
Abstract
Background:
There are very few studies on noncoplanar radiation in tomotherapy because deformable image registration is not implemented in the TomoTherapy Planning Station, a treatment planning device used in tomotherapy. This study examined whether noncoplanar radiation can be performed on the head using a tilt-type head and neck fixture and deformable image registration.
Methods:
Planning target volume spheres with diameters of 2, 3, and 4 cm were set on a head phantom, and computed tomography images were taken at 0° and 40° using a tilt-type head and neck fixture. Irradiation plans were created in the Tomotherapy Planning Station. Noncoplanar radiation was simulated, and the dose volume was evaluated by adding the 0° dose distribution and 40° dose distribution using the deformable image registration of the RayStation treatment planning system.
Results:
The ratio of the phantom volume to the irradiation dose for 20% to 30% of the planning target volume in noncoplanar radiation was smaller than that for 40% to 90% of the planning target volume in single-section irradiation at 0° or 40°.
Conclusions:
Noncoplanar radiation on the head region using tomotherapy was possible by using a tilt-type head and neck fixture, and the dose distribution could be evaluated using deformable image registration. This method helps reduce the dose of the organ-at-risk region located slightly away from the planning target volume.
Keywords
Introduction
Stereotactic irradiation (STI) is a method of focusing well-defined radiations on specific targets in the brain and may consist of stereotactic radiosurgery (SRS), which delivers one large dose of radiation, and stereotactic radiotherapy (SRT), which involves a course of multiple radiations. Generally, SRS is selected for Gamma Knife, which uses highly focused radiation treatments, while both SRS and SRT are individually selected for Cyber Knife, a robotic radiotherapy system, and linear accelerator, a medical linear accelerator for external beam radiation treatments. In tomotherapy, the positioning accuracy of STI can be guaranteed using megavoltage computed tomography (CT), but the dose distribution of STI is wider than that of Gamma Knife or CyberKnife. 1,2 Tomotherapy is a special modality for coplanar irradiation in which the gantry of the device performs a fixed helical irradiation, so that irradiation is performed on the axial section during the planned CT. This technique causes the dose distribution to spread out of the planning target volume (PTV), in contrast to STI devices, such as Gamma Knife and Cyber Knife, which irradiate from hundreds or more directions. Since the dose around the PTV is higher in tomotherapy than in Gamma Knife or CyberKnife, hair loss among other uncommon side effects is likely to occur. It is known that the smaller the earlier reaction/late reaction (α/β) and the larger the single dose, the more easily brain cells are affected.
In the Tomotherapy Planning Station (TPS), a treatment planning device used in tomotherapy, treatment plans using 2 CT images cannot be added. However, in recent years, the concept of deformable image registration (DIR) has been implemented in various treatment planning devices. 3 Deformable image registration generates a vector for moving each pixel of the deformed image to a corresponding pixel position in the target image, transforming the deformed image to match the target image. This technique allows the summation of 2 or more doses calculated for the same patient.
In head irradiation, the head is usually fixed using a setup that allows the patient to easily sleep. However, if necessary, a tilt-type head and neck fixture for radiation treatment may be used to lower the chin while irradiating the patient. Using this method, it is thought that noncoplanar radiation (NCR) is also possible in tomotherapy, but there are only a handful of basic studies on NCR in tomotherapy. 4 Here, we performed a basic study of NCR in tomotherapy using DIR and a head and neck fixture with a tilting mechanism.
Materials and Methods
Materials
Radiotherapy equipment: TomoHDA (Accuray Incorporated)
Radiotherapy planning equipment: TPS (Accuray Incorporated)
DIR software: RayStation (DIR algorithm: Hybrid intensity and structure based, Ray Research Laboratories)
Tilt-type head and neck fixture for radiotherapy: MT2013CF with a carbon fiber tilting baseplate (CIVCO Radiotherapy)
Treatment planning CT: Aquarion LB (Toshiba)
Phantom for head radiotherapy (volume, 4264 mL)
Methods
The head phantom was fixed to the head and neck fixture using the following conditions: At a tilt angle of 0° At a tilt angle of 40°
Under each of the conditions (A and B), the treatment plan CT images were taken with a slice thickness of 1 mm. A spherical PTV with a diameter of 2, 3, or 4 cm was created in the sella turcica, and treatment planning was performed with CT of A and B using TPS. The irradiation conditions were as follows: PTV dose covering 95% of the volume (D 95), 7 Gy; no organ-at-risk (OAR) setting; jaw size, 2.5 cm; modulation factor, 1.5; and plan calculation grid, 0.25 × 0.25 cm.
The dose distributions of A and B were then transferred to the RayStation. Noncoplanar radiation was simulated, and the dose distribution of B was subjected to DIR based on the CT of A. Hence, the following methods applied:
Method 1. Dose distribution of A × 2
Method 2. Dose distribution of B × 2
Method 3 (NCR). Dose distribution of A + dose distribution of B
(D 95 was considered to be at 14 Gy under all conditions.)
The phantom volume was calculated at 10%, 20%, 30% to 90% of the PTV D 95.
Results
Figure 1 shows the DIR results (2-cm PTV sphere) in the RayStation. We discovered that the RayStation could evaluate 2 different CT images that TPS alone could not.

Dose distribution map at a tilt angle of 0° (A). Deformable image registration was performed on the dose distribution map of the computed tomography image with a tilt angle of 40° (B) and that with a tilt angle of 0° (C). (D) is a 1:1 comparison between the dose distribution maps of (A) and (C). All images were for 2-cm spheres of planning target volume.
Table 1 presents the ratio of the phantom volume to the irradiation dose. Regardless of the diameter of the PTV, at 40% to 90% of the dose volume, the ratios did not differ significantly between the 3 methods. However, NCR excelled except for 60% to 90% of the 3-cm PTV sphere. Moreover, the superiority of NCR at 20% to 30% of the dose volume was clear, and the ratio for 20% of the 4-cm PTV sphere was 15.04 with NCR (method 3) compared with 20.27 with 40° 1-sided irradiation (method 2). The irradiation volume was also smaller for ≥5% of the dose volume.
Ratio of the Phantom Volume to the Irradiation Dose.
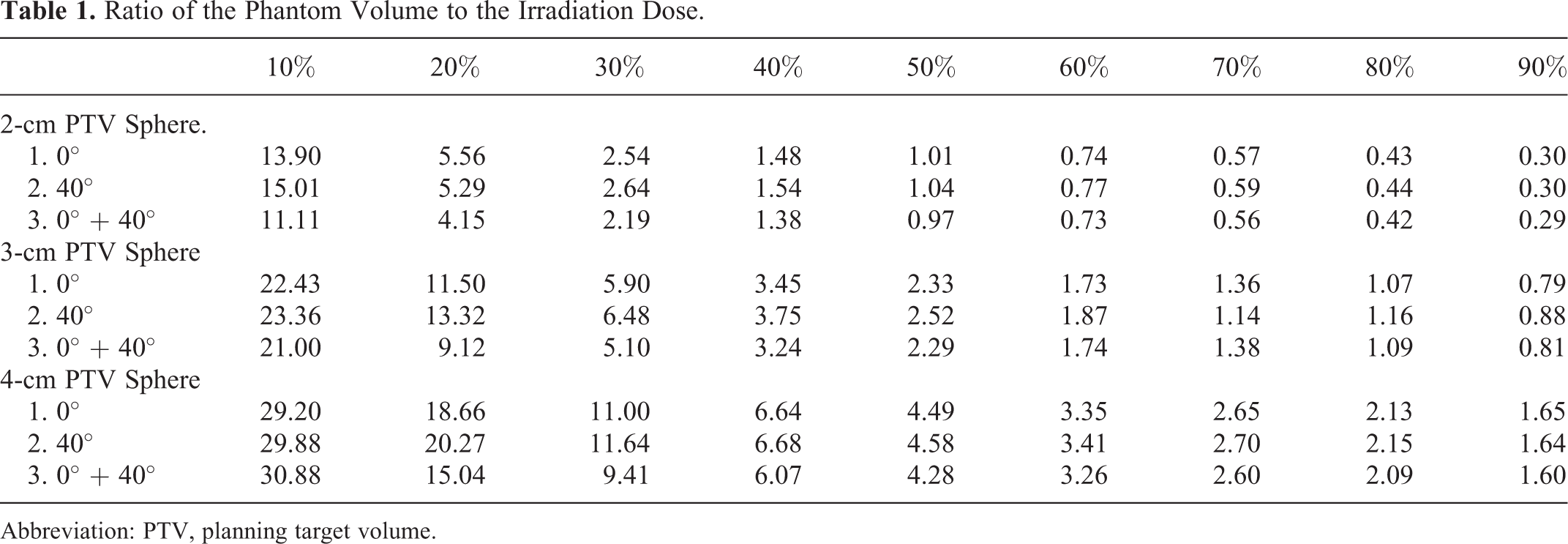
Abbreviation: PTV, planning target volume.
Table 2 shows the dose distribution under each condition. CI = V95/VPTV, HI = (D 2-D 98)/D 50 according to ICRU83, D 99, D average, D 1, and dose of sphere center. In method 3, none of outcomes were poor compared to the ones from method 1 and 2.
Details of Dose Parameter (D 95 = 14 Gy).
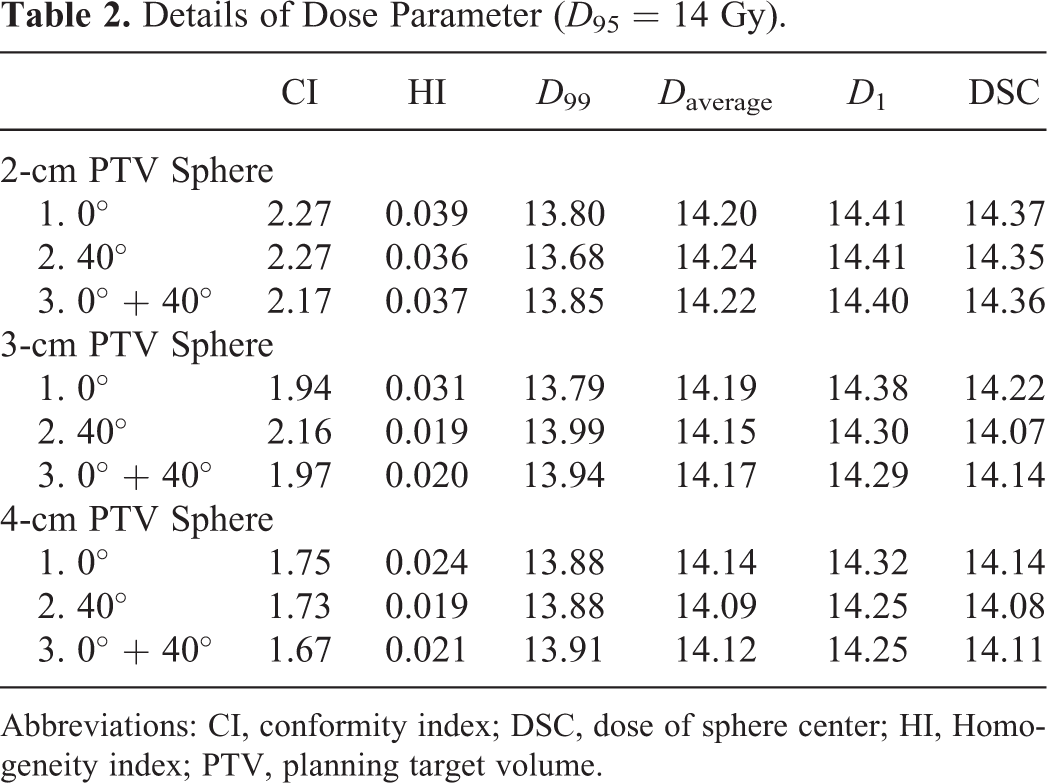
Abbreviations: CI, conformity index; DSC, dose of sphere center; HI, Homogeneity index; PTV, planning target volume.
Discussion
Unlike image fusion, a conventional process of displaying images superimposed on each other by parallel and linear movements of rotation, DIR is an image processing technique that transforms one image set with respect to a reference image set and combines them in voxel units. According to the amount of displacement between images calculated in voxel units by DIR, it becomes possible to compare and evaluate the temporal accumulation of the dose over multiple image sets and the dose during the treatment planning. This is carried out by transforming the contour information of organs and targets depicted on the CT image used to create the treatment plan or by transforming the dose distribution results calculated on other images into a CT image used to create the treatment plan. This is a core technology that is essential for making 4D treatment planning and adaptive planning more realistic. However, since the TPS used in tomotherapy does not implement image fusion and DIR, a software with DIR function is required to add the dose distribution maps obtained from 2 CT images. In this study, the Ray Station was not only capable of deforming the cumulative dose into a new image and imprinting it. 5 It also had a function that allowed movement to the treatment adaptation tool without performing complicated operations and that allowed smoothly adapting the treatment plan, as has been shown in a study that conducted a comparative evaluation of the cumulative dose and the initial planned dose through the dose tracking function. 6
As seen in Table 2, Tomotherapy can provide a better CI or HI than Gamma Knife and Cyber Knife, but it is associated with a wider spread of low-dose radiation. 1,2 Recently, most physicians use various techniques, such as STI, NCR, and volumetric modulated arc therapy, to improve dose distribution around the target. 7 However, there is a concern that the irradiation field may cover many normal tissues, resulting in an increase in the volume of exposed normal tissues and an increase in the amount of exposure due to an increase in the monitor unit value. 8 Jo et al suggested that low-dose lung irradiation in hypofractionated tomotherapy is a risk factor for metastatic lung cancer and that the percentage of lung volume with a dose exceeding 5 Gy (V5) should be <65% to prevent clinical radiation pneumonitis. 9
There are only a handful of studies on NCR in tomotherapy. Our study shows that on NCR using a tilting mechanism, NCR showed a slightly better ratio of the phantom volume to the irradiation dose for 40% to 90% of the 2- to 4-cm PTV sphere than one-plane irradiation did. In addition, our study showed that the ratio for 20% to 30% of the dose volume was clearly lower with NCR than with one-plane irradiation. Considering that NCR with a tilting mechanism is effective in reducing the dose in the OAR region located slightly away from the PTV, there are 2 major clinical benefits: First, compared with ordinary tomotherapy irradiation, which only limits the dose to OARs if present in the irradiated volume, NCR also allows the dose to be delivered to another section. For example, even if the hippocampus enters the irradiation field at a certain slice, NCR may be able to positively reduce the hippocampal dose and protect cognitive function. This may be useful not only in STI but also in IMRT of primary brain tumors. Radiation dose to the IMRT is lower compared to the STI, and considered to be a biological advantage when using NCR. However, due to the IMRT irradiation count the effort required will be a problem.
Second, NCR can prevent hair loss, which is often observed in STI using tomotherapy. Temporary hair loss generally occurs with a single dose of 2 to 5 Gy. 10,11 Since irradiation is performed in 2 sections in NCR, it is possible to reduce the skin dose to a level that does not cause hair loss.
In conclusion, this study revealed that NCR using tomotherapy could be performed on the head region using a tilt-type head and neck fixture and the dose distribution could be evaluated using DIR. With this method, the ratio of the phantom volume to the irradiation dose was lower in 20% to 30% of the PTV, and the dose of OARs placed slightly away from the PTV was reduced.
Footnotes
Authors’ Note
Our study did not require an ethical board approval because it did not contain human or animal trials.
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.