
Abstract
Objective:
In this study, by comparing coplanar and noncoplanar intensity-modulated radiation therapy (IMRT) treatment planning in treating tongue cancer, the significance of noncoplanar fields in the protection of the lip and buccal mucosa was determined, and a reasonable solution was selected.
Methods:
Forty-eight tongue cancer patients treated from June 2019 to February 2021 were selected and randomly divided into a coplanar field group and a noncoplanar field group. The mucosal dose limit changed from 15 Gy to 45 Gy for comparison of the two treatment plans. The evaluation indicators (conformal index (CI); homogeneity index (HI); D5, D50, and D98 of the target volume; and the dose of normal tissues) were calculated under different mucosal dose limits. The clinical observation of the lip and buccal mucosa of 48 cases was monitored and graded carefully according to NCI-CTCAE V4.0. Statistical analyses were performed.
Results:
The differences in CI, HI, D98, D50 and D5 between the two groups in the target volume tended to decrease when the mucosal dose limit was less than 30 Gy, with a significant difference (P < 0.05). When the limit exceeded 30 Gy, significant differences in other indicators except CI (P < 0.05) were still noted. In normal tissue, differences in doses between the two groups existed when the mucosal limit was less than 20 Gy, with a significant difference (P < 0.05). When the limit exceeded 20 Gy, no significant difference was noted. Patients in the noncoplanar group showed significantly better results than those in the other group in terms of the radiation-related toxicity of the lip and cheek membrane(P < 0.001).
Conclusions:
Compared with coplanar field radiotherapy, noncoplanar field radiotherapy can effectively reduce the exposure dose to the lip and buccal mucosa. The application of noncoplanar treatment plans exhibits good clinical significance and deserves to be promoted.
Keywords
Introduction
Radiotherapy, which represents an effective management for curing tongue cancer, plays a crucial role in improving the prognosis of patients with the disease. However, the surrounding normal tissue inevitably received various levels of X-ray exposure when the target volume received a lethal dose of irradiation. Oral mucositis, one of the most prevalent side effects resulting from radiotherapy, typically occurs in the oral cavity, throat and pharynx. Approximately all patients with head and neck cancer after radiotherapy and 20%-40% patients receiving chemotherapy will eventually develop oral mucositis. 1,2 The possibility of radiation-related complications is mainly impacted by the exact X-ray dosage. A study showed that oral mucositis may develop into hyperkeratosis upon exposure to 10-20 Gy irradiation 3 with the manifestation of a slight lack of color; mucosal erythema and related pain may appear when the exposure dose exceeds 20 Gy. 4 Once the cumulative radiation dose reaches 30 Gy, the symptoms may become much more severe with the occurrence of mucosal ulcers, which provide an ideal environment for bacterial growth. 4 In clinical practice, the distance from the target volume area of tongue cancer to the lip and buccal mucosa is approximately 0.5 cm on average, whereas the mean dosage of mucous membrane in the oral cavity is 40 Gy. Given that radiotherapy-related side effects are inevitable, how to lower the exposure dose and alleviate painful symptoms for patients are the main clinical concerns and popular topics. This study employed the noncoplanar radiation field method, which added 2 vertical sagittal fields on the basis of 7 equal fields. The technique optimizes the angle of the radiation field to decrease the exposure doses by making the central axis of the radiation field tangent to the region of the mucous membrane. This study was approved by the ethics committee of Shanghai Ninth People’s Hospital.
Patients and Methods
Patient Characteristics
We collected 48 cases (age from 34 to 78 with median age 56.9, 28 males and 20 females) with tongue cancer ranging from stage T2-4, any N, M0 who underwent radiotherapy after surgery between June 2019 and February 2021 at the Department of Oral Maxillofacial Head and Neck Oncology at the Shanghai Ninth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine. All patients underwent simultaneous glossectomy and rehabilitation of the primary tongue tumor. Then, the pathological features indicated squamous cell carcinoma as noted by experienced pathologists after the operation. No residual tumor or positive margins were recorded on the pathological reports. Postoperative radiotherapies were arranged according to clinical guidelines. Patients were excluded if concurrent comprehensive therapies (chemoradiotherapy, targeted therapy and immunotherapy) were planned, previous surgeries or radiation treatments for head and neck cancer were performed, or the patient has a history of tumor elsewhere in the body in the past 5 years. This study was approved by the Ethical Committee of the institution, and informed consent was obtained from all cases included.
Methods
Scout scan
The patient was fixed with a foam mat and mask for a scout scan by CT (GE, USA). The positioning center was placed in the central region of the tongue. The CT imaging covers from the top of head to subclavian.
Target volume contouring
The scout CT images were transmitted to the Monaco treatment planning system (ELEKTA, Sweden) and fused with contrast-enhanced MRI imaging. Physicians contoured the target area based on the fused images, pathological features postoperatively and other high-risk characteristics. The final contouring targets were confirmed by 2 experienced physicians of radiation oncology. The radiation dose of the target area was normally 60 Gy.
Treatment planning
Radiation planning is determined by both the target volume above and dose limitation of surrounding normal tissue. Normal tissue and organs include the spinal cord, throat, bilateral parotid gland, pharyngeal constrictor and oral mucosa (including the lip and upper and lower buccal mucosae). The treatment planning of the oral cavity mucous membrane adopted a serial function with a radiation dose between 15-45 Gy and 5 Gy per interval. The function of other tissues remained the same, and the calculation method took normal tissue as a priority. All 48 cases were randomly divided into a coplanar field group and a noncoplanar field group with 24 patients each. The former group used 9 fields on average, whereas the latter group adopted 7 fields simultaneously with 2 other fields that required turning the bed 270 degrees to make the angle of radiation rays tangent to the region of the mucous membrane. Every field control points were set 20. With the other dose-limitation function of surrounding tissue unchanged, different calculating data were produced according to the changes of function on oral membrane. Otherwise, one plan was determined without any mucous membrane function. After the calculation procedure was completed, all the radiation doses were integrated as the prescription dose included a 95% target volume. Each patient in the 2 groups underwent a calculation process 8 times, and the corresponding functions were as follows: 15 Gy, 20 Gy, 25 Gy, 30 Gy, 35 Gy, 40 Gy, 45 Gy and no limitation.
Comparison of plans
To investigate the treatment plans above and calculate the results of normal tissue, the evaluation indicators included conformal index (CI), homogeneity index (HI), D5, D50, and D98. The conformal index was calculated from CI=VPTV × VTV/TV2 PV to determine the extent of the prescription dosage covering the target volume. Here, VPTV indicates the volume of PTV, VTV indicates the total volume of prescription isodose curve coverage, and TVPV means the exact volume of PTV covered by VTV. The lower the CI, the better the conformity of the target dosage is. The homogeneity index equals D5%/D95%, and D5% and D95% indicate the minimum dose of 5% and 95% target volumes, respectively. The lower the HI, the better the homogeneity.
Clinical follow-up
The 48 patients were strictly monitored during the radiotherapy process to assess radiation-related side effects of the oral cavity, especially the lip and buccal mucosa. The patients were regularly checked by 2 physicians every week during the 6-week treatment period, and accurate clinical manifestations were precisely recorded, classified and graded using the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events, version 4.03 (CTCAE, v. 4.03). Finally, the grades of the manifestations of lip and buccal mucositis after 6 weeks of radiotherapy were managed by statistical analysis for the comparison between the 2 groups.
Statistics
The results were analyzed using SPSS 18.0, and measurement data with a normal distribution are expressed as X±S. The mean between groups was analyzed by paired t test, whereas the nonnormal distribution was investigated by nonparametric test. The classification of lip and cheek mucositis grades between the 2 groups was compared by the rank sum test (Mann-Whitney U test). The test level was α = 0.05.
Results
Comparison of Dosages Between Coplanar Fields and Noncoplanar Fields With a Dose Limit of 20 Gy on the Oral Membrane
As shown in Figure 1, the left panel (1A) shows transverse and sagittal imaging of the coplanar field, and the right panel (1B) shows the noncoplanar field of the same patient (Figure 1). The principle of the noncoplanar radiation field underscores the notion that the angle of the X-ray should be tangent to the region of the mucous membrane for protection purposes.

The left and right images are the corresponding transverse and sagittal images of the coplanar field (A) and noncoplanar field (B) of the same patient. The red line represents the dose line, the yellow line represents the target volume, and the blue line contours the area of the lip and cheek membrane.
The Results of 2 Treatment Plans Under Different Dose Limitations of the Oral Membrane
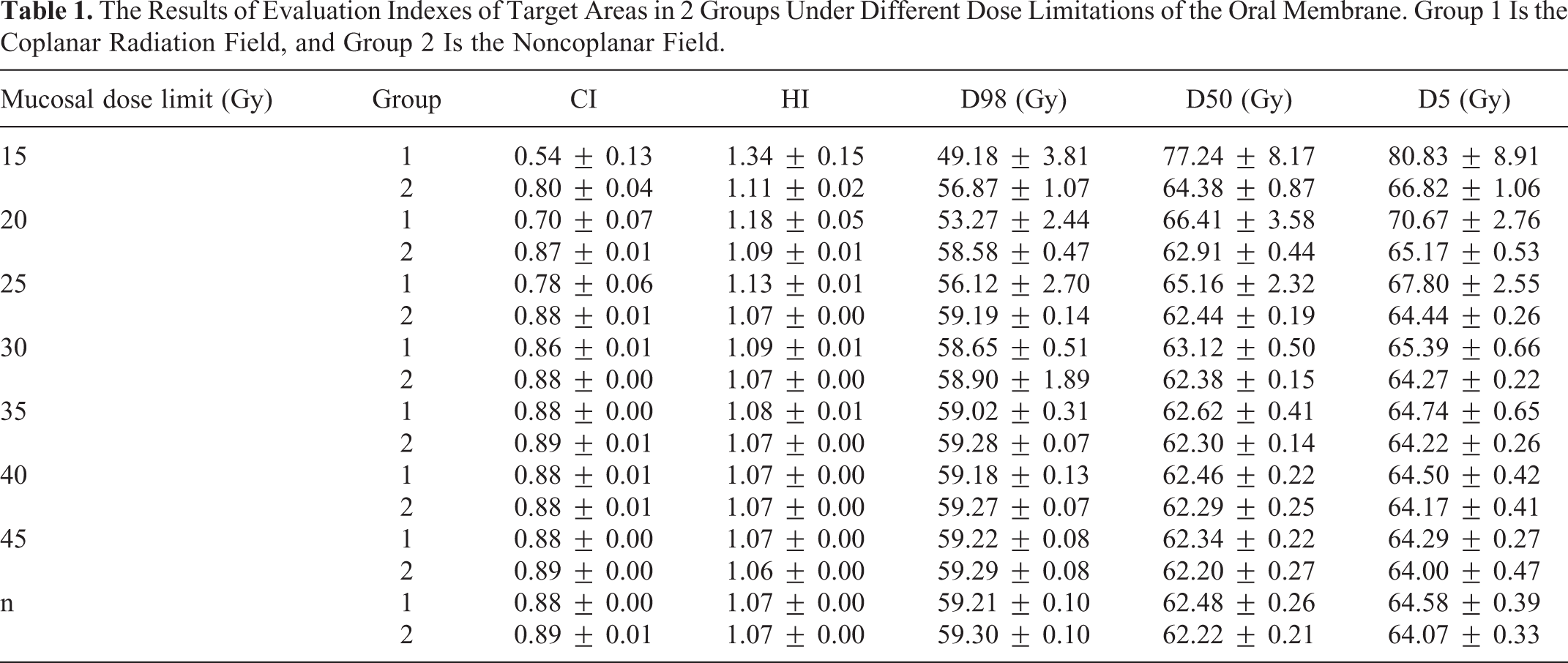
Tables 1 and 2 show the results of evaluation indexes of the target areas and normal tissues in 2 different treatment methods when the mucosal dose limit changed from 15 to 45 Gy or without limitations. Figures 2 and 3 present the bar chart, line chart and curves obtained according to the above data. For the target area, when the membrane dose limit increased from 15 to 30 Gy, the difference in the evaluation indicators, including CI, HI, D50, D98 and D5, between the 2 groups tended to gradually decrease. However, when the limit exceeded 30 Gy or there was no dose limitation, minimal differences were noted. In terms of normal tissue, a gap between the effect of doses on normal tissues exists between 2 groups when the mucosal limit was less than 20 Gy but is gradually reduced. However, when the limiting dose exceeds 20 Gy or there is no dose limitation, the difference in doses between the 2 methods is not statistically significant. The curve of monitor unit (MU) in the 2 groups indicates that the lower the mucosal dose limit, the greater the gap of MU between coplanar and noncoplanar fields, and the lower the energy utilization efficiency of the coplanar field treatment plan. When the limit exceeds 25 Gy, the difference between the 2 methods is minimal, and the noncoplanar field seems to have a certain advantage.
The Results of Evaluation Indexes of Target Areas in 2 Groups Under Different Dose Limitations of the Oral Membrane. Group 1 Is the Coplanar Radiation Field, and Group 2 Is the Noncoplanar Field.
The Dose Results on Normal Tissues in 2 Groups Under Different Dose Limitations of the Oral Membrane. Group 1 Is the Coplanar Radiation Field, and Group 2 Is the Noncoplanar Field.


The bar chart shows the results of D98, D50 and D5 of the target areas between the coplanar field and noncoplanar field under different mucosal dose limits. The curve shows the CI and HI results of the target areas between the coplanar field and noncoplanar field under different mucosal dose limits. The X-axis is the dose limitation of oral mucosa. The left-Y axis is the radiation dose, and the right Y-axis is the index rate.

The line chart shows the results of D98, D50 and D5 of the normal tissues between the coplanar field and noncoplanar field under different mucosal dose limits. The curve shows the MU of the treatment plan between the coplanar field and noncoplanar field under different mucosal dose limits. The X-axis is the dose limitation of oral mucosa. The left Y-axis is the radiation dose, and the right Y-axis is the MU.
Statistical Analysis of 2 Treatment Plans Under Different Mucosal Function Settings
Table 3 shows that there were significant differences (P < 0.05) in D98, D50, D5, CI and HI of the target area between the 2 groups when the mucosal function setting was less than 30 Gy. When the mucosal function setting exceeded 30 Gy, there was no significant difference in CI, but significant differences in the other settings were noted (P < 0.05). In normal tissue, there was a significant difference (P < 0.05) between the 2 treatment plans when the mucosal function setting was less than 20 Gy. If the dose exceeded 20 Gy, no significant difference was noted.
The Statistical Results of 2 Treatment Plans Under Different Mucosal Function Settings.

Clinical Manifestations of the Lip/Cheek Membrane During Radiotherapy
Radiation-related toxicity includes difficulty swallowing, pain with swallowing, decreased appetite, dry mouth, hoarse voice, pain, mouth or throat sores, nausea, vomiting, pain in the mouth or throat, cough, skin burns from radiation, skin cracking at the mouth, and increased phlegm. Given that the tongue and mouth floor were all included in the target volumes, the presentation of mucositis was observed on the tongue and mouth floor in all included cases. Nevertheless, the manifestation of mucositis on the lip and cheek membrane differed between the 2 groups.
In the noncoplanar field group, the incidence rate and classification of severity were considerably lower than those in the other group. Patients typically developed lip and buccal mucositis after the fourth week during radiotherapy, and symptoms of most cases were classified as mild. After all the patients completed their radiotherapy treatments, the manifestations of lip and buccal mucositis were recorded and graded according to NCI-CTCAE V4.0. The statistical analysis of the data revealed significant differences (P < 0.001) between the 2 groups. In the coplanar group, 5 patients developed grade II lip and buccal mucositis; grade III toxicity occurred in the other 19 patients. In the noncoplanar group, the manifestations of the symptoms were mild or moderate. Classifications of 21 cases ranked grade I, whereas the remaining 3 ranked grade III. No grade IV side effects were reported in either group with the application of mouthwash and antibiotics (Table 4).
Cases of Lip and Cheek Mucositis in the Coplanar Field Group and the Noncoplanar Field Group.

Discussion
When rotating the treatment bed, the central axis of each radiation field is not in the same plane, and multiangle and multiradian irradiations in geometric space are realized with the noncoplanar field technique. 5 Irradiation of the noncoplanar field has been effectively applied among different kinds of tumor radiotherapy treatments. Panet-Raymond et al 6 found that in radiotherapy for frontotemporal high-grade glioma invading the optic path, the noncoplanar technique can reduce equivalent uniform doses of the contralateral anterior globe, temporal lobe and retina. However, superior sparing of contralateral optic organs was also achieved. Park et al 7 suggested that the dose delivered to parotid glands and lenses could be reduced with the aid of a noncoplanar field in whole-brain radiotherapy. Kim et al 8 discovered that noncoplanar partial arc volumetric-modulated arc therapy(VMAT) exhibited more favorable plan quality than coplanar VMAT in stereotactic ablative radiotherapy of lung cancer tumors located close to the heart.
Different intensity-modulated techniques produce different dose distributions because of various X-ray fields and incident angles. 9 The advantage of the noncoplanar field is that radiation rays can reach the target area via a much shorter distance or avoid normal tissue with adequate dose exposure of the target area. This is considered the ideal method to optimize the incident angle of X-rays, which optimizes the beam path as the ultimate purpose. 5
The appearance of radiation-related oral mucositis is due to the target volume covering the oral cavity area. 10,11 X-rays interfere with the normal physiological function of the mucous membrane and salivary gland, which decreases the production of saliva and oral self-cleaning ability in addition to hyperemia and edema of the membrane in the irradiation field. 12 Li et al 10 concluded from the clinical analysis that V30Gy was the determining factor for inducing severe radiation-related oral mucositis.
Different irradiation volumes and mucosal limits have a significant impact on the severity of radiation oral mucositis. 13,14 Trotti et al 15 found that patients with head and neck cancer receiving altered fractionation radiotherapy presented severe mucositis compared to those prescribed conventional radiotherapy. This study aims to reduce the radiation dose to the oral membrane in patients, especially the lip and buccal mucosa. For tongue cancer patients, the membrane of the lip and cheek is located at the lateral margin near the target area of the tumor bed. In the radiotherapy plan of the coplanar field, greater than half of the incident angles near the membrane must pass through membrane tissue before reaching the target volume. During the optimization process, to meet the prescription dose of the target volume, it is inevitable for TPS to increase the weight of this incident angle, leaving the oral cavity membrane unprotected. In contrast, with the recruitment of the noncoplanar field, the problem could be resolved to some extent. The X-ray path is tangent to the mucosal tissue, which guarantees an adequate radiation dose to the target area and keeps membrane tissue away from exposure. The same result is concluded from our study analysis. When the dose limitation of the membrane is set to less than 20 Gy, there is an obvious advantage of the plans using a noncoplanar field for both normal tissue and the target volume. Significant differences (P < 0.05) were found compared with the coplanar field, and all the parameters conformed to the regulation of IMRT treatment in the clinic. In the IMRT plans of 9 radiation fields, the control of hot and cold spots in the target volume does not satisfy the clinical standard, and the dose of the normal tissue also highly surpasses the RTOG limitations. However, along with the increase in dose limitation on the membrane, the gap in IMRT plan quality between the noncoplanar field and 9 normal fields is narrowed. Specifically, the advantage of the noncoplanar field on the target area still exists but is not obvious. This fact indicates that the 9-field plan could complete the modulation of the IMRT plan effectively under this mucosal dose limit, and there is no indispensable request to use a noncoplanar angle when considering facilitating clinical practice.
In reality, if the noncoplanar field technique is performed in the IMRT plan, multiple fields from different angles could only be achieved with precise cooperation between the treatment bed and gantry. Given that this method further increases the higher demand for quality control accuracy and positioning by technicians, a noncoplanar field is not recommended when presenting the same effect of tissue protection. Furthermore, the inflammation severity of oral cavity membrane tissue, as the second type of protective organ, was influenced by multiple factors, including the application of chemotherapy, sanitary condition of the oral cavity and patients’ physical status. Physicians and physicists should take reality into account. On one hand, the noncoplanar field technique can be adopted in the IMRT plan. On the other hand, individualized and personalized therapy should be proposed to a single patient with the consideration of feasibility and optimization.
Footnotes
Authors' Note
This study was approved by the Ethics Committee of Shanghai Ninth People’s Hospital (SH9H-2021-T78-2).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.