
Abstract
Introduction
Despite a low incidence among solid tumors, pancreatic cancer (PC) represents the fourth leading cause of cancer-related death in the United States and most European countries.1,2 In fact, it is the least common solid tumor among the 10 most common types of cancer listed by the American Cancer Society in 2020. 2 With a 5-year survival rate of only 9%, it carries a devastating prognosis and mortality rates remain unacceptably high. 2 At diagnosis, most people are above the age of 70 years and PC is more common in men than in women.3,4
Curative surgery remains the standard therapy for localized PC whereas only 15% to 20% of patients present with technically resectable disease.5,6 Adjuvant chemotherapy is the standard therapeutic approach and/or—although efficacy is not yet clear—chemoradiotherapy (in case of R1 resection). 7 Despite considerable progress in systemic therapy in advanced PC, the treatment intent for the latter patients remains palliative. However, the vast majority of phase III clinical trials investigating drugs for PC failed and only the results of three studies (investigating gemcitabine, nab-paclitaxel plus gemcitabine, and FOLFIRINOX) in the period from 1997 to 2015 should be considered practice changing.8–11 Despite the limited overall survival (OS) data in advanced PC, around 60% and 35% of patients receive a palliative second- and third-line therapy, respectively.12,13 The latter circumstance highlights the medical need for systemic therapeutic options beyond second line. Moreover, the clinical and OS benefit of a systemic third-line therapy remains unclear.
Preclinical studies suggest doxorubicin as a potential cytotoxic agent for PC and found that (pegylated) liposomal doxorubicin may yield better anti-tumor activity than free doxorubicin. 14 Data on the efficacy of liposomal doxorubicin in advanced PC patients are sparse with only small patient cohorts.15,16 Based on the latter reports, we offered nonpegylated liposomal doxorubicin (Myocet®) to advanced PC patients beyond second-line at our tertiary cancer center.
Material and Methods
In this retrospective analysis, patients with advanced/metastatic PC undergoing palliative systemic therapy with liposomal nonpegylated doxorubicin (Myocet®) at our institution were included. All patients were over 18 years old and suffered from pathologically confirmed pancreatic adenocarcinoma. Treatment decisions were based on the European Society for Medical Oncology (ESMO) guidelines at the time of treatment and interdisciplinary tumor board decision. 17 Patient data were obtained from medical records at the Department of Internal Medicine III, as well as from records from the Institute of Pathology. The study was conducted in accordance with the relevant guidelines and regulations. We retrospectively evaluated patient characteristics, Eastern Cooperative Oncology Group (ECOG) performance score, date of diagnosis, start of nonpegylated liposomal doxorubicin treatment, dose modifications during treatment, toxicity, response rates, and OS. Radiologic response assessment was based on computed tomography (CT) scans and if available on PET CT scans. Tumor response was classified as partial response, stable disease or progressive disease according to the World Health Organization criteria. 18 OS under liposomal doxorubicin was defined as the period between the date of treatment-start with liposomal doxorubicin and the day of death from any cause. Dose modifications were made at the discretion of the treating physician. As per our institutional standard treatment was continued until disease progression or unacceptable toxicities.
Nonpegylated liposomal doxorubicin (Myocet®) cycle intervals varied between 2 to 4 weeks. Based on the ECOG performance status, 5 patients required a reduced initial dose.
At the time of data analysis all patients had succumbed to their PC disease. The analysis was approved by the Salzburg Ethics Commission (EP/73/789) and informed consent was waived by the decision of the same institution.
Statistics
Descriptive statistics was chosen to analyze the data. Data are presented with median and if appropriate with range.
The objective response rate (ORR) was calculated as the sum of the rates of and partial remission.
OS estimates were calculated using the Kaplan–Meier method.
Results
In total, 475 PC patients were treated between 2006 and 2020 at our institution. Between 2008 and 2018, 28 patients with PC received liposomal doxorubicin at our center. Distribution between male and female was balanced (13 vs 15 patients). Figure 1 depicts the prior surgical and systemic therapy approaches of the 28 patients undergoing liposomal doxorubicin therapy.

Consort diagram showing the heterogeneous patient cohort at initial diagnosis (tx = treatment).
At the start of treatment with liposomal doxorubicin (Table 1), the median age was 67.5 years, ranging from 47 to 90 years. Liposomal doxorubicin was applied as palliative second line therapy in 5 patients (18%), third line in 18 patients (64%), fourth line in 4 patients (14%) and fifth line in 1 patient (4%). Prior palliative treatment included FOLFIRINOX (n = 18), gemcitabine plus nab-paclitaxel (n = 23), gemcitabine monotherapy (± antibody therapy within a clinical trial) (n = 4), nal-irinotecan plus leucovorin and 5-fluorouracil (5-FU) (n = 3) (with a total of 9 lines of diverse regimens).
Patient baseline characteristics prior to initiation of liposomal doxorubicin. (no. = number of patients, FOLFIRINOX = folinic acid, 5-fluorouracil, irinotecan, and oxaliplatin; 5-FU = 5-fluorouracil).

Among the 28 patients 55 cycles of nonpegylated liposomal doxorubicin were administered (median: 1.5 cycles/patient). Fourteen (50%) patients received only 1 cycle, 7 patients received two cycles (25%), 5 patients received 3 cycles (18%), and 2 patients received 4 or more cycles. For patients receiving more than 1 cycle, a tri-weekly treatment interval was most frequently chosen (n = 11, 79%), followed by bi-weekly (n = 2, 14%) and monthly (n = 1, 7%) intervals, respectively.
At the start of palliative treatment with liposomal doxorubicin liver metastases were most frequently detected (n = 18; 64%), followed by pulmonary (n = 8; 29%) and peritoneal (n = 5; 18%) metastases. The median level of carcinoembryonic antigen (CEA) was 11.4 ng/mL (range: 1.8-43 843) and the median level of CA 19 to 9 was 1031 U/mL (range: 7-38 787). After the last application of nonpegylated liposomal doxorubicin, the median CEA and CA19 to 9 levels rose to 33.6 ng/mL and 5418.5 U/mL, respectively (Figure 2).

Box plot diagram demonstrating the tumor marker dynamics before the start of nonpegylated liposomal doxorubicin and after the last application. The median (50th percentile) is marked by the cross (X) and upper (75th percentile) and lower quartiles (25th percentile) are marked by the borders of the box. The whiskers show the minimal and maximal values (apart from outliers outside of the 1.5 of the interquartile range). CEA in ng/mL, CA19 to 9 in U/mL.
Radiologic response assessment was feasible in 14 patients (50%). Progressive disease was documented in 12 patients (43%). One patient achieved a stable disease (SD) and a partial remission (PR), respectively, yielding an objective response rate of 7.1% (=1/14). Thirteen patients succumbed prior to the radiologic re-assessment and 1 patient was lost to follow-up.
The OS from initial advanced PC diagnosis among the 28 patients receiving liposomal doxorubicin was 20.9 months since initial diagnosis. The OS from start of liposomal doxorubicin was 2.1 months (for OS, please refer to Table 2).
Clinical outcome among 28 patients undergoing non-pegylated liposomal doxorubicin therapy (no. = number of patients, OS = overall survival).

Medical complications (episodes) after start of liposomal doxorubicin. (no. p. = number of patients, LFP = liver function parameters).
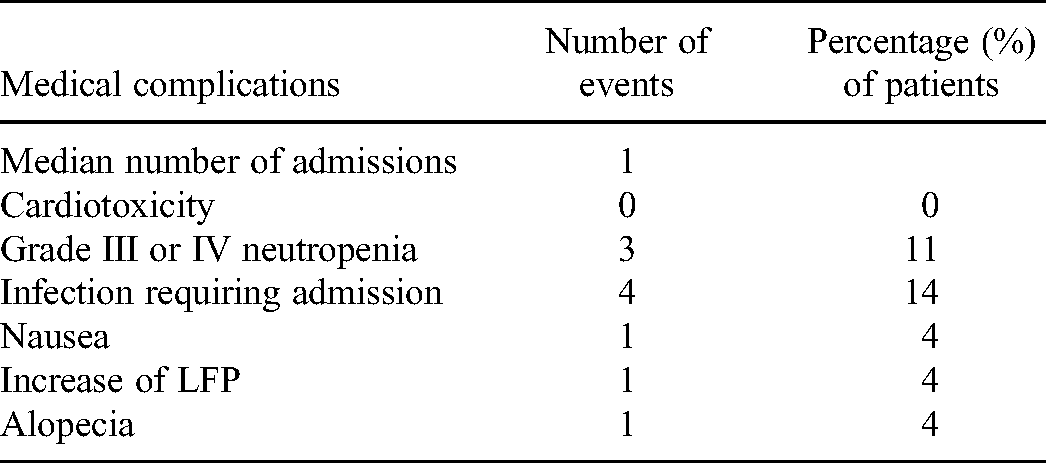
No case of cardiotoxicity was reported. Three patients developed neutropenia grade III or IV. Four patients required hospital admission due to infectious complications. In addition to that, one patient suffered from alopecia, one experienced an increase in liver parameters and one patient developed nausea after therapy. The median number of hospitalizations was 1. In 12 cases, the admission was required due to a reduction of general condition or pain associated with the underlying disease. No reductions were necessitated after the initiation of nonpegylated liposomal doxorubicin therapy.
Discussion
In this retrospective analysis, 28 patients with pretreated advanced PC were treated with liposomal doxorubicin after failure of established palliative standard regimens. Around 35% of patients diagnosed with PC qualified for third-line palliative systemic therapy. However, a standard third-line palliative therapy has not been established so far in PC.12,13
Chemoresistance by a plethora of mechanisms remains a major challenge for treatment of PC. 19 For example the extensive fibrosis surrounding tumor cells caused by cancer-associated fibroblasts inhibits drug delivery to tumor cells.20,21 Therefore, novel therapies have been extensively investigated. 22 In a minority of patients, molecular alterations offer targeted therapy options: Programmed cell death protein 1 inhibitors in case of mismatch-repair deficiency (dMMR) or microsatellite instability (MSI-high), larotrectenib and entrectinib in case of tropomyosin receptor kinase (TRK)-fusion positivity, and the poly(adenosine diphosphate–ribose) polymerase inhibitor olaparib in case of germline BRCA1/2 mutations.23–26 Some examples of recently investigated approaches to target the stroma include hedgehog inhibitors, recombinant human hyaluronidase, CD40 agonists, vitamin D analogues, and pegylated recombinant human IL-10.27–31 Aiming at targeting the tumor's metabolism, selective inhibition of pyruvate and ketoglutarate dehydrogenase as well as the use of L-asparaginase have been investigated. 32 Other more recent approaches used in clinical trials include masitinib plus gemcitabine, chemotherapy in combination with nivolumab, and the CD40 agonistic antibody sotigalimab.33–35
To our knowledge this retrospective analyses is the largest published cohort of patients with metastatic PC treated with liposomal doxorubicin. Furthermore, it is the first analysis report of nonpegylated liposomal doxorubicin efficacy among heavily pretreated patients. Two previous reports evaluated the anthracycline efficacy in 21 and 22 (with 16 evaluable for response) chemotherapy-naïve patients, respectively.15,16 In a phase II study by Halford et al published in 2001, 22 patients with unresectable PC were treated with pegylated liposomal doxorubicin. 15 Syrigos et al administered a combination of liposomal doxorubicin and docetaxel to a cohort of 21 chemotherapy-naïve patients with unresectable PC. 16 Data from the first study were inconclusive regarding the clinical benefit but 6 patients (38%) achieved stable disease after 2 cycles. 15 In the second study, despite clinical improvement after treatment, it did not translate into a statistically significant progression free survival. 16
We observed a partial remission in one patient and an SD in a second patient. Unfortunately, a disease progression was evident based on clinical, laboratory and radiologic findings among the remaining patients. The median OS of our study cohort was 2.1 months since the start of liposomal doxorubicin. If patients lost to follow up are included into the analysis until last time seen alive, these are (at least) 22.2 and 1.7 months, respectively. However, a slowdown of disease progression by the application of nonpegylated liposomal doxorubicin cannot be ruled out. We did not observe a clear objective benefit from the administration of liposomal doxorubicin. Although our analysis represents the largest patient cohort reported so far, the small sample size as well as the patient heterogeneity may be limitations of this analysis.
The efficacy of doxorubicin combined with other therapies such as L-DOS47 is currently being investigated in ongoing clinical trials (NCT04203641). L-DOS47 is an antibody–urease conjugate and liberates ammonia, which is thought to increase the microenvironment pH, thereby counteracting one of the tumor's resistance mechanisms. In addition to that, ammonia is cytotoxic and thereby thought to act synergistically with doxorubicin on tumor cells.
Furthermore, treatment with nonpegylated liposomal doxorubicin was generally tolerated in our cohort as evidenced by only a few adverse events during therapy.
Conclusion
Nonpegylated liposomal doxorubicin monotherapy did not achieve encouraging clinical outcome in pretreated pancreatic adenocarcinoma after failure of established treatment regimens. Our findings do not support its use beyond second line in daily clinical practice.
Footnotes
Acknowledgments
None
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
The analysis was approved by the Salzburg Ethics Commission (EP/73/789) and informed consent was waived by the decision of the same institution.