
Abstract
Many factors affect the prognosis of patients undergoing tumor surgery, and anesthesia is one of the potential influencing factors. In general anesthesia, inhalation anesthesia is widely used in the clinic because of its strong curative effect and high controllability. However, the effect of inhalation anesthetics on the tumor is still controversial. More and more research has proved that inhalation anesthetics can intervene in local recurrence and distant metastasis of tumor by acting on tumor biological behavior, immune response, and gene regulation. In this paper, we reviewed the research progress of diverse inhalation anesthetics promoting or inhibiting cancer in the critical events of tumor recurrence and metastasis, and compared the effects of inhalation anesthetics on patients' prognosis in clinical studies, to provide theoretical reference for anesthesia management of patients undergoing tumor surgery.
Introduction
Cancer, the world's second leading cause of death, kills about 10 million people a year. Due to the growth and aging of the population, as well as an increasing prevalence of risk factors such as smoking, overweight and environmental pollution, the incidence of cancer is increasing. Based on GLOBOCAN estimates, about 19.3 million new cancer cases in 2020 worldwide, Female breast cancer has surpassed lung cancer as the most common cancer, with an estimated 2.3 million new cases (11.7%), followed by lung (11.4%), colorectal (10.0%), prostate (7.3%), and stomach (5.6%) cancers. In addition, the global cancer burden is projected to reach 28.4 million cases by 2040, a 47% rise from 2020. 1 Cancer has become a significant challenge threatening human health, so it is of great practical significance to improve the prognosis and survival rate of patients.
Surgery remains the primary and preferred treatment for most solid tumors, with 60% of cancer patients receiving surgical treatment. 2 However, metastatic disease is still common despite more sophisticated surgical techniques and advances in adjuvant therapy such as radiotherapy, chemotherapy, and immunotherapy. The mechanism of tumor metastasis after surgery is complicated, in addition to factors such as tumor pathological staging and degree of differentiation, etc, physiological reactions such as increased circulating catecholamine levels, inflammation, wound healing, immunity, and platelet activation caused by surgery can also affect the local recurrence and distant metastasis of tumors and directly affect the prognosis of the patient.3–5 Anesthesia, as an essential part of the surgery, can directly or indirectly affect postoperative metastasis and recurrence of the tumor by participating in the above process. 6 Inhalation anesthetics can be used for induction and maintenance of general anesthesia, including sevoflurane, isoflurane, desflurane, halothane, enflurane, nitrous oxide, and xenon. They mainly enter the human body from the respiratory tract and exert anesthetic effects in the form of volatile gases. 7 In addition, inhalation anesthetics can prevent ischemia-reperfusion injury while anesthetizing, and provide patients with a certain degree of protection of the heart, brain, and kidneys. 8
Recent studies have shown that inhalation anesthesia can modulate gene and protein expression in tumor cells in a unique and time-dependent manner, 9 and inhalation anesthetics expose patients to a higher risk of cancer metastasis by impairing the immune system and inflammatory response. 10 However, the regulation of anticancer signals by inhalation anesthetics is also receiving increasing attention. 11 There is still controversy about whether inhalation anesthesia affects tumor progression. Therefore, this paper reviews the mechanisms of inhalation anesthetics promoting or inhibiting cancer at each key node of tumor metastasis (Figure 1, Table 1). In addition, it also compares the effects of inhalation anesthesia with local anesthesia or propofol-dependent intravenous anesthesia on common tumors in clinical studies in recent years (Table 2).

The role of volatile anesthetics in promoting or inhibiting cancer at each key node of tumor metastasis. Inhalation anesthetics can interfere with tumor metastasis by acting on tumor cell proliferation and apoptosis, angiogenesis, matrix invasion, platelet function, immune response, and gene expression. The red dashed boxes represent the promotion and the blue solid boxes represent the inhibition.
Preclinical In Vitro and In Vivo Studies of Inhalation Anesthetics and Cancer.
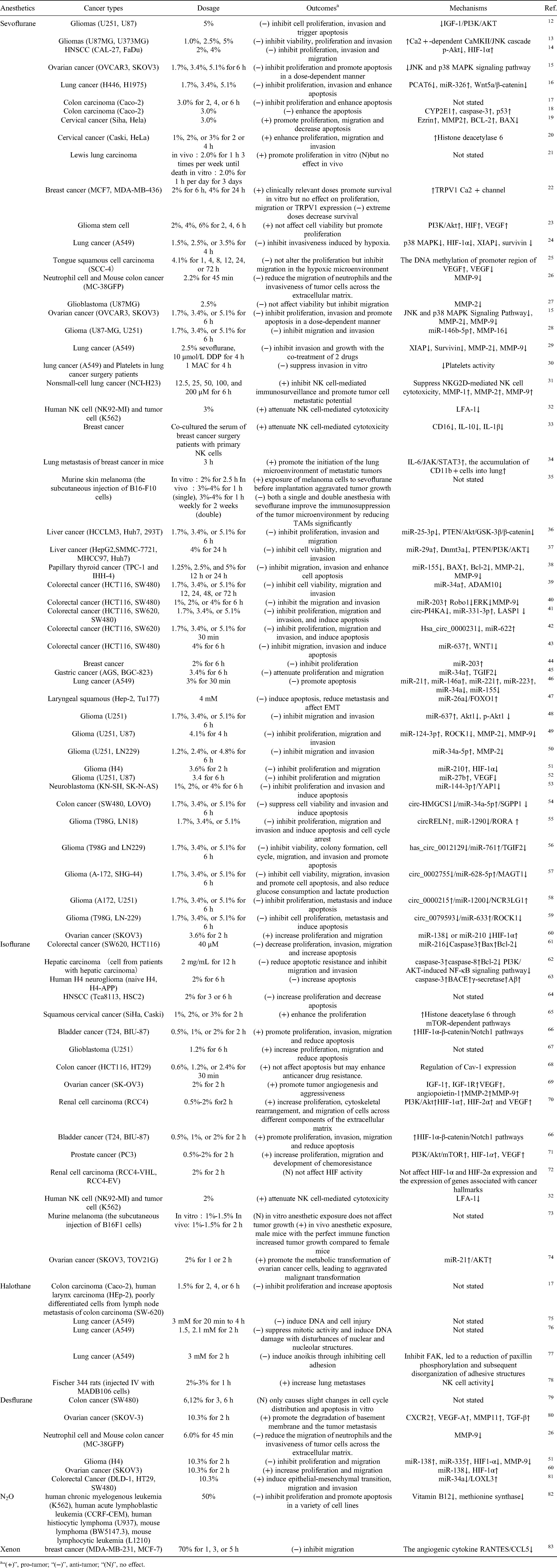
“(+)”, pro-tumor; “(−)”, anti-tumor; “(N)”, no effect.
Effect of Inhalation Anesthesia on the Prognosis of Patients With Cancer.

Tumor Metastasis and Colonization
In 1889, Stephen Paget proposed the “Seed-soil” theory for the organ specificity of tumor metastasis, which holds that the organ specificity of tumor metastasis is not accidental, it mainly depends on the specific affinity of cancer cells (“Seeds”) to the organ microenvironment (“Soil”),
116
and the theory is still applicable today. More and more studies show that tumor metastasis occurs through a series of successive rate-limiting steps. At present, metastasis and implantation of tumor can be summarized as the following significant stages117–119:
The proliferation of primary cancer cells and the formation of new blood vessels. Tumor cells invade the basement membrane and enter the vasculature. Tumor cells circulate in the form of a single cell or cell cluster. Stagnating in the distant capillary. Extravasation into the target organ parenchyma to form colonization.
Tumor invasion and metastasis is an initiative, nonrandom, multistep process, with relatively specific patterns and rules, and many substances participate in the above process, which involves oncogenes, tumor suppressor genes, proteolytic enzymes, and many cytokines and regulatory factors. In the early stages of metastasis and implantation, the tumor microenvironment (TME) composed of tumor cells, extracellular matrix, and mesenchymal tissue is critical. Among them, fibrocytes and immune cells like tumor-associated macrophages or mast cells can provide a robust supportive environment for tumor proliferation, angiogenesis, and degradation of extracellular matrix by secreting a variety of substances, mainly including matrix metalloproteinase (MMPs), cyclooxygenase 2 (COX2), vascular endothelial growth factor (VEGF), tumor necrosis factor (TNF), hypoxia-inducible factor (HIF), platelet-derived growth factor (PDGF), and so on.120–122 After tumor cells enter the circulation, circulating tumor cells (CTCs) will exist in the form of single cells or cell clusters,
123
which can avoid damage such as blood shear force, oxidative stress, immune surveillance, and other damages through the mechanical barrier formed by platelets.
124
Tumor cells arriving at new target organs are vulnerable to immune surveillance mediated primarily by T cells and natural killer (NK) cells.
119
Only a fraction of CTCs can survive and then infiltrate the target organ for colonization. Among the above, gene regulation plays a complex and extensive role. Thus, tumor metastasis involves multistep, multistage, and multifactor changes. In laboratory studies, inhalation anesthetics may have different effects on these key metastatic events (Figure 1).
Inhalation Anesthesia and Cell Proliferation and Apoptosis
It is well known that the most prominent feature of tumors is abnormal cell proliferation accompanied by a decrease in apoptosis. Apoptosis is a kind of programmed cell death, mainly through the external pathway mediated by CD95/Fas receptor or TNF receptor and the internal pathway mediated by mitochondria. It plays a vital role in regulating the metastasis efficiency of tumor cells in 3 key steps: cell detachment from the primary environment, circulation, and transplantation after extravasation. 125 In recent years, more and more studies showed that inhalation anesthesia may play a role in tumor cell proliferation and apoptosis.
Sevoflurane
Some studies have found that sevoflurane is associated with the growth and apoptosis of tumor cells. In gliomas, sevoflurane inhibits the proliferation, invasion, and migration of cancer cells and promotes their apoptosis, which is regulated by the IGF-1-PI3K/Akt signaling pathway or Ca2+ dependent CaMKII/JNK cascade reaction.12,13 Consistent with the previous studies, sevoflurane can inhibit the proliferation, invasion, and migration of head and neck squamous cell carcinoma (HNSCC) cells by activating HIF-1α signaling pathway. 14 Similarly, sevoflurane inhibits ovarian cancer cell proliferation in vitro and in vivo and promotes ovarian cancer cell apoptosis in a dose-dependent manner. 15 In addition, sevoflurane can promote apoptosis in other types of lung cancer 16 and colon cancer.17,18 However, after sevoflurane treatment of cervical cancer cells, it was found that cell proliferation and migration increased significantly, and cell apoptosis decreased.19,20 Similarly, sevoflurane exerted a stimulative effect on the proliferation and migration of ovarian cancer cells. 60 This contradictory experimental result may be related to different tumor types. In addition, different experimental conditions also affect the role of sevoflurane. According to a study involving in vivo and in vitro, sevoflurane in vitro can promote Lewis lung carcinoma (LLC) cell proliferation, but it may not affect the proliferation of LLC cells in vivo. 21 Similarly, different sevoflurane treatment concentrations also affected tumor metastasis progression, Deng et al. exposed breast cancer cells to the clinically relevant concentration of sevoflurane, and found that the survival rate of breast cancer cells increased, but exposure to the extreme concentrations and durations paradoxically decreases the survival. 22
Isoflurane
Isoflurane has been shown to induce normal cell apoptosis via the mitochondrial apoptosis pathway.126,127 In a colorectal cancer study, isoflurane treatment can suppress tumor malignant potential by accelerating cell apoptosis. 61 Hu et al. isolated liver cancer cells from liver cancer patients and treated them with isoflurane. They found that isoflurane reduced apoptotic resistance by activating caspase-3 and caspase-8 and inhibiting Bcl-2, and through downregulation of PI3K/AKT-induced NF-κB signaling pathways significantly inhibited migration and invasion. 62 In addition, isoflurane can increase apoptosis in human H4 neuroglioma cells. 63 Nevertheless, a large number of studies have shown the opposite result. Isoflurane treatment of HNSCC cells may increase the degree of malignancy by increasing cell proliferation and inhibiting apoptosis. 64 In addition, isoflurane can also upregulate histone deacetylase 6 through mTOR-dependent pathways to enhance the proliferation of squamous cervical cancer cells. 65 Isoflurane was also observed to promote proliferation, invasion, and migration of bladder cancer cells in a concentration-dependent manner and to reduce apoptosis. 66 Moreover, it is reported that after treatment of glioblastoma stem cells with isoflurane at a clinically relevant concentration (1.2%) and incubation time (6 h), the proliferation of cancer cells increases, and apoptosis is less, the further studies have found that isoflurane enhances the ability of cancer cells to migrate in vitro and the migration distance in vivo was increased. 67 In an in vitro experiment, transient isoflurane exposure (30 min) did not directly affect apoptosis but led to resistance against tumor necrosis factor-related apoptosis-inducing ligand (TRAIL)-induced apoptosis via Cav-1-dependent mechanisms. As TRAIL is a potential anticancer agent, this also suggests that isoflurane treatment may enhance anticancer drug resistance. 68
Halothane
In an in vitro study, clinical doses of halothane were found to exert cytotoxic effects on tumor cells in a time-dependent manner, and halothane had the most substantial inhibitory effect on tumor cell growth compared with sevoflurane and isoflurane. This may be related to the bromine-containing chemical structure of halothane molecules. Another significant result of this study was that the halothane treatment of human colon cancer (Caco-2), human laryngeal cancer (Hep-2), colon cancer lymph node metastasis poorly differentiated cells (SW-620) cell lines all have varying degrees of apoptosis. 17 Similarly, a study showed that after exposure to halothane in vitro, the survival rate of lung cancer A549 cells was significantly reduced, accompanied by DNA damage and apoptosis.75,76 In addition, it has been demonstrated that halothane can inhibit the expression of tumor cell membrane adhesion molecules, causing tumor cells deprived of adhesion ability to undergo a kind of detachment-induced apoptosis, called anoikis. 77 These laboratory data support the pro-apoptotic effect of halothane in a variety of cancers.
Other Inhalation Anesthetics
At clinically relevant doses, desflurane treatment of colon cancer cells does not or only causes slight changes in cell cycle distribution and apoptosis. 79 For nitrous oxide, in vitro studies, have shown that nitrous oxide rapidly inhibits methionine synthase by depleting vitamin B12, thus inhibiting proliferation and promoting apoptosis in a variety of cell lines. 82 Furthermore, an in vitro study confirmed that xenon inhibits the migration of breast cancer cells. 83 In short, there are relatively few studies on the effects of desflurane, nitrous oxide, and xenon on tumor cell proliferation and apoptosis, and further experiments are still needed to verify their mechanism of action.
Inhalation Anesthesia and Tumor Angiogenesis
Tumor angiogenesis plays a vital role in tumor metastasis. When tumor cells are genetically changed, or related inflammation and immune cells are recruited, the expression of angiogenic factors increases, including VEGF, PDGF, COX-2, and transforming growth factor-α(TGF-α), chemokines, etc. 128 Under the induction of the above factors, endothelial cells proliferate and assemble into tubular structures, or form vessel-like structures through a process denoted as vascular mimicry. The formation of new tumor blood vessels provides an essential pathway for the growth of primary and metastatic tumors to transport nutrients and remove metabolic waste. On the other hand, it also provides an important pathway for tumors to leave the primary site and enter the bloodstream, extensively involved in tumor cell growth, metastasis, and colonization process.129–131 Some studies have suggested that tumor angiogenesis may be affected by inhalation anesthesia.
Sevoflurane
HIF-1 is a major transcription factor in response to hypoxia and regulates the production of VEGF.132,133 Previous studies have shown that sevoflurane can induce the expression of HIF-1α and VEGF in a concentration and time-dependent manner after treating glioma stem cells in vitro, thereby promoting tumor progression. in which the PI3K/Akt signaling pathway may play an important role. 23 However, under hypoxia, sevoflurane treatment will down-regulate HIF-1α expression in lung adenocarcinoma A549 cells and inhibit the invasiveness of tumor cells induced by hypoxia. 24 In addition, sevoflurane also has been shown to prevent invasion by reducing hypoxia-induced VEGF levels, which is independent of the HIF-1α pathway. 25 These studies show that sevoflurane can promote tumor angiogenesis in vitro, but in hypoxic conditions, sevoflurane can inhibit hypoxia-induced angiogenesis.
Isoflurane
An experiment noted that isoflurane treatment increases the expression of VEGF and angiopoietin-1 in ovarian cancer cells, promoting tumor angiogenesis, and increasing aggressiveness. 69 Consistently, isoflurane increased the expression of HIF-1α, HIF-2α, and VEGF in human renal carcinoma cells in a timeand concentration-dependent manner, which was associated with poor prognosis. 70 In addition, the increase of HIF-1 and malignant potential after isoflurane treatment was also observed in bladder cancer 41 and prostate cancer. 71 The above-mentioned studies show the adverse effects of isoflurane on tumors in vitro to varying degrees, but a recent study has put forward a different point of view. Sumi et al. used a type of RCC4-EV cell derived from human renal cell carcinoma, which lacks VHL (a tumor suppressor that targets the degradation of HIF), even under normoxic conditions HIF-1 and HIF-2 activated. They found isoflurane treatment did not upregulate HIF-1α and HIF-2α expression in RCC4-EV cells under 20% O2 conditions, and further studies confirmed that isoflurane also did not affect the expression of genes associated with cancer hallmarks. 72 Therefore, the inhibitory effect of isoflurane on tumor angiogenesis still needs to be verified in different tumor types.
Other Inhalation Anesthetics
Xenon, a relatively ideal anesthetic gas, has been shown to play a protective role in renal ischemia-reperfusion by inducing the expression of HIF-1α and its downstream VEGF. 134 Similarly, xenon inhibits migration and reduces the secretion of the angiogenic cytokine RANTES/CCL5 compared to sevoflurane in breast cancer. 83 At the same time, other anesthetic gases, such as nitrous oxide, desflurane, and halothane, are rarely studied in tumor angiogenesis, and still need further exploration and discovery.
Inhalation Anesthesia and Matrix Invasion
The tight connection between the extracellular matrix (ECM), basement membrane and vascular system is a barrier that tumor cell metastasis must overcome. During the local invasion stage of the tumor cells, zinc-dependent MMPs play an essential role in ECM degradation. MMPs are the main enzymes that degrade ECM in the human body, and they can decompose almost all the basic structural components of ECM except polysaccharides, thereby promoting tumor cell infiltration and metastasis. On the other hand, it can also participate in tumor growth and angiogenesis by regulating TGF-β, EGFR, VEGF, and other substances.135,136 Among them, gelatinases MMP-2 and MMP-9 are the most widely studied matrix metalloprotd it has been shown to be highly expressed in many types of cancer, such as bladder cancer, 137 breast cancer, 138 prostate cancer, 139 and colorectal cancer, 140 even can be used as a potential biomarker for cancer. 141 Other types of MMP-1, MMP-3, and MMP-11 are also involved in tumor progression. 142
Sevoflurane
One study revealed that in colon cancer, 2.2% sevoflurane pretreatment inhibited IL-8-induced MMP-9 expression, further alleviating extracellular matrix degradation and subsequent cell invasion. 26 Similarly, in glioblastoma sevoflurane has been shown to inhibit MMP-2 activity and tumor cell migration. 27 In addition, in studies on ovarian cancer, sevoflurane can inhibit the expression of MMP-2 and MMP-9, and inhibit the invasion of cells, the mechanism of which is related to the JNK and P38 MAPK signaling pathway. 15 In an in vitro study, sevoflurane treatment reduced MMP-16 expression, thereby inhibiting glioma cell migration and invasion. 28 In addition to acting alone, sevoflurane can act synergistically with chemotherapy drugs. Studies have confirmed that sevoflurane and cisplatin (DDP) can have a stronger inhibitory effect on tumor cell growth and invasion. The synergy of the two drugs will lead to a significant down-regulation of XIAP, Survivin, MMP-2, and MMP-9, and the synergistic effect of invasion inhibition may be closely related to the down-regulation of MMP-2 and MMP-9. 29 Therefore, sevoflurane inhibits matrix degradation and increases sensitivity to chemotherapeutic agents in some tumors.
Desflurane
One study conducted the effect of volatile anesthetics on the expression of metastasis gene in human ovarian cancer SKOV-3 cells, it was found that the expression of MMP-11 mRNA was significantly increased after pretreatment with desflurane, indicating that desflurane is possible to promote the degradation of basement membrane and the tumor metastasis. 80 The opposite effect was observed in colon cancer cells. Pretreatment with desflurane decreased MMP-9 release and inhibited tumor cell migration. 26 These differences may be related to tumor cell types, desflurane concentration and treatment time, gene and protein expression, and the specific mechanisms, which need to be further explored.
Inhalation Anesthesia and Platelets
Platelets are a crucial factor in protecting the safety of tumor cells in circulation. Platelets can form complexes with tumor cells through adhesion molecules such as integrin or platelet p-selectin on the membrane to help cancer cells escape from the immune surveillance and high shear force damage caused by blood flow, and accelerate the adhesion of tumor cells to the endothelium. 143 Furthermore, platelets, as a vital source of TGF-β, enhance tumor epithelial-mesenchymal transition and involve in tumor growth, proliferation, and angiogenesis.144,145 Camerer et al. demonstrated that lung metastasis in mice is closely associated with changes in platelet count and function. This study used an NF-E2-deficient mouse model with few circulating platelets, followed by tail vein injection of B16-F10 melanoma cells to measure lung metastasis by counting tumor cells, and the final results found that the median tumor count, tumor burden, and maximum surface tumor number in NF-E2–/– mice were lower than in the control group. 146 Thus, the interaction between platelets and tumor cells is the precondition of successful blood metastasis. However, there is still a lack of tumor-related research on the effect of inhalation anesthesia on platelets.
Sevoflurane
Sevoflurane, rather than isoflurane, has been found to reduce the invasiveness of lung cancer cells in vitro by inhibiting platelet activity. 30 The mechanism by which sevoflurane inhibits platelet activation remains unclear, and some studies suggest that may be at least partly by adjusting the platelet p-select expression, and decreased expression of platelet p-selectin results in decreased binding of tumor cells to platelets, thereby inhibiting tumor cell metastasis. 147 Moreover, sevoflurane can also impair platelet activation by inhibiting cyclooxygenase activity or thromboxane A2.148,149 However, in a nonneoplastic in vitro study, sevoflurane has been found to enhance the expression of platelet p-selectin and enhance its binding to lymphocytes, neutrophils, and monocytes. 150 This has also been verified in vivo studies. The inhalation of low-dose sevoflurane in humans can inhibit the aggregation of platelets and granulocytes induced by agonists. 151
Other Inhalation Anesthetics
At present, there are relatively few studies on the ability of other inhaled anesthetics to interfere with tumor metastasis through platelets. Therefore, we have reviewed a large number of nontumor studies on the effects of inhaled anesthetics on platelet activity. In an in vitro study, clinically relevant concentrations of xenon did not affect the expression of platelet p-selectin. 152 Nitrous oxide promotes platelet aggregation, which can be reversed by the addition of halogenated anesthetics halothane or isoflurane. 153 Further studies have shown that halothane,154–156 isoflurane,157–159 and desflurane 154 have antiplatelet activity, which may inhibit tumor metastasis to some extent. Paradoxically, under different experimental conditions, these inhaled anesthetics have no effect on platelets 160 or even the opposite effect. 161 Therefore, there is still much work to be done on the effects of inhalation anesthesia on platelet function in tumor research.
Inhalation Anesthesia and Immune Response
The interaction between tumor cells and immunity is a research hotspot in the process of tumor metastasis. The primary tumor microenvironment is induced by tumor cells to form a relatively immunosuppressed environment, cancer cells that leave this survival zone are vulnerable to immune cells and molecule-mediated immune surveillance and therefore are attacked in circulation or metastatic organs. In this process, only a few tumor cells survive to form metastases.162–164 Thus, the influence of inhalation anesthesia on the immune response is significant to the prognosis of tumor patients.
Sevoflurane
There is a growing body of evidence that anesthesia can cause dysfunction of NK cells and helper and cytotoxic T cells, resulting in increased immunosuppression and metastasis. 165 In an in vitro study, sevoflurane inhibited NK cytotoxicity and increased migration in nonsmall cell lung cancer. 31 Another study reported that in vivo experiments on mice, repeated exposure to sevoflurane inhalation anesthesia resulted in a decrease in the absolute numbers of peripheral white blood cell and lymphocyte counts. 166 In addition, the mechanism of sevoflurane attenuating NK cell-mediated cytotoxicity may be related to the inhibition of adhesion molecule leukocyte function-associated antigen-1 (LFA-1). 32 Similarly, Buckley et al. co-cultured the serum of breast cancer patients who received sevoflurane-opioid (GA) anesthesia with primary NK cells and found that the serum of the GA group reduced the NK cell activation receptor CD16, IL-10, and IL-1β level. 33 The immunosuppressive effect of sevoflurane has also been verified in clinical studies. In the randomized controlled trial of patients undergoing laparoscopic radical hysterectomy for cervical cancer, it was found that the immune indexes of the sevoflurane group were all lower than the basic level. CD3+ cell count, CD4+ cell count, NK cell count, and CD4+ /CD8+ ratio in the sevoflurane group were significantly lower than those in the propofol group. 111 Consistently, in breast cancer surgery patients, sevoflurane anesthesia combined with fentanyl postoperative analgesia can adversely affect the immune function of the patient by reducing the toxicity of NK cells. 86 In addition, recent studies have shown that IL-6 plays a key role the process of sevoflurane in promoting lung metastasis of breast cancer. Specifically, sevoflurane can increase the level of IL-6 in serum and further activate STAT3 and the infiltration of CD11b+ myeloid cells into the lung and promotes the initiation of the lung microenvironment of metastatic tumors. 34 Paradoxically, sevoflurane may play a beneficial role by improving the immunosuppression of the tumor microenvironment. Tumor-associated macrophages (TAM), as the “undercover” of immune cells, can promote tumor growth and survival, angiogenesis, and immunosuppression. Sztwiertnia et al. found that treatment with sevoflurane can significantly reduce TAM and play a beneficial effect in the mouse melanoma model. 35
Isoflurane
Isoflurane has been shown to induce apoptosis of human T lymphocytes in a dose-dependent manner, 126 and the inhibitory effect of isoflurane on NK cells has also been observed in tumor cells. 32 Gender differences should also be taken into account when studying the effects of inhalation anesthesia on immune function. Meier et al. demonstrated in a male and female mouse melanoma model that the tumor growth rate of male mice with perfect immune function will increase after exposure to isoflurane, but it has no effect in females with perfect immune function. 73 Thus, isoflurane affects melanoma growth in mice in a sex-specific, immune-dependent manner.
Other Inhalation Anesthetics
In other types of inhalation anesthetics, desflurane maintained IL-2/IL-4 and CD4+/CD8 + T cell ratios, while there was no significant change in the number of NK cells in the desflurane anesthetized group compared with the propofol anesthetized group. 167 In rats, halothane anesthesia resulted in decreased NK cell activity and increased lung retention of tumor cells. 78 Also, nitrous oxide exhibited some degree of immunosuppressive activity in vitro. 168 In addition, xenon anesthesia had no significant difference in white blood cell function compared with sevoflurane anesthesia in nontumor surgical studies, but xenon anesthesia can result in fewer lymphocytes. 169 However, the effect of these inhaled anesthetics on the immunity of tumor patients is limited and further investigation research is needed.
Inhalation Anesthesia and Gene Expression
MicroRNA (miRNA) are small noncoding RNA that participate in negative posttranscriptional regulation of gene expression mainly through translation inhibition, mRNA cleavage, and mRNA decay induced by miRNA-guided rapid deadenylation. 170 Dysregulated miRNAs can act as tumor suppressor genes or oncogenes to regulate tumor growth, invasion, angiogenesis, and immune evasion.171,172In addition, miRNA can be regulated by circular RNA (circRNA), which are novel endogenous noncoding RNA with characteristics of conservation, abundance, and tissue specificity. 173 Research shows that circRNA is closely related to the progression of many types of cancer. Because circRNA molecules are rich in miRNA binding sites, they can act as miRNA “sponges,” competitively inhibit the binding of miRNAs to their mRNA targets, and increase the level of target genes.174,175 Recent many studies have found that inhalation anesthesia can regulate miRNA or circRNA expression in cancer.
Sevoflurane
miR-25-3p is a well-known oncogenic miRNA. Sevoflurane can inhibit the proliferation and invasion of liver cancer cells by down-regulating the expression of miR-25-3p and regulating the PTEN/Akt/GSK-3β/β-catenin signaling pathway. 36 In addition, a study found that sevoflurane can restore the down-regulated miR-29a in liver cancer tissues and cells, resulting in down-regulating the expression of Dnmt3a to play an anti-tumor effect. 37 In other types of cancer, sevoflurane can inhibit papillary thyroid carcinoma cells activity in a dose-dependent manner, primarily by down-regulating cytosolic miR-155 to enhance cell apoptosis, and inhibit migration and invasion. 38 In colorectal cancer, sevoflurane can inhibit cancer cell progression by upregulating miR-34a, 39 miR-203, 40 miR-331-3p, 41 miR-622, 42 or miR-637. 43 Sevoflurane also inhibits breast cancer cell proliferation by upregulating miR-203. 44 Similarly, sevoflurane also attenuates the proliferation and migration of gastric cancer by upregulating miR-34a and inhibiting TGIF2 expression. 45 In lung cancer, sevoflurane also can promote apoptosis by interfering with miRNA expression that regulates apoptosis. 46 Also, sevoflurane promotes the apoptosis of laryngeal squamous cell carcinoma in-vitro and inhibits its malignant progression via miR-26a/FOXO1 axis. 47 In a large number of glioma studies, sevoflurane has shown anti-tumor effects through multiple miRNA pathways, For example, increasing the expression of miR-637, 48 miR-124-3p, 49 miR-34a-5p, 50 miR-146b-5p, 28 miR-210, 51 miR-27b, 52 or miR-144-3p 53 to regulate its corresponding downstream molecules and inhibit the migration and invasion of glioma cells. In addition to directly acting on miRNA, sevoflurane can play a regulatory role by acting on upstream circRNA. He et al. confirmed that circ-HMGCS1 was downregulated by sevoflurane treatment and knockdown of circ-HMGCS1 suppressed SGPP1 expression via sponging miR-34a-5p, which ultimately inhibited the progression of colon cancer. 54 Moreover, a study has confirmed that sevoflurane can block glioma progression by increasing circRNA reelin (circRELN) expression, and circRELN played a role in glioma partly by regulating the miR-1290/RORA network. 55 Similarly, other circRNA-miRNA axes are involved in sevoflurane-mediated glioma inhibition. For example, has_circ_0012129/miR-761/TGIF2, 56 circ_0002755/miR-628-5p/MAGT1, 57 circ_0000215/miR-1200/NCR3LG1, 58 circ_0079593/miR-633/ROCK1, 59 and so on. However, contrary to the above anti-tumor results, sevoflurane has been observed to enhance the malignancy of ovarian cancer cells by inhibiting the expression of miR-138 or miR-210. 60 Overall, sevoflurane exerts some anticancer effects by modulating circRNA or downstream miRNA in most tumor types.
Isoflurane and Desflurane
A study has shown that isoflurane can promote glucose metabolism and inhibit mitochondrial oxidative phosphorylation by upregulation of miR-21 in ovarian cancer cells, suggesting that isoflurane treatment can promote the metabolic transformation of ovarian cancer cells, leading to aggravated malignant transformation. 74 In addition, desflurane can respectively inhibit HIF1-α and MMP-9 expression through miR-138 and miR-335, thereby exerting anti-neuroglioma effects. 51 However, in ovarian cancer, desflurane exposure enhances cell proliferation and migration of ovarian cancer cells through down-regulation of miR-138. 60 Similarly, desflurane anesthesia confers colorectal cancer cells metastatic capacity through deregulation of miR-34a/LOXL3. 81
Inhalation Anesthesia and the Prognosis of Cancer Surgery Patients
Many studies have revealed the influence of anesthesia on the prognosis of cancer patients, and this article summarizes the clinical studies related to the influence of inhalation anesthesia on the prognosis of cancer patients in the recent 5 years (Table 2). Some of these studies have shown that inhalation anesthesia does not affect the prognosis of cancer patients after surgery. In certain types of surgery, such as digestive cancer, 101 breast cancer,87,89–95 high-grade glioma, 113 colorectal cancer,96,99 colon cancer, 25 oral cancer, 115 and gastric cancer, 102 there was no significant difference between inhalation anesthetics and propofol in tumor patients immunity, circulating tumor cells, or survival outcomes. Consistent with these results, after anesthesia with desflurane or isoflurane in glioblastoma, the survival rate after surgery is similar, and the addition of propofol is not associated with longer survival. 112 However, there may be differences between the various inhalation anesthetics. For example, xenon anesthesia in renal cell carcinoma surgery showed no significant effect on early renal function but less adverse events compared to isoflurane. 109 Similarly, in lung cancer, sevoflurane can inhibit tumor cell invasion by inhibiting platelet activation compared with isoflurane. 30
Nevertheless, some studies have put forward the opposite view that inhalation anesthesia may be related to poor clinical prognosis. In colorectal cancer, a retrospective study showed that exposure to inhalation anesthetics is associated with an increased risk of recurrence. 97 Another retrospective study also confirmed that in patients undergoing gynecologic cancer, sevoflurane anesthesia is associated with worse overall, cancer-specific, and recurrence-free survival. 110 thus, some studies recommend intravenous anesthesia and local anesthesia alone or in combination with tumor anesthesia. In a retrospective study of HCC patients, it was found that compared with desflurane anesthesia, Propofol anesthesia is associated with longer survival, with significantly reduced distant metastasis and local recurrence. 104 Similarly, clinical studies of other types of tumors have confirmed the adverse effects of inhalation anesthesia on the prognosis of tumors, and propofol anesthesia is more recommended.84,98,100,105–107,111 In addition, in a clinical randomized controlled study on breast cancer surgery, inhalation anesthesia did not show an excellent anticancer effect, and lidocaine may reduce recurrence. 85 Similarly, in some types of tumor surgery, the combined use of intravenous anesthesia and local anesthesia techniques will show better results than inhalation anesthesia.88,108,114
Therefore, the above series of studies indicate that inhalation anesthesia has no significant effect on the prognosis or leads to poor survival results in most types of tumors. However, a large part of this evidence is retrospective studies and may be biased, and future prospective multicenter studies are needed to determine the impact of inhaled anesthesia on the prognosis of cancer patients.
Conclusion
Inhalation anesthesia can trigger different molecules and pathways to act on the whole process of tumor metastasis and play an interference role in tumor progression. Sevoflurane, as one of the commonly used inhalation anesthetics in clinical practice, has been widely studied in tumor metastasis, but its role in tumor biological behavior and gene regulation is still uncertain. In addition, sevoflurane has been shown to have significant immunosuppressive and cancer-promoting properties in most studies and reviews. However, a study has shown that sevoflurane can improve the immunosuppression of the tumor microenvironment by reducing TAMs. In some tumor types, isoflurane can promote the occurrence and development of some tumors and lead to malignant progressions through different mechanisms, such as regulating the activity of cancer cells, promoting tumor angiogenesis, inhibiting immune function, and regulating oncogenic gene expression. Besides, there are a few studies on halothane, desflurane, nitrous oxide, and xenon, but it is worth noting that xenon inhibited tumor angiogenesis and invasion in a laboratory study, and further clinical studies showed that xenon has a good effect in reducing adverse events in patients with kidney cancer surgery. Although it is expensive and has not been widely used in the clinic, the role of xenon in anticancer is worthy of further study. In summary, the effects of inhalation anesthetics on tumor metastasis remain uncertain and contradictory, which may be mainly due to the specificity of tumor types and cell lines, the lack of simulation of complex tumor growth environments, and differences in inhaled anesthetics types, treatment concentration and time.
In recent years, with the rapid development of genetic testing technology and bioinformatics technology, noncoding RNAs have been extensively studied to explain the effects of inhalation anesthesia on tumor metastasis at the gene level as much as possible, but there are still many deficiencies. First, platelet activity has been widely recognized as a key factor interfering with tumor cell survival, but the effect of inhalation anesthesia on platelets in tumor patients has been largely unstudied. Second, most of the current studies rely on a single tumor type, and the findings cannot be applied to most tumor types due to the variability among different tumors. Third, the current study does not comprehensively cover all types of inhalation anesthetics, inhalation anesthetic concentrations, and methods of use. At last, current studies mainly rely on in vitro studies between specific cancer cells and related molecules, pathways, immune cells, platelets, and other factors under the treatment of inhalation anesthesia, which lacks the simulation of the complex overall environment of tumors. These research results still need to be further verified in vivo and in the clinical environment. In the future, it is necessary to improve in vivo experiments of inhaled anesthetics involving more tumor types, types, and concentrations, and complete large-sample multicenter prospective clinical studies. At the same time, the synergistic influence of inhalation anesthesia with perioperative anti-inflammatory and analgesic factors, blood transfusion, vasoactive drugs, and other factors should be considered in tumor metastasis, to provide personalized anesthesia programs for patients undergoing tumor surgery.
Footnotes
Ethics Statement
This article does not contain any studies with human participants or animals.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article