
Abstract
The evaluation of megakaryocytes is an important part of the work up on bone marrow smear examination. It has significance in the differential diagnosis, therapeutic efficacy assessment, and predication of prognosis of many hematologic diseases. The process of manual identification of megakaryocytes are tedious and lack of reproducibility; therefore, a reliable method of automated megakaryocytic identification is urgently needed. Three hundred and thirty-three bone marrow aspirate smears were digitized by Morphogo system. Pathologists annotated megakaryocytes on the digital images of marrow smears are applied to construct a large dataset for testing the system's predictive performance. Subsequently, we obtained megakaryocyte count and classification for each sample by different methods (system-automated analysis, system-assisted analysis, and microscopic examination) to study the correlation between different counting and classification methods. Morphogo system localized cells likely to be megakaryocytes on digital smears, which were later annotated by pathologists and the system, respectively. The system showed outstanding performance in identifying megakaryocytes in bone marrow smears with high sensitivity (96.57%) and specificity (89.71%). The overall correlation between the different methods was confirmed the high consistency (r ≥ 0.7218, R2 ≥ 0.5211) with microscopic examination in classifying megakaryocytes. Morphogo system was proved as a reliable screen tool for analyzing megakaryocytes. The application of Morphogo system shows promises to advance the automation and standardization of bone marrow smear examination.
Introduction
The bone marrow (BM) is the body's primary hematopoietic organ. Quantitative and qualitative changes of BM cells result in various hematologic malignancies, making BM examination particularly important, and even decisive, for the diagnosis and follow-up care of many hematological conditions.1,2 Hematopathologists examine BM smears by the microscope, classify and count nucleated cells, calculate the granulocyte to erythrocyte ratio, and count visible megakaryocytes on the whole smear. This is a tedious and time-consuming process requiring a high level of professional skills, and the microscopy results are limited by the inter- and intra-observer variability. 3 To improve the quality and efficiency of BM examinations in clinical settings, it is urgent to improve the consistency and automation of cell counts.
Currently, blood cell analysis devices have automated cell counts in peripheral blood and cerebrospinal fluid.4,5 The complexity of BM smears makes it difficult to accurately frame the target cells from the stacked cells, resulting in a lag in the automation of BM smear examination. 6 The deep application of artificial intelligence (AI) techniques, especially convolutional neural networks (CNN), in the field of medical image processing has made it possible to automate BM examination. Studies have confirmed that the watershed algorithm and support vector machine (SVM) exhibit superior segmentation and classification performance in detecting BM cells. 7 The accuracy of Mask R-CNN to detect and classify BM nucleated cells improves with the expansion of the training dataset. 8 However, related studies have focused more on the development of BM cell detection algorithms, which are not adapted to analytical devices and have limited clinical applicability. The BM cell morphology analysis system (Morphogo) with CNN and whole slide imaging is one of the few devices suitable for BM smear examination. 9 A pilot study showed that Morphogo identified BM nucleated cells with an overall accuracy of 90.1%, highly consistent with the proportion in the cell lines obtained by microscopy. 10 Based on this device, we attempted to address the automated analysis of BM megakaryocytes by constructing CNN algorithms. To complement the automation of whole-slide counting and classification of megakaryocytes not involved in BM examination studies.
The examination of megakaryocytes in BM smear is important for the diagnosis, therapy, efficacy observation, and prognosis of hematologic malignancies as well as the determination of BM transplantation outcomes. 11 Megakaryocytes, being very rare large cells (50-100 μm), represent only 0.05% of the total number of cells in human BM, and their proliferation is strictly controlled. 12 Therefore, the deviations in megakaryocyte quantity and quality may indicate the progression of myeloproliferative neoplasms (MPN) and other pre-leukemic disorders. 13 In this study, an automated CNN-based megakaryocyte analysis tool was developed, allowing a standardized assessment of whole-slide megakaryocytes for the first time. It assists physicians in disease diagnosis and prognostic stratification by replacing pathologists in completing whole-slide counting and classification of megakaryocytes in BM examinations and is expected to provide new indicators or techniques for the diagnosis and monitoring of hematologic malignancies.
Materials and Methods
This is a retrospective clinical study. BM smears were scanned and digitized by Morphogo system. Based on digital smears, pathologists annotate megakaryocytes in the whole smear. The system localized the whole-slide megakaryocytes by localization algorithm. The localized cells were identified as megakaryocytes or not by classification algorithm with 40× objective. Then, 25 megakaryocytes were classified with 100× oil lens. Finally, the automated analysis results of BM megakaryocytes were generated. The workflow of Morphogo system has shown in Figure 1. The megakaryocyte annotation data for the pathologist and the system, as well as the megakaryocyte examination data on the case reports, are available in the electronic Supplemental Material.
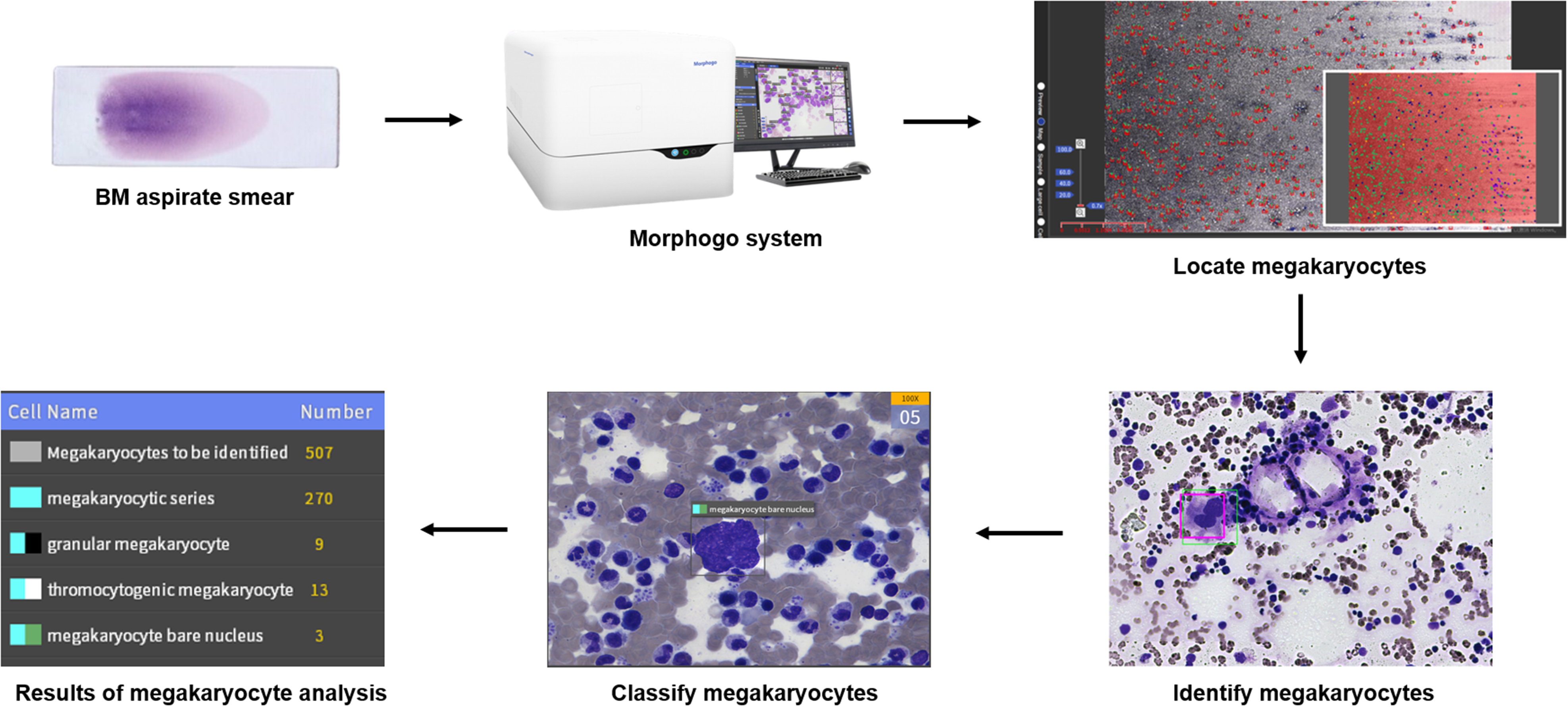
Workflow of Morphogo system for examination of megakaryocytes in BM smears.
Clinical Sample
We retrospectively collected BM smear samples from the patients diagnosed in Sir Run Run Shaw Hospital affiliated with Zhejiang Medical University from 2016 to 2021. All patients did not receive relevant treatment prior to BM examination. A total of 333 samples were divided into five groups: chronic myeloid leukemia (CML, n = 54), essential thrombocythemia (ET, n = 49), immune thrombocytopenia (ITP, n = 30), acute leukemia (AL, n = 100), and control group (n = 100). Samples of the control group were obtained from patients with normal BM characteristics. The patients with CML, ET, ITP, and AL met the diagnostic criteria of the latest WHO classification (2016). 14 All smears were well stained using the Wright-Giemsa method. Preparation quality was consistent with the requirements of the International Committee for Standardization in Hematology. 15
Instrument
Morphogo system (Zhiwei Information Technology Co., Ltd Hangzhou, China) consists of hardware and software. The hardware part consists mainly of an automatic scanner and a computer. The scanner was fitted with a microscope unit with a 40× objective (Plan N 40×/0.65 FN22, resolution 0.42 μm, Olympus, Japan), a 100× oil lens (Plan N 100×/1.25 FN22, resolution 0.22 μm, Olympus, Japan), and a camera with 4000 × 3000 pixels (E3ISPM12000KPA with 12MP 1/1.7″ (7.40 × 5.55) SONY Exmor CMOC Sensor (ToupCam, China). The software part consists of an acquisition terminal, a review terminal, and a consultation terminal. Morphogo system acquires high-resolution images of BM smears through the scanner, performs image stitching at the acquisition terminal to obtain digital smears, and acquires cell images. Based on CNN, Morphogo system analyzes the cell images and identifies megakaryocytes in the image. Users can review the cell identification results at the review terminal and communicate the results of BM smear analysis at the consultation terminal.
Algorithm Development and Training
We referenced existing works in computer vision to construct a robust algorithm for megakaryocyte localization and recognition. Existing neural network architectures are designed for general image recognition with objects that vary significantly in color, texture, and size. Whereas cell localization, as a downstream task with a low tolerance to errors, requires a more carefully designed pipeline to fully capture the morphological features of megakaryocytes and eliminate issues caused by cell image overlay. We designed a convolutional network consisting of a localization algorithm and a classification algorithm (Figure 2), which was deeply optimized based on the characteristics of megakaryocytes mainly from four aspects: (1) The size of pre-defined anchor boxes is optimized to match the scale of megakaryocytes. (2) Random rotations, crops, flips, and color jittering in the data augmentation stage are redesigned to fit cell images. (3) We integrated the idea of rotated object detection considering the rotational invariance of cellular images. (4) We added a series of post-processing steps after Non-Maximum Suppression: we used the Watershed algorithm to resolve image overlay, followed by a clustering approach to separate megakaryocytes. We trained our network on more than 1 million cell images collected from digital smears and then fine-tuned them to adapt megakaryocyte-related tasks. Megakaryocyte images as well as images of cells similar to megakaryocytes were used to test the network, with 65 746 cell images used for localization testing and 64 936 cell images used for recognition testing. Results revealed strong representational capability and robustness of our pipe.
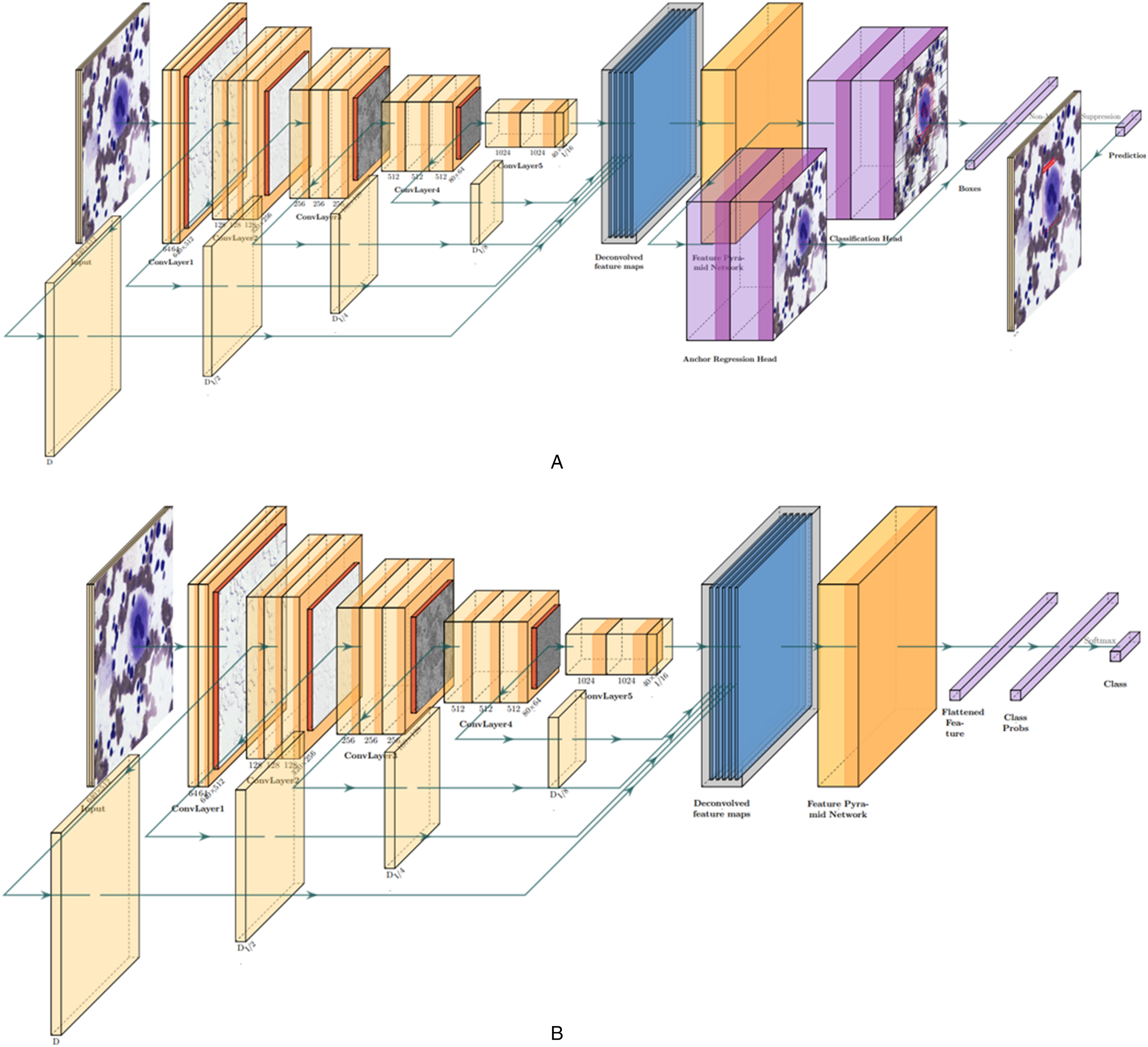
CNN structure of the bone marrow megakaryocyte detection algorithm. (A) Megakaryocyte localization algorithm. (B) Megakaryocyte classification algorithm.
Preliminary Testing
The generalization ability of the AI model needed to be tested using a new dataset. Three hundred and thirty-three BM smears were digitized by Morphogo system and submitted to pathologists to annotate megakaryocytes. Digital images containing megakaryocytes were transmitted to Morphogo system as the test data. When the system recognized pathologist-annotated megakaryocytes, they were categorized as true positive (TP) data. Conversely, they were categorized as false negative (FN) data. Due to the presence of other cells in the digital images, when the system identified them as megakaryocytes, they were categorized as false positive (FP) data. The performance of Morphogo system in identifying megakaryocytes was evaluated using precision, and F1-score.


Performance Validation of Whole-Slide Megakaryocyte Counting
For each BM smear, the results of whole-slide megakaryocyte count were obtained by three methods to assess the correlation between megakaryocyte counting methods. Morphogo method: Morphogo system detects megakaryocytes from BM smear and automatically counts whole-slide megakaryocytes. Manual method: The pathologist annotates megakaryocytes on digital smears to obtain the total number of megakaryocytes per smear. Microscopy method: Whole-slide megakaryocyte counts are obtained from the patient's pathology report.
Performance Validation of Megakaryocyte Classification
Megakaryocytic series included megakaryoblasts, promegakaryocytes, granular megakaryocytes, platelet-producing megakaryocytes, and nude-nuclear megakaryocytes. The cell ratios of different megakaryocyte types were obtained by Morphogo and microscopy, respectively, to assess the consistency of the two methods of megakaryocyte classification. Morphogo method: Morphogo automatically classifies 25 megakaryocytes in the region of interest (ROI) with 100× oil lens and is reviewed by pathologists. For BM smears with megakaryocytes number ≤25, classification of all megakaryocytes is required. Microscopy method: the cell ratios of different megakaryocyte types were obtained from the pathology report of patients.
Statistical Analysis
The results of megakaryocyte count in each group were described in the form of mean ± standard deviation (SD). The accuracy test was performed using confusion matrices, and the correlation coefficient was determined by the Pearson correlation test. All analyses were conducted with Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and GraphPad Prism 6 (GraphPad Software Inc., San Diego, CA, USA). All tests were performed using a two-tailed t-test, with P < .05 indicating statistical significance.
Results
Morphogo System Detects Megakaryocytes with High Sensitivity and Specificity
BM smears were scanned by Morphogo to generate high-definition digital images, and the pathologist annotated megakaryocytes at the distribution interface of the digital smears (Figure 3A). In Figure 3B, we show the annotation of megakaryocytes by the pathologist on BM smears from different case sources under a 40× objective. This facilitated to effectively construct a large dataset containing 79 712 megakaryocytes, which was used for testing the generalization ability of the AI recognition model of Morphogo system. We obtained Morphogo's recognition results for megakaryocytes in the test dataset, using precision and recall to evaluate the predictive performance of the system for the new dataset. We found that the precision and recall of Morphogo system for recognizing megakaryocytes in the test dataset were 82.88% and 82.53%, respectively (Table 1). Overall, Morphogo system was able to identify megakaryocytes with high precision and recall, which is a good balance between accuracy and completeness of megakaryocyte detection.
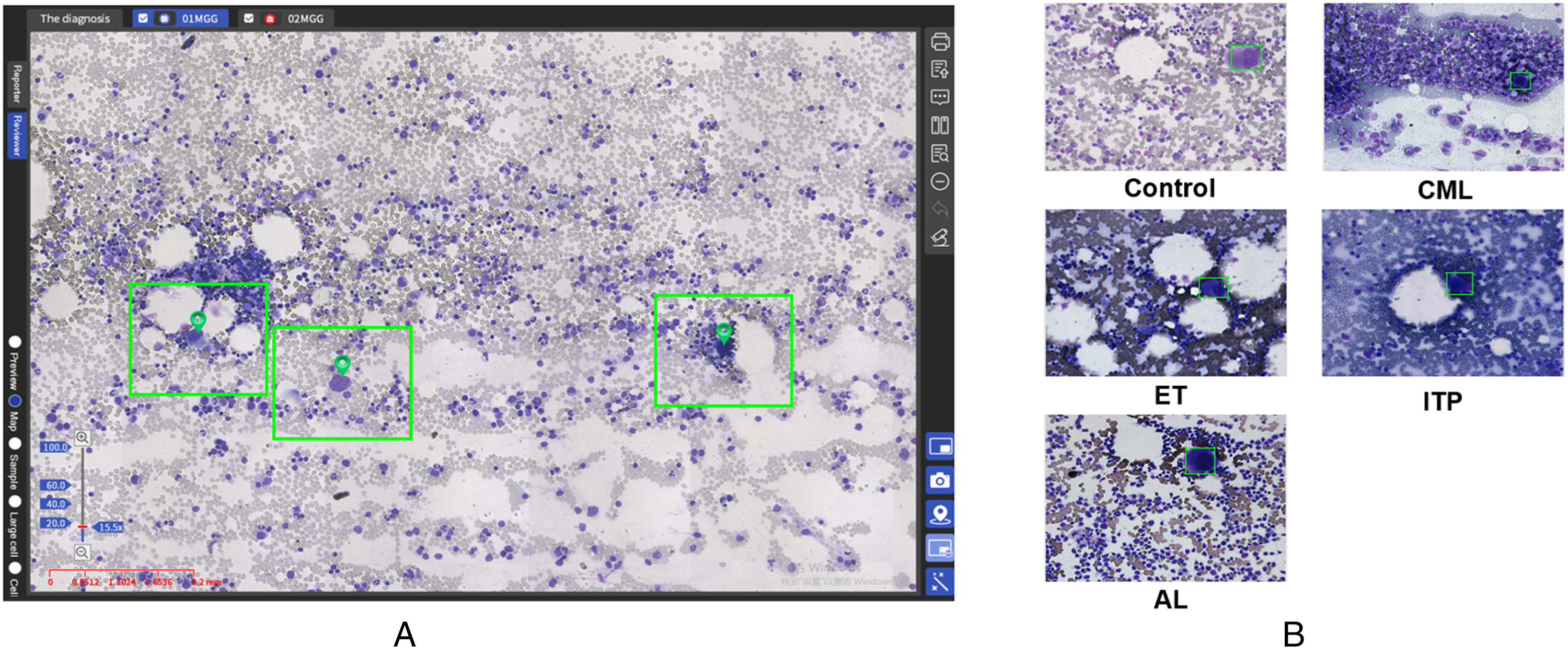
Pathologists using Morphogo system to annotate megakaryocytes. (A) Cell distribution map interface of BM smears on Morphogo system. (B) View of digital smears from each group for megakaryocyte annotation.
Validation of the Precision and Recall of the Megakaryocyte Recognition Algorithm.
Further, we grouped BM smears according to case information and validated Morphogo's performance in detecting megakaryocytes in BM smears from different types of patients. The performance analysis was completed by confusion matrix based on the results of megakaryocyte annotation by pathologists. In the Morphogo interface, the red frames are the megakaryocytes automatically recognized by the system and the green frames are the megakaryocytes annotated by the pathologist (Figure 4). The accuracy and sensitivity of Morphogo system for identifying megakaryocytes in BM smears were very high, above 90% in different types of patients’ BM smears, with a slightly lower sensitivity of 84.42% for detecting megakaryocytes in BM smears from the ITP group (Table 2). The specificity of Morphogo for the detection of megakaryocytes varied widely, from 76.27% to 99.07%, but still showed good performance overall. The FPR was below 20% in all groups of samples except the ET group. In general, the number of megakaryocytes is higher in BM smears from ET patients, so the detection of more megakaryocytes in them by Morphogo has no impact on the evaluation of BM smears and the diagnosis of the disease. In addition, the results for megakaryocyte annotation by Morphogo system were in line with the pathologists with Kappa values in the range of 0.70 to 0.98. Namely, Morphogo system can be used to detect megakaryocytes in BM smears.
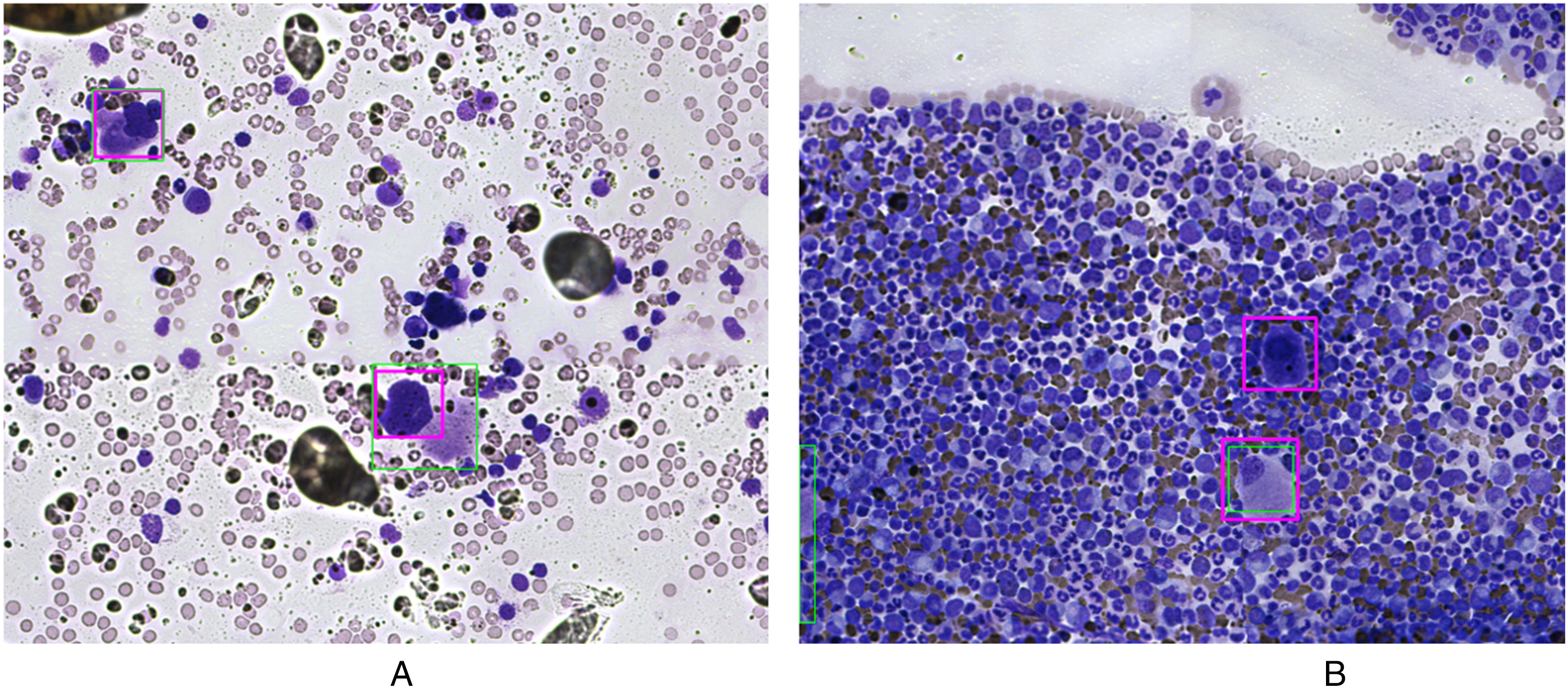
The results of Morphogo system for megakaryocyte identification are compared with the annotations of pathologists. (A) The annotations of the system agree with the pathologist, the red frame is the system annotation and the green frame is the manual annotation. (B) The annotations of the system do not agree with the pathologist.
Performance of the Device to Identify Megakaryocytes in BM Smears.
Whole-Slide Counting of Megakaryocytes by Morphogo Shows a High Correlation with Manual Microscopy
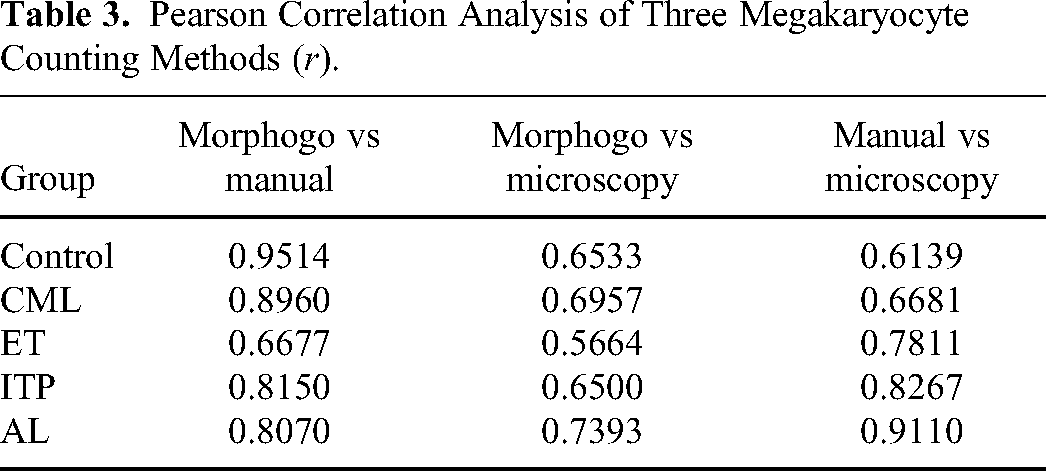
To further explore Morphogo system's performance in the practical application of BM megakaryocyte examination, we recorded the megakaryocyte count results for each sample obtained by Morphogo system, manual counting, and microscopy. Difference analysis showed that the number of megakaryocytes was significantly increased in the CML, ET, and ITP groups compared with the control group (Figure 5). Correlation analysis was performed on the megakaryocyte count results obtained by the three methods mentioned above (Table 3). Except for the ET group, the overall correlation between the automated counting of megakaryocytes by Morphogo system showed an extremely high correlation with that of the system-assisted manual counting (r > 0.80) and a high correlation with that of microscopy (r > 0.65). The correlation between megakaryocytes counted by pathologists on digital smears and manual microscopy is slightly higher than the correlation between Morphogo and manual microscopy. Therefore, it is feasible to use Morphogo system instead of or to assist pathologists in performing a whole-slide count of megakaryocytes when performing a clinical BM examination, and Morphogo can detect more megakaryocytes.
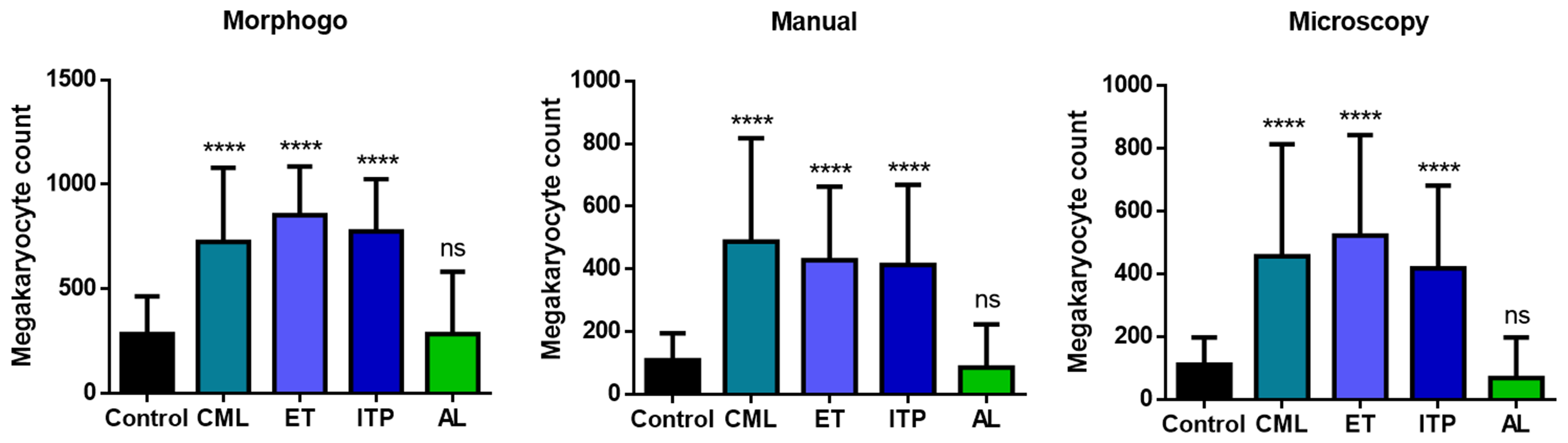
Differential analysis of megakaryocyte counts obtained by the three megakaryocyte counting methods for each group. ****P < .0001; ns, the difference is not statistically significant.
Pearson Correlation Analysis of Three Megakaryocyte Counting Methods (r).
Morphogo System Works for Automated Classification of Megakaryocytes in BM Smears
Morphogo system's performance of megakaryocyte classification is important to be assessed for the evaluation of its clinical feasibility. Morphogo system completed the classification of megakaryocytes and the results were reviewed by pathologists. Megakaryoblasts were not seen in the classification tests of the research. Therefore, Morphogo system classified megakaryocytes into four categories (Figure 6A). Among the 6922 megakaryocytes automatically classified, granular megakaryocytes and platelet-producing megakaryocytes accounted for the majority, and promegakaryocytes and nude-nuclear megakaryocytes were rare (Figure 6B). We calculated the proportion of different morphological megakaryocytes in each BM smear based on the classification results of megakaryocytes. Morphogo system showed a high correlation with manual microscopy in classifying megakaryocytes (r ≥ 0.7218, P < .0001). In the CML, ITP, and AL groups, the proportions of megakaryocytes of different morphological types obtained by both methods were extremely close, showing a high degree of consistency in classifying megakaryocytes (Figure 7). It confirms that Morphogo system can replace or assist pathologists in the classification of megakaryocytes in BM smear examinations in addition to whole-slide counting.
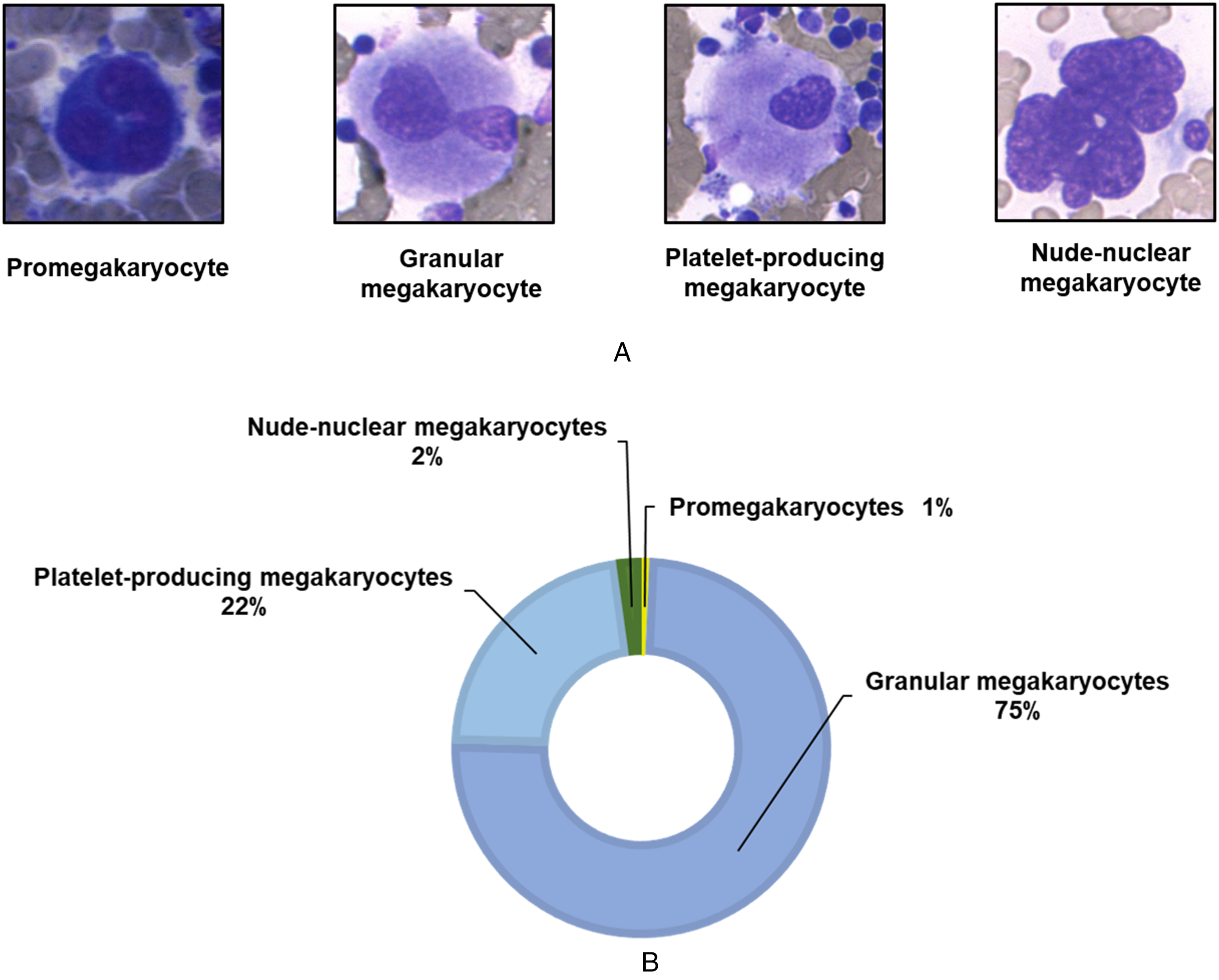
Four morphological structures of BM megakaryocytes. (A) Four types of megakaryocytes. (B) The 6922 megakaryocyte images used to test the classification performance of Morphogo system were assigned to the four morphological categories.
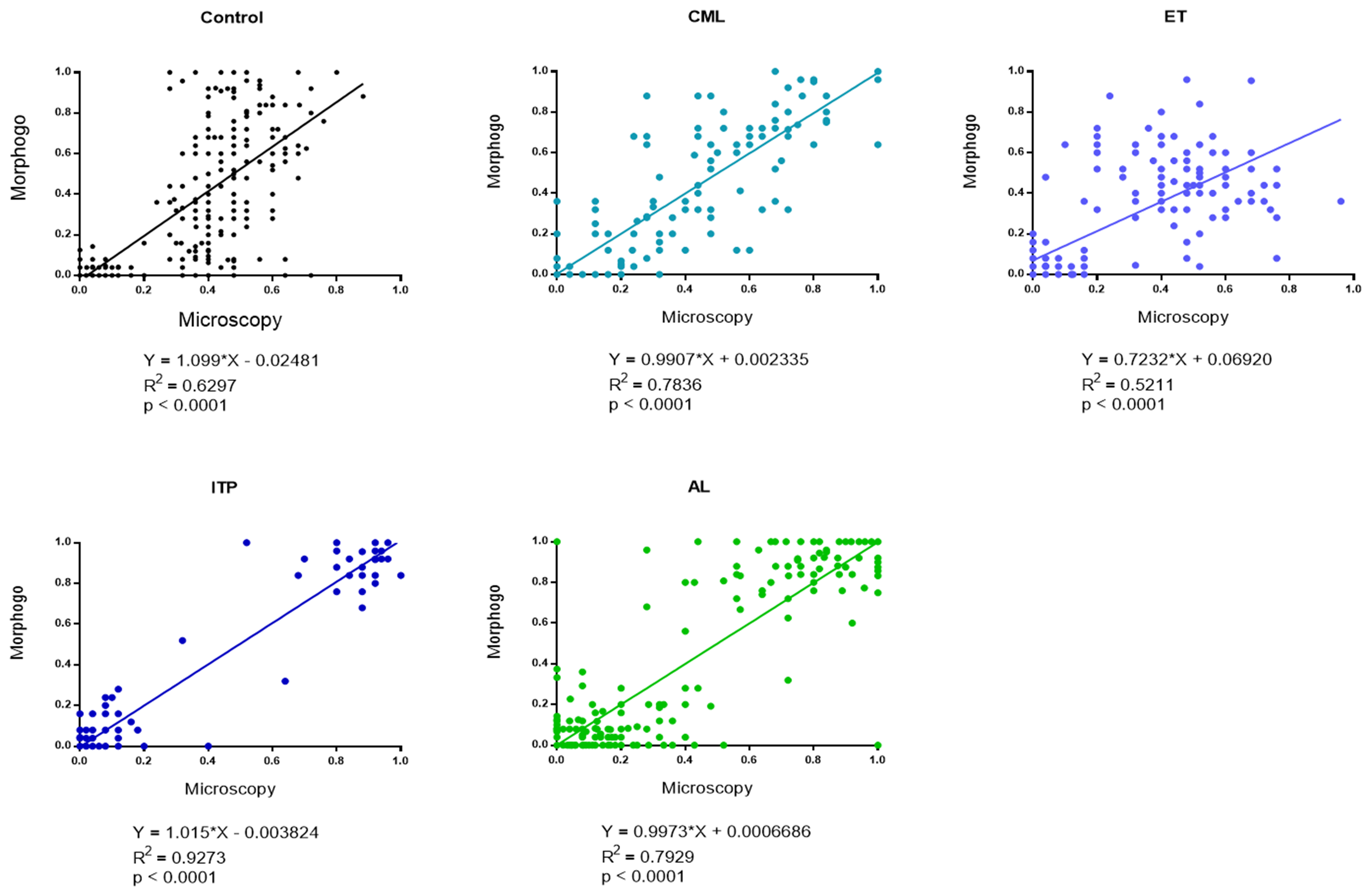
Scatter plots of linear regression lines generated from BM smears of each group of patients after classifying megakaryocytes by Morphogo system and microscopy.
Discussion
With AI applications in laboratory medicine, it has become a consensus that cells can be quantified by machines. Medical image classification is gradually moving toward intelligent processing, from the FCM clustering algorithm 16 and decision tree algorithm 17 to the use of a neural network to obtain high-latitude features in images. 18 Our team developed a neural network-based data-driven learning algorithm to locate megakaryocytes in BM smears by referring to the localization of peripheral blood leukocytes. 19 For the overlap of megakaryocytes, we use the Watershed algorithm to deal with this challenge and separate megakaryocytes by clustering methods. This study carried out a series of tests on Morphogo system's performance in BM megakaryocytes examination. It confirms that complex morphological features of megakaryocytes can be captured on digital images of BM smears. That is, we developed a reliable method for automated detection of megakaryocytes.
In the generalization ability test of the AI recognition model, Morphogo system did not perform as well as the recognition of megakaryocytes in normal BM when recognizing megakaryocytes from CML patients and ET patients. Possible reasons for the occurrence of misidentification include significant BM hyperplasia and more staining residues in the BM smears of some patients in the CML and ET groups, and some vacuoles and artifacts were classified as megakaryocytes by the recognition algorithm leading to lower precision of recognition. 20 Overall, the accuracy and sensitivity of the Morphogo system for detecting megakaryocytes from BM smears were around 95%. In comparison with previous studies, the neural network named Single Shot Multibox Detector identified megakaryocytes with an average accuracy of 86%, slightly inferior to the Morphogo system. 21 Compared with the superior megakaryocyte recognition performance shown by Morphogo, the above neural network model is only based on the construction of the megakaryocyte library of 20 ET patients. The ability of the model to extract, learn and identify megakaryocyte features needs to be improved by expanding the training database. Tzu-Hsi Song et al proposed a framework to delineate megakaryocytes in digitized images of BM trephine biopsies with an accuracy of 85%, which was the best performance of the existing model framework at that time. 22 Recently, a deep learning algorithm (BMSNet) was developed to help hematologists interpret BM smears, identifying 42 megakaryocytes with an accuracy of 71.0% and recall of 56.4%, respectively. 23 Although the BMSNet model performs well in classifying BM nucleated cells, its use requires an experienced technician to manually adjust focus and brightness during photography, and automatic slide scanning needs to be configured and optimized for clinical application. The latest model, CMLcGAN, was developed to segment megakaryocytes from BM cells with an accuracy of 95.1%. 24 Morphogo, the automated analysis device we developed, detects megakaryocytes in BM digital images with up to 95% accuracy and combines automated scanning and automatic identification functions. Our data strongly confirms that Morphogo system is a better solution for identifying megakaryocytes in BM smears.
Recently, potential applications of AI-based technologies for megakaryocytes have begun to emerge. Machine learning confirmed the independent role of megakaryocytic dysplasia in predicting the response to AML chemotherapy. 25 By analyzing the gene expression profiles and BM morphological alterations in patients living with myelodysplastic syndrome (MDS), researchers have identified five morphological features that can differentiate patients with different prognoses, including elevated megakaryocyte counts. 26 We found elevated megakaryocyte counts in the CML, ET, and ITP groups as well. In the BM examination of patients with CML, increased megakaryocytes are seen in the chronic phase, while megakaryocytes are rare or absent in patients with acute changes. 27 Abnormal accumulation of megakaryocytes in the BM is both a typical feature and one of the main diagnostic criteria of ET. 28 Patients living with ITP have a compensatory proliferation of megakaryocytes in the BM with various morphological abnormalities. 29 Clinically, the degree of BM megakaryocyte hyperplasia serves as a good prognostic indicator in ITP patients. 30 In our study, the automated counting of Morphogo system was in highly positive correlation with manual counting by the system-assisted pathologist and moderate positive correlation with microscopy. However, it did not hold in the ET group. Compared with the microscopy and manual counting, the system counted more megakaryocytes in BM smears for several possible reasons as follows. First, the microscopy was performed with 10× objective, which was very likely to miss some megakaryocytes as micro megakaryocytes. Second, interobserver variation existed in microscopic examinations. The correlation between the results of manual counting and microscopy ranged from 0.6139 to 0.9109. The large variation between the data points to the existence of interobserver variation. However, a high consistency was found between the Morphogo system and microscopic examination in classifying megakaryocytes, especially in the CML, ITP, and AL groups.
Our study provides a quantitation of megakaryocytes in BM biopsies and smears was performed using a simple direct method of counting. The precise quantification of megakaryocytes has a statistical significant in predicting the trend for cellularity, myelopoiesis, and megakaryocytes with age in the cohort of patients. In addition, the specific morphological features of megakaryocytes are the “hallmark” in the conjecture of differential diagnosis of MDS, ITP, and MPN, such as essential thrombocythemia, polycythemia vera, and primary myelofibrosis. 31 Thrombocytopenia may be encountered in various hematological and nonhematological conditions and may be associated with dysplastic megakaryocytes which is a feature of MDS, even though they can be observed in non-MDS hematological conditions. Dysplastic megakaryocytes are common in non-MDS-related thrombocytopenia and their mere presence should not lead to the diagnosis of MDS. Hence, a proper diagnosis should be made on megakaryocyte morphology, patient's clinical findings, and other hematological parameters. This understanding can improve the diagnostic accuracy for a wide range of hematological disorders.
Morphogo system presents an overall satisfactory performance in the practical application of BM smear megakaryocyte examination. Morphogo system has a scanning time of ≤1 s for 1 mm2 under 40× objective and a generation time of <10 min for a digital smear. The CNN-based algorithm enables rapid counting of whole-slide megakaryocytes with a stable recognition performance. It does not vary with time, location, or user internal variation. It can also be continuously optimized by machine learning, significantly reducing technicians’ and pathologists’ workloads. In addition, there are limitations to the study. We only performed algorithmic learning and feature extraction for four types of megakaryocytes and did not address morphological changes in megakaryocytes, including dysplastic and non-dysplastic features. Dysplastic features included multiple separated nuclei, micro megakaryocytes, and hypogranular forms. Micromegakaryocytes were those megakaryocytes with a size similar to that of large lymphocytes or monocytes and had single or bilobed nuclei. Hypogranular forms were those megakaryocytes that had a clear cytoplasm with no or sparse granules. Nondysplastic features included immature forms, emperipolesis, platelet budding, cytoplasmic vacuolization, and bare megakaryocyte nuclei. 32 Immature forms are the young megakaryocytes which lack nuclear lobulation and have scant basophilic cytoplasm. At least thirty megakaryocytes were evaluated on BMA smears, and dysplastic alterations were considered significant only when 10% or more of megakaryocytes observed show the changes. Morphogo based on the above characteristics to detect the morphological changes of the megakaryocytes to indicate that dysplasia is the direction of subsequent research and the future scope of Morphogo's application in the clinical BM examination process.
Moreover, the proposed automated analysis tool for BM megakaryocytes could shorten the time for clinicians to produce reports, allowing for more timely diagnosis and treatment of patients, and reducing hospitalization time and costs. AI systems that can help automate and standardize megakaryocyte examination for universal clinical use will facilitate the establishment of a consensus on the standardization of BM megakaryocyte count, which in turn will promote standardization of diagnosis and standardization of treatment outcomes.
Conclusion
Morphogo system is reliable in automatic identification, counting, and classification of megakaryocytes in BM aspirate smears, and can assist pathologists in the early diagnosis and monitoring of hematologic malignancies.
Supplemental Material
sj-xlsx-1-tct-10.1177_15330338221150069 - Supplemental material for The Application of Morphogo in the Detection of Megakaryocytes from Bone Marrow Digital Images with Convolutional Neural Networks
Supplemental material, sj-xlsx-1-tct-10.1177_15330338221150069 for The Application of Morphogo in the Detection of Megakaryocytes from Bone Marrow Digital Images with Convolutional Neural Networks by Xiaofen Wang, Ying Wang, Chao Qi, Sai Qiao, Suwen Yang, Rongrong Wang, Hong Jin and Jun Zhang in Technology in Cancer Research & Treatment
Footnotes
Acknowledgments
The authors thank Xinyi Cao for feedback on the manuscript, Zhen Huang and Junlin Feng for technical assistance, and Jun Yan for collecting data from hospital.
Declaration of Conflicting Interests
Ying Wang is employed by Hangzhou ZhiWei Information Technology Co. Ltd. The remaining authors declare no competing financial.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Zhejiang Province (grant number LYY20H310001).
Ethics Declarations
The project was approved by the Ethics Committee of Sir Run Run Shaw Hospital affiliated with the Zhejiang University School of Medicine (No. 2022-657-01). Since BM smears in this retrospective study have been used in clinical examination, the informed consent of patients was exempted.
Data Availability
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.