
Abstract
Keywords
Introduction
Primary retroperitoneal liposarcoma (PRLS) are rare and biologically heterogeneous tumors whose management may be extremely challenging due to their size and location.1,2 Large PRLS may simultaneously involve several organs potentially increasing the risk of post-operative complications, including urinary tract injuries. 3 In particular, ureter could be displaced, compressed, or encased by these tumors in most cases. Generally, extended multivisceral resection with ipsilateral nephrectomy is advocated for the treatment of PRLS. However, the kidney may be preserved to balance between surgical margins adequacy and expected morbidity in specific situations.4–6 In particular, our surgical policy is achieving extended resection with ipsilateral lipectomy whereas kidney maybe spared in specific circumstances such as well-differentiated sarcomas, young patients, easy freeing from the tumor during operation, solitary kidney and presence of multiple comorbidities. Thus, renal preservation is required sometimes, and the surgeon has to identify and preserve the ipsilateral ureter, detaching it from the tumor. In these cases, the ureter can be accidentally transected, de-vascularized, kinked or ligated. Thermal injuries related to the use of energy devices have been also identified as possible causes of ureteral injuries (UIs). 7 UIs may significantly affect the post-operative course, increasing morbidity and lowering the quality of life of the patients.8–10
Several authors have proposed prophylactic ureteral catheter placement (PUCP) as possible strategy to facilitate the identification of the ureter and to prevent UI, in particular in colorectal surgery.11,12 A retrospective study including 51 125 patients undergoing colectomies showed that PUCP applied in 4.9% of colectomies was associated with a lower rate of UIs, although this reduction failed to reach a statistically significant level. 13 Other studies demonstrated that PUCP could help to identify ureter without reducing the actual incidence of UIs.14–16 Nevertheless, urinary tract infection, urinary obstruction, and longer hospital stay were often observed in patients undergoing PUCP.17,18 In the last decades, cost-efficacy issues have been also raised when evaluating the use of PUCP in colorectal, urology, and gynecology surgery.19,20 Up to now, no data on the role of PUCP in retroperitoneal sarcoma (RPS) surgery have been reported in literature. The aim of this study is to evaluate the efficacy of PUCP in reducing the incidence of UI in PRLS surgery.
Methods
Study Design and Patients
This study was a retrospective study, conducted in accordance with the Declaration of Helsinki (as revised in 2013), following STROBE retrospective cohort guideline. 21 It was approved by institutional review board of Peking University International Hospital (PKUIH-NO.2019-032(BMR)) and individual consent for this retrospective analysis was waived. Medical records of consecutive patients operated for PRLS at PKUIH from January 2015 through December 2018 were retrieved from our database.
All records were de-identified and stored in encrypted computer once data were collected. Patients who underwent surgeries for the first time with pathological findings of retroperitoneal liposarcoma were included in this study. Exclusion criteria were patients younger than 18 years, tumors located above the kidney at the preoperative CT scan, other histological subtypes of sarcoma, recurrent sarcoma, and tumors requiring nephrectomies. Demographics, surgical and pathologic variables were analyzed. PUCP was determined by sarcoma surgeons and catheters were placed by staff urologists via a rigid cystoscope at lithotomy position under general anesthesia prior to surgery. Intra-operative catheterizations were not considered as prophylactic catheter placement. All sarcoma operations were performed by same surgical team. As above mentioned, our surgical policy is achieving extended resection with ipsilateral lipectomy whereas kidney maybe spared under the following circumstances: well-differentiated sarcomas, younger age, lysised from tumor easier during operation, solitary kidney and multiple comorbidities.
UI comprised UI secondary to any damages during the surgical procedures or with any evidences of hydronephrosis, ureteral leakage postoperatively. As to relationships between tumor and ureter, tumor involvement of ureter larger than 180° was defined as encasement, while smaller than 180° was adjacent. Complications were evaluated through Clavien-Dindo Classification system in present study. 22
Primary endpoint was the rate of UIs during and after retroperitoneal liposarcoma resection procedures.
Statistics
Categorical variables were reported as frequency (%) and continuous variables were reported as mean with standard deviation (SD) or median with interquartile range (IQR). UIs were compared between groups PUCP and No PUCP through Fisher exact test. Risk factors of postoperative UIs were tested using univariate and multivariate analysis. A P value of less than .05 was considered statistically significant. Software of STATA Version 14.0 was used for statistics.
Results
Patient Characteristics
Fifty-five patients with PRLS were finally included in our study as reported in Figure 1. Main clinical and pathological characteristics of the analyzed patients are shown in Table 1. Fourteen out of fifty-five (25.5%) patients underwent PUCP. Patients’ characteristics were compared between groups of PUCP and No PUCP. There was no statistically significant difference between the 2 groups, except slightly higher level of hemoglobin in the No PUCP group.

Flow chart of patients.
Clinical and Pathologic Characteristics of the Patients and Comparisons Between PUCP Group With No PUCP Group.

Abbreviations: PUCP, prophylactic ureteral catheter placement; WBC, white blood cell.
Operative Outcomes
Surgical and short-term outcomes are shown in Table 2. A total number of 25 organs were concomitantly resected in 19 patients. Median blood loss was 600 mL (range 100-5000 mL) and operative time was 222 min (range 100-490 min). Median hospital stay was 29 days (IQR 22, 35). Fifteen out of 55 patients (27.3%) developed various post-operative complications, of which gastroplegia was the most common one (7.3%). Five (9.1%) had major morbidities (Clavien-Dindo complication grade ≥3), including 3 admitted in ICU for cardiac arrest, 1 intestinal fistula, and 1 urinary leak. There was no operative mortality. There were no significant differences in terms of morbidities, type of resection, and length of hospital stay (LOH) between the 2 groups (PUCP and No PUCP; Table 2).
Comparisons of Operative Outcomes Between Groups PUCP and No PUCP.
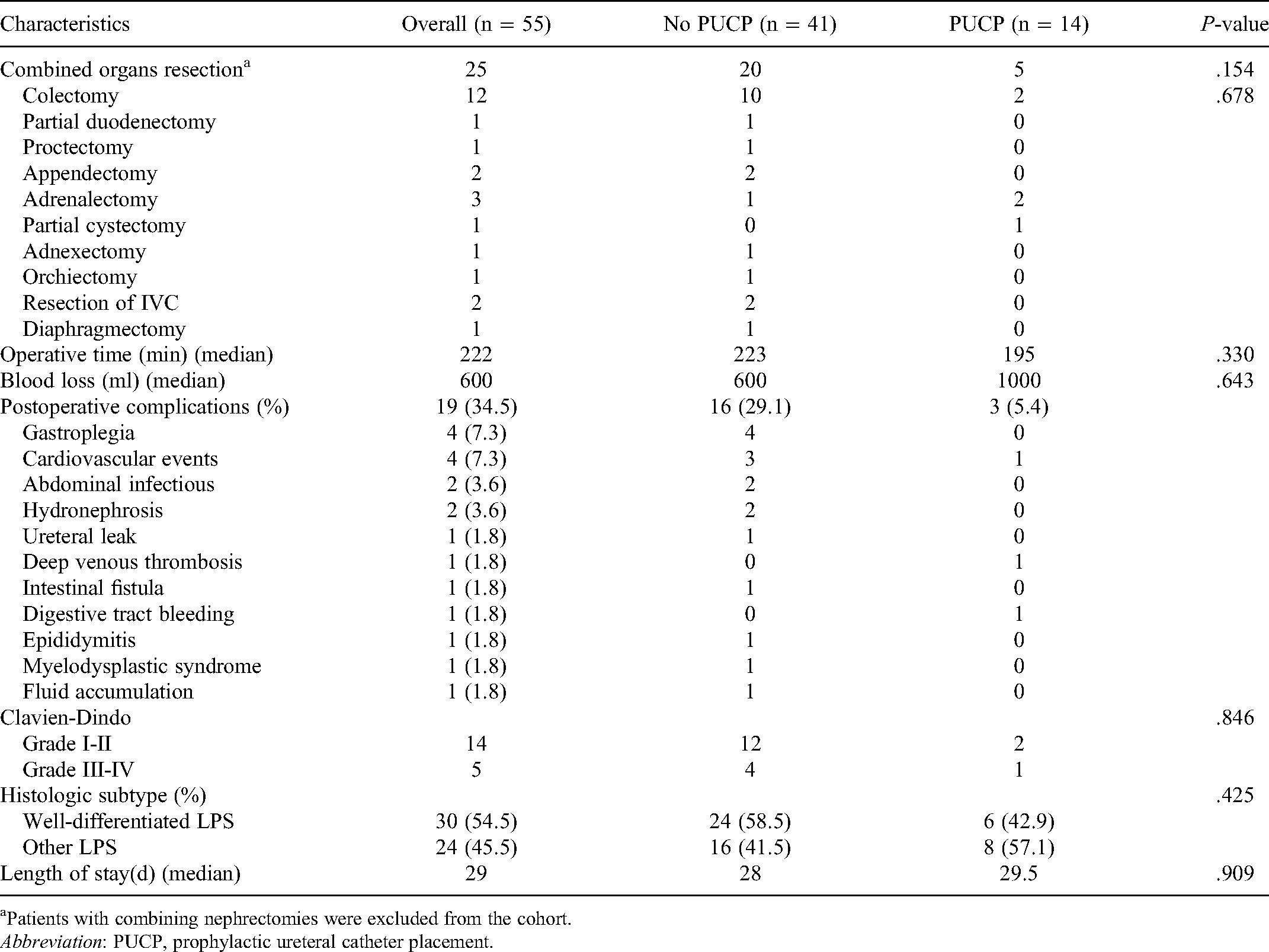
Patients with combining nephrectomies were excluded from the cohort.
Abbreviation: PUCP, prophylactic ureteral catheter placement.
Ureteral Injuries
A total of 16 patients (29%) developed UIs intraoperatively with 2 confirmed post-operatively through urography phase imaging. Causes or presentations of UIs were listed in detail (Table 3). Fifteen out of 16 patients did not undergo PUCP, while only 1 patient received prophylactic PUCP. There were significant differences of UIs between PUCP group and No PUCP group (P < .05) (Table 4). In univariate analysis, significant differences of BMI, tumor–ureter relationship, co-colectomy were shown between Groups UIs positive and negative, while in multivariable analysis, co-colectomy and tumor-ureter relationship were the 2 risk factors associated to UIs (P = .045, 95%CI [1.05-62.36] and P = .010, 95%CI [1.66-41.43]) (Table 5).
Detailed Causes and Presentation of UIs in the Patients.

Abbreviation: PUCP, prophylactic ureteral catheter placement.
Comparison of UIs Between PUCP and No PUCP Groups.

Abbreviation: PUCP: prophylactic ureteral catheter placement.
Univariate and Multivariate Analyses of Ureteral Injury in all Patients Undergoing Primary Retroperitoneal Liposarcoma Resection.

Discussion
Prophylactic urinal stenting was discussed and advocated as a potential strategy to prevent UIs by colorectal surgeons, urologists, and gynecologists. However, debates over this topic never stopped and there were no evidence-based guidelines existing regarding indications for PUCP during pelvic surgery. 23 Ureteral catheterization did not lead to a decrease of iatrogenic UI as expected according to some studies.16,24 Nevertheless, the procedure of catheterization itself could also cause ureteric perforation, urinal bleeding, etc.17,25 Besides, postoperative hematuria, urinary tract infection, prolonged operative time, and hospital stay were commonly reported associating with catheterization. Hematuria occurs in nearly a hundred percent of patients after ureteral catheterization. 14 Thus, whether we should place ureteral catheter prior to pelvic surgeries remains confliction.
In terms of RPS surgeries, unlike pure colorectal or gynecological surgeries, ureters were often compressed, displaced, and encased by bulky and invasive tumor. 26 PUCP is more likely to be recommended in surgeries involving retroperitoneal and pelvic area preoperatively due to its aids on identification and guidance of ureter.27,28 Unfortunately, there is no study found specifically focused on the utilization of catheter and intraoperative UIs in RPS surgeries before. The largest RPS series reported from TARPSWG only disclosed a 0.4% (4/1007) percentage of urinal leak after RPS surgeries. 29 No data about PUCP or other urinal morbidities were collected in that work. In this study, all 16 patients who had UIs received prophylactic, intermittent, or postoperative stent placements. Three of sixteen (18.8%) postoperative urinal events comprising of 1 ureteric leak and 2 hydronephrosis were documented. And the patient who had ureteric leak underwent a reconstruction surgery for rescuing the leakage followed with stenosis.
Regarding PUCP, patients presented with solitary kidney, tumor infiltrated to/encased with kidney, ureter or bladder, too big size, pelvic tumor, preoperative hydronephrosis were considered at high risk of intraoperative UIs and were suggested undergoing PUCP. Encouragingly, only 1 case out of 14 patients who underwent PUCP developed with UI postoperatively. Patients without PUCP had much higher probability of UIs, comparing with PUCP group. Experiences from our surgical practice showed that, skilled surgeons would proactively find the ureteral catheter in patients with PUCP during surgeries which was very helpful for preventing from UIs. On the opposite, surgeons sometimes were even unaware of the UI during surgeries in patients without PUCP, because of their overconfidence of surgical technique or misidentification of ureter. A total of 86.7% (13/15) patients without PUCP developed with UI in this study due to these causes (Table 3). Ureter transected intendedly during surgeries in order to achieve en-bloc resection was not considered of iatrogenic UI and calculated in this study. Those with ureter encased by tumor had significant risks of UI compared with patients with ureter adjacent to tumor.
Nevertheless, if the colon was involved or infiltrated by the sarcoma, hemicolectomy was often combined in order to achieve a better surgical vision and exposure of retroperitoneal space as well as a better oncological outcome. And the ureter locating between the sarcoma and colon in the retroperitoneal space would be inevitable injured during this procedure. In our study, resection surgeries combining colectomies were calculated as an independent risk factor associated to UI through uni- and multivariate analysis regardless PUCP or not (Table 4).
This study has its intrinsic limitations. It was conducted as a retrospective review with small samples. And the decision to place ureteral catheters was at the surgeon's discretion though all patients were operated by the same team. Patients with recurrent RPS were not enrolled in this study for avoiding potential selection bias of patients. Besides, our institution is the first and largest RPS center all over China. Therefore, most of our patients were transferred from other 3-tier institutions because of extreme complexities of tumors. More than half (27/55) of these patients received combined organ resections and 60.7% (34/55) patients received ipsilateral or total lipectomy. That could be an explanation of relatively higher urinal morbidities, compared to previous reported data. Well-designed prospective study is needed to better understand the impact of PUCP as a risk stratification model in avoidance of UI in PRLS patients.
Conclusion
In conclusion, PUCP might be an effective option of decreasing intraoperative UIs in PRLS patients, when kidney preservation is required, especially in patients with ureter encased by tumor or anticipated colectomy during surgical process.
Footnotes
Abbreviations
PUCP, prophylactic ureteral catheters placement; PRLS, primary retroperitoneal liposarcoma; RPS, retroperitoneal sarcoma; LPS, liposarcoma; WBC, white blood cell; ASA, American Society of Anesthesiology; TARPSWG, Transatlantic Australasian Retroperitoneal Sarcoma Working Group
Acknowledgments
Partial results were previously reported in 2019 Connective Tissue Oncology Society (CTOS) Annual Conference.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was kindly supported by a grant from Development Center for Medical Science & Technology, National Health Commission of the People's Republic of China (WA2020RW29).
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by institutional review board of Peking University International Hospital (NO.2019-032(BMR)) and individual consent for this retrospective analysis was waived.