decubitus with the breast suspended in degassed water (to minimize artifacts and beam attenuation) or gel for acoustic coupling.11,53 Conscious sedation, a pectoralis major block, or a combination of local anesthesiologic techniques can be useful to reduce the pain. The transducer is placed under or to the side of the breast. For US guidance, an elliptical HIFU therapeutic probe (12 cm in diameter) is used with a conventional imaging probe positioned in the center. For MRI guidance, a dedicated system has been developed specifically for HIFU treatment of BC and currently the most commonly used devices are the ExAblate 2000 and 2100 systems designed by InSightec-TxSonics Ltd (Haifa, Israel, and Dallas, TX) and the Sonalleve MR HIFU system (Sonalleve, Philips Healthcare, Vantaa, Finland).54,55
The possible indication for HIFU can be ESBC < 2 cm. 56 Guan et al analyzed 57 25 BC patients treated with HIFU. The endpoint was to evaluate recurrence, based on hematoxylin-eosin (HE) staining, elastic fiber staining by Victoria blue and Ponceau's histochemical staining, and vascular endothelial cell immunohistochemical staining with biotinylated-ulex europaeus agglutinin I. During a follow-up time of 12 months, no local recurrence or distant metastatic lesions were detected, and histological examination demonstrated that HIFU ablation can destroy all proliferating tumor cells and their growing vascularities simultaneously. In consideration of the short follow-up period, the overall survival of HIFU treatment investigation in this study will be continued (Table 4). 57
Ablation Modality, Lesion Type, Lesion Size, Anesthesia, Complications and Recurrence of BC.
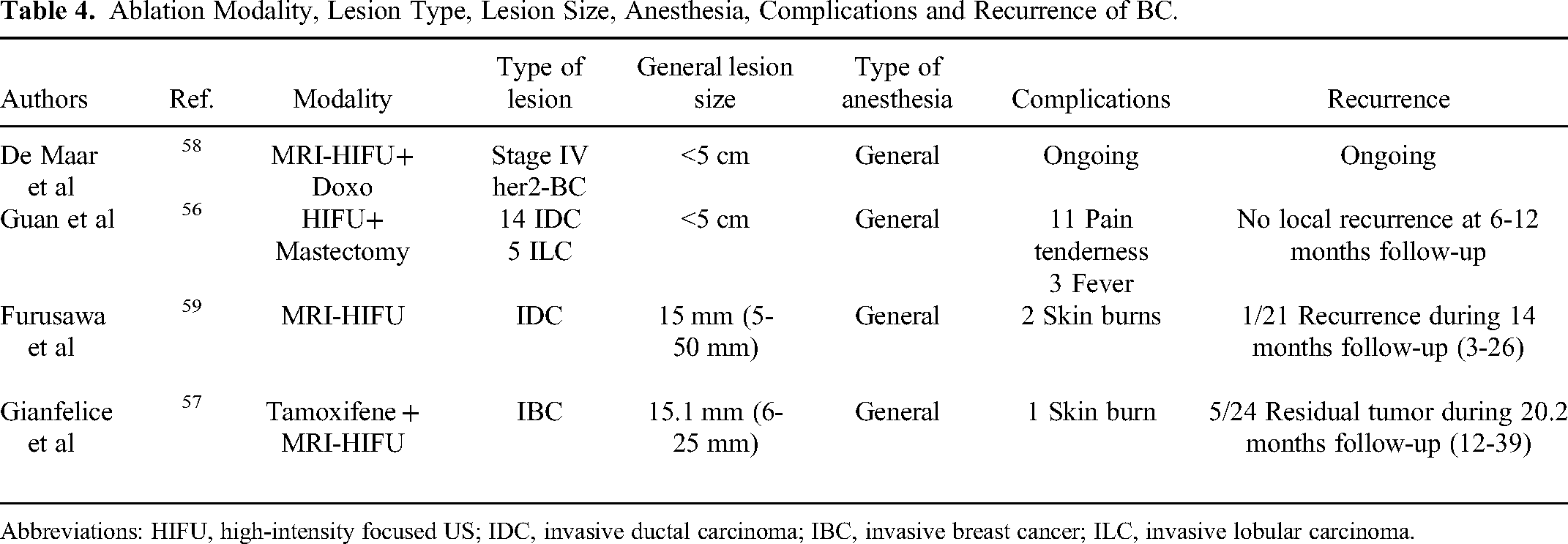
Abbreviations: HIFU, high-intensity focused US; IDC, invasive ductal carcinoma; IBC, invasive breast cancer; ILC, invasive lobular carcinoma.
In a Chinese Clinical Experience reported by Wu et al, 22 patients with malignant BC (stages I to IV) were enrolled. Patients were treated with ultrasound-guided HIFU as an adjunct to chemotherapy, radiotherapy (RT), and tamoxifen. The safety margin was 1.5 to 2 cm around the ultrasound visible tumor. Post-procedural biopsy revealed coagulation necrosis of the entire target tumor in all cases (100%). After a median follow-up of 55 months, one patient died (5%) and two patients (9%) developed local recurrence. All patients were still alive in the follow-up time and all but one resulted disease-free. The 5-year disease-free survival (DFS) was 95%. 57 Lin et al metanalysis 59 evaluated the potential application of HIFU ablation on BC and showed that a pooled technical success of HIFU of 98%, highlighting that the surrounding ablation margin must be more than 1.0 cm to achieve a technical efficacy of 95%. HIFU complications mostly consist of local skin reactions, pain, hemorrhages, post-procedural nausea and vomiting, and nonpathological enlargement of loco-regional lymph nodes. In case of skin reaction, hydro-dissection or lidocaine-dissection can be a protective method. 59
Gianfelice et al enrolled 24 patients with BC at increased surgical risk, who underwent MR-HIFU ablation associated with chemotherapy with Tamoxifene. The endpoint was to rule out metastatic disease through routine clinical and MR studies (10 days and 1, 3, and 6 months after the treatment session). Percutaneous biopsy was performed after a 6-month follow-up, and if residual tumor was present, a second MR imaging-guided focused US surgery treatment session was performed, followed by a repeat biopsy 1 month later. Results demonstrated that 19 of 24 patients had negative biopsy results after one or two treatment sessions and only one patient had a side effect (second-degree skin burn resolved with local treatment). All patients remained free of metastatic disease on routine follow-up physical examinations, imaging, and blood analysis (mean follow-up 20.2 months; DFS 100%; Table 4). 60
Another clinical trial by Furusawa et al evaluated the feasibility of this technique, enrolling 21 patients with invasive/noninvasive ductal carcinoma, who underwent MR-HIFU ablation. Recurrence was evaluated with follow-up every 3 months with MRI, US, and core needle biopsy. After a median period of observation of 14 months, only one case of recurrence (mucinous carcinoma) was observed (DFS 95%) and only 2 cases of skin burn were reported. 61
Nevertheless, HIFU has disadvantages as its sensitivity to patients’ movement can lead to incomplete target ablation or collateral damage such as near-field heating. In fact, a well-designed immobilization covering the complete breast is recommended in order to reduce movements.58,62 Another limit is the duration of the procedure, which can last several hours.
In addition, HIFU enables the guidance of drug injection; in fact, in a phase I feasibility study, de Maar et. al enrolled 12 chemotherapy-naïve patients with de novo stage IV Her2 negative BC that underwent 6 cycles of Lyso thermosensitive Liposomal Doxorubicin (LTLD) administered during MR-HIFU induced hyperthermia. 63 The primary endpoints were safety and tolerability of MRI-HIFU plus Doxorubicin based on the incidence and severity of eventual adverse events, the incidence of dose-limiting toxicity, the necessity for dose adjustments, delay, or early cessation, and finally incidence and severity of postprocedural pain. Feasibility was evaluated with the number of cycles in which hyperthermia treatment was deemed sufficient, the quality of MR thermometry data acquired during the MR-HIFU treatment, and the total duration of the studied procedures on a treatment day. Secondary endpoints were efficacy parameters based on the assessment of distant radiological objective response rates. A significant overall survival benefit for the combination treatment (HR for overall survival 0.63 [C.I. 95%], in favor of RFA + LTLD with ≥45 min heating was observed. The study is still ongoing with the aim of further demonstrating its safety and effectiveness [Table 4]).
LA in Breast Cancer
Percutaneous LA represents a minimally invasive method with great potential in the management of ESBC, capable of treating the tumoral area while minimizing side effects on surrounding healthy tissue. A cooled laser fiber guided by imaging (mammography, US, or MRI), is inserted percutaneously until it reaches the tumor site, which is destroyed as a result of heat production. 64 Laser electromagnetic radiation causes thermal damage because, at the interface between laser radiation and biological tissue, photons of laser light are absorbed by surrounding tissue molecules, causing excitation and release of thermal energy, with a sudden rise in tissue temperature and irreversible damage to cell and tissue architecture. 65 To achieve proper tissue penetration, wavelengths between 590 and 1064 nm must be used. 65 There are two main lasers used today: diode lasers (wavelength between 800 and 980 nm) and the continuous Nd:YAG laser (wavelength of 1064 nm). Dowlatshahi et al, 7 years after a pilot study of 36 patients, enrolled 54 patients diagnosed with in situ or invasive BC who underwent LA; surgical removal of the treated area was performed over a period of 1 to 8 weeks. The primary objective of the study was to evaluate the rate of complete tumor ablation with laser therapy alone, implementing certain technical precautions that in his previous study were partly considered the reason for the technical failure. The authors demonstrated that no major post-procedural complications occurred in any patient, and the overall success rate for complete tumor ablation was 70%. The main reasons behind treatment failure were the inadequate application of laser energy (<60°), technical difficulties (malfunctioning thermal probes, fluid pump), suboptimal visualization of the target, typically occurring after the injection of anesthetic around the target lesion, and the size of the tumor itself (above 2 cm). 100% technical success was achieved in all those cases where these issues were corrected or did not occur (Table 5). 66
Nori et al evaluated the feasibility of echo-guided laser treatment of unifocal BC: they recruited 12 elderly patients unfit for surgery, with breast tumors no larger than 2 cm in size. 1 Complete LA was achieved in 100% of the cases, with no major post-procedural complications and optimal cosmetic results (Table 5). After treatment, these patients were monitored with a median follow-up time (by ultrasound and mammography) of about 28.5 days (range 6-51 months) and no progression or recurrence of disease was noted. 1
Van Esser et al, in their study, enrolled 14 patients with palpable invasive BC diagnosed by needle biopsy who underwent LA; the efficacy of the treatment was assessed by reviewing histological staining (HE and nicotinamide adenosine diaphorase) of the surgical piece excised after ablative treatment. The results showed that the tumor was completely excised in 50% of patients and that was completely ablated in 88% of patients with a lesion less than 2 cm in size. From the obtained results, therefore, the technical success of laser treatment of BC appears to be obtainable when confined to the treatment of nonlobular, small carcinomas without extensive angioinvasive growth (Table 5). 5 In fact, laser ablation should be excluded for certain tumor histologies, since lobular carcinoma has a diffuse growth pattern that is more extensive than what is seen with imaging, 5 and in tumors with extensive angioinvasive growth. This feature cannot be studied with mammography or ultrasonography, so it is necessary to improve preoperative evaluation, for example, by resorting to the use of MRI. Haraldsdóttir et al evaluated the technical aspects of Interstitial laser thermotherapy (ILT) as a method for the local treatment of BC. A total of 24 patients, most of whom were diagnosed with ICD, but including others with lobular carcinoma and only one with lobulo-ductal carcinoma, were treated.. The maximum tumor diameter, measured by ultrasound, ranged from 5 to 35 mm. On average, standard surgical excision was performed after 12 days. In general, the procedure was well tolerated, with no major complications. In the follow-up, 13 and 58 months after ILT, 21 patients showed no recurrence of disease; 2 of them died after 1 year due to metastatic disease; while one patient had to receive chemotherapy after treatment, she presented with positive axillary lymph nodes and distant spread on admission; (OS 91.5%; DFS 87.5%). 67 In conclusion, LA is a feasible and effective option in selected patients who are not candidates for surgical treatment.
Ablation Modality, Lesion Type, Lesion Size, Anesthesia, Complications, Recurrence of BC and Overall Survival.
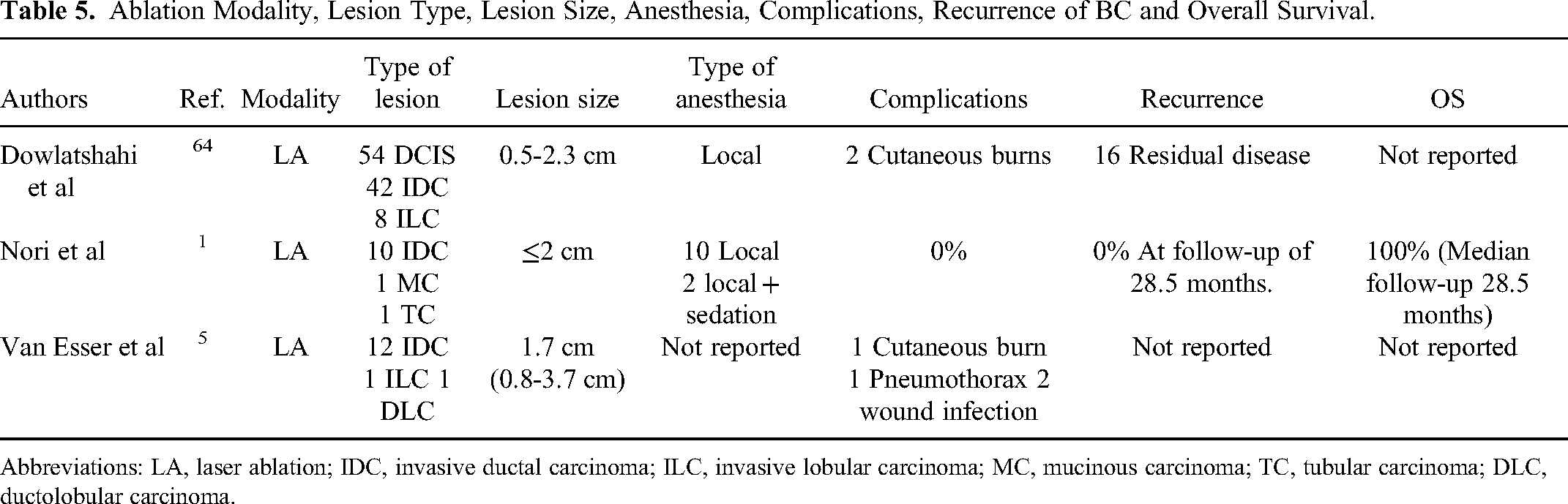
Abbreviations: LA, laser ablation; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma; MC, mucinous carcinoma; TC, tubular carcinoma; DLC, ductolobular carcinoma.
Breast Cancer Ablation and Immunotherapy
Nowadays it has been demonstrated that there is a relationship between ablation and immune response. 68 It has been observed that CYA favors the formation of a pro-inflammatory environment that induces the release of antigens that activate a tumor-specific immune response. 52 Based on this, a low number of studies have evaluated the efficacy and safety of combining CYA with target therapy based on the use of monoclonal antibodies or checkpoint inhibitors (ICI). 52 A randomized phase II study by McArthur et al compared the peri-operative combination of checkpoint inhibitors Ipilumab (anti-PD-L1) + Nivolumab (anti-CTLA-4) + Cryoablation versus definitive surgery for residual (>1.0 cm) operable triple-negative ESBC after taxan-based neoadjuvant chemotherapy. The primary endpoint is 3-year event-free survival. Secondary endpoints include invasive DFS (iDFS), distant DFS (DDFS), overall survival (OS), and safety. The study is ongoing but has so far shown that the combination of cryoablation with Nivolumab-Ipilumab is safe and induces a strong intra-tumor and systemic immune response. 69 The study by Habibi et al evaluated the efficacy of combining RFA with intratumoral administration of IL7 and IL15, injected after RFA, in murine tumors differentiated into neu-over-expressed mammary carcinoma and 4T1 tumors. The combination of RFA + IL7/IL15, as demonstrated in the murine models, improves the induction of anti-tumor immune responses and results in the inhibition of tumor recurrence or metastasis, and reduces myeloid-derived suppressor cell. 70
Also, HIFU can trigger an anti-tumor immune response. Zhu et al enrolled 48 patients with BC divided into two groups (HIFU and mastectomy) to evaluate the immune response after HIFU for tumor-draining lymph nodes (TDLNs). The study showed that in the HIFU group, axillary LN had a greater immune reaction than in the control group (100% vs 64%). 71
A phase I clinical trial by the University of Virginia is currently underway to examine the combination of Pembrolizumab either before or after HIFU, in patients with advanced/metastatic BC (R). 72 Complete response was 64.8% in the pembrolizumab–chemotherapy group and 51.2% in the placebo–chemotherapy group. After a median follow-up of 15.5 months, 58 of 784 patients (7.4%) in the pembrolizumab–chemotherapy group and 46 of 390 patients (11.8%) in the placebo–chemotherapy group had disease progression that precluded definitive surgery, had a local or distant recurrence or a second primary tumor, or died from any cause. Across all treatment phases, the incidence of treatment-related adverse events of grade 3 or higher was 78.0% in the pembrolizumab–chemotherapy group and 73.0% in the placebo–chemotherapy group, including death in 0.4% (3 patients) and 0.3% (1 patient), respectively. With 104 events, Kaplan–Meier estimated the 18-months percentage of patients who were alive without disease progression that precluded definitive surgery, without local or distant recurrence, and without a second primary tumor, obtaining 91.3% in the pembrolizumab–chemotherapy group and 85.3% in the placebo-chemotherapy group. 73
A final mention must be reserved to RT, which has also been shown to modulate the antitumor immune response. Cirincione et al evaluated the efficacy of HIFU on one hand at increasing tumor radiosensitivity, thus reducing the dose of RT, and on the other hand at inducing a specific antitumor immune response in association with immunotherapy approaches. Indeed, it has been observed as how the mechanical HIFU treatment can augment anti-tumor immune response by inhibiting STAT3 activity and this could be one of the beneficial effects of combining HIFU and RT treatments, in order to improve rates of tumor radio-sensitivity and reduce the RT inflammatory–mediated side effects.
Conclusion
Image-guided thermal and nonthermal ablative techniques such as RFA, MWA, CYA, LA, and HIFU are promising therapeutic options for BC in a selected population. PMIT can be adopted to treat patients unfit for surgery, women who refuse it, or elderly patients with comorbidities judged unfit for surgery. The advantages of these techniques are less morbidity, less cost, less scarring and pain, and better cosmetic results. Nevertheless, only a few up to date studies are available about BC ablation, and prospective studies are strongly needed to better understand the potential role of ablative techniques for local treatment of early BC. Technological advances, prospective studies comparing ablative techniques to the standard of care and longer follow-ups are necessary in order to further confirm the value and safety of the ablative techniques.
Footnotes
Acknowledgments
None.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.