
Abstract
Introduction
Radical nephrectomy is the preferred treatment for locally advanced renal cell carcinoma (RCC). However, a certain amount of waiting time before surgery is inevitable due to various reasons, such as the patient's attitude towards the disease, relative contraindications for surgery (such as cardiovascular and cerebrovascular accidents, COPD, etc), physical tolerance, the capacity of high-volume medical centers and the patient turnover rate.
Waiting for surgery can be a great anxiety for patients with little medical knowledge. 1 They may worry the disease progression that occurs while waiting for surgery will affect the prognosis. 2 Although some previous studies have shown that delayed surgery to some extent does not affect the prognosis of gastric and pancreatic cancers.3–5 However, it is not uncertain about the relationship between delayed surgery and survival of RCC. In 2006, a Canadian consortium of experts proposed a recommended maximum wait time of 90 days in cases with T1a RCC and 28 days in cases with symptomatic tumors. 6 During the COVID-19 pandemic, many operating rooms were reserved exclusively for emergent surgeries and many elective surgeries were forced to defer. A retrospective study analyzed whether delayed surgery in patients with clinical T1b-T2bN0M0 RCC led to disease progression or affected overall survival (OS). The results revealed that delaying surgery up to, and even beyond, 3 months did not increase the risk of tumor progression to clinically localized RCC. 7 Although these studies suggest that surgical wait time for localized RCC does not affect the prognosis, there is still no evidence for locally advanced RCC. Moreover, since the progression kinetics of clinically localized RCCs are lower than that of locally advanced RCCs, it is important to elucidate the relationship between surgical wait time and the prognosis of locally advanced RCC.
Thus, the present study aimed to evaluate the impact of preoperative wait time on OS in patients with pT3 RCC.
Patients and Methods
Surgical wait time was defined as the interval between initial imaging diagnosis and radical surgery of RCC. The vast majority of RCC patients were diagnosed incidentally through imaging examinations, and only a small number of patients were admitted to the hospital due to some symptoms (such as gross hematuria and flank pain).
OS was calculated from the date of surgery to the date of last contact or date of death. Cancer-specific survival (CSS) was defined as death primarily due to metastatic RCC. Recurrence-free survival (RFS) was defined as the length of time from completion of radical nephrectomy to disease recurrence.
Causes of death are defined as “all diseases, conditions and injuries that directly cause or indirectly contribute to death, as well as circumstances of accident or violence that cause any such injury.” In this study, the causes of death of patients were mainly divided into 2 kinds. The first is tumor-related, which is the recurrence and metastasis of RCC after surgery. The second is other causes, including accidents (such as traffic accidents, trauma, drowning, suicide, etc), chronic diseases (such as cardiovascular and cerebrovascular accidents, COPD, etc), and other primary tumors (such as liver cancer, lung cancer, etc).
In this study, patients were divided into 2 groups based on surgical wait time: short-wait group (≤60 days) and long-wait (>60 days) group. The clinicopathological characteristics and surgical data of each group were compared. The OS, CSS, and RFS of each group were calculated and compared. Age, gender, interval, tumor size, pathological grade, Eastern Cooperative Oncology Group performance status (ECOG PS), surgical approach, year of surgery, and pathological type were included in the multivariable model. Tumor size was included as a continuous variable in the multivariable model for analysis. Surgical wait time was included as a categorical variable in the multivariable model for analysis.
Patients and Data Collection
We retrospectively evaluated 138 consecutive patients with T3 RCC between July 2009 and December 2019. All of the patients underwent radical nephrectomy. We collected clinical and pathological data from the medical records, including age, gender, ECOG PS, American society of anesthesiologists (ASA) score, Charlson comorbidity index (CCI), clinical T stage, clinical N stage, body mass index (BMI), surgical wait time, tumor size, surgical approach, year of surgery, pathological type, tumor grade, pathological T stage, pathological N stage, and venous involvement. The study was approved by the institutional review board. Written informed consent was obtained from the involving patient for the publication of this study.
To confirm the original diagnosis, we invited an experienced urological pathologist to check all the pathological specimens again. The tumor stage was determined based on the American Joint Committee on Cancer (AJCC) TNM staging system for kidney cancer (eighth, 2017). The tumor grade was defined according to the 2016 WHO classification grading system.
Statistical Analysis
Median (interquartile range [IQR]) assessed continuous variables. Frequencies and proportions characterized categorical variables. Continuous variables were compared by independent sample t-test and Kruskal–Wallis test. The χ2 test was used to evaluate categorical variables. Cumulative survival was estimated by the Kaplan–Meier curves. Independent prognostic factors were identified by univariable and multivariable analyses using the Cox proportional hazards model. A two-sided P-value of <.05 was considered significant. All the statistical analyses were conducted using SPSS version 26.0 (IBM Corporation).
Results
Figure 1 shows the wait time from initial imaging examination to radical surgery. Table 1 summarizes the clinical characteristics. The median age of all patients was 60 years (IQR 52-68 years). The median surgical wait time for all patients was 16 days (IQR 10-77 days). The median surgical wait time of the short-and long-wait group was 12 days (IQR 8-16 days) and 92 days (IQR 79-115 days), respectively. The median body mass index is 22.2 kg/m2 (IQR 18.9-24.7 kg/m2). There were 56 patients(40.6%)with cT1, 45 patients (32.6%) with cT2, and 37 patients (26.8%) with cT3 (P = .328). There were 124patients with cN0, and 14 patients with cN1. There are no patients with M1 in our study. There were no significant differences in gender, ECOG performance status, ASA score, Charlson comorbidity index, clinical T stage, clinical N stage, and body mass index. As shown in Table 2, there were 128 patients (92.8%) with pT3a disease and 10 patients (7.3%) with pT3b disease. There was no patient with pT3c. The median tumor size of both groups was 7.0 cm (IQR 5.0-9.0 cm). Most patients underwent laparoscopy surgery, and approximately 50 (36.2%) of patients underwent open surgery. The majority of pathological subtypes were clear cell RCCs. There were 10 patients with papillary RCCs, 4 patients with chromophobe cell carcinoma, 3 patients with sarcomatoid RCC, 1 patient with multilocular cystic RCC, 1 patient with renal medullary carcinoma, 1 patient with translocation RCC. In all the patients, 9 patients (6.5%) with pN1. There are 5 cases (3.6%) in the short-wait group and 4 cases (2.9%) in the long-wait group (P = .373). There are no patients with distant metastasis and positive surgical margin in our study. Postoperative pathology showed venous involvement in 37 patients (26.8%), including 26 patients (18.8%) in the short-wait group, and 11 patients (8.0%) in the long-wait group (P

Wait time from the initial diagnosis to surgery.
Clinical Characteristics of Patients in the Short-and Long-Wait Groups.
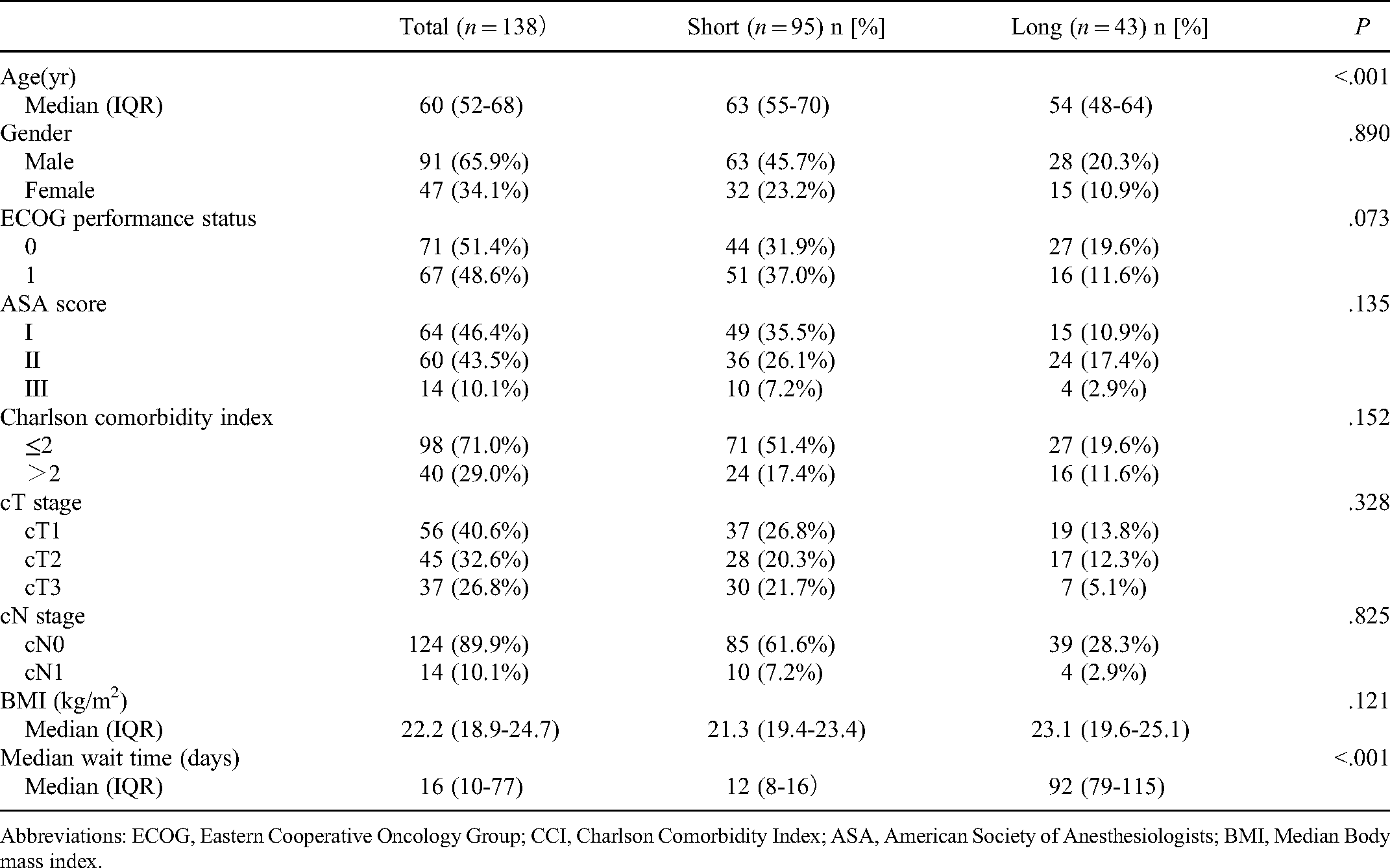
Abbreviations: ECOG, Eastern Cooperative Oncology Group; CCI, Charlson Comorbidity Index; ASA, American Society of Anesthesiologists; BMI, Median Body mass index.
Surgical and Pathological Characteristics of Patients in 2 Groups.

Abbreviations: ccRCC, clear cell renal cell carcinoma; n-ccRCC, non-clear cell renal cell carcinoma.
Until the last follow-up, 54 patients died. Among them, 49 patients (90.7%) died of tumor-related causes, and 5 patients (9.3%) died of other causes. There are 1 and 4 cases in the short-wait and long-wait groups, respectively. As shown in Table 2, there were no significant differences in tumor size, surgical approach, year of surgery, pathological type, tumor grade, pathological T stage, pathological N stage, and venous involvement.
Multivariable Analyses for OS and CSS
The median follow-up time for all patients was 36 months. The 5-year OS of the entire cohort was 56%. The 5-year OS of the short-wait group and the long-wait group was 65.0% and 40.9%, respectively (P = .03) (Figure 2). The 5-year CSS rates of the short- and long-wait time groups were 68.7% and 51.5%, respectively (P = .012). The 5-year RFS rates of the short- and long-wait time groups were 61.5% and 46.8%, respectively (P = .119). Table 3 describes the multivariable Cox regressions for patients with T3 RCC tumors. Multivariable analysis revealed that wait time and tumor size were independent risk factors for OS and that wait time was also an independent risk factor for CCS.

Comparison of overall survival curves between patients with different wait groups.
Multivariable Cox Model for Cancer-Specific Survival and Overall Survival.

Abbreviations: ccRCC, clear cell renal cell carcinoma; n-ccRCC, non-clear cell renal cell carcinoma; ECOG PS, Eastern Cooperative Oncology Group performance status.
Discussion
In this study, we try to explore the relationship between surgical wait time and outcomes of T3 RCC. The definition of surgical wait time is different in various studies and various tumors. In a study regarding gastric cancer, it was defined as the time from endoscopy for the initial diagnosis of gastric cancer to surgery. 4 In another study on prostate cancer, the surgical wait time was defined as the interval between prostate biopsy and radical prostatectomy. 8 This may be related to the different ways of diagnosis in different types of tumors. In this study, we defined it as the interval between the initial imaging diagnosis of RCC and the achievement of radical nephrectomy. For RCC, CT has a high diagnostic accuracy, so we do not recommend further preoperative renal tumor biopsy in patients due to undergo surgery. 9
Surgical wait time in cancer patients is affected by various factors, including patient- and health system-related factors. Patient-related factors include surgical contraindications (such as cardio-cerebrovascular accidents and poor respiratory function). These relative contraindications make the patients unable to tolerate surgery and need to be transferred to internal medicine for further treatment. In addition, the health care systems of different areas are organized in different ways. Due to the conflicts of a huge number of patients being referred to them and the limited capacity of hospital beds, a certain time is needed to be admitted for high-volume centers. Sometimes patients' subjective factors can also lead to a delay in surgery. This problem seems to have become more pronounced since the outbreak of COVID-19. A survey of urological patients who chose to postpone surgery due to fear of COVID-19 infection found that 47.9% of 332 urological patients chose to postpone surgery. In the oncology group, 87% of patients who requested a delay in surgery wanted to postpone surgery by more than 6 months. Among all the patients surveyed, 182 patients believed that the risk of COVID-19 was greater than the risk of delayed surgery. 10
From 1995 to 2005, wait time for cancer treatment has increased for all cancers in the United States. With the increase of caseloads, the median time from diagnosis to treatment is likely to continue increasing, potentially resulting in additional treatment delay. 11 In view of this situation, many scholars have studied the relationship between treatment delay and the prognosis of cancers. Some studies found that shortening the preoperative wait time has a positive impact on breast cancer patients,12,13 while some other researchers believed that preoperative waiting time had nothing to do with the prognosis of breast cancer.14–16 This controversy can be seen in other cancers. 17 Some studies even revealed that patients with long waiting time had better postoperative survival than those with the short waiting time. 18 The reason for this paradox may be related to the fact that patients in the short-wait group have advanced cancer stages, high tumor marker levels, less frequent R0 resection, and low body mass index. All of these factors were negative prognostic factors.11,18–20
In 2006, a Canadian consortium of experts proposed a recommended maximum wait time of 90 days in cases with T1a RCC and 28 days in cases with symptomatic tumors. 6 This recommendation seems to set a threshold beyond which patients may have adverse outcomes. However, a recent study on cT1b-cT2bN0M0 RCC patients found that delaying surgery >3 months after diagnosis did not significantly increase the risk of tumor progression and mortality in localized RCC. 7 The results of the 2 studies seem to be inconsistent. The differences may be partly due to the different criteria of inclusion and a different definition of preoperative wait time. So far, there were no studies exploring the relationship between preoperative wait time and prognosis of locally advanced RCCs. Therefore, our study included patients with T3 RCC. In our study, preoperative waiting time is an independent risk factor for OS for T3 RCCs. Delaying surgery beyond 60 days confers adverse prognosis among patients with T3 RCCs. Therefore, we believe that we should pay attention to this problem in the context of the shortage of medical resources in various countries during the current COVID-19 epidemic. A study on the priority treatment strategy of major uro-oncologic surgery during the COVID-19 pandemic found that of the 2387 large-scale urological cancer operations, 32.3% were listed as high-priority operations, of which radical nephrectomy accounted for 17.3%. They believe that about two-thirds of patients with prostate cancer, urothelial cancer, and renal cancer do not require priority surgery. The radical nephrectomy of cT2 and cT3 RCC should be included in the high-priority surgery group. And they found that among patients requiring high-priority surgery, about a quarter of patients are considered to have a higher perioperative risk (such as ASA ≥3), and these patients may occupy more medical resources. 21
In this study, we found that tumor size was also an independent risk factor for T3 RCC. This is consistent with previous studies.22–24 A study on the impact of tumor size on patient survival after radical nephrectomy for pathological T3a renal carcinoma suggested that tumor size significantly affected the prognosis of patients with pT3aN0M0. 24 They divided pT3a renal cancer patients into 3 groups according to the tumor size. The OS, CSS, and RFS of the patients in the (≤4 cm) group were significantly better than those in the (4-7 cm) group and the (>7 cm) group. Chen et al evaluated the prognosis significance of tumor size in pT3a RCC and found that patients with larger tumors tended to exhibit higher rates of symptoms and higher Fuhrman grades. Besides, large tumors indicated more necrosis features and were more likely to invade the collecting system and renal vein. 23
The present study has some limitations. Firstly, this study is a single-center retrospective study, there were only 138 cases between July 2009 and December 2019 in our hospital. And the follow-up time span is large (up to 11 years), so there is some loss in the process of data collection. Secondly, the stages of most patients are T3a diseases. There were only 10 patients with pT3b. There are no patients with T3c RCC. Therefore, we could not include the pathological T stage in the multivariable model. Thirdly, due to the small sample size, we cannot include all factors into the multivariable model, which is also one of the limitations of this study. Finally, the distribution ranges of wait time are relatively wide in the long-wait group. Further study is required to evaluate the influence of prolonged wait time on the prognosis of locally advanced RCCs.
Conclusion
For patients with T3 RCC, delay in radical surgery beyond 60 days conferred an adverse impact on OS and CCS. Therefore, surgeries should be arranged as soon as possible after excluding surgical contraindications for these patients.
Footnotes
Acknowledgments
This work was supported by the 2018 Doctoral Project for Innovation and Entrepreneurship of Jiangsu Province and the Natural Science Foundation Youth Project of Jiangsu Province (BK20190989).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for the publication of this report.
Ethical Approval
Ethical Statement: Our study was approved by the Medical Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (approval no. XYFY2021-KL031-01). All patients provided written informed consent prior to enrollment in the study.
Data Availability Statement
All data are available on request to the authors.
Trial Registration
Not applicable, because this article does not contain any clinical trials.