
Abstract
Objective:
To evaluate the prognostic value of tumor infiltrating lymphocytes (TILs) in nasopharyngeal carcinoma (NPC) patients.
Method:
Meta-analysis was performed on eligible studies that was identified by systematic searching of Google scholar, MEDLINE, CNKI, Scopus, PubMed, PMC, Embase and Web of Science databases. The study protocol was registered in International Platform of Registered Systematic Review and Meta-Analysis Protocols-INPLASY (registration number: INPLASY202160014). Databases were searched from inception to January 20, 2020 to identify eligible studies. Those studies that evaluated survival in the form of hazard ratio (HR) in TILs of NPC patients was analyzed. All statistical analysis was performed by using STATA version 16.0 software.
Result:
Fourteen studies with a total of 3025 patients was analyzed. The pooled result showed that high TILs was significantly associated with favorable overall survival (OS) (HR = 0.55; 95%CI = 0.39-0.77; P = 0.001) and disease free survival (DFS) (HR = 0.60; 95%CI = 0.44-0.81; P = 0.04). Interestingly, high intratumoral TILs had relatively better OS (HR = 0.45; 95%CI = 0.35-0.58; P = 0.006) than stromal TILs (HR = 0.59; 95%CI = 0.36-0.97; P = 0.03). Moreover, an increased level of CD4+ cells infiltration was correlated with favorable OS (HR = 0.4; 95%CI = 0.18-0.85; P = 0.01). CD3+, CD8+ and FoxP3+ lymphocyte’s better prognosis was not statistically significant for OS (P = 0.09; P = 0.07; P = 0.52) and for DFS (P = 0.13; P = 0.29) respectively. However, subgroup analysis of intratumoral CD3+ (HR = 0.48; 95%CI = 0.33-0.70; P = 0.05) and intratumoral CD8+ (HR = 0.32; 95%CI = 0.16-0.62; P = 0.001) was significantly associated with improved OS, but not significant in stromal CD3+ (HR = 0.66; 95%CI = 0.20-2.20; P = 0.62).
Conclusion:
TILs were variably correlated with better prognosis depending on their microanatomic location and subset of TILs in NPC patients. CD4+, intratumoral CD3+ and intratumoral CD8+ lymphocytes could predict favorable patient outcome which suggest that their role in mediating antitumor immune response could potentially be exploited in the treatment of NPC patients. Future large study on the prognostic value of microanatomic location of TILs is needed for confirmation.
Introduction
Nasopharyngeal carcinoma (NPC) is a common malignancy in head and neck with distinct racial and regional prevalence. 1 -3 Due to its highly invasive and relatively high metastatic potential of the disease, NPC has unfavorable prognosis. 1,4,5 Evidences show that approximately 20%-30% of cases would recur, despite substantial improvement in radiotherapy and the widespread use of concurrent chemotherapy for localized therapy exists. 4,6
Recent advances in the characterization of immune status in the tumor microenvironment (TME) is becoming a breakthrough in treating recurrent or metastatic NPC patients. Particularly, tumor infiltrating lymphocytes (TILs) as a rapidly emerging powerful prognostic tool to guide treatment, their presence is associated with favorable outcome in different types of cancers. 7,8 However, different subset of lymphocytes have different or even opposing biological function in tumor microenvironment which suggest that TILs have dual role by conducting both host defense and tumor progression. 1,8 For instance, evidences show that high CD3+ or CD8+ infiltration was an independent factor for favorable overall survival (OS) and disease specific survival (DSS) in head and neck cancer. 9 -11 In contrast, as regulatory T-cells’ main role is maintaining immunological tolerance, therefore are considered suppressors of antitumor immune response. 12 Furthermore, according to Lei et al, the prognostic value of CD3+ and CD8+ T-cells could depend on lymphocytes infiltration pattern. 13 Here, it is the TILs that are within tumor cells or located with close proximity to tumor parenchyma that determines the prognosis. 13 Contrarily, some studies indicated that stromal TILs didn’t exhibit prognostic value. 14,15 Therefore, TILs as the complicated functional heterogeneity and as the most important monitor of immune response, are a focus of research in NPC. A number of studies on the association of TILs and NPC had conducted, however, their locational prognosis in intratumoral and stromal TILs remain controversial. Therefore, we conducted meta-analysis on prognostic value of TILs in NPC patients which was expressed as hazard ratio for overall survival and disease free survival.
Materials and Methods
Search Strategy
We used the strategy of the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guideline. 16 The protocol for this study has been registered in the International Platform of Registered Systematic Review and Meta-Analysis Protocols-INPLASY (registration number: INPLASY202160014). We systematically searched the Google Scholar, MEDLINE, Scopus, PubMed, Embase, Web of Science and PMC databases to identify and include potential studies before January 20, 2020. The search was performed using the following keywords: “prognosis OR survival” AND “tumor infiltrating lymphocytes OR lymphocytes, tumor infiltrating OR TILs” and “nasopharyngeal carcinoma.”
The following eligibility criteria were used to include studies in the meta-analysis: (a) published original articles. (b) Studies that evaluated the prognostic value of TILs in NPC. (c) Studies that reported disease free survival (DFS) or overall survival (OS) expressed in the form of HR with 95% confidence interval (CI), or that reported Kaplan Meier (KM) curve. (d) Studies that used immunohistochemistry (IHC).
Studies that did not provide enough data for analysis such as conference abstracts, case reports and non-English articles were excluded.
Data Extraction and Quality Assessment
The retrieved published articles were sorted by EndNote 7.0 (Thomson Reuters). Two pathologist extracted the data based on the established inclusion and exclusion criteria. Consensus was reached when discrepancies appeared. The extracted data from the included studies were: first author, publication year, country, sample size, cutoff value, lymphocytes subtypes, location of infiltrating lymphocytes, disease stage, follow-up time, age range and outcome.
We evaluated the quality of each study by using Newcastle-Ottawa quality assessment scale (NOS). Studies with score of ≥6 were regarded as high quality.
Statistical Analysis
Each study’s hazard ratio along with its 95%CI was extracted. If only Kaplan Meier curve was provided, then the survival data were extracted from it by using WebPlotDigitizer version 4.4 (https://automeris.io/WebPlotDigitizer). 17 Statistical heterogeneity was assessed by Chi-square (I2) test and visual inspection forest plot. I2 > 50% indicated heterogeneity. Random effect model was used if hazard ratio showed heterogeneity, otherwise fixed effect model was used. In order to identify the source of heterogeneity and evaluate the influence of different adjustment factors or confounders, subgroup analysis was conducted accordingly. If HR estimate was reported in opposite direction, we inverted the HR and 95% CI. All statistical analysis was evaluated using STATA version 16.0 software. P-value < 0.05 was considered as statistically significant.
Results
Study Characteristics
PRISMA flow diagram of identified studies for the meta-analysis is shown in Figure 1. Thus, 14 studies from Austria, China, Finland, Japan, Netherland, Saudi Arabia, and Thailand, Tunisia countries were included in the analysis (see the Table 1). All studies we identified were retrospective cohort studies.

PRISMA flow diagram for retrieved articles.
Characteristics of Included Studies in the Meta-Analysis.

Abbreviations: OS, Overall survival; DFS, Disease free survival; ROC, Receiver operating characteristic curve; TIL, tumor infiltrating lymphocyte; S-TIL, stromal TIL; I-TIL, intratumoral TIL; NOS, Newcastle-Ottawa quality assessment scale; NR, not reported.
Sample size of each study ranged from 55 to 1490 patients which totaled 3025 patients. HR and its corresponding 95%CI for OS and DFS was extracted directly from the given data of most studies, while few remaining studies were calculated from KM curve.
Meta-Analysis Results
Fourteen studies 5,18 -30 were pooled and evaluated for analysis of TILs lymphocytes for OS and DFS in NPC patients. Wang et al 24 have analyzed a large cohort and validated it with an independent cohort focusing on the total intensity of TILs, however most the rest of the studies focused on a set of phenotypic subtypes of immune cells (including CD3, CD4, CD8, regulatory T cells and macrophages). The pooled result showed that TILs were favorable prognostic markers for DFS (HR = 0.60; 95%CI = 0.44-0.81; P = 0.04) and OS (HR = 0.55; 95%CI = 0.39-0.77; P = 0.001) in overall population (Figure 2). Favorable OS was also found in intratumoral TILs (HR = 0.44; 95%CI = 0.34-0.57; P = 0.006) and stromal TILs (HR = 0.59; 95%CI = 0.36-0.97; P = 0.03) (Figure 3A). Moreover, improved DFS showed in intratumoral TILs (HR = 0.55; 95%CI = 0.41-0.74; P = 0.005), but not statistical significant in stromal TILs (HR = 0.75; 95%CI = 0.36-1.55; P = 0.13) (Figure 3B).

Forest plot of the relationship between TILs (A) OS, and (B) DFS in total NPC populations. TILs indicates tumor infiltrating lymphocytes; NPC, nasopharyngeal carcinoma; OS, overall survival; DFS, disease free survival; HR, hazard ratio.

Forest plot of the relationship between TILs location and (A) OS; (B) DFS in NPC. TILs indicates tumor infiltrating lymphocytes; NPC, nasopharyngeal carcinoma; OS, overall survival; DFS, disease free survival; HR, hazard ratio.
Epstein-Barr virus (EBV) tended to be associated with better outcome in NPC patients, though the correlation was not statistical significant (HR = 0.92, 95%CI = 0.38-2.26, P = 0.48 for DFS; HR = 0.77, 95%CI = 0.28-2.09, P = 0.24 for OS) (Figure 4).

Forest plot of EBV+ NPC for DFS and OS. EBV+, Epstein-Barr Virus positive; NPC, nasopharyngeal carcinoma; OS, overall survival; DFS, disease free survival; HR, hazard ratio.
Subgroup Analysis of TILs Subsets
CD3+
Four studies evaluating the prognostic value of CD3+ in NPC were included in our study. The pooled result revealed that high CD3+ lymphocytes tended to improved OS (HR = 0.45; 95%CI = 0.16-1.25; P = 0.09) (Figure 5). Further subgroup analysis indicated that patients with high intratumoral CD3+ lymphocytes infiltration was correlated with better OS (HR = 0.48; 95%CI = 0.33-0.70; P = 0.005), while stromal CD3+ had no statistical significant correlation for DFS (HR = 0.66; 95%CI = 0.20-2.20; P = 0.62) (Figure 6).

Forest plot of the relationship between subset of TILs and OS in NPC. TILs indicates tumor infiltrating lymphocytes; NPC, nasopharyngeal carcinoma; OS, overall survival; HR, hazard ratio.

Forest plot of the relationship between locational subtype of TILs and OS in NPC. TILs indicates tumor infiltrating lymphocytes; NPC, nasopharyngeal carcinoma; OS, overall survival; HR, hazard ratio.
CD4+
Data from only 2 studies were pooled to analyze the impact of CD4+ cells infiltration on OS. These 2 studies were conducted on EBV-associated NPC study. Here, high CD4+ infiltrate was associated with better OS (HR = 0.4; 95%CI = 0.18-0.85; P = 0.01) (Figure 5). This suggest that CD4+ immunity could contribute for EBV control.
CD8+
Most of the included studies reported the prognostic value of CD8+ TILs. The pooled result showed that high infiltration of CD8+ cells seem to have improved prognosis (HR = 0.57, 95%CI = 0.26 -1.24, P = 0.07 for OS; HR = 0.71, 95%CI = 0.22-2.33, P = 0.29 for DFS), although the association was statistical insignificant (Figures 5 and 7) respectively. However, in subgroup analysis, CD8+ cells infiltrated in the intratumoral site showed significantly improved OS (HR = 0.31; 95%CI = 0.16-0.62; P = 0.001) (Figure 6). Because only one study, Wang et al, 20 reported on the association of CD8+ stromal TILs with OS, we did not perform meta-analysis on this subgroup.

Forest plot of the relationship between subset of TILs and DFS in NPC. TILs indicates tumor infiltrating lymphocytes; NPC, nasopharyngeal carcinoma; DFS, disease free survival; HR, hazard ratio.
FoxP3+
Only 3 articles analyzed the association between FoxP3+ and OS. The pooled result indicated that FoxP3+ lymphocytes did not show statistical significant for prediction of OS (HR = 0.84; 95%CI = 0.28-2.54; P = 0.52) (Figure 5).
Geographical region
According to the geographical locations of the included studies, high TILs in endemic (HR = 0.63; 95%CI = 0.42-0.93; P = 0.03) and sporadic (HR = 0.40; 95%CI = 0.21-0.74; P = 0.01) NPC patients was variably associated with improved OS; while in sporadic NPC populations was statistical insignificant for DFS (HR = 0.79; 95%CI = 0.322-1.93; P = 0.49) (Figure 8).
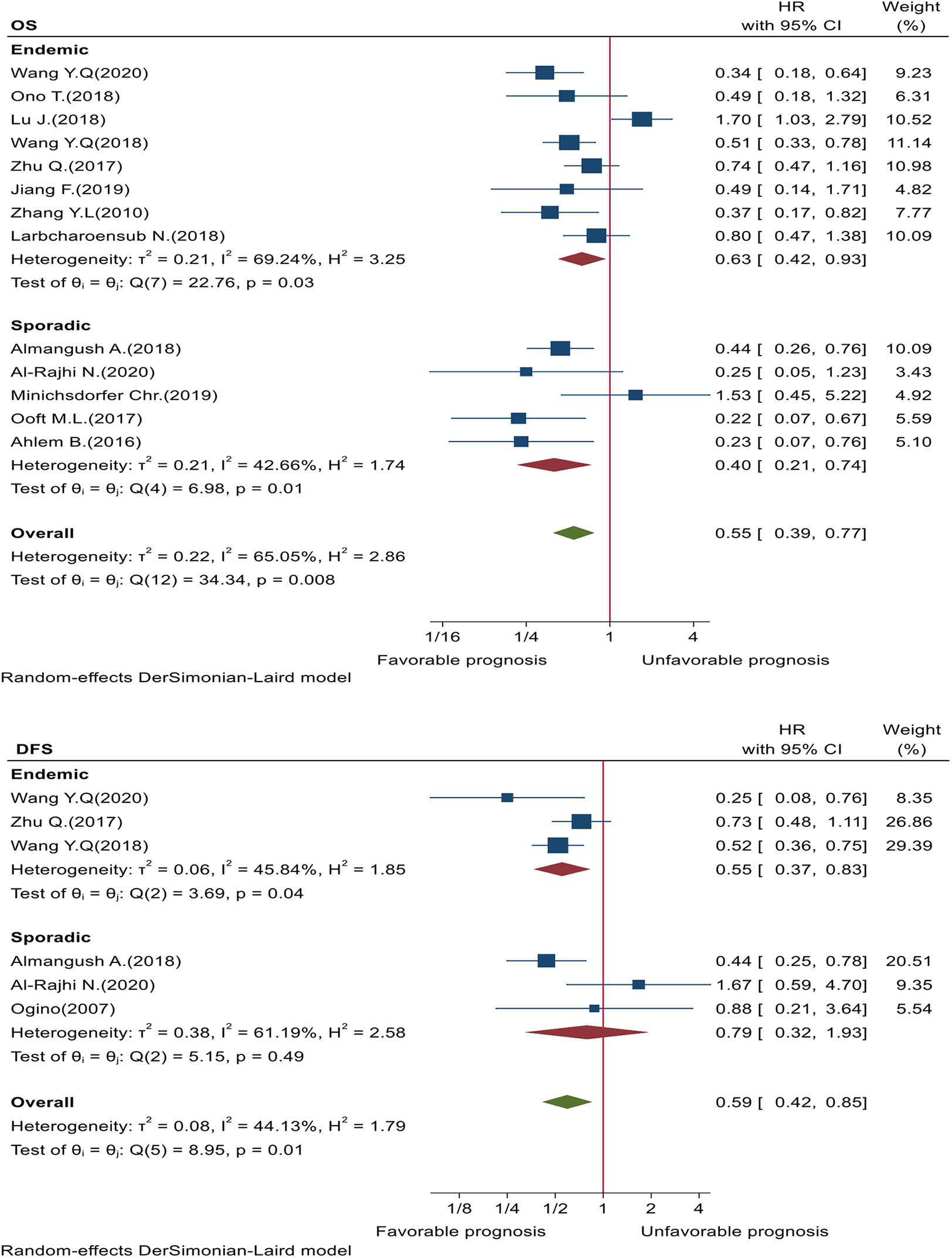
Forest plot of NPC by geographical region for OS & DFS. NPC indicates nasopharyngeal carcinoma; OS, overall survival; DFS, disease free survival; HR, hazard ratio.
Discussion
To our knowledge, this is the first meta-analysis that evaluated the prognostic value of TILs in different micronatomic locations of NPC patients. Our pooled analysis revealed that high TILs was significantly associated with better OS and DFS in NPC patients. The result was consistent with previous meta-analysis studies in TILs of nasopharyngeal carcinoma, 31 head and neck squamous cell carcinoma, 8 oral squamous cell carcinoma, 32 colorectal cancer, 33 breast cancer, 34 ovarian cancer, 15,35 esophagus cancer, 36 pancreatic cancer, 37 hepatocellular carcinoma, 38 non-small cell lung cancer, 39 and in cohort study of head and neck carcinoma. 7,9 Our study is different from the previous meta-analysis study on NPC 31 that we have evaluated on the microanatomic location of TILs in predicting prognosis for NPC patients.
NPC, particularly non-keratinizaing NPC is associated with EBV. And it is associated with high lymphocytes infiltration in tumor stroma which is considered a target for immunotherapy. 3 Our pooled result indicated that EBV was related with improved outcome for NPC patients, though it was not statistical significant. Some reasons might be explained why the observed association was not significant. First, as TILs could be significantly different EBV negative and positive, it is especially the composition of the lymphocytes infiltrate that determines the prognosis. 25 The other reason could be attributed due to the functional heterogeneity of EBV strains that lead to variety interactions with TILs in NPC patients. Therefore, multiclassification analysis might be feasible and reasonable. For instance, our meta-analysis result on 2 EBV-associated NPC studies revealed that high CD4+ was associated with improved OS. This suggests that CD4+ lymphocytes recognition of EBV products may mediate protective immunity against EBV-associated NPC. Moreover, as the studies included in our meta-analysis were characterized by different baseline patient characteristics (such as age, tumor stage, and treatment regimen), sample size, follow-up time, scoring method, we should cautiously interpret these results.
Furthermore, to clarify the role of TILs location for prognosis, we found that an increase in both intratumoral and stromal TILs was related with improved OS. This was in line with previous cohort studies on ovarian cancer 40 for both TIL sites, and melanoma 41 for intratumoral sites only. However, this partialy contradicts with studies on bladder cancer 14 and ovarian cancer 15 that stromal TILs were reported as statistically insignificant to predict OS.
For subtypes of TILs, although FoxP3+ tregs suppress immunity which might lead to worse prognosis, however, our pooled result indicated that FoxP3+ presence did not show statistical significant for prediction of OS. This might be due to in our included studies, contrasting studies had assessed the FoxP3+ cells which might affect the overall result, and that calls further large study in this area. The other reason might be partly due to the fact that CD4+ co-receptor is also expressed on FoxP3+ tregs. 42 Here, our pooled result showed that higher infiltration of CD4+ cells was related with better OS. This seems CD4+ lymphocytes aid in antitumor activity, either by direct elimination of MHC II+ tumor cells or directly through modulation of tumor the microenvironment. 43,44
Additionally, we investigated that high CD3+ and CD8+ cells infiltration indicated favorable outcome, though the result wasn’t statistical significant. Nonetheless, subgroup analysis of both intratumoral CD3+ and CD8+, but not stromal CD3+, was correlated for predicting favorable prognosis. This might suggest that different CD3+ and/or CD8+ lymphocytes infiltration location has contrasting role within tumor microenvironment in NPC patients. In other words, the different microanatomic localization of TILs in various tumor tissues could have distinct clinical role in determining their correlation to disease prognosis. 41,45,46 Our favorable prognosis result on intratumoral CD8+ infiltration was consistent with previous cohort study on breast cancer, 47 colorectal cancer, 48,49 as well as with the study on ovarian cancer, 15,35 and hepatocellular carcinoma 38 for both intratumoral CD3+ and CD8+ cells. This was in contrast to the study that reported worse DFS to intratumoral CD8+ lymphocytes in breast cancer. 50
Interestingly, in the present study, we found that intratumoral TILs had better OS than stromal TILs in NPC patients. Here, the better prognostic of intratumoral TILs might be due to by the fact that the biological rationale T-lymphocytes activation necessitates physical contact with tumor cells so as to engage the T-lymphocytes receptor. 40,51 More importantly, understanding the biological properties of the suppressed and activated immunophenotypes of intratumoral and stromal TILs in different tumor microenvironment is important to in order to rationally modulate their behavior to enhance antitumor immunity.
There were certain limitations that must be acknowledged. First, patients had received different treatment regimen before and after surgery. Second, due to insufficient data, this study did not evaluate the effect of subtypes of NPC and clinicopathological factors which may determine the prognostic value of TILs. Third, there was also differences in antibody used, cell-scoring criteria and cutoff value in those included studies. Finally, the analysis was exclusively based on studies published in English.
Conclusion
TILs were variably correlated with better prognosis depending on microanatomic location and subsets of TILs in NPC patients. CD4+, intratumoral CD3+ and intartumoral CD8+ lymphocytes could predict favorable patient outcome which suggests that their role in mediating antitumor immune response could potentially be exploited in the treatment of NPC patients. However, in terms of the limitations mentioned before, further well-designed study are needed to confirm our results and highlight the prognostic value of microanatomic location of TILs.
Footnotes
Abbreviations
CI, confidence interval; DFS, disease free survival; EBV, Epstein-Barr virus; HR, hazard ratio; NPC, nasopharyngeal carcinoma; OS, overall survival; TILs, tumor infiltrating lymphocytes.
Authors’ Note
This is meta-analysis that data sources are publicly available, so, no ethical approval was required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by fund by Joint fund of Hubei Health and Family Planning Commission (Number: WJ2018H0018).