
Abstract
Introduction
The management of advanced non-small cell lung cancer (NSCLC) has developed rapidly and relies on the wide usage of novel therapeutics, including targeted therapy, immunotherapy, and so on. Patients harboring actionable genomic alterations, such as epidermal growth factor receptor (EGFR), anaplastic lymphoma kinase (ALK) and ROS1 alterations can benefit from the corresponding targeted therapy.1–3 EGFR tyrosine kinase inhibitors (EGFR-TKIs) are currently the standard first-line treatment for advanced NSCLC patients harboring sensitive EGFR mutations and have improved outcomes when used as an adjuvant treatment after complete resection, according to the ADAURA study. 4 Currently, systemic administration of monoclonal antibodies against programed death 1 (PD-1) and its ligand PD-L1 has been established as new standard of care for patients with advanced NSCLC.5,6 Compared with the standard regimen of chemotherapy, treatment with immune checkpoint inhibitors (ICIs) alone or in combination with chemotherapy has brought significant survival benefits for selected NSCLC patients.5,6 However, patients harboring sensitive EGFR mutations or ALK rearrangement are believed to have a poor response to immunotherapy. Therefore, actionable genomic alterations are considered to play different roles in the response of NSCLC to different therapeutics.
Alterations in the MET gene are identified as actionable oncogenic alterations, 7 and MET gene amplification plays an important role in the growth and survival of NSCLC 8 via enhanced binding to receptor tyrosine kinases (RTKs), which can then initiate a series of cellular signaling pathways associated with proliferation and metastasis. 9 In addition to amplification of the MET gene, mutations in MET, especially exon 14 skipping alterations, are other gain-of-function alterations in MET. In NSCLC patients harboring MET mutations, the administration of MET-TKIs, such as crizotinib, has been proven in previous studies to achieve a satisfactory response.10–12 Immunotherapy is another treatment option for NSCLC patients with MET alterations.13–15 However, the efficacy of different therapeutics in NSCLC patients with MET amplification remains to be further elucidated.
In this study, we included NSCLC patients with MET amplification to estimate the efficacy of various therapeutics in different lines of treatment and further performed a meta-analysis of current and previous studies to determine the therapeutic outcomes based on a larger sample size. Acquired MET amplification is an important mechanism of resistance to EGFR-TKI treatment among NSCLC patients harboring concomitant sensitive EGFR mutations. 16 However, the therapeutic outcomes after EGFR-TKI treatment failure remain unclear. Therefore, we included another group of patients who received first-line EGFR-TKI therapy and acquired resistance via MET amplification to observe the efficacy of different therapeutics.
Methods
Study Patients
In this retrospective study, a total of 33 NSCLC patients (n = 33) harboring primary MET amplification, who admitted in our hospital since January 2015, were included in this study. The inclusion criteria were as follows: (a) Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2; (b) stage IV disease with pathological tissues available for next-generation sequencing (NGS); (c) primary MET amplification; and (d) available follow-up information. The exclusion criteria were as follows: (a) NGS findings—wild-type or MET mutation alone or in combination with other actionable genomic alterations (EGFR, ALK, ROS1, BRAF V600E, KRAS, etc); (b) ECOG performance status > 2; (c) loss to follow-up or refusal to participate.
Another 9 NSCLC patients (n = 9) in the Affiliated Hospital of Qingdao University harboring acquired MET amplification were included. The inclusion criteria were as follows: (a) ECOG performance status 0 to 2; (b) stage IV disease with pathological tissues available for NGS; (c) primary sensitive EGFR mutations (19 DEL or 21 L858R) and failure of first-line EGFR-TKI treatment; (c) acquired MET amplification; and (d) available follow-up information. The exclusion criteria were as follows: (a) treatment with other modalities except EGFR-TKIs; (b) ECOG performance status > 2; and (c) loss to follow-up or refusal to participate.
Basic clinical and demographic information, including age, sex, diagnosis, treatment information, etc was collected from all enrolled patients. All tumors were staged according to the 2019 American Joint Committee on Cancer (AJCC) TNM staging system for lung cancer. Disease progression was diagnosed by 2 professional physicians experienced in clinical medical oncology. The current study was performed according to the instructions of STROBE Statement. 17 All patients were de-identified in this study. This study was approved by the Ethics Committee of the Affiliated Hospital of Qingdao University, and the investigations were carried out following the guidelines established in the Declaration of Helsinki. Written informed consent was obtained from all patients included in the study, and all experiments were carried out in accordance with the National Health and Family Planning Commission of the PRC's guidelines.
Targeted Sequencing and Bioinformatic Analysis
In this study, alterations in MET and EGFR and other actionable genomic alterations were confirmed by NGS. The NGS details have been reported in our previous study. 18 Here, tissue samples from 42 NSCLC patients were analyzed by NGS using 3 capture-based targeted sequencing panels. In addition, data for 143 NSCLC patients (n = 143, 12 patients harboring MET alterations) obtained from the cBioPortal for Cancer Genomics19,20 were included to perform survival analysis of patients stratified by immunotherapy. Data from TIMER21,22 and TISIDB 23 were used to examine the abundance of infiltrating immune cells in NSCLC patients. In addition, Kaplan–Meier Plotter 24 was used to perform survival analysis.
Meta-Analysis
We searched 4 databases independently—PubMed, ScienceDirect, ClinicalTrials.gov and the Cochrane Library—for literature selection. All MeSH terms for the keywords (MET; NSCLC) were used in the search. The following data were extracted: study ID, a number of patients, MET alterations, treatment methods, progression-free survival (PFS) and overall survival (OS). All statistical analyses in the meta-analysis were performed using Stata 14.0 software (Stata Corp.). The results are expressed as incidence rates and 95% confidence intervals (CIs). In this study, we used a random-effects model to perform statistical analyses, and the chi-squared test and I2 statistic were used to assess inter-study heterogeneity. A P-value > .1 and an I2< 50% indicated that the heterogeneity was not statistically significant. 25
Statistical Analysis
All statistical analyses were performed using GraphPad Prism 8.0 software (GraphPad), and Student's t test was used to determine statistical significance. P values were determined by 2-tailed tests, and P < .05 was used to define statistical significance. The log-rank test was used for survival analysis.
Results
the Prevalence of
MET
Alterations and Their Role in the Immunotherapy Response of NSCLC Patients
Two studies of immunotherapy for NSCLC patients from the cBioPortal were selected for the analysis, as shown in Figure 1A. Alterations in common driver genes of NSCLC were detected based on these 2 studies, and the findings suggested that alterations in KRAS are the most common genomic signature in NSCLC, with an incidence of 35%, followed by alterations in EGFR (14%), PIK3CA (8%), ALK (7%), MET (7%), ROS1 (6%), ERBB2 (4%), BRAF (4%), NTRK1 (4%), RET (4%), and NRAS (2.2%). The PFS times of patients harboring actionable genomic alterations described above, were significantly shorter than those of the wild-type (WT) groups (P = .0322), as shown in Figure 1B. In these 2 studies, 12 patients harbored MET alterations without any other genomic alterations. Compared with the WT group, MET was an independent risk factor for immunotherapy failure in NSCLC (4.2 months vs 6.2 months, P = .0149), and patients harboring MET alterations had shorter PFS times, as shown in Figure 1C.

The prevalence of actionable genomic alterations among NSCLC patients and the relationship between MET alterations and immunotherapy. (A) The prevalence of driver genes in cBioPortal; (B) alteration of driver genes is associated with a poor response to immunotherapy; (C) MET alterations are associated with a poor response to immunotherapy; (D) the median PFS time of patients harboring primary MET amplification who received immunotherapy; (E) representative cases of patients harboring primary MET amplification who received immunotherapy. Abbreviations: NSCLC, non-small cell lung cancer; PFS, progression-free survival.
Efficacy of Various Therapeutics in NSCLC Patients Harboring Primary
MET
Amplification
To further elucidate the response to different therapeutics among NSCLC patients harboring primary MET amplification, 33 NSCLC patients harboring primary MET amplification were included in this study. The selected patients were treated with immunotherapy, targeted therapy or chemotherapy. The basic information and clinical features of these 33 patients are summarized in Table 1. Generally, the median age of these patients was 64.0 years and ranged from 33.0 to 78.0 years, and most of the patients were diagnosed with stage IV (97.0%) lung adenocarcinoma (LUAD, 63.6%). A total of 87.9% of NSCLC patients in this study harbored MET amplification, and others harbored concomitant alterations of MET amplification and concomitant exon14 skipping (12.1%). The median follow-up time was 1308 days, ranged from 273 days to 2343 days.
The Characteristics of Patients Harboring

Abbreviations: ECOG, Eastern Cooperative Oncology Group; LUAD, lung adenocarcinoma; LUSC, lung squamous cell carcinoma; PD-L1, programed death-ligand 1.
Immunotherapy
For the 11 patients receiving immunotherapy, only 1 patient was treated with single ICIs and 10 patients were treated with ICIs (anti-PD-1 or anti-PD-L1 antibodies) in combination chemotherapy. As shown in Figure 1D, the median PFS time of patients who received immunotherapy was 75.0 days (95% CI: 34.0-96.0 days). Figure 1E shows the CT scans of 2 typical patients who received immunotherapy; the best response of patient 1 was partial response, but patient 2 did not benefit from the treatment. As concluded in Table 2, the objective response rate (ORR) for the best therapeutic response was 9.1%, and the disease control rate (DCR) was 72.7%.
The Summary for the Efficacy and Endpoint of Evaluation for Patients in our Center.
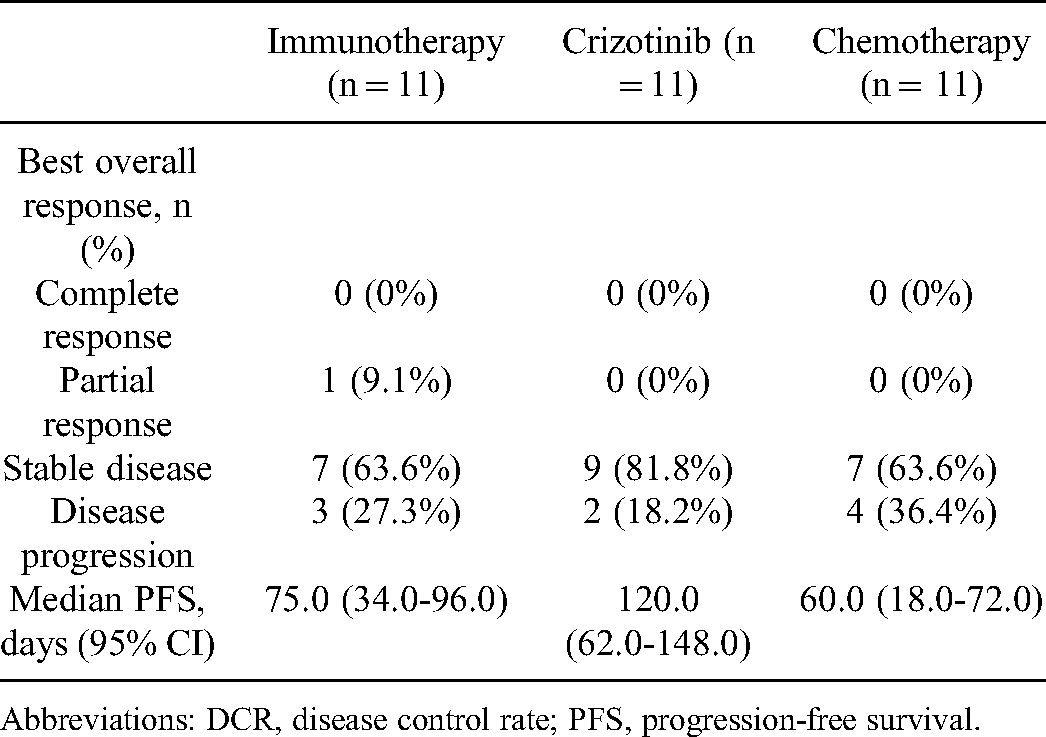
Abbreviations: DCR, disease control rate; PFS, progression-free survival.
Crizotinib
In this study, 11 stage IV NSCLC patients (n = 11) included in this study were treated with crizotinib. The median PFS time for this group of patients was 120.0 days (95% CI: 62.0-148.0 days), as shown in Figure 2A. The CT scans shown in Figure 2B demonstrate the treatment process, including the best response (stable disease, SD), of a patient who received crizotinib. The DCR and ORR of crizotinib treatment was 81.8% and 0%, respectively, in this study according to Table 2.

Comparison of different therapeutics among NSCLC patients harboring primary MET amplification. (A) The median PFS time of crizotinib in patients harboring primary MET amplification; (B) representative case for patients harboring primary MET amplification who received crizotinib; (C) the median PFS time of chemotherapy among patients harboring primary MET amplification; (D) representative case of patients harboring primary MET amplification who received chemotherapy; (E) the comparison of the PFS between patients treated with different therapeutics; (F) the comparison of the response to immunotherapy based on the expression level of PD-L1; (G) the comparison of the efficacy of different therapeutics in different treatment lines among patients harboring primary MET amplification. Abbreviations: NSCLC, non-small cell lung cancer; PFS, progression-free survival; PD-L1, programed death ligand 1.
Chemotherapy
Another 11 stage IV NSCLC patients (n = 11) were treated with a standard regimen of chemotherapy in this study. As shown in Figure 2C, the median PFS time of chemotherapy was only 60.0 days (95% CI: 18.0-72.0 days). Figure 2D displays the CT scans of the treatment process of 1 typical patient who had progressive disease (PD) after chemotherapy. The DCR of chemotherapy was 63.6% and the ORR was 0%.
The Comparison of the Different Groups of Patients
The comparison of the PFS times of the patients from the 3 groups shown in Figure 2E indicates that crizotinib treatment seems to be a better choice for NSCLC patients with MET amplification than chemotherapy or immunotherapy. In addition, ICIs did not exhibit the expected efficacy, and the prognostic effect of the PD-L1 expression status for ICI treatment did not demonstrate its important role (P = .7295) in NSCLC patients with MET alterations, as shown in Figure 2F. For those patients with concurrent high PD-L1 expression (≥50%), which accounted for 45.4% of the patients who received immunotherapy in this study, the median PFS time was only 77.5 days, similar to that of patients with concurrent low expression of PD-L1 (50%, median PFS time: 85.0 days).
To further explore the efficacy of different therapeutics in NSCLC patients with MET amplification in different lines of treatment, we performed subgroup analysis based on the treatment line. As shown in Figure 2G, crizotinib (first-line: n = 5; second line: n = 6) displayed the best efficacy, followed by ICIs (first-line: n = 5; second line: n = 5) and chemotherapy (first-line: n = 8; second line: n = 3), both in first-line (120.0 days vs 85.0 days vs 60.0 days, P = .0378) and second-line treatment regimens (120.0 days vs 106.0 days vs 40.0 days, P = .0181).
Meta-Analysis of Studies on the Treatment of Patients With Primary NSCLC Harboring
MET
Alterations
After literature selection, a total of 6 studies on the treatment of patients with primary NSCLC harboring MET alterations were included in the meta-analysis. The basic information of the involved studies is summarized in Table 3. Ninety patients who received crizotinib treatment (n = 90) and 111 patients who received ICI treatment (n = 111) were included in the meta-analysis. As the results of the meta-analysis show

Meta-analysis of studies on the treatment of non-small cell lung cancer (NSCLC) patients harboring primary MET alterations. (A) Meta-analysis of patients who received crizotinib in the included studies; (B) meta-analysis for patients who received immunotherapy in the included studies.
The Summary for Studies on the Treatment of NSCLC Patients Harboring

Abbreviations: PFS, progression-free survival; OS, overall survival; ICIs, immune checkpoint inhibitors; NA, not available; NR, not reached.
Efficacy of various Therapeutics in NSCLC Patients Harboring Acquired
MET
Amplification After Resistance to First-Line EGFR-TKIs
As shown in Table 4, 9 stage IV LUAD patients (n = 9) harboring sensitive EGFR mutations (7 patients harboring 19 DEL, 2 patients harboring 21 L858R) were enrolled and treated with standard first- to third-generation EGFR-TKIs (gefitinib, erlotinib or osimertinib). After treatment with EGFR-TKIs, all 9 LUAD patients developed resistance to EGFR-TKIs, and NGS demonstrated that all of the patients harbored acquired MET amplification after first-line treatment with EGFR-TKIs, which constituted the mechanism of resistance. The median PFS time in the second-line treatment group after the failure of EGFR-TKIs was 90.0 days, as shown in Figure 4A. We further explored the differences between the efficacy of different therapeutics as second-line treatments in these patients. As shown in Figure 4B-C, chemotherapy plus bevacizumab (n = 3) may have superior efficacy (310.0 days versus 73.5 days, P = .0360) compared with MET-TKIs ± EGFR-TKIs (n = 6).

Treatment of patients harboring acquired MET amplification after the failure of first-line treatment with EGFR-TKIs. (A) The median PFS time after second-line treatment among patients harboring acquired MET amplification; (B) survival analysis of the PFS time between patients treated with different therapeutics; (C) the comparison of the PFS time between patients treated with different therapeutics. Abbreviations: PFS, progression-free survival; EGFR-TKI, epidermal growth factor receptor-tyrosine kinase inhibitor.
Basic Information for Patients Harboring Acquired

Abbreviations: EGFR, epidermal growth factor receptor; TKIs, tyrosine kinase inhibitors; PFS, progression-free survival; LUAD, lung adenocarcinoma; PD, progressive disease.
MET is Associated With the Immune Microenvironment and Predicts Poor Prognosis in Patients With NSCLC
In this study, we found that NSCLC patients harboring MET amplification did not benefit from the therapeutics and had poor prognoses; therefore, we further explored the potential mechanism related to MET-induced insensitivity to the treatment. As shown in Figure 5A, the protein expression of MET was positively associated with that of a series of molecules related to inhibition of the tumor immune microenvironment (TIME), including CD274 (PD-L1, P < .0001), PDCD1 (PD-1, P = .0017), PDCD1LG2 (PD-L2, P < .0001) and TIGIT (P < .0001), which suppress the tumor immune response via the PD1/PD-L1 pathway or suppress T-cell activation by promoting the generation of mature immunoregulatory dendritic cells, and that of molecules related to poor prognosis or even hyperprogressive disease with ICI treatment, including MDM2 (P < .0001) and CCND1 (P < .0001). As shown in Figure 5B, amplification of the MET gene was found to be associated with a trend of low infiltration of the TIME, especially in lung squamous cell carcinoma. Furthermore, the MET protein serves as a biomarker for the poor prognosis of NSCLC patients, as shown in Figure 5C. NSCLC patients with higher MET protein expression had poor disease-free survival (P < .0001) and OS (P < .0001).

The role of MET in the tumor microenvironment and the prognosis of non-small cell lung cancer (NSCLC). (A) The relationship between the expression of MET and that of a series of molecules; (B) the infiltration level of a variety of tumor-infiltrated cells between patients with different types of MET alterations; (C) survival analysis of NSCLC patients according to the MET expression level.
Discussion
The standard treatment for NSCLC patients has recently been considerably transformed with the development of targeted therapy and immunotherapy. NSCLC patients harboring actionable genomic alterations, such as sensitive EGFR mutations and ALK rearrangement, benefit from standard treatment with the corresponding TKIs.26,27 However, previous studies proved that EGFR and ALK alterations are associated with a poor response to ICI treatment. 28 Therefore, patients harboring actionable genomic alterations respond differently to therapeutics. MET alteration is a relatively rare genomic alteration in NSCLC patients, 29 and in this study, approximately only 7% of patients harbored MET amplification and/or mutation. Although multiple studies10–15 have explored the response of NSCLC patients harboring MET alterations to different therapeutics, the sample sizes were small, and no study has made a horizontal comparison of different therapeutics in NSCLC patients harboring MET amplification. In this study, we enrolled a group of patients who received 3 types of treatment—immunotherapy, crizotinib treatment, and chemotherapy—to explore the response of NSCLC patients harboring primary MET amplification to these therapeutics. The results suggested that crizotinib, which is a MET-TKI, demonstrated better efficacy than the other 2 types of therapeutics, regardless of the treatment line. However, even crizotinib treatment maintained SD for only 4.57 months, according to the meta-analysis based on 90 patients who received this treatment in real-world studies. No significant heterogeneity was detected in this meta-analysis, suggesting no significant difference in the treatment response between patients with different kinds of MET alterations. According to this study, primary MET amplification seems to be for a predictor of poor response to the therapeutics listed above, and novel therapeutics need to be explored. Clinical trials with patients harboring MET alterations might provide these patients with more options. 30 In the GEOMETRY trial, capmatinib (INC280) achieved an inspiring 12.6-month duration of response (DOR) as first-line treatment and a 9.7-month DOR as second-line treatment. Other trials for tepotinib (VISION trial) and savolitinib (NCT02897479) proved the convincing efficacy of these TKIs. Despite the promising efficacy of TKIs in clinical trials, real-world studies in patients harboring primary MET amplification are still needed.
For immunotherapy, MET amplification was a biomarker for a poor response to ICI treatment in this study. The 2.94-month DOR according to the meta-analysis based on 111 patients was not as satisfactory as the efficacy of the treatment in the real-world study. High expression of PD-L1 has been proven to be associated with a good response to immunotherapy and a good prognosis, as described in the KEYNOTE-189 trial. 31 However, NSCLC patients with MET amplification and concurrent high PD-L1 expression did not benefit from ICI treatment in this study. To explore the potential mechanism related to insensitivity to ICIs, we investigated the relationship between MET expression and factors related to a poor response to ICI treatment. The results suggested that MET expression is related to increased expression of molecules that inhibit the immune response in the TIME, such as TIGIT, which induces and maintains immune tolerance, participates in modulating the activation threshold of T-cells and limits the T-cell effector response.32,33 As a result, the level of tumor tissue infiltration was found to be relatively low in patients with MET amplification. In addition, MDM2 and CCND1 are believed to be associated with a poor response to ICI treatment, and MDM2 amplification is especially likely to induce hyperprogressive disease. 34 In this study, MET was also found to be associated with the expression of these 2 molecules. Further studies are needed to determine the relationship of these molecules.
Acquired MET alterations are one of the mechanisms underlying resistance to EGFR-TKIs through the resulting high affinity for RTKs and continuous activation of RTK signaling pathways. For these patients, it is unclear what kind of treatment would have the greatest benefit. According to previous studies, treatment with MET-TKIs such as tepotinib or capmatinib (INC280) plus gefitinib35,36 achieved a good response in this subpopulation, and the PFS time of patients treated with tepotinib plus gefitinib was 4.9 months. In this study, we performed a survival analysis of patients treated with 3 types of therapeutics and suggested that chemotherapy plus bevacizumab might be the best choice for this subpopulation of patients. Specifically, the efficacy of chemotherapy plus bevacizumab might be better than that of combination therapy with MET-TKIs and EGFR-TKIs. However, the small sample size in the 2 groups of patients limit the accuracy of the analysis and larger scale trials are warranted to verify the results.
Admittedly, several limitations exist in this study. First, given the low incidence of MET alterations, the sample size of NSCLC patients harboring primary or acquired MET alterations is small, and as a result, the calculation and justification of the sample size selected for this study were not performed. To expand the results in this study, we should perform a meta-analysis based on a larger sample size. In addition, the role of MET in the TIME lacks verification via further experiments.
Conclusion
MET amplification is a biomarker for poor prognosis in NSCLC and correlates with a low response to immunotherapy. For patients harboring primary MET amplification, crizotinib or other MET-TKIs is likely to be an optional treatment with worth-expecting efficacy. Chemotherapy plus bevacizumab may benefit patients harboring sensitive EGFR mutations and acquired MET amplification after the failure of EGFR-TKI treatment. These results warrant further large prospective studies.
Footnotes
Abbreviations
Acknowledgements
The authors thank for the kind support from Professor Junling Li, Professor Puyuan Xing, and Dr Fei Teng from Cancer Hospital, Chinese Academy of Medical Sciences.
Authors' Contributions
Conception/design was planned by Helei Hou and Hong Li; provision of study material or patients was handeled by Junyan Tao, Weihua Yan, Jingjuan Zhu, Hai Zhou, and Helei Hou; collection and/or assembly of data was carried out by Dantong Sun, Junyan Tao, Yingying Sheng, and Chaofan Xue; data analysis and interpretation was done by Dantong Sun, Helei Hou, and Hong Li; manuscript writing was done by Dantong Sun and Helei Hou; final approval of manuscript was done by all authors.
Consent for Publication
All authors approved publication of the article.
Availability of Data and Material
All data and material in this study are available.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: Special Funding for Qilu Sanitation and Health Leading Talents Cultivation Project (to Helei Hou); Chinese Postdoctoral Science Foundation (2017M622143 to Helei Hou); Qingdao Postdoctoral Application Research Funded Project (2016052 to Helei Hou).
Ethical Approval
This study was approved by the ethical committee of the Affiliated Hospital of Qingdao University (No. 16, Jiangsu Road, 266000, QINGDAO, China) on March 26, 2021, and the approval number is QYFY WZLL 27234.
Informed Consent
Written informed consent was obtained from all patients included in the study.