
Abstract
Objective:
This study analyzed the correlation between the average segment width (ASW) and gamma passing rate according to the multi-leaf collimator (MLC) position error.
Method:
To evaluate the changes in the gamma passing rate according to the MLC position error, 21 volumetric modulated arc therapy (VMAT) plans were generated using pelvic lymph node metastatic prostate cancer patient's data which is sensitive to MLC position errors as they involve several long, narrow, irregular fields. The ASW for each VMAT plan was calculated using our own code developed using Visual Basic for Applications (VBA). The gamma passing rate of the VMAT plan according to the MLC position error was evaluated using ArcCHECK (Sun Nuclear, Melbourne, FL, USA) while inducing symmetric MLC position errors in 0.25 mm intervals from −1 mm to +1 mm in the infinity medical linear accelerator (Elekta AB, Stockholm, Sweden). Finally, we examined the correlation between the change in the passing rate (
Results:
The ASW and
Conclusion:
These results are expected to be employed as guidelines to minimize the dose uncertainty due to MLC position error in VMAT.
Introduction
Intensity modulated radiation therapy (IMRT) and volumetric modulated arc therapy (VMAT) are the most common radiation therapy technologies. 1 IMRT and VMAT use a small and complex field created by a multi-leaf collimator (MLC) to generate a dose distribution optimized as per the size and shape of the tumor. Therefore, the role of MLC in IMRT and VMAT is considerably more important than that in conventional radiotherapy. Thus, patient-specific delivery quality assurance (DQA) is performed as one of the ways to find mechanical and dosimetric errors in a treatment machine, such as MLC position error, data transmission error, and treatment planning errors.
The effects of position error of MLC on the dose delivery accuracy of VMAT have been researched extensively.2–7 According to previous studies, some types of mechanical errors, such as incorrect gantry and collimator angles, did not have a significant impact on the DQA results and could be easily checked by an indicator during DQA process.2,3 On the other hand, MLC is a key mechanical component that produces a variety of dose distributions used in IMRT or VMAT, hence, even a small MLC position error has a significant impact on the DQA results. The DQA renders different results depending on the type of MLC position error. Random errors caused by the position errors of individual leaves have negligible effect on the DQA results, whereas systematic errors caused by incorrect calibration of the MLC position or error in the leaf guide position have a significant impact on the DQA results.4,5
Heilemann G et al. evaluated DQA results for VMAT plans for the prostate and head and neck for the systematic error in the MLC position. 6 The results of gamma analysis showed that the gamma passing rate sharply decreased to less than 90% even with a system position error of only 0.5 mm. Thus, a systematic error in the MLC position can cause a serious error in the dose delivery accuracy in VMAT.
Previous studies have shown that systematic MLC positioning errors have a direct effect on dose delivery error. However even for the identical shape and size of the treatment site and the treatment technique, the degree of change in the DQA results by systematic MLC positioning error varies.4–7 This implies that the effect of MLC positional errors on DQA results varies depending on each segment fields used in the treatment plan, even with the same treatment site and technique. To determine the effect of the minimum width of the segment field on the VMAT plan, Wang et al. 8 evaluated the gamma passing rate and plan quality changes such as coverage(D95%), conformity index (CI) and gradient index (R50) in the treatment plan by limiting the minimum segment width of the VMAT. The minimum segment width parameter determines the minimum leaf separation between two opposing leaves within the segment field of a given segment in the sequencing algorithm of the Monaco Treatment Planning System. The results confirmed that the increase in minimum segment width can improve the gamma passing rate without changing the plan quality. Nevertheless, the direct correlation between the segment width and the gamma passing rate is yet to be identified in the VMAT plan.
In this study, we investigated the effect of systematic error in the MLC position on the DQA of the VMAT plan as a function of the average segment width (ASW) as one of the indicators representing the segment field shape. Moreover, we examined the correlation between the gamma passing rate and the ASW for a given MLC position error in VMAT. We also proposed a method of reducing dose uncertainty due to MLC position error in the treatment planning stage.
Method
Figure 1 shows the logical flowchart of our investigation. This study was conducted as follows. First, to evaluate the dose accuracy of the VMAT plan according to the MLC position error, we induced systematic errors in the MLC position by moving the MLC leaf guide of the linear accelerator from −1 mm to +1 mm in the interval of 0.25 mm. Subsequently, we measured the dose distribution for the VMAT plan using ArcCHECK (Sun Nuclear, Melbourne, FL, USA) and evaluated the gamma passing rate using the SNC patient program (version 6.4.0). Finally, we calculated the ASW from the MLC position information of the VMAT plan using our own Visual Basic for Applications (VBA) code and then examined the correlation between the gamma passing rate and ASW according to the MLC position error.

Schematic of the experiment for evaluating the correlation between ASW and gamma passing rate according to MLC position error.
Patient Selection and Treatment Plan
This study was conducted after receiving approval from a certified institutional review board. The data used in this study consisted of data of patients who received radiotherapy for prostate and pelvic lymph nodes. Using this data, we generated 21 VMAT plans to evaluate the changes in the gamma passing rate according to the MLC position error. VMAT plans for prostate including pelvic lymph nodes are sensitive to MLC position errors as they involve several long, narrow, irregular fields. 9
The VMAT plans for all the patients were designed using the Monte Carlo algorithm of Monaco 5.11 (IMPAC Medical Systems Inc., Maryland Heights, MO [a subsidiary of Elekta AB, Stockholm, Sweden]). The dose delivery was investigated through the infinity linear accelerator with the AgilityTM multileaf collimator (Elekta AB, Stockholm, Sweden), which has 160 leaves of 5 mm width. The prescribed dose for 95% of the planning target volume (PTV) was normalized to 45 Gy in 25 fractions. The cost function of the VMAT plan was set slightly differently depending on the tumor size and organ position.
Every plan case had a dual arc with a collimator angle of 30° including clockwise and anticlockwise 360° reciprocal rotations with an increment of 20° from the gantry angle of 180°. The fluence-smoothing parameter was set to medium mode and the control points per arc were limited to 150. For the calculation of the final dose, we used 2.5 mm grid spacing and 3% statistical uncertainty per control point.
ASW Calculation Using the VBA Code
VMAT plans generate segment fields of various sizes to satisfy the dose distribution desired by the user. The segment field shape is determined by 150∼200 control points in general. One segment field has position data for 160 leaves. Therefore, calculating the ASW using the position data of leaves not only takes considerable time but also makes it difficult to guarantee the accuracy of the calculations. Therefore, in this study, we calculated the ASW using our own VBA code.
Figure 2 shows the logical flowchart of the VBA code used in this study. The segment field information about each treatment plan is obtained from the segment field report of Monaco RTP. The segment field report provides the position data of all the 160 leaves included in the segment field. To calculate the leaf pair gap used to form the segment field shape, it was determined under the following conditions:



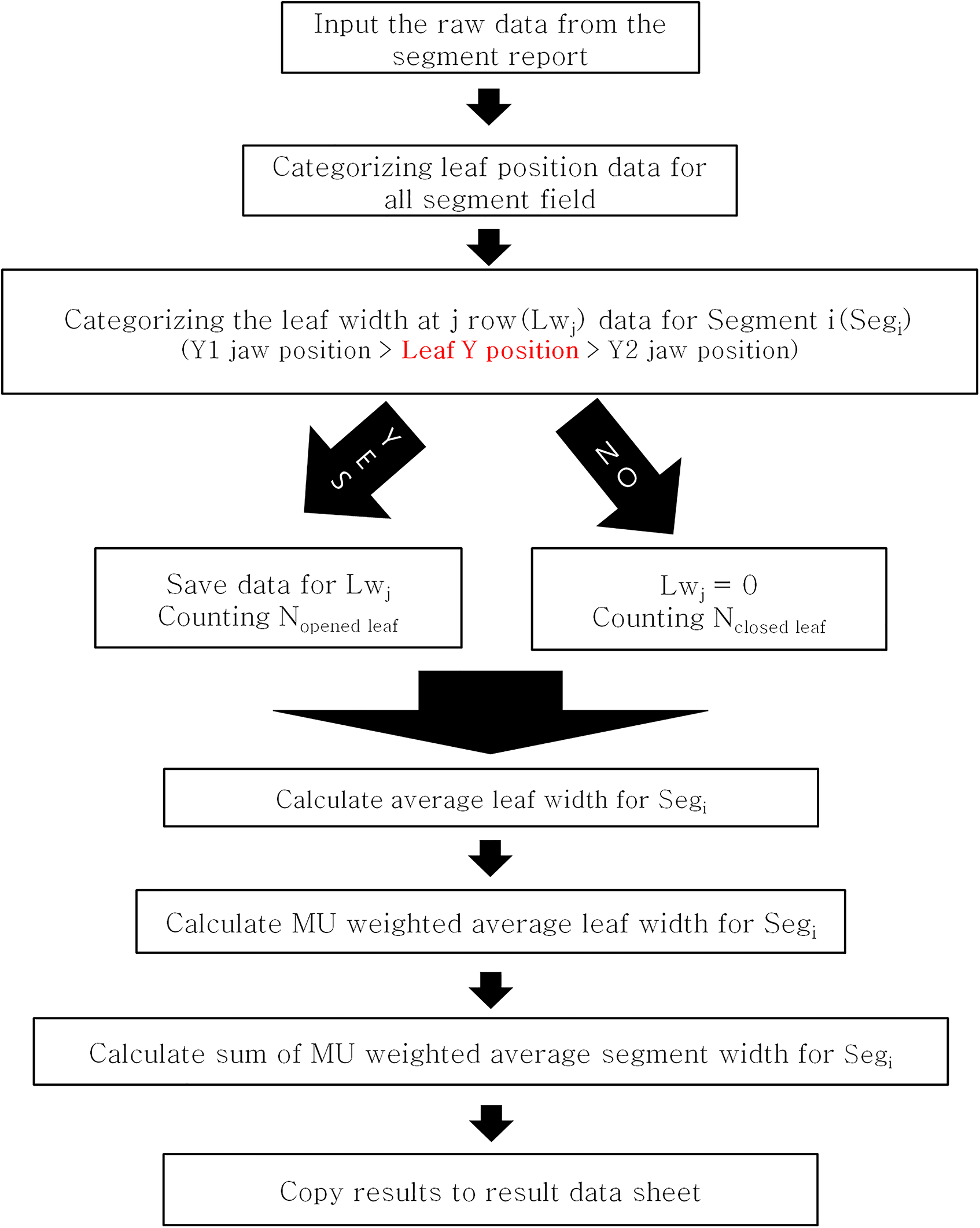
Logical flowchart of the VBA code for evaluating the correlation between ASW and gamma passing rate according to MLC position error.
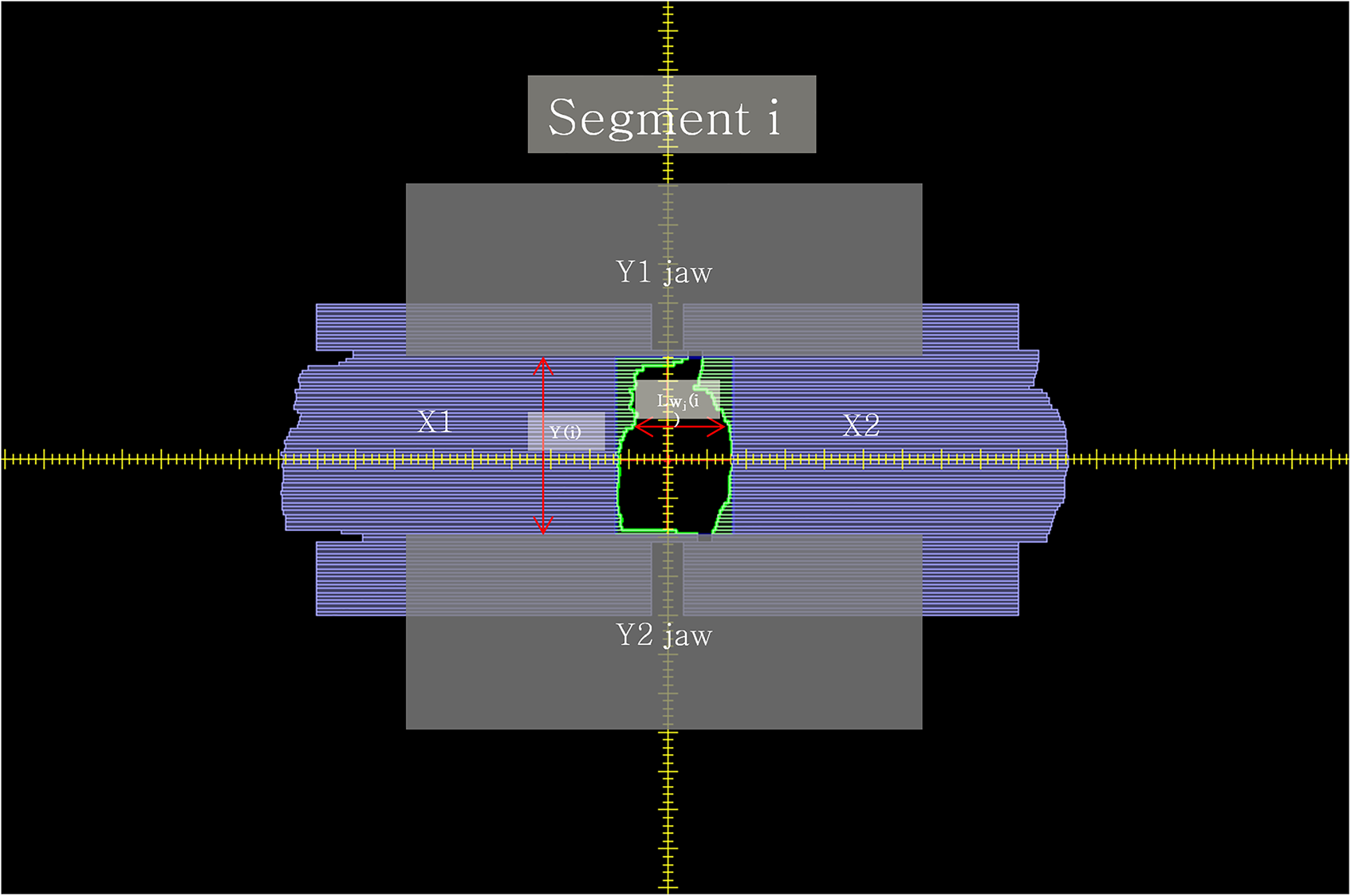
Depiction of leaf pair width and Y jaw length for segment i.
To weigh the segment field according to the irradiated monitor unit(MU) for each segment field, we calculated the MU-weighted average segment width (ASWMU) by applying the MU weight in each segment field as:

Introducing MLC Position Error
AgilityTM MLC is composed of 80 pairs of 5 mm leaves, where the leaf position is determined through an optical system included in the linear accelerator head. The position of each leaf is verified by the light from the source at the tip of each leaf, which is transmitted to a charge-coupled device camera via a reflector. The detailed leaf positions are calibrated by adjusting the leaf offset or gain parameter. There are two leaf offset options: the major leaf offset option is used to control the positions of all leaf guides, and the minor leaf offset option is used to adjust the individual leaf position.
10
In this study, the major leaf offset option was adjusted to reproduce the occurrence of various MLC position errors, through which systematic MLC position errors were induced from the reference position of the MLC leaf guides to
Comparison of Dose Distribution Using Gamma Analysis
The treatment plan for DQA was recalculated using the virtual phantom CT provided by the manufacturer as the diode detector of the ArcCHECK phantom caused artifacts in the CT. The densities of the ArcCHECK body and air used in the dose calculation of the DQA plan in Monaco RTP were set to 1.15 and 0.01 g/cm3, respectively.
The SNC patient program was used to determine the gamma passing rate by comparing the dose distribution measured by ArcCHECK and the dose distribution calculated by the Monaco RTP. The global gamma passing rate was evaluated using the absolute dose mode with the threshold dose of 10%. The tolerance of gamma evaluation was set to 2%/2 mm to examine the effects of fine MLC position errors.
Correlation Analysis
To produce empirical results, we obtained the gamma passing rate according to the MLC position error for each VMAT plan, and the change in the gamma passing rate was represented by the gamma gradient (
Results
Table 1 lists the gamma passing rate and

Average gamma analysis results based on 2%/2 mm criterion for each MLC position error.
Gamma Analysis Results and Gradient of VMAT Plans for Prostate According to MLC Position Error.

Figure 5(a) and (b) show the change in the average gamma passing rate according to the direction of the MLC position error. The

Gradient of average gamma passing rate due to MLC position error: (a) Opened MLC position error, (b) Closed MLC position error.
Figure 6 shows the changes in the gamma passing rate according to

Gamma passing rate versus the MU weighted AWS for each position error. Each symbol shows a gamma passing rate according to the MLC position error, this graph shows that the change in the gamma passing rate for the MLC position error differs depending on each
Figure 7(a) and (b) represent the plot of the 


Correlation between the average segment width and the gradient as a function of MLC position error: (a) Opened MLC position error, (b) Closed MLC position error. A lower gamma gradient means that MLC position error has less impact on the gamma passing rate.
Figure 8 shows the average

The average MU weighted AWS according to the minimum segment width parameter for prostate plans.
Discussion
The results of this study showed that the gamma passing rates according to various systematic MLC position errors tended to decrease for the MLC position errors of 0.5 mm or higher. This is in good agreement with the previous studies.8,11 In addition, the rate of change in gamma passing rate as a function of the MLC position error was found to have a linear relation with
The gamma analysis using ArcCheck is one of the most commonly used patient QA method before VMAT treatment. Hilleman et al. 6 noted that gamma analysis using the 2%/2 mm criterion is more effective to check MLC position errors. Therefore, We evaluated gamma analysis results using ArcCheck based on 2%/2 mm criterion, and the difference in gamma passing rate was clearly observed depending on the MLC position error. Gamma analysis based on 2%/2 mm using ArcCHECK is a very useful method to find out the effect of MLC position errors on DQA results in a VMAT plan.
How
Systematic MLC position error are confirmed by picket fence QA after MLC position calibration. However, systematic MLC position error can occur over time due to mechanical defects (loosening of motor belt, change of motor rotational power with respect to motor current value, etc), and even after picket fence QA, if the QA result does not exceed the tolerance, correction is not performed every time. However, even small systematic position errors have been found to have a large impact on gamma pass rate.4,5,9,10 It is important to manage this risk. Therefore, it is recommended to check the plan's
Since this study was limited to prostate cases and VMAT plan, the correlation between
This study used only Monaco RTP to evaluate the effect of
Our study revealed a linear correlation between the
As a supplementary study, we established the VMAT plans for the same prostate patient by applying only the minimum segment width parameters differently as 5 mm and 15 mm, respectively. In addition, we evaluated gamma analysis using the 2%/2 mm criterion for VMAT plan with 0.25 mm systematic MLC position error. The results were 90.4% and 94.3% for 5 mm and 15 mm of the minimum segment width parameters, respectively. With a minimum segment width parameter of 15 mm, gamma passing rate is improved by approximately 3.9%. If
For example, if the minimum segment width is set to a small value when establishing the treatment plan, it will result in improved plan quality and a relatively narrow
Conclusion
We investigated the effect of MLC position error on the correlation between the change of gamma passing rate and
Footnotes
Abbreviations
Authors’ Note
This study was conducted after receiving approval from a certified institutional review board (D-1901-030-002, Dongnam Institute of Radiological & Medical Sciences Institutional Review Board). There is no probability of toxicity and side effect on the patient because it is a retrospective planning study conducted with the patient's existing records.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP) (NRF-2019R1C1C1008911).