
Abstract
Background:
Lung cancer is the leading cause of cancer-related deaths and pulmonary carcinoids (PCs) account for almost 2% of all pulmonary malignancies. However, few published articles have reported prognosis and related factors of pulmonary carcinoid patients.
Material and Method:
The Surveillance, Epidemiology, and End Results (SEER) database was used to collect data of patients diagnosed with metastatic PCs from 2010 to 2016. The prognosis and survival of these patients were compared by employing Cox proportional hazards and the Kaplan-Meier survival analysis.
Results:
A total of 1763 patients were analyzed. The liver (668, 25.6%) was shown to be the most common metastatic site in the isolated organ metastasis cohort, followed by the lung (636, 24.4%), bone (562, 21.6%), and brain (460, 17.6%). Among the patients, the tumor metastasized to a single distant site included the liver, bone, lung, and brain. Cancer-specific survival (CSS) in metastatic PCs is determined by the site of metastasis and the total number of such sites. Pulmonary carcinoid patients with isolated liver metastasis manifested more favorable survival rates in comparison to patients having isolated metastasis in the lung, brain, or bone. The median CSS was 45, 7, 6, 5 months (P = 0.011). The number of distant metastatic sites and the location of distant metastasis were found to be independent risk factors for CSS. For patients with distant isolated metastasis, liver metastasis (P < 0.0001) had better CSS in comparison to those with bone metastasis. When compared to patients whose carcinoids had metastasized to the bones, patients with a brain (P = 0.273) or lung (P = 0.483) metastasis had the same CSS.
Conclusion:
Cancer-specific survival in metastatic PCs depends on the site of metastasis and the total number of such locations. PC patients with isolated liver metastasis manifested more favorable survival in comparison to patients with isolated metastasis in the lung, brain, or bone.
Introduction
Pulmonary carcinoids are the most commonly diagnosed pulmonary malignancies in children and adolescents. Although many efforts have been undertaken to improve the prognosis of PCs, few published studies have looked at the incidence and outcomes of carcinoid lung tumors in patients. PCs are a group of malignancies that fall into the category of neuroendocrine tumors (NETs) and share immunohistochemical, molecular, morphological, and ultrastructural characteristics. PCs are thought to be responsible for 0.5%-2% of all primary malignancies in the lungs. 1 -4 Recent studies have reported their age-adjusted incidence rate as 0.2-2/100,000 population/year in the western hemisphere. Twice as many females are diagnosed with PCs than males, 4 -6 and the patients with PCs are on average 10 years younger at diagnosis than those with other lung malignancies. 2,7 -9 In fact, PCs are undoubtedly the most usually diagnosed pulmonary cancers in children and adolescentst. 10,11 Four categories of these tumors commonly exist and include the typical pulmonary carcinoids (TPCs) with a more common occurrence, the large cell neuroendocrine carcinomas (LCNECs), the atypical pulmonary carcinoids (APCs) with a rather rare occurrence, and the common small cell carcinomas (SCLCs). In comparison to more common lung carcinomas such as non-small cell (NSCLCs) and small cell lung carcinomas, the risk factors of PCs have not been completely understood. Since atypical carcinoid was first described 12 and included in WHO classification, the lung carcinoid has been classified as typical and atypical. The major histological differences between the 2 types are mitotic rate and necrosis. It is generally believed that atypical carcinoid is more invasive than typical carcinoid and is more likely to metastasize to local lymph nodes and distant organs. 13 We tried to help clinicians in understanding the patterns and effects of distant metastasis in pulmonary carcinoids, which may facilitate correct treatment decisions and improved patient’s management. To investigate the association among the patterns and prognosis of distant metastasis in pulmonary carcinoids, we selected a large-scale electronic database such as the Surveillance, Epidemiology, and End Results (SEER). This research focuses on investigating the effects of site-specific patterns of distant metastasis on cancer-specific survival (CSS) in PC patients registered in the SEER database.
Methods
Patients
The SEER 18 registry database provides information and cancer data on the outcomes based on comprehensive data collected from patients across the United States, which accounts for 28% of the total population. Thus, data were collected from the SEER database and were then analyzed retrospectively. Though detailed records on the PCs could not be obtained right away from the SEER database, the selection variables of “Primary Site-Labeled” encoded C34.0 (main bronchus), C34.1 (upper lobe), C34.2 (middle lobe), C34.3 (lower lobe), C34.8 (overlapping lesion of the lung) and C34.9 (lung, NOS) let us get the PCs. 14 The tumor cases investigated in the current research came from patients identified in the SEER database (2010-2016). The inclusion criteria included: (1) Patients having PCs; (2) Patients manifesting definite lung, brain, liver, bone, and others metastases; (3) ICD-O-3 code lying within 8240/3 8244/3 8246/3 8249/3; (4) except PCs, patients exhibited no other primary tumor; (5) Survival information of the patients were documented; (6) Diagnosis was verified by histological analysis. Patients whose data showed no information of TNM status, distant metastatic sites, surgery, or follow-up, or whose diagnosis was based on a death certificate or an autopsy, were excluded. The variables included sex, race, age, primary tumor site, year of diagnosis, the occurrence of remote metastases (bone, lungs, liver, brain), histology, other remote metastases, however, none to brain, lung, liver, bone, and remote lymph node, survival time (months), survival status, surgery data, radiation therapeutics, and chemotherapeutics, vital status recode, T stage (T1, T2, T3, T4), N stage (N1, N2, N3, N4) and M stage (M0, M1) in 7th edition AJCC system. Due to the completeness of the chemotherapy record or biases arising from non-documented reasons for having or not getting chemotherapy, these data were categorized as “No/unknown” or “Yes.”
Statistical Methods
The Kaplan-Meier estimator was used to estimate survival curves, and the log-rank test was used to compare them. CSS was the primal endpoint considered for this work and was estimated from diagnosis date to the date of pulmonary carcinoids-specifically death. The Cox proportional hazards regression model was used to compare the univariate and multivariate survival analyses. Only factors that were significantly associated with survival were considered. Further identification of independent prognostic factors was carried out using multivariate Cox regression. The 95% confidence intervals (CIs) and representative hazard ratios (HRs) were determined from the model. IBM SPSS 25.0 software (IBM Corporation, Chicago, IL, USA) was used for performing the statistical analysis. The two-sided P-value < 0.05 was considered statistically significant.
Results
Characteristics of Patients
Using the SEER database, 1763 patients, including 1468 (83.27%) white, and 218 (12.37%) black, suffering from PC tumors were included in this study. Among all included patients, 856 (48.55%) were males. The mean age was 66 years (Table 1).
Clinical Features of the 1763 Patients With Metastatic Pulmonary Carcinoid Tumors.

a Percentages may not sum to 100%, due to rounding.
b Other race include: Asian/Pacific Islander, American Indian/AK Native.
c Resection of original tumor involves local tumor destruction, local tumor excision.
d Radiotherapy may include external beam radiation, radioactive implants only, radioisotopes only, and radiation not otherwise specified.
Treatment
A total of 151 (8.56%) patients went through surgery, 645 (35.59%) patients received radiotherapy, while 977 (55.42%) patients received chemotherapy (Table 1).
Patterns of Distant Metastases
Out of the total 1763 patients, 856 patients (48.55%), had distant metastasis at one site only, 626 patients (35.5%) manifested multiple organ metastasis, and 281 patients (15.9%) had other metastases. Further, 213 patients (12.08%) had isolated brain metastases, 318 patients (18.04%) had isolated lung metastases, 136 patients (7.71%) manifested isolated bone metastases, and 189 patients (10.72%) manifested liver metastases alone. In total, 1763 patients acquired distant metastases in 2607 sites. The liver was shown to be the most common metastatic site (668, 25.6%), whereas metastasis in the lung, bone, and brain was reported to be 24.4% (636), 21.6% (562), and 17.6% (460), respectively. Table 2 presents the location and distribution of remote metastasis in detail.
Patterns of Distant Metastasis for the 1763 Patients Who Had Metastatic Pulmonary Carcinoid Tumors.
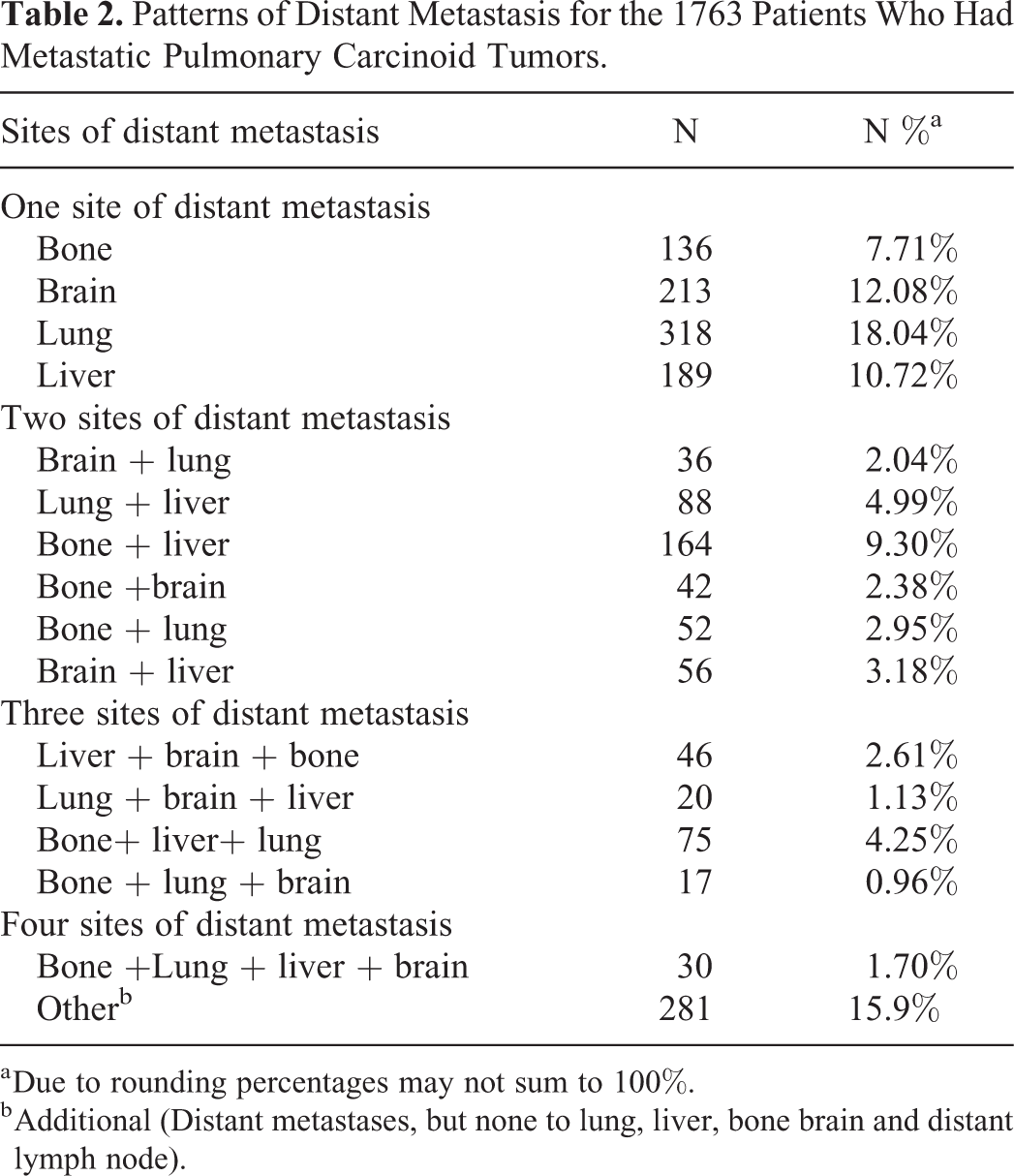
a Due to rounding percentages may not sum to 100%.
b Additional (Distant metastases, but none to lung, liver, bone brain and distant lymph node).
Survival of Patients and the Influence of Metastatic Patterns on Prognosis
The median CSS for distant metastasis involving multiple sites was 5 months. The median CSS for distant metastasis at a single location was 7 months. The values for CSS in both cases differed significantly (P < 0.001; Figure 1), and the statistical power was 91%. The median values of the patients’ CSS for single-site distant metastasis were 45, 7, 5, and 6 months for patients with liver, bone, brain, and lung metastasis, respectively (Figure 2). The results of Univariate Cox regression analysis showed that for individuals with remote metastasis at a single site (n = 856), CSS was found to be associated with age, sex, T stage, N stage, surgical resection of the primary tumor, radiotherapy as well as the location of remote metastasis (Table 3). Sex, age, T stage, radiation, N stage, remote metastasis site, and surgical resection of the primary tumor were all determined to be valid prognostic factors for CSS in the entire cohort (Table 3).
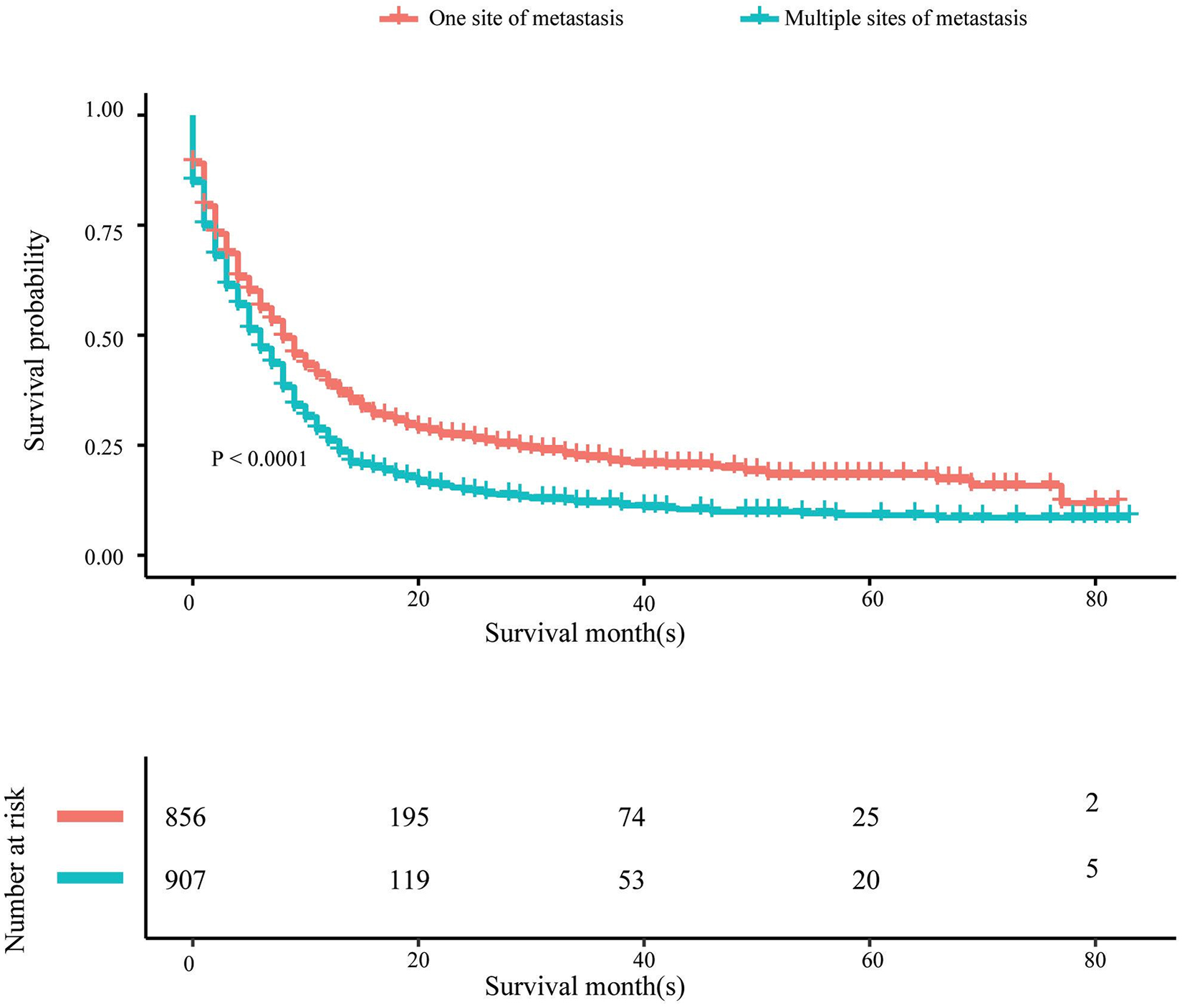
Cancer-specific survival curves for a subject having only one site of remote metastasis and multiple sites of remote metastasis.

Cancer-specific survival curves for subjects having the various single site of remote metastasis.
Univariate Cox Regression Analysis of Prognostic Factors for Cancer-Specific Survival in Metastatic Pulmonary Carcinoid Tumors.

a HR in the light of Cox proportional hazards model.
b Other race include: Asian/Pacific Islander, American Indian/AK Native.
c Resection of the original tumor comprises local tumor excision, local tumor destruction.
d Radiotherapy involves radioisotopes only, radioactive implants only, external beam radiation and radiation not otherwise specified.
Subsequently, multivariate Cox regression analysis was performed and revealed that age, N stage, chemotherapy, the location of remote metastasis, surgical resection of the original tumor, and the location of distant metastasis were independent prognostic factors for individuals with only one distant site of metastasis (Table 4). When the entire cohort (n = 1763) was considered, the age, chemotherapy, N stage, resection of the original tumor by surgery, and the location of distant metastasis were found as independently acting prognostic factors for CSS (Table 4).
Multivariate Cox Regression Analysis of Prognostic Factors for Cancer-Specific Survival in Metastatic Pulmonary Carcinoids.

a HR in the light of Cox proportional hazards model.
b Other race include: Asian/Pacific Islander, American Indian/AK Native.
c Resection of the original tumor comprises local tumor excision, local tumor destruction.
d Radiotherapy involves radioisotopes only, radioactive implants only, external beam radiation and radiation not otherwise specified.
Among patients with a single site of distant metastasis, multivariate analysis showed that the site of distant metastasis was an independent prognostic factor for CSS.
Multivariate analysis revealed the location of distant metastasis as an independent prognostic factor for CSS in individuals whose tumor had metastasized to a single distant location (Table 4). Keeping bone metastasis as a point of reference, patients with liver metastasis (HR = 0.45; 95% CI = 0.33-0.6; P < 0.0001) were found to have an improved CSS, whereas lung (HR = 1.09; 95% CI = 0.86-1.37; P = 0.483) and brain (HR = 1.15; 95% CI = 0.9-1.46; P = 0.273) metastases had similar identical CSS.
Multivariate analysis revealed the total count of metastasis locations as an independent prognostic factor when the entire cohort was taken into account for predicting CSS (Table 4). Patients with only isolated distant metastasis had a longer CSS when compared to patients with multiple metastatic locations (HR = 1.596; 95% CI = 1.416-1.800; P < 0.001).
Discussion
According to the SEER database, the number of PCs has increased at a remarkable rate of 6% per year over the last 3 decades. 7,15 This article elaborates the relationship between prognosis and site-specific metastatic patterns in PC tumors, including age, sex, race, T stage, and N stage, using data from the SEER database. The findings will provide useful information for the therapy and diagnosis of PC cancers. The liver (25.6%) was shown to be the most prevalent metastatic site in our analysis of 1763 patients with PC tumors, with the proportion of metastasis in other organs being as follows: lung (24.4%), bone (21.6%), and brain (21.6%). (17.6%). These proportions were in good agreement with autopsy findings and are also consistent with previous reports. 16 Because the SEER database does not contain the explicit ICOD code for typical carcinoid tumor, it is unable to discriminate between typical and atypical carcinoids. Furthermore, our research does not adequately reflect metastasis from PC tumors because the SEER database only includes 4 metastatic sites at diagnosis.
In this case, 1120 (63.5%) patients had T3 or T4 disease and 1095 (62.1%) patients had N2 or N3 disease. The late development of symptoms, the majority of which are symptoms without specificity, is one crucial aspect that explains these findings. For instance, 30% of patients were asymptomatic at presentation. 5 Multivariate Cox regression analysis showed that survival rates were similar regardless of the T stage. Yaldız et al also emphasized that tumor size was not prognostic in their experience. 17
In terms of the N stage, patients with N1, N2, and N3 cancer had a lower survival rate than those with N0 cancer. Although no comparison was done between the survival of N1, N2, and N3 patients, HR increased as the N stage increased. Aydin et al and Yaldız et al emphasized that the involvement of lymph-node was the key prognostic factor affecting long-term survival. 17,18 On the other hand, Karapınar et al reported that, contrary to their expectation, N status did not impact survival in their investigation. 19 The apparent disagreement between the outcomes of these studies can be attributed to the relatively limited size of the sample in earlier works, which subsequently makes it harder to determine the correlation between N-state and survival.
Our study indicated that the total count of metastasis sites and the exact location of distant metastasis are valid independent prognostic factors and affect the survival outcome of PC patients experiencing distant metastases. For individuals with brain, liver, bone, and lung metastases, the median CSS was estimated to be 5, 45, 7, 6, months, respectively.
In our study, both the location and count of distant metastasis were determined as independent prognostic factors for CSS. Some retrospective studies of non-small cell lung cancer have found that single-site metastasis has a better prognosis than multi-site metastases and that single-site metastatic survival varies from site to site, with liver metastasis having the worst prognosis. However, previous studies have not investigated the interrelation between site-specific distant metastasis and prognosis in PCs. 20 -23 According to our data, patients with a single distant metastasis also have a longer survival time than those with multiple metastases sites. Our data revealed that patients with bone metastasis have a poorer CSS in comparison to those with liver metastasis, whereas CSS in patients with brain, lung, and bone metastasis did not differ significantly. This is different from previous studies. The main reason may be that liver metastases are easier to be completely removed than brain or lung metastases in PC patients. In our study, metastasis resection rate was highest in patients with liver metastasis (37, 19.6%), and for the brain, bone, and lung metastases, the resection rates were 5.6% (12), 8.8% (12), and 11.9% (38), respectively. A 70% rise in the 5-year overall survival rate has been reported upon complete resection of liver metastases. 24 Nagashima et al and Hakoda et al also found that resection of liver metastases from NSCLC may offer the possibility of long-term survival. 25,26 Thus, the results of our study may be useful in making practical and informed clinical decisions, such as a more precise assessment of the prognosis of patients with metastasized PC tumors.
For early and resectable PC tumors, surgery is a key therapeutic intervention. 18,24,27 Most surgeons recommend the surgical resection of carcinoid tumors. 27,28 Some previous retrospective investigations have reported considerably better survival outcomes for patients who underwent surgery, than those who were not subjected to surgery. 29,30 In our current research, the multivariate Cox regression analysis revealed the surgical resection of the original tumor as an independent prognostic factor in both categories. However, the prospects of the treatment of PC tumors by surgical resection must be confirmed by prospective large randomized studies in the coming years.
The prognostic values of radiation therapy or systemic chemotherapy have been reported for PC tumors by some limited evidence with small cohorts. However, the results were not consistent. 31,32 Nussbaum et al have found that patients who underwent lobectomy did not show improved survival when subjected to adjuvant chemotherapy. 33 On the contrary, Caplin et al have reported that inoperable tumors, particularly low-grade TCs and ACs are therapeutically affected by chemotherapeutics. 34 For instance, for both advanced TC and AC, chemotherapy was found to be an effective regimen by Patrick M and T. Walter. 16,35 Chemotherapy also surfaced as an independent prognostic factor in this work, both in patients who had a single metastatic site as well as in the entire cohort. Hence our conclusions validate the status of chemotherapy as the recommended strategy for treatment. However, there may be a need for surgery to control the local disease. As for palliative radiotherapy, no consensus exists regarding its value in metastatic PC tumors. Our results demonstrated that radiotherapy results in improved survival, however, it does not qualify as an independent prognostic factor. Consequently, it suggests the use of chemotherapy and radiotherapy in combination to improve survival.
The current research analysis has certain limitations. The retrospective collection of patient data is one important aspect limiting the overall significance of our study, thus the study inherently involves selection bias. Additionally, laboratory tests, smoking history, imaging, detailed chemotherapy regimens, and tumor recurrence, and certain other key variables may have a direct influence on the survival analysis. However, they were not taken into consideration due to the limitations of the SEER database. Similarly, because the SEER database was based on data for just 4 synchronous sites of distant metastasis, we were unable to obtain more information on the timings and occurrence of secondary metastasis, as well as data on additional sites of metastasis. Finally, the sample size was relatively limited for the analysis of the subjects with bone or brain metastasis. This in turn reduces the reliability of statistics and the extent of confidence of any associations comprising the 2 sites of metastasis. It is also noteworthy that the “no/unknown” category in the SEER database limits the patient information due to the uncertainty as to whether the patients categorized in the category are due to missing data or due to the lack of treatment. However, the possibility of survival benefits erroneously being linked to surgery and chemotherapy cannot be ruled out. Hence, more studies based on the use of reliable data are required to validate the findings and develop a deeper understanding of the treatment’s effects on survival.
Conclusion
In conclusion, our study demonstrated that both the location and the number of metastatic lesions were independent prognostic factors of PCs. Patients with multiple metastatic lesions had a worse prognosis than patients who just had one. And patients suffering from PCs with metastasis in the liver seemed to have improved outcomes and survival statistics in comparison with patients who manifested isolated lung, brain, or bone metastasis. We also found that resection of the primary lesion and chemotherapy can improve the survival of patients. Altogether, understanding the prognostic value of different metastatic PC sites may be useful for individualized precision treatment and improving future outcomes.
Footnotes
Authors’ Note
Jiandong Zhang and Qiongjie Yu contributed equally to this work. Conception and design: Jiandong Zhang and Qiongjie Yu. Administrative support: Dezhi Cheng and Zhifeng He. Provision of study materials or patients: Jiandong Zhang. Collection and assembly of data: Jiandong Zhang. Data analysis and interpretation: Qiongjie Yu and Yi He. Manuscript writing: All authors. Final approval of manuscript: All authors. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. Since the data were from the SEER database, informed patient consent and ethical approval were not required.
Acknowledgments
The study was supported by Wenzhou Public Welfare Science and Technology Plan (No. Y20180175). In addition, I thank Xuedan Du for comments on the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Wenzhou Public Welfare Science and Technology Plan (No. Y20180175).