
Abstract
Keywords
Introduction
Pancreatic squamous cell carcinoma (PSCC) is a rare exocrine pancreatic malignancy, accounting for 0.5% to 3.5% of all pancreatic neoplasms.1,2 Chronic inflammation (ex. chronic pancreatitis) causes malignant metaplasia of ductal columnar cells to squamous cells, which is the leading cause of PSCC. 3 Besides, malignant differentiation of a progenitor cell into squamous cell carcinoma (SCC) and cancerization of an aberrant squamous cell are possible theories inducing PSCC. 4 Due to the rarity of PSCC, other common histologic types should always be excluded before the identified diagnosis of it. 5 Pancreatic adenocarcinoma (PAC) is the most frequent pancreatic malignancy which consists of 90% primary pancreatic cancers. 6 Based on the data available, male, black, and elders have a higher incidence suffering from pancreatic cancers, which suits PAC as well.7,8 Patients in developed countries acquire higher mortality and incidence rate than developing countries. 9
Nowadays, the epidemiology and clinicopathologic characters of PAC have been widely explored while studies focusing on PSCC are documented in case reports and retrospective studies with small sample size.2,5,10 Given the uncommon disease characters and a lack of clinical experience, information on treatment patterns and survival outcomes remains limited. Treatment modalities of PSCC are similar to that of PAC and there is no standard of care for it. 11 Surgery is still the mainstay treatment when tumors are operable. 12 Chemotherapy is always applied as neoadjuvant therapy or to PSCC patients without indications of operation. 13 However, the therapeutic effects to PSCC have not been systemically reviewed. Therefore, in our case-control study, we analyze the survival and potential risk factors of PSCC, comparing the differences between PSCC and PAC based on Surveillance, Epidemiology and End Results (SEER) database, in search for better treatment modalities for it.
Materials and Methods
Patients and Data Collection
Patients diagnosed with PSCC and PAC between January 1, 2004 and December 31, 2015 in SEER Research Plus Data, 18 registries were enrolled for our case-control study. PSCC and PAC were defined according to the International Classification of Diseases for Oncology, third edition (ICD-O-3). Morphology codes used in SCC were 8070/3-8076/3 and in adenocarcinoma (AC) were 8140/3, 8141/3, 8211/3, 8480/3, 8481/3.14,15 Topographical codes were C25.0 (Head), C25.1 (Body), C25.2 (Tail), C25.3 (Duct), C25.7 (Other specified parts), C25.8 (Overlapping lesions), C25.9 (NOS). TNM stage was recorded according to the 6th edition of American Joint Committee on Cancer (AJCC). Patients met all the following criteria were eligible: (1) age ≥ 18; (2) diagnosed with primary PAC or PSCC; (2) survival time ≥ 1 month; (3) complete information on demographics, clinicopathologic characteristics, treatment, and survival. Patients with unknown race, SEER stage, TNM stage, survival time < 1, age < 18, diagnosis without positive exfoliative cytology, microscopic or histological confirmation were excluded (Figure 1).
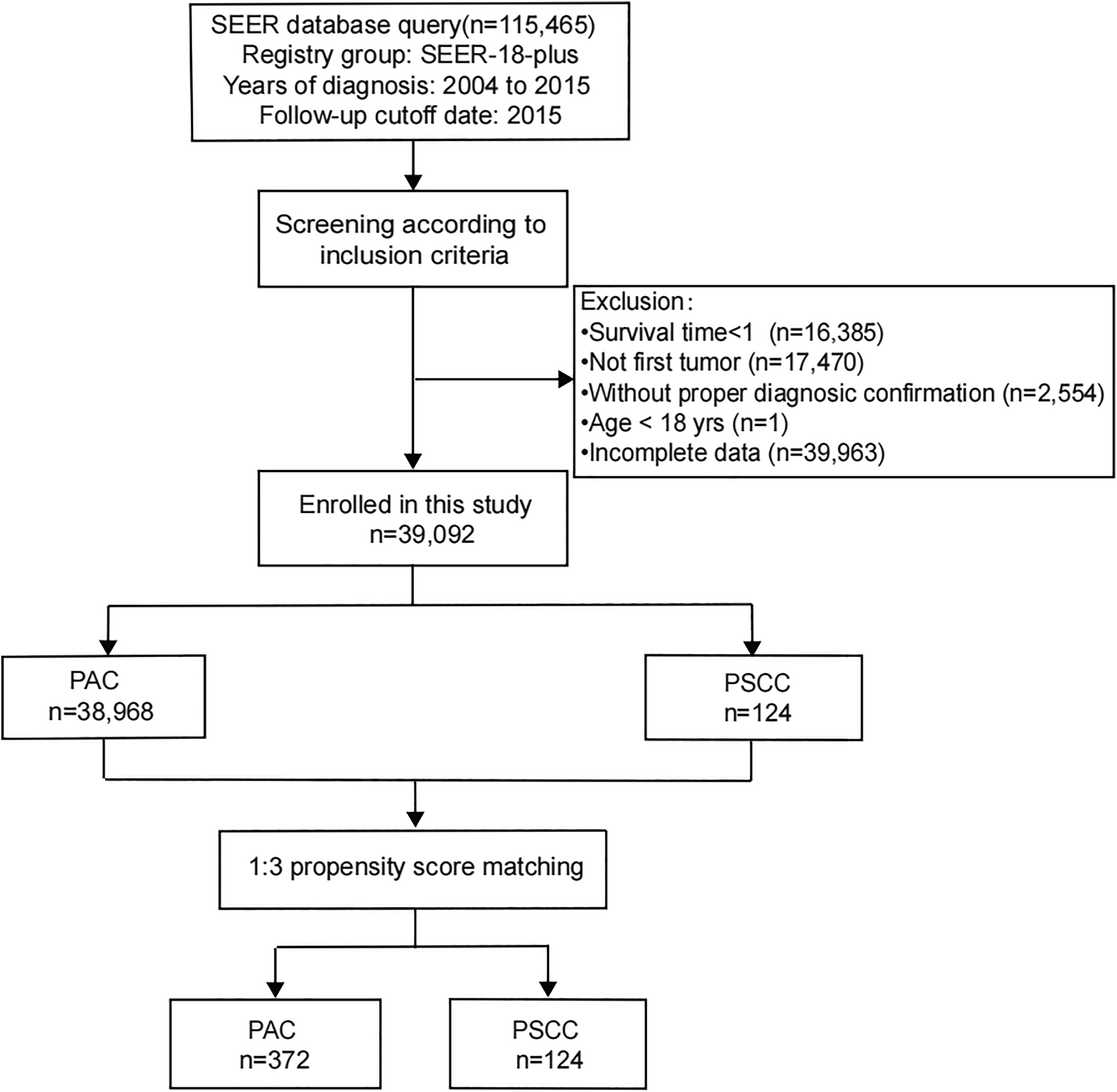
Flow diagram showing process of selecting patients.
Variables
Age was defined as categorical variables divided as following intervals: ≤40; 40-60; >60. Besides, categorical variables abstracted from SEER also include sex, race, primary location, marital status, SEER stage (reginal, localized, distant disease), grade, TNM stage, treatment modalities (surgery, chemotherapy, radiation therapy).
Data Analysis
Categorical variables were expressed as counts and percentages. Unordered categorical variables of demographics and clinicopathological characteristics were compared by chi-square test while ordered categorical variables were compared by rank sum test. OS and CSS are outcome variables. OS represents the lifetime which is ceased because of any reasons while CSS documents death caused by cancer. Propensity-score matching (PSM) was performed to eliminate the influence of confounding factors using logistic regression. A 1:3 matching between patients with PAC and PSCC were accomplished using the nearest neighbor matching method with a caliper width equal to 0.20 standard deviation of logit of propensity score. Matched variables contain all the categorical variables which are statistically significant in multivariate analyses of PSCC and PAC cohorts before PSM (Tables 1 and 2; Supplementary Table 1). Kaplan-Meier analyses were performed to analyze OS and CSS. Survival curves of treatment modalities were compared by log-rank test. Univariate and multivariate cox proportional hazards analyses were used in multiple variables for suspicion of risk factors. PSM was performed by R version 3.6.2 (http://www.R-project.org). Statistical analysis was conducted by SPSS version 25 (IBM). P < .05 indicated statistical significance. The reporting of this study conforms to RECORD guidelines. 16
Univariate and Multivariate Cox Analyses of Patients With PSCC Before PSM.
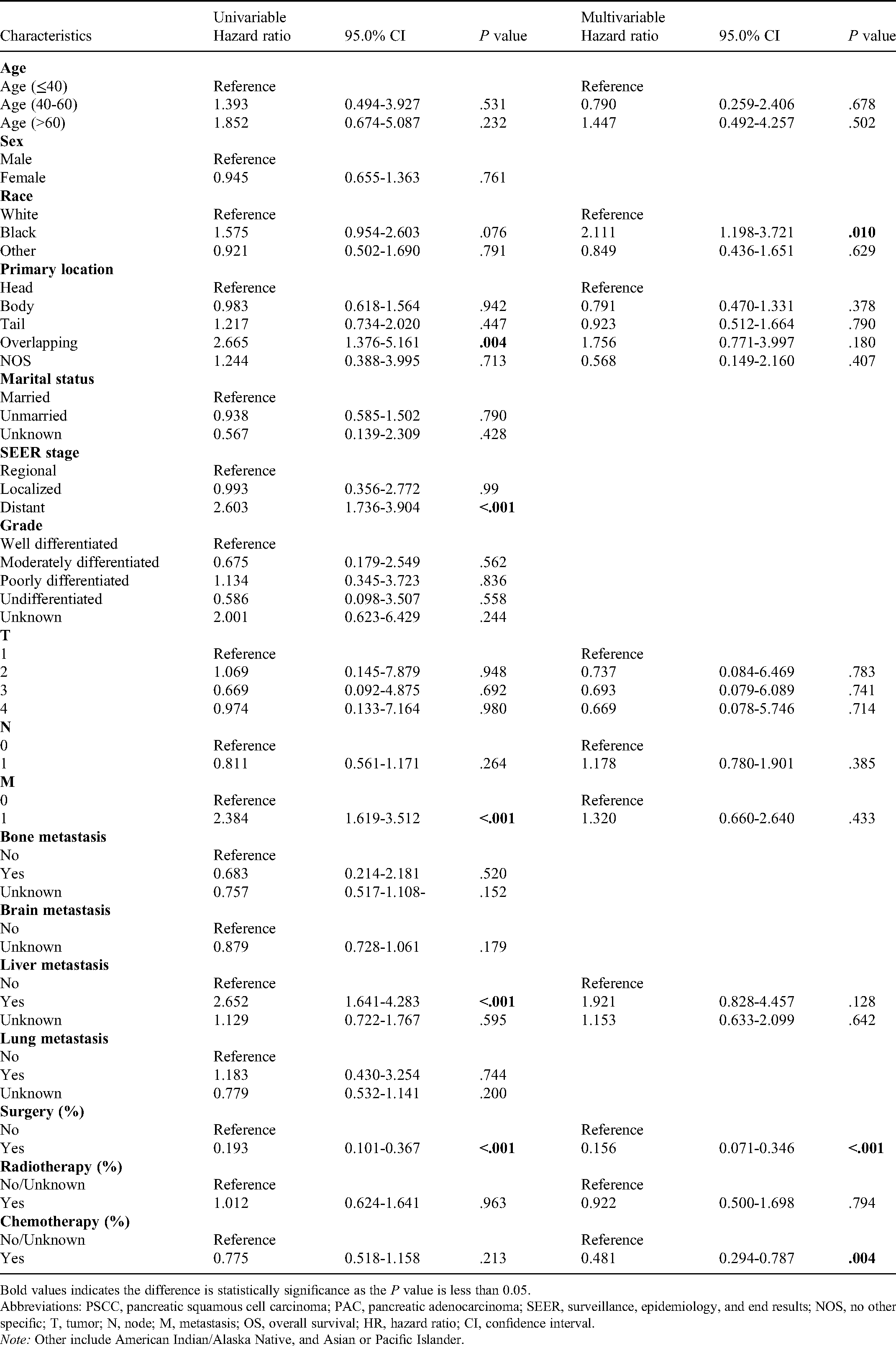
Bold values indicates the difference is statistically significance as the P value is less than 0.05.
Abbreviations: PSCC, pancreatic squamous cell carcinoma; PAC, pancreatic adenocarcinoma; SEER, surveillance, epidemiology, and end results; NOS, no other specific; T, tumor; N, node; M, metastasis; OS, overall survival; HR, hazard ratio; CI, confidence interval.
Note: Other include American Indian/Alaska Native, and Asian or Pacific Islander.
Univariate and Multivariate Cox Analyses of Patients With PAC Before PSM.

Bold values indicates the difference is statistically significance as the P value is less than 0.05.
Abbreviations: PSCC, pancreatic squamous cell carcinoma; PAC, pancreatic adenocarcinoma; SEER, surveillance, epidemiology, and end results; NOS, no other specific; T, tumor; N, node; M, metastasis; OS, overall survival; HR, hazard ratio; CI, confidence interval.
Note: Other include American Indian/Alaska Native, and Asian or Pacific Islander.
Results
Demographic Patterns and Clinicopathologic Characteristics of Study Cohort
A total number of 39 092 patients who met the inclusive criteria were eligible in this study, consisting of 99.7% PAC patients (n = 38 968) and 0.3% PSCC patients (n = 124). After 1:3 PSM, 124 PSCC patients and 372 PAC patients were obtained (Figure 1). Baseline characters of eligible patients were enumerated in Table 3. More than half of patients with PSCC were female while male accounts for a larger proportion in patients with PAC. PSCC was most likely to invade the head of pancreas (46.0%), followed by body (23.4%), then tail (19.4%). In addition, PSCC had a higher tendency to be poorly differentiated than PAC. Compared with PAC, liver metastasis occurred more frequently in patients with PSCC. In PSCC patients, liver was the most common site in single-organ metastasis (86.5%) (Figure 2a). Similar trend was observed in PAC patients with a proportion of 71.2% to liver and 9.0% to lung (Figure 2b). Double-organ metastases mostly occurred in liver and lung both in PAC and PSCC patients. Patients with 4-organ metastases occupied 0.1% in PAC patients while there were no 4-site metastases in PSCC patients.
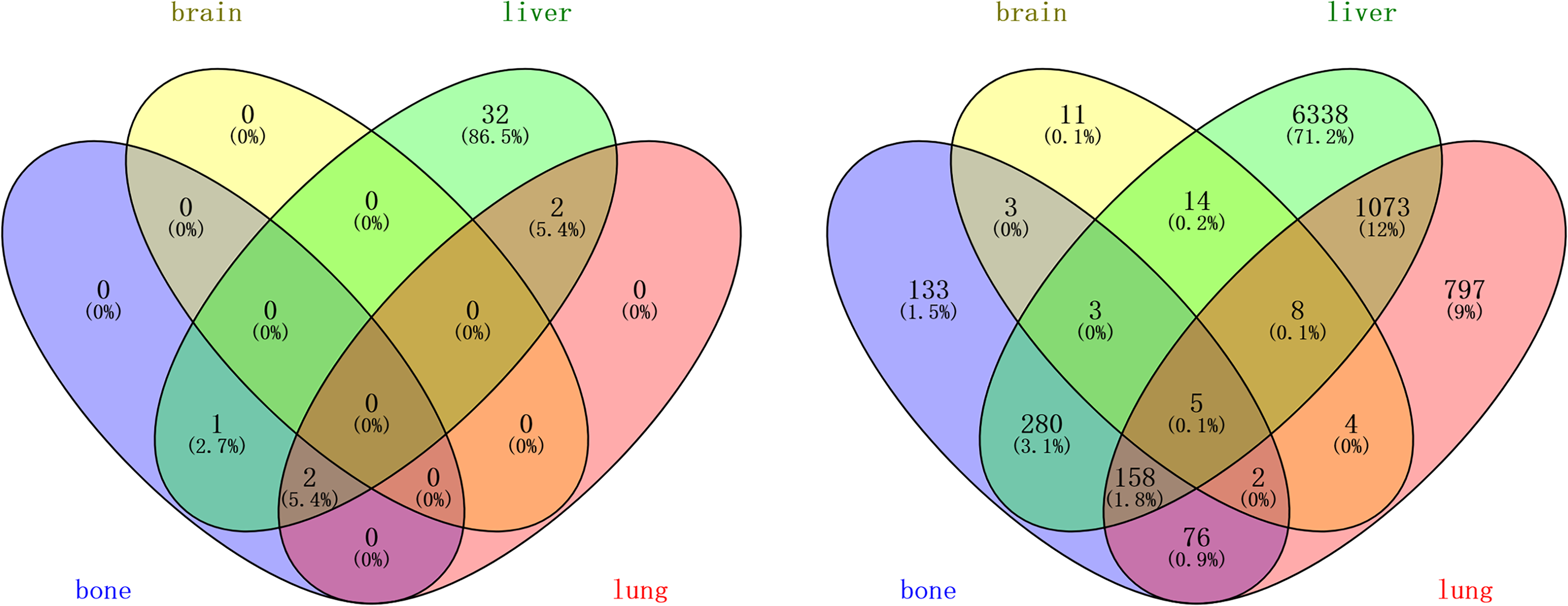
Venn diagram showing distribution of metastasis in (a) PSCC cohort and (b) PAC cohort.
Demographics and Clinicopathological Characteristics of Patients.
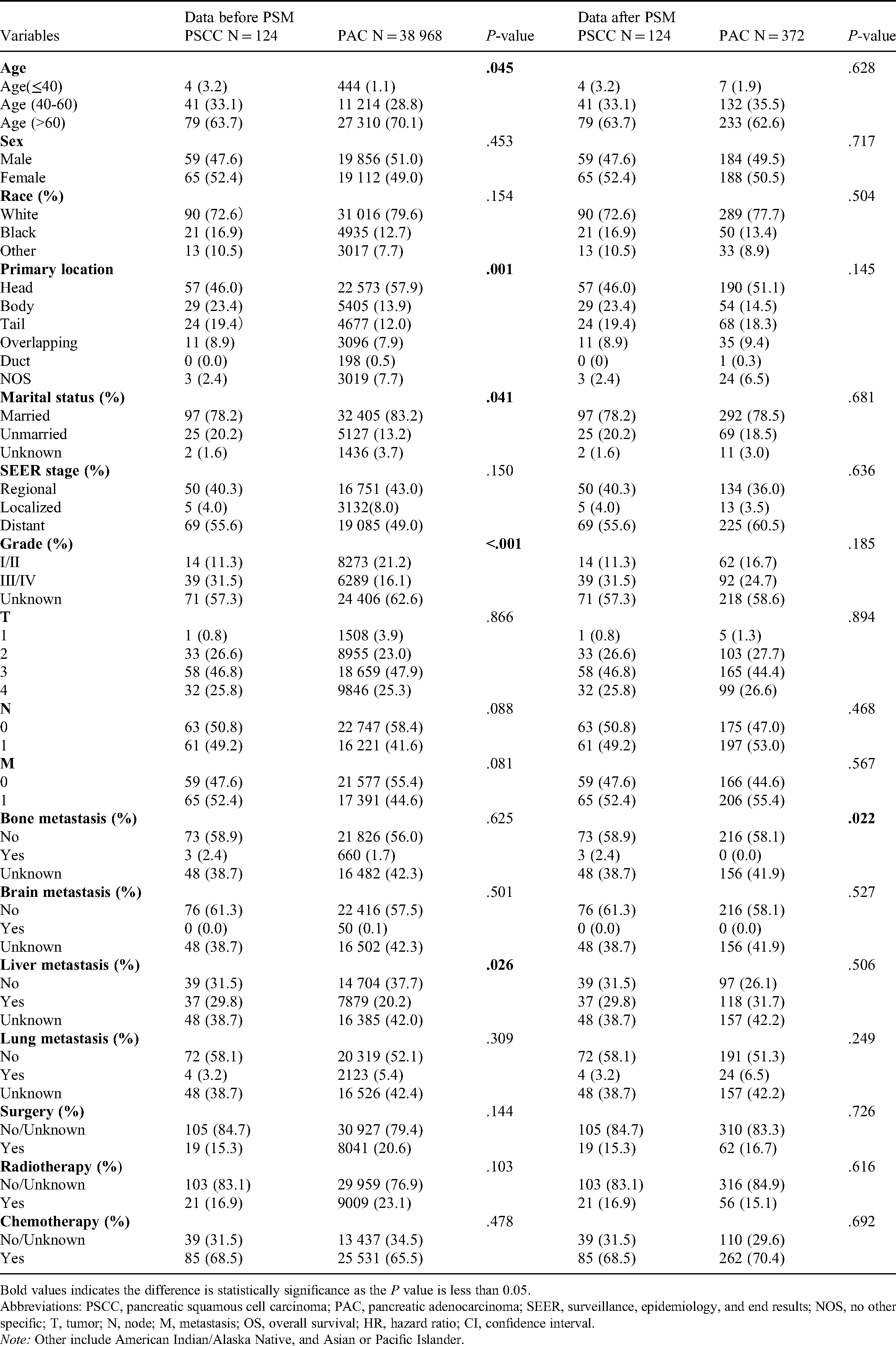
Bold values indicates the difference is statistically significance as the P value is less than 0.05.
Abbreviations: PSCC, pancreatic squamous cell carcinoma; PAC, pancreatic adenocarcinoma; SEER, surveillance, epidemiology, and end results; NOS, no other specific; T, tumor; N, node; M, metastasis; OS, overall survival; HR, hazard ratio; CI, confidence interval.
Note: Other include American Indian/Alaska Native, and Asian or Pacific Islander.
Similarly, PSCC had a higher potential to metastasize distantly. No statistically significant differences were detected in sex, race, SEER stage, TNM stage, metastasis to bone, brain and lung between PAC and PSCC patients. Chemotherapy was the most common treatment modality applied in both groups. Besides, radiation therapy and surgery were conducted less in patients with PSCC than PAC. After the PSM of age, race, primary location, marital status, SEER stage, TNM stage, grade, metastasis to bone, brain and liver, surgery, radiation therapy and chemotherapy, there was no statistically significant difference between PSCC and PAC.
Survival Analysis of PSCC
In univariate analysis of PSCC patients, distant metastasis in SEER stage (HR = 2.603; 95%CI, 1.736-3.904; P < .001) and metastasis in TNM stage (HR = 2.071; 95%CI, 1.460-2.938; P < .001) were prognostic factors which increased the risk of death (Table 1). Conduction of surgery (4 months vs 21 months, HR = 0.260; P < .0001) was associated with improved OS (Figure 3a and d). Similar trend was also observed in CSS (4 months vs 25 months, HR = 0.244; P< .0001). Higher mOS (2 months vs 5 months; HR = 0.806; P = .25) and CSS (2 months vs 6 months; HR = 0.771; P = .17) was achieved with the application of chemotherapy in PSCC patient (Figure 3c and f). Patients with tumors located in overlapping anatomical region of pancreas and tumors metastasizing distantly were associated with a significant worse prognosis. As for organs of metastasis, liver indicated a strong correlation to worse prognosis. After adjusting the confounding factors of each variable, in multivariate analysis, surgery (HR = 0.156; 95%CI, 0.071-0.346; P < .001) and chemotherapy (HR = 0.481; 95%CI, 0.294-0.787; P = .004) were independent predictive factors for better prognosis.

Kaplan-Meier curves of CSS and OS in PSCC patients according to surgery (a and d), radiation (b and e), and chemotherapy (c and f).
Prognosis of PSCC patients was significantly worse than PAC patients, reflected in OS (4 months vs 8 months; HR = 1.287; 95%CI, 1.046-1.584; P = .0046) and CSS (4 months vs 8 months; HR = 1.318; 95%CI, 1.064-1.632; P = .0024) (Figure 4b and a). 1-year, 2-year OS rates were 32.5%, 14.0% in PAC patients and 19.8%, 8.9% in PSCC patients. 1-year, 2-year CSS rates were 34.3%, 15.4% in PAC patients and those in PSCC patients were 21.5%, 9.7%, respectively.

Kaplan-Meier plot and log-rank test of (a) CSS and (b) OS before PSM.
After PSM, PSCC was associated with a worse prognosis than PAC in both OS (4 months vs 7 months; HR = 1.176; 95%CI, 0.944-1.465; P = .11) and CSS (4 months vs 7 months; HR = 1.193; 95%CI, 0.953-1.494; P = .088) (Figure 5b and b). Based on survival curves of Kaplan-Meier analyses, the 1-year, 2-year OS rates were 19.8%, 8.9% in PSCC patients and 29.9%, 10.1% in PAC patients. CSS rates were 21.5%, 9.7% in patients with PSCC, 32.1%, 11.4% in patients with PAC, respectively.

Kaplan-Meier plot and log-rank test of (a) CSS and (b) OS after PSM.
Stratified Analysis
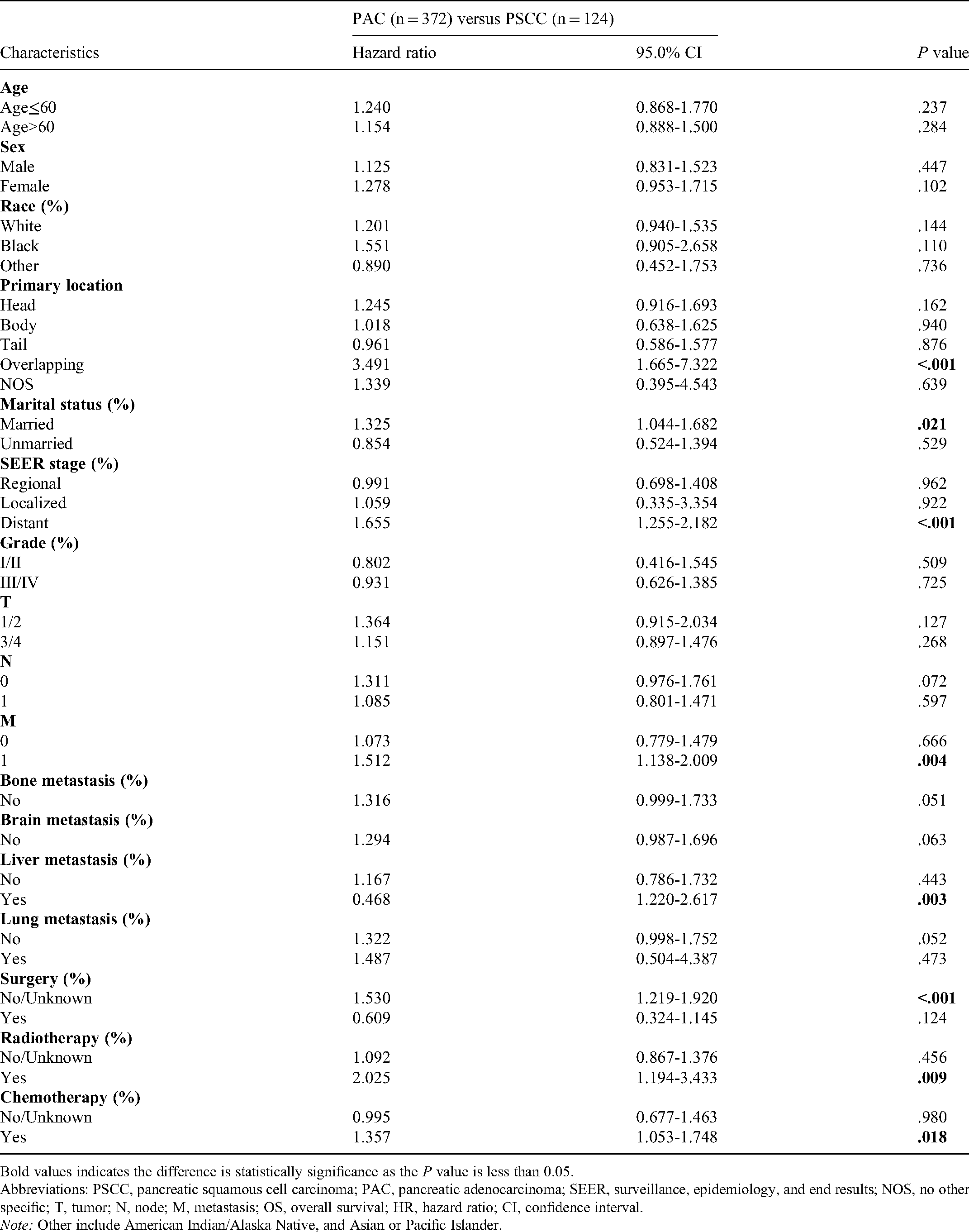
After the stratification of each variable, the prognosis of patients with PSCC was significantly more dismal than patients with PAC in married patients. Prognosis of PSCC patients at distant SEER stage, M1 with primarily invaded pancreatic overlapping region, with liver metastasis was also significantly worse than PAC patients (Table 4). In patients treated with chemotherapy (HR = 1.357; 95%CI, 1.053-1.748; P < .001), radiotherapy (HR = 2.025; 95%CI, 1.194-3.433; P = .009), prognosis of PSCC group was worse than PAC group. Patients without surgery in PSCC group had an unfavorable prognosis compared with PAC (HR = 1.530; 95%CI, 1.219-1.920; P < .001). Comparable prognosis was observed in PAC and PSCC patients treated with surgery.
Stratified Analyses of the 1:3 Matched Cohort (OS).
Bold values indicates the difference is statistically significance as the P value is less than 0.05.
Abbreviations: PSCC, pancreatic squamous cell carcinoma; PAC, pancreatic adenocarcinoma; SEER, surveillance, epidemiology, and end results; NOS, no other specific; T, tumor; N, node; M, metastasis; OS, overall survival; HR, hazard ratio; CI, confidence interval.
Note: Other include American Indian/Alaska Native, and Asian or Pacific Islander.
Discussion
Current studies focusing on the survival and prognostic factors of PSCC are limited. There is also no comprehensive understanding in PSCC due to lack of comparisons between the most common PAC and extremely rare PSCC. Therefore, our study concentrated on the characteristics of PSCC and discrepancies between PSCC and PAC. We discovered that the majority of PSCC patients were elders, white and female. In addition, PSCC presented to be poorly differentiated and metastatic when diagnosed, with a more dismal prognosis than PAC. T stage could not be regarded as a predictive factor as there was only 1 PSCC patient at T1 stage. Liver and lymph nodes were the most common metastatic sites. As for treatment, PSCC patients received more favorable prognosis from surgery and chemotherapy. The therapeutic effects of radiotherapy to PSCC patients is worth discussing and it indicated better efficacy in PAC than PSCC. Conduction of surgery led to comparable prognosis in PAC and PSCC patients.
Another SEER-based study and a retrospective analysis using National Cancer Database (NCDB) of PSCC reached analogous conclusions with our study. Common conclusions showed the vulnerable population were elders and the most predilection site of pancreatic was head. PSCC patients had a higher proportion of poor differentiation and inferior survival. On the contrary, NCDB-based study indicated a higher frequency of PSCC occurred in male, which was in accordance with PAC. While the proportional differences in sex distribution between PSCC and PAC were not statistically significant in NCDB-based study and our study. Corresponding to previous retrospective studies and case reports,15,17,18 surgery was identified as an independent positive prognostic factor both in univariate and multivariate analysis.
In our study, 1-year OS rate in PSCC patients was 19.8%, which was close to another SEER-based analysis with 1-year OS rate of 14.0%. 15 Statistically significant worse mOS in PSCC group compared with PAC group (4 months vs 8 months) was detected in our analysis before PSM. After PSM, there was no significant difference between PSCC and PAC in mOS in our study (4 months vs 7 months), similar trend was observed in NCDB-based study (4 months vs 4.8 months). In NCDB-based analysis, matched variables contained age, sex, race, insurance, Charlson-Deyo score, year of diagnosis, facility type, tumor grade, stage, surgery, radiation, and chemotherapy. In our study, in addition to variables related to demographics, variables closely connected to prognosis, including primary location, SEER stage, grade, TNM stage, and 3 sites of metastasis (bone, brain, liver) were matched. Meanwhile, metastatic tumor and tumor without positive cytological, microscopic, or histological confirmation were excluded, together with patients with unknown information in race, SEER stage, TNM stage. Although the sample size of the retrospective analysis extracted from NCDB was larger, inclusion of metastatic tumor and tumor without diagnostic confirmation with golden standard increased the influence of confounding factors. Therefore, discrepancies between PAC and PSCC could not be accurately obtained. Variables covered in multivariate analysis were limited in NCDB-based study, containing age, sex, race, Charlson-Deyo score, insurance status, grade, and therapy received. In another SEER-based study, there were no disparities in primary tumor location, extent of disease between PAC and PSCC, which were not corresponding to our results. Distinctions in results are possibly derived from the different inclusive year and the historically diagnostic standard. In addition, propensity score matching was not conducted to balance the confounders. 15 Information of 4-organ metastasis were analyzed in our study which was not mentioned in that previously published SEER-based study. Liver metastasis was identified as a predictive factor with worse prognosis in PSCC. Therefore, conclusions reached in our study give a more comprehensive and precise description to PSCC, as well as a clear understanding on differences between PAC and PSCC.
Previous study has proved that the primary location of pancreatic cancer is a prognostic factor for survival, reflected in decreased lifetime in patients with body and tail lesions than head lesions. Pancreatic cancer with primary location on body and tail lesions seems to late manifestations in those patients.19,20 In our study, worse prognosis of PSCC patients may be associated with higher proportion of tail and body lesions discovered in PSCC (42.8%) than PAC (25.9%). Interestingly, overlapping lesions indicated strongest correlation with worse prognosis in PSCC cohorts rather than PAC cohorts, which may be a noteworthy character related to histology type. We also identified that PSCC was always prone to be poorly differentiated and the lower differentiation may be related to worse prognosis in univariate analysis, although the difference was not statistically significant. Significant better relapse-free survival in low/moderate grade PSCC tumors than high grade tumors (3 months vs 16.2 months) was identified in another study. 18 Distant metastasis was regarded as a risk factor in our analysis, with a lower possibility of surgery and short survival time observed in case reports.5,21 Based on the analytical results and case reports, nearly 70% of PSCC patients are diagnosed at advanced stage, indicating a possibility of curative resection less than 30%. 18 But for patients who present with operable PSCC, a pooled survival analysis indicated a significantly 6-month longer OS. 18 Similarly, a prominent better OS of 21 months in PSCC patients with resection at stage I/II was observed in a population-based study. 17 In agreement with our study, surgery was regarded as an independent prognostic factor with remarkably improved OS. For patients with palliative treatment, combined chemotherapy has been proved effective while the prolongation to OS is not notable in every patient. 13
In addition to pancreas, AC and SCC have been compared in lung, esophagus, cervix, rectum, and anus. According to population-based analysis of AC and SCC in different anatomical regions, better OS in SCC was observed in rectum, 22 anus, 23 and cervix.24,25 Patients with AC obtain better clinical outcomes in esophagus. 26 In lung cancer, studies reach different conclusions in survival advantages between AC and SCC, and it is difficult to tell whether prognosis is related to pathologic patterns. 27 Regardless of pathologic patterns, the root cause of different prognosis in tumor is the influence of prognostic factors. It has been demonstrated that epidemiology (age, sex, race), clinicopathologic characteristics (tumor location, histologic grade, tumor stage, TNM stage), and treatment modalities (surgery, chemotherapy, radiotherapy) have synergistic effects on tumors prognosis. However, due to the heterogenicity of tumors, prognostic factors should be analyzed in each pathological type of tumor to establish a comprehensive understanding for it.
There are several limitations in our study. Firstly, data we extracted was completely based on the SEER database and it is a retrospective, nonrandomized study. Significant information including the biology of tumor, type of surgical procedure, therapeutic regimen of chemotherapy, dose of radiotherapy, information of neoplasm recurrence, environmental risk factors were not taken into consideration due to their absence in SEER database. Some specific information correlated with the therapeutic decisions like ECOG score standard were not included as variables in SEER database which could be confounding factors to survival. There was no information on stage when patients underwent operations, and it was difficult to tell whether better prognosis was derived from the conduction of surgery or an early stage of tumor. Secondly, the sample size of PSCC in SEER database without missing information was relatively small. Thirdly, the individual difference in gene expression was not analyzed with relevance to prognosis and response to treatment as this information was not applicable in SEER database. In this condition, prospective studies need to be conducted to verify the results we obtained.
Conclusion
Our results indicate that the prognosis of PSCC patients was worse than PAC patients in survival analyses. PSCC occurs mainly in elders, white and female. It is mostly located on pancreatic head, followed by body, then tail. PSCC invading overlapping regions are associated with worse prognosis. Compared with PAC, PSCC could have a higher proportion to be poorly differentiated and distantly metastatic when diagnosed. Liver and lymph nodes are most common metastatic sites in PSCC. We identify that surgery and chemotherapy are independent prognostic factors which improve the OS in PSCC patients. These findings help to establish a comprehensive understanding on PSCC and give a comparison between PAC and PSCC, which may provide basic information for prospective study and clinical instructions.
Supplemental Material
sj-docx-1-tct-10.1177_15330338221106533 - Supplemental material for Epidemiology, Treatment, and Outcome of Pancreatic Squamous Cell Carcinoma and Pancreatic Adenocarcinoma: A Propensity Score-Matching Analysis Based on SEER-Database
Supplemental material, sj-docx-1-tct-10.1177_15330338221106533 for Epidemiology, Treatment, and Outcome of Pancreatic Squamous Cell Carcinoma and Pancreatic Adenocarcinoma: A Propensity Score-Matching Analysis Based on SEER-Database by Yuqing Wang, Yuwen Zhou, Yueyun Chen, Ruolan Xia and Jiyan Liu in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Author Contributions
YWang and YZhou collected data, reviewed the literature, analyzed all data, and wrote the manuscript. YChen collected data, wrote, and revised the manuscript. RXia collected data and rechecked the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Sichuan Science and Technology Department Key Research and Development Project (2019YFS0539), 1.3.5 Project for Disciplines of Excellence, West China Hospital, Sichuan University (ZYJC18022).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.