
Abstract
The life expectancy of patients with advanced cancer has been prolonged with the development of systemic treatment technology. Spinal metastasis is one of the common ways of metastasis of advanced tumors, leading to spinal cord compression and compression fractures, which often lead to a significant reduction in patients’ quality of life and physical function. Therefore, surgical treatment is still needed for functional recovery and local control. Separation surgery has been known since 2014 when it was purposed. Combined with radiotherapy, it can achieve an ideal goal of local control. This paper gives a brief introduction to separation surgery, hoping to increase the reader's understanding and consider this method in the course of treatment.
Introduction
The spine is the most common site of bone metastasis in malignant tumors. About 30% to 70% of patients with malignant tumors will have spinal metastases.1,2 Spinal metastases can lead to local pain, spinal instability, vertebral pathological fractures, spinal cord compression, and then cause neurological function damage and even paralysis, seriously affecting patients’ quality of life and shortening the survival time of patients. 5% to 10% of the patients of cancers will have spinal cord compression.3,4 Even 20% of patients presented with malignant spinal cord compression (MSCC) as the first presentation of malignancy. 5 Lung, breast, and prostate cancers account for over 60% of MSCC cases. Lumbar spine seems most frequently involved, followed by the thoracic and cervical segments, but thoracic spine occupies the highest proportion of clinically symptomatic spinal metastases. 5 The treatment of spinal metastases advocates the combination of multiple disciplines, and the treatment can be roughly divided into 2 categories: systemic treatment and local treatment. Systemic therapy includes analgesic drug therapy, endocrine therapy, corticosteroid therapy, chemotherapy, bisphosphonate, immune and targeted drug therapy, local treatment includes radiotherapy, surgery, and so on.
Treatment should be available in 24 h. High dose of steroids is recommended to use in 12 h after diagnosis, to provide analgesia, decrease spinal cord vasogenic edema, and the secondary complication of reduced arterial flow and therefore, prevent further neurological deterioration, 6 even directly decrease tumor size in certain situations steroids. 5 And should be weaned after RT or surgery over 5 to 7 days to avoid side-effects.
Before radiotherapy was popularized in clinic, posterior laminectomy was the only option for patients with spinal cord compression of metastatic tumors. With the introduction of spinal radiotherapy in the 1950s, several retrospective studies7–10 and a small-scale randomized trial 11 showed that laminectomy combined with radiotherapy had no benefit compared with radiotherapy alone, and surgical treatment was basically abandoned. In the 1980s, direct decompression surgery combined with intraoperative spinal reconstruction changed the status of surgery. Several studies12–14 and meta-analysis 15 showed that direct decompression surgery, with or without postoperative radiotherapy, is superior to radiotherapy alone. Patchell et al 16 compared 50 patients treated with direct decompression surgery combined with radiotherapy and 51 patients undergone radiotherapy alone. They found that neural function (ability of walking) was better reserved or revered in the operation group, and the demand for corticosteroids and opioid analgesics was also significantly reduced. Therefore, surgery became an alternative to radiotherapy.
Back then, before advanced radiotherapy techniques came out, conventional external beam radiation (cEBRT) was mainly used to consolidate the local control caused by surgery, and it is limited by the radio-resistance of the tumor. 17
On the side of operation style, it has also undergone multiple changes in terms of surgical technique with the development of people's cognition. 18 Up to the 1990s, the main surgical approach for the epidural disease was a simple posterior bony decompression with a bilateral laminectomy as a more promising solution than primary external-beam radiation therapy (EBRT). In 2005, a landmark trial of Patchell et al 16 demonstrated that surgical circumferential decompression of the spinal cord combined with postoperative EBRT had significant benefits in terms of functional outcomes.
Then, new radiotherapy techniques were invented: stereotactic radiosurgery (SRS) and stereotactic body radiotherapy (SBRT). These complex techniques allow high doses to be delivered to the target in a highly conformal fashion, with steep dose ‘fall-off’ gradients around the target of approximately 10% per millimeter, thus minimizing dose to surrounding critical structures and normal tissues. 19 It led a better cooperation between surgery and radiotherapy, making separation surgery possible.
The separation surgery was used as a surgical method to separate the anterior sulcus in the spinal canal from the posterior edge of the vertebral body. 20 Not only can the dural compression be relieved, but the cerebrospinal fluid space around the spinal cord can be restored to build the radiotherapy gradient zone, and SBRT can be safely performed for severe ESCC cases caused by radiotherapy-insensitive tumors thanks to the gap. 21 After the safe gap was built, conventional radiotherapy can be performed for radiotherapy-sensitive tumors, and the effect of traditional radiotherapy on spinal cord tissue can be avoided for radiotherapy-insensitive tumors with the existence of the gap. The prototype was first described by Bilsky et al 22 as a single-stage posterolateral transpedicular approach for spondylectomy, epidural decompression, and fusion of spinal metastases. In 2010, Molding et al 23 first applied radiosurgery to 21 patients with spinal metastases after surgical decompression and instrumentation. In 2013, Laufer et al 24 applied circular decompression of epidural tumors plus postoperative radiotherapy to 186 patients with spinal metastases under epidural compression and put forward the concept of “separation operation” for the first time.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were followed for the identification of the studies (Moher et al 25 ). Existing literature focus on allogenic tendon transplantation along with donor and recipient characteristics were identified using MEDLINE via Pubmed, Embase, and Cochrane Library database. The searching process was performed by 2 independent investigators, using search MESH term: “separation surgery.” Reference traction and citation traction (also called “snowballing”) were also performed using the citation information in studies to identify additional data who did not cover in the electronic search.
Indication
The primary indications for surgery are relief of high-grade epidural spinal cord compression (ESCC) caused by tumors radioresistant to cEBRT or gross spinal instability.26,27 Current guidelines based on conventional surgical techniques for ESCC suggest conservative management for patients with life expectancies less than 6 month, whereas patients with life expectancies between 6 month and 1 year are recommended to receive limited palliative surgery. 28
The selection of patients for separation surgery is mainly based on the NOMS (neurologic-oncologic-mechanical-systemic) decision framework, which was originally proposed by the spinal expert group of the Sloan-Kettering Memorial Cancer Center, and later improved by Bilsky. 29 In NOMS, the neurologic consideration is an assessment of the degree of epidural spinal cord myelopathy, compression, and/or functional radiculopathy. The oncologic consideration is predicated on the durability of response to available treatments and expected tumoral response, such as chemotherapy, hormones, immunotherapy, biologics, cEBRT therapy, SRS, or surgery. Mechanical instability caused by pathologic fractures is a separate consideration; the treatment considerations include brace application, percutaneous vertebroplasty and/or pedicle screw augmentation, or open surgery. S, the abbreviation of “system,” is the extent of systemic disease and medical comorbidities to evaluate the ability of the patient to tolerate a proposed treatment and the overall expected patient survival based on tumor histology and extent of disease.
The decision framework recommends that conventional radiotherapy should be used for radiotherapy-sensitive tumor types (any ESCC grade), stereotactic radiotherapy for low-grade ESCC (grade 1) and tumor types insensitive to radiotherapy, separation surgery combined with stereotactic radiotherapy for patients with high-grade ESCC (grades 2 and 3) and tumor types insensitive to radiotherapy, and radiotherapy should be performed for patients whose systemic condition cannot tolerate surgery. For patients with vertebral instability, the vertebral stabilization technique should be combined. 30 However, the treatment of MSCC caused by chemosensitive disease, ewing's sarcoma for example, is still under discussion. Because of the chemosensitivity, potential negative affect after surgery, and the lack of clinical practice caused by the rareness of ewing's sarcoma, surgical decompression is not irreplaceable. Neurological deficit is recovered following treatment with chemotherapy to the same extent. 31
Procedure
The operation was completed in 2 steps:
The patient takes prone position, C-arm positioning, routine disinfection and towel laying, and intubation under general anesthesia. Taking the diseased vertebra as the center, the exposure range includes 2 segments of the diseased vertebra, the pedicle of the upper and lower segments of the diseased vertebra is placed before the operation, the pedicle screw is placed, one side of the connecting rod is installed to maintain the stability of the spine during the operation, the spinous process, lamina and ligamentum flavum are removed, the unilateral and bilateral facet joints are removed, and the tumors around the dura mater and the posterior longitudinal ligament and part of the vertebral body are removed circularly so that a space is formed between the spinal cord and the tumor. It is not necessary to completely remove the tumor and vertebral body around the spinal cord. To avoid the high risk of recurrence and symptomatic cord compression, it is necessary to ensure the circumferential decompression and the reconstitution of the thecal sac are achieved to allow for ideal local control.
32
When the resection of the vertebral body is less than 50%, simple posterior reconstruction is enough. When the vertebral body resection is more than 50%, it could be necessary for massive allogeneic bone, or titanium mesh filled with allogeneic bone, or bone cement are placed through the posterior approach for reconstruction. C-arm fluoroscopy was performed again during the operation. After the position of internal fixation was satisfactory, the operation field was irrigated and the incision was closed. After full decompression of the spinal cord, follow-up stereotactic radiotherapy was performed 2 to 4 weeks after the operation.
Because of the existence of internal fixation, MRI examination could be influenced by artifacts, making it more difficult to determine the location and boundary of the dura mater. Therefore, a CT scanning of the spinal canal becomes a proper replacement to determine the dura mater boundary after separation.
Clinical Outcomes
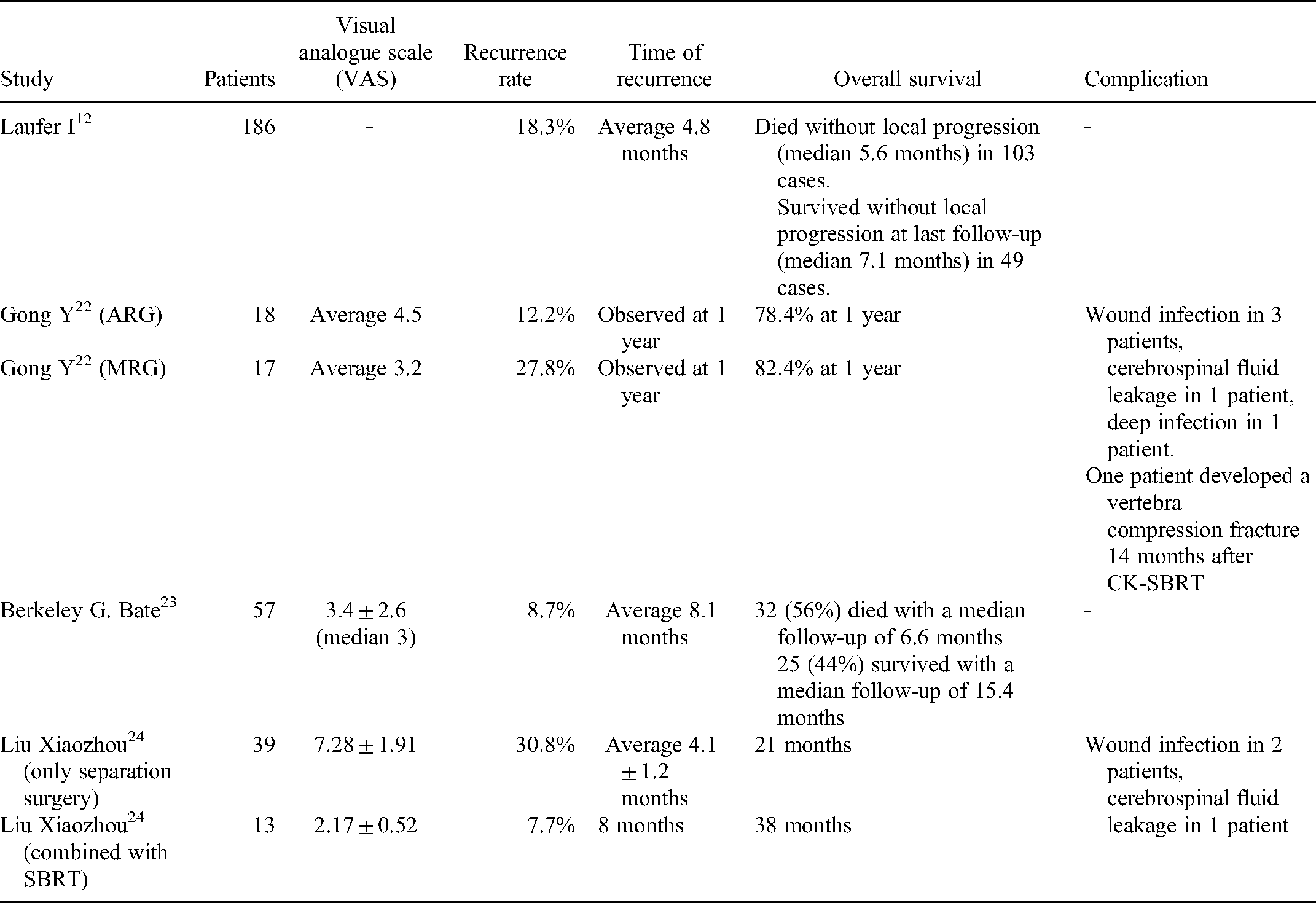
Separation surgery combined with stereotactic radiotherapy can achieve good local control of tumors, improve patients’ neurological function, and relieve patients’ pain (Table 1).
Clinical Outcomes of Separation Surgery Combined With SBRT.
The postoperative effect is affected by the radiation dose and the minimum distance between the residual tumor and the spinal cord. However, because SBRT can maximize the dose of vertebral tumor radiation at a safe dose for the spinal cord, the histology and radiotherapy-insensibility are no longer crucial influence factors that need to be taken into account. 33 Neither does the degree of preoperative epidural compression correlate with outcomes. The overall survival is related to various factors, such as preoperative neurologic deficit, Karnofsky performance scores (KPS), 23 preoperative embolization, postoperative complications, progressive systemic disease, interval time between SBRT courses, 34 metastasis therapy after SBRT, 35 and local progression of the disease after spinal SRS. However, there were no significant correlations with sex, radiation sensitivity of tumor histology, grade of ESCC, or extent of surgical decompression. 30
Gong et al 36 assigned 36 patients cured with hypofractionated SBRT to the aggressive resection group (ARG) or moderate resection group (MRG) whether the ventral dural mass was further resected after a safe gap was reached, and the large cavity in the vertebral body was replaced with polymethylmethacrylate. Local control (LC), overall survival (OS), distance of separation (DS), and quality-of-life parameters were analyzed. There were no significant differences between ARG and MRG in estimated LC or quality-of-life parameters at 1 year. But it is noticed in the MRG that there is a significant difference in “local control” between the patients with a distance of separation <3 mm and the ones with DS ≥3 mm. It is proved that moderate resection of ventral dural mass matters little in reducing patients’ prognosis in separation surgery. However, it is important to keep the minimal distance between the postoperative residual epidural tumor and spinal cord over 3 mm for a reliable disease control effect.
Laufer 24 applied separation surgery combined with stereotactic radiotherapy to 186 patients with spinal metastases under epidural compression. Radiosurgery was performed 2 to 4 weeks after the operation, 40 (22%) patients of the patients received high-dose radiotherapy (24 Gy), 37 patients received low-fractionated high-dose radiotherapy (24-30 Gy/3f), and 109 patients received low-fractionated high-dose radiotherapy (24-30 Gy/3f). The patients received low fractionated low dose radiotherapy (18-36 Gy/5-6f) and were followed up for an average of 4.8 months (0.2-38 months). The local progression rate 1 year after operation was 16.4%, 9.0% in the single radiotherapy group, and 22.6% in the low dose radiotherapy group. While the rate of the high-dose radiotherapy group was 4.1%, which is inspiring and shows us a good path to go through.
Bate et al 37 used stereotactic radiotherapy in 57 patients with spinal metastases (69 lesions, 48 lesions only received stereotactic radiotherapy; 21 lesions received separation surgery combined with stereotactic radiotherapy). The average follow-up was 10 months, 69 lesions were treated, 63 (91.3%) of them achieved the purpose of local tumor control (the tumor size decreased or remained unchanged on enhanced MRI). But local recurrence occurred in 6 tumors (8.7%), including 3 from the stereotactic radiotherapy group and 3 from the combination therapy group. Of the 48 lesions treated in the stereotactic radiotherapy group, 43 (90%) had a remained Frankel grade, but the Frankel grade of 5 lesions (10%) improved. In the combined treatment group which includes 21 lesions, 17(80%) had a stable Frankel grade, and the grade of 3 lesions (14%) had improved. But unluckily, 1 patient developed new cervical radiculopathy that was not caused by tumor compression, which led a decline in Frankel grade. And for 45 patients who were recorded the state of pain, the postoperative visual analog scale score had a decrease of 3.4 ± 2.6 (median 3).
Liu Xiaozhou et al 38 analyzed the clinical data of 52 patients with spinal metastases retrospectively. After separation surgery, 46 patients had pain relief (88.5%). Muscle strength grading decreased in 7 cases, remained unchanged in 2 cases, and recovered in 19 cases. Postoperative Frankel grade and KPS were both significantly improved compared with preoperative scores. The patients who accepted separation surgery were followed up for 9 to 47 months (26.3 ± 18.1 months), and 15 patients died due to the deterioration of the primary tumor. Thirteen patients received SBRT after surgery, 12 cases of them got relief from the pain. The average VAS score of all these 13 patients who received SBRT after surgery decreased to 1.64 ± 0.41 points, which was significantly improved than before, and muscle strength recovered in 8 cases. Frankel grade and KPS of these patients were also significantly improved. Median survival time was up to 38 months for patients treated with separation surgery combined with SBRT, and 21 months for patients without SBRT, and showed a significant difference statistically.
Nduka M. Amankulor et al 39 mentioned the local control rate in the report about hardware failure. The patients who received separation surgery combined with single fraction (24 Gy) or hypofractionated (18-36 Gy/3-6f) radiotherapy showed a local control rate of 84% 1 year after the operation, which is similar to the result of Laufer.
Vega et al 40 published a better outcome of minimally invasive surgical with a lower blood loss (340.1 mL vs 714.3 mL) and a shorter period of bed rest (2.0 days vs 3.6 days). 41 Echt et al 42 also noticed a significant difference of blood loss (430 mL vs 783 mL), with similar rates of local recurrence and hardware failure.
Complications
Due to the limitation of focus debridement, the safety of separation surgery is similar or better than that of other surgical treatments. Xu et al. 43 reported 55 patients treated with piecemeal spondylectomy or separation surgery. Patients underwent separation surgery had less blood loss (1165.52 ± 307.38 mL vs 1784.62 ± 833.64 mL), less complications (15.38% vs 3.45%), and shorter operation time (3.73 ± 1.15 h vs 4.76 ± 0.93 h) than piecemeal spondylectomy.
Bate et al 37 used stereotactic radiotherapy in 57 patients with spinal metastases (69 lesions, 48 lesions only received stereotactic radiotherapy; 21 lesions received separation surgery combined with stereotactic radiotherapy). 5 patients had fractures after the operation, all of them came from the stereotactic radiotherapy group, 4 of them received fractionated radiotherapy and the rest received single radiotherapy; 1 patient developed mild esophagitis after the operation and the symptoms disappeared after 3 months. There were no symptoms of radiation-induced spinal cord injury.
Nduka M. Amankulor et al 39 statistically analyzed 318 patients with spinal metastases who underwent separation surgery, which involves posterolateral decompression and posterior screw-rod fixation without supplemental anterior fixation. After the operation, 9 patients (2.8%) had instrument fixation failure, and all patients needed re-operation. 7 patients failed for more than 3 months after operation (screw loosening or screw prolapse or rod fracture or screw fracture). The failure time of instrument fixation in 2 patients was 14 days after the operation and 22 days after the operation (accompanied by acute compression fracture or pain). In 1 patient, the wound was ruptured due to the protruding of the instrument caused by the deformity. And they found that patients who underwent chest wall resection and those with initial construct length greater than 6 contiguous spinal levels had a statistically significantly higher risk of symptomatic hardware failure than others. They also observed an increased risk of failure in women compared with men.
According to the report of Gong et al, 36 about 36 patients and their complications, there were 3 cases of wound infection, 1 case of cerebrospinal fluid leakage, and 1 case of deep infection. One patient developed a vertebra compression fracture 14 months after SBRT operated with the technology of the CK robot equipment. No radiation myelopathy was found.
Research Progress
Fabio et al 44 performed 3D endoscope-assisted transpedicular thoracic corpectomies on 9 patients and confirmed the safety and feasibility of the procedure. All cases were confirmed by imaging that the tumors were well separated from the spinal cord, axial pain and neurological function were always improved after operation, and no complications occurred during and after the operation. The average postoperative hospital stay was 4 days. No local recurrence was found in the last follow-up. However, follow-up (4-8 months) is still too short to draw any definitive conclusions on the ability of the technology about local control or specific oncology advantages, or to notice potential long-term complications such as hardware failure.
Summary
Separation surgery is a safe and effective method for the palliative treatment of patients with spinal metastases. But as Nduka M. Amankulor et al 39 pointed out, the risk of death still outweighed the risk of hardware failure in this cohort of patients. This reminds us that while we attach importance to relieving patients’ symptoms and improving their quality of life, efforts still need to be made to prolong the lives of patients.
Footnotes
Acknowledgments
We thank Xiong-gang Yang, MD and Hao-ran Zhang, MD, for their encouragement and support during our study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.