
Abstract
Background
The incorporation of noncoplanar beam arrangements has been proposed in liver radiotherapy modalities, which can reduce the dose in normal tissues compared to coplanar techniques. Noncoplanar radiotherapy techniques for hepatocellular carcinoma treatment based on the Linac design have a limited effective arc angle to avoid collisions.
Purpose
To propose a novel noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system and investigate its performance in hepatocellular carcinoma patients.
Methods
The computed tomography was deflected 90° to meet the structure of a cage-like radiotherapy system and design the noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system plan in the Pinnacle3 planning system. An noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system plan was customized for each of 10 included hepatocellular carcinoma patients, with 6 dual arcs ranging from −30° to 30°. Six couch angles were set with an interval of 36° and distributed along with the longest diameter of planning target volume. The dosimetric parameters of noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system plan were compared with the noncoplanar volumetric modulated arc therapy and volumetric modulated arc therapy plan.
Results
The 3 radiotherapy techniques regarding planning target volume were statistically different for D98%, D2%, conformity index, and homogeneity index with χ2 = 9.692, 14.600, 8.600, and 12.600, and P = .008, .001, .014, and .002, respectively. Further multiple comparisons revealed that noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system significantly reduced the mean dose (P = .005) and V5 (P = .005) of the normal liver, the mean dose (P = .005) of the stomach, and V30 (P = .028) of the lung compared to noncoplanar volumetric modulated arc therapy. Noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system significantly reduced the mean dose (P = .005) and V5 (P = .005) of the normal liver, the mean dose (P = .017) of the spinal cord, V50 (P = .043) of the duodenum, the maximum dose (P = .007) of the esophagus, and V30 (P = .047) of the whole lung compared to volumetric modulated arc therapy. The results indicate that noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system protects the normal liver, stomach, and lung better than noncoplanar volumetric modulated arc therapy and protects the normal liver, spinal cord, duodenum, esophagus, and lung better than volumetric modulated arc therapy.
Conclusions
The noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system technique with the arrangement of noncoplanar arcs provided optimal dosimetric gains compared with noncoplanar volumetric modulated arc therapy and volumetric modulated arc therapy, except for the heart. Noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system should be considered in more clinically challenging cases.
Introduction
Hepatocellular carcinoma (HCC), or liver cancer, is the sixth most common cancer worldwide and the third leading cause of cancer deaths in the world in 2020 1 according to a report by the International Agency for Research on Cancer. 2 Surgical resection is generally regarded as the primary treatment for HCC and has demonstrated effective results. 3 However, for selected HCC patients with surgical contraindications and inoperable tumors, radiotherapy could be an effective treatment choice. 4
With advances in radiotherapy modalities, 3-dimensional conformal radiotherapy can accurately irradiate the target volume while limiting radiation to the healthy liver, perhaps prolonging the lives of some HCC patients.3,5 Intensity-modulated radiotherapy (IMRT) has the ability to generate complicated spatial dose distributions for HCC patients that conform more closely to the target volume while sparing critical organs by employing an inverse planning algorithm.6–11 Volumetric modulated arc therapy (VMAT), the newest form of IMRT, can improve the time efficiency of dose delivery and deliver more conformal dose distributions to HCC patients by changing treatment apertures (dynamic multiple leaf collimators) as well as providing a modulated dose rate.12–14 Recently, the incorporation of noncoplanar beam arrangements has been proposed in liver radiotherapy modalities, which can reduce the dose in normal tissues compared to coplanar techniques. de Pooter et al proved that IMRT with optimized noncoplanar configurations led to the best sparing of organs at risk (OAR) (healthy liver, spinal cord, and bowel). 15 Hsieh et al proposed that noncoplanar IMRT was a potentially effective radiotherapy technique for HCC patients. 16 Dong et al demonstrated that the noncoplanar radiation delivery technique significantly improved dose gradient, reduced high-dose spillage, and improved OAR sparing compared with state-of-the-art VMAT plans. Thibault et al demonstrated that a combination of coplanar full and noncoplanar partial arc in liver VMAT radiotherapy was sufficient for HCC patients. 17 Sharfo et al demonstrated that noncoplanar VMAT (N-VMAT) could reduce the dose received by healthy liver volumes. 12 Lin et al 18 considered that N-VMAT could improve OAR sparing more than VMAT, with only a small and acceptable increase in delivery time. 19
However, to avoid collisions, noncoplanar radiotherapy techniques for HCC treatment based on the C-arm linear accelerator (C-Linac) design have a limited effective arc angle and significantly increased treatment time, which does not reflect the benefits of noncoplanar radiotherapy techniques. Niu et al designed a cage-like radiotherapy system (CRTS) to further promote the clinical application of noncoplanar radiotherapy. 20 The CRTS comprises 2 stands, 2 O-rings, several arc girders, an X-ray head, an imaging subsystem, and a treatment couch. 20 The X-ray head moves along with the arc girder and rotates using O-rings around the patient's body. In addition, the CRTS enabled precise noncoplanar irradiation without movement of the patient body, automated control of the motions of different parts without the risk of collisions, and continuous radiation across an angle far greater than a full turn.
This study aimed to design a novel noncoplanar radiotherapy technique based on the CRTS (N-VMAT-Cage) and investigate its performance in HCC patients. N-VMAT and VMAT plans based on the C-Linac were designed for comparison.
Materials and Methods
Patient Data
Ten patients with HCC (8 men and 2 women) were selected from our institution between July and November 2021. The prescription dose was 44 to 50 Gy. All plans were normalized to deliver 100% of the prescribed dose to 95% of the planning target volume (PTV). The PTV ranged from 533.13 to 2609.47 cc, and the healthy liver volume, defined as the total liver minus gross tumor volume (Liver-GTV), ranged from 506.18 to 1412.35 cc (see Table 1). The mean patient age was 55 (range, 47-76) years. Planning computed tomography (CT) data were acquired using a CT scanner (Sensation Open, Siemens Healthineers) using 1.3-mm thick slices. A 4-dimensional CT image set was acquired. Details of baseline characteristics of the patients and tumors are listed in Table 1. Our institution does not require ethical approval for reporting individual cases or case series. For this study, anonymized patient data were used. According to our local ethics committee, this does not require ethics approval. This study was a retrospective randomized study.
Patient Characteristics for the Treatment Techniques Being Studied.

Abbreviations: ECOG, Eastern Cooperative Oncology Group; PTV, planning target volume; GTV, gross tumor volume.
Treatment Planning
All plans were designed using the Pinnacle 3 treatment planning system (version 16.2, Philips Healthcare) with Collapsed Cone Convolution Superposition algorithm and delivered using an Elekta Versa HD accelerator (Elekta Oncology Systems). All plans used 6-MV FFF X-rays and were calculated on a dose grid with 4-mm3 voxels using a collapsed cone convolution algorithm. The prescribed dose was 2 Gy delivered per fraction for all patients.
Noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system
The structure of CRTS is somewhat similar to the Tomotherapy machine (Accuray). 21 The gantry of CRTS is mainly composed of several arc girders that stretch across the O-rings at −45° to 45° of rotation and rotate around the longitudinal axis that passes through the isocenter. The details of the structure of CRTS were shown in Appendix. In the Pinnacle 3 TPS (version 16.3), a CT deflection of 90° was needed to meet the gantry of CRTS. Then, the N-VMAT-Cage plan was designed in TPS by rotating the couch and gantry. Deflection CT was mainly divided into 5 steps: (1) Export CT DICOM image from TPS; (2) Open the exported DICOM image using Image J software (Image J 1.50v, NIH) and use the “Transform J Rotate” command to deflect 90°; (3) Export the deflected image, with a raw format; (4) Use the program simulated in MATLAB (R2020b, Mathworks, Inc.) to convert the format to DICOM; and (5) Import DICOM images into the Pinnacle planning system, deflect CT images to re-register, replicate regions of interest, and design the N-VMAT-Cage plans. Moreover, the gantry of CRTS rotating around the longitudinal axis was determined based on the couch rotation (Linac). In this study, 6 couch angles with 60° arcs (6*60° = 360°) were designed to approximately simulate a full arc.
The design of the N-VMAT-Cage plan was primarily divided into 5 steps. Step 1, 90° CT deflection (realize the setting of the CRTS in the TPS) image was imported in the TPS to design an N-VMAT-Cage plan.; Step 2, the gantry angle was initially determined on the transverse slice, and the arc size was −30° to 30° to reduce high doses in OARs; Step 3, the couch angle was selected on the coronal slice, which was distributed along with the longest diameter of the PTV. Six couch angles were set with an interval of 36°, and the couch range was 180° ((6−1) × 36 = 180); Step 4, in the BRV view on the coronal slice (the orientation was Y1/Y2), the gantry angle (arc size was 60°) was finely adjusted to minimize exposure to the OAR (all arcs were dual arcs); Step 5, dosimetric parameters were optimized in the TPS.
Noncoplanar volumetric modulated arc therapy
The design of the N-VMAT plan was primarily divided into 2 steps. Step 1: set 6 couch angles of 30°, 60°, 90°, 330°, 330°, and 360° referring to Yuan et al 22 to better compare with the N-VMAT-Cage, and Step 2: design arc size and ensure that the gantry angle can reach the maximum range without collision (all arcs are dual arcs). To determine the range of the gantry angle with different couch angles, the thermoplastic mask of an HCC patient was buckled on the couch plate of the Elekta Versa HD accelerator (Elekta Oncology Systems). The gantry was rotated at 6 couch angles. The range of the gantry angle without collision between the gantry, couch, or thermoplastic mask is shown in Table 2. All operations conformed to clinical practice.
Range of the Gantry Angle With 6 Couch Angles.

Abbreviation: ACW, anticlockwise.
Volumetric modulated arc therapy
The patients were clinically treated using VMAT plans with either dual coplanar full or dual coplanar partial arcs entering the body proximal to the tumor, depending on the tumor laterality. Five VMAT plans used full arcs, and others used partial arcs.
Planning Evaluation
Several parameters, such as conformity index (CI) and homogeneity index (HI), of PTV were evaluated. CI was based on Paddick's formula
23
:
Regarding OARs, mean dose (Dmean), max dose (Dmax), and volume of structure receiving 5 Gy (V5(cc)) were calculated for the healthy liver (Liver-GTV). In addition, Dmean, Dmax, and percentage of structure volume receiving 20 Gy (V20(%)) for the left kidney (Kidney L) and right kidney (Kidney R); Dmean and Dmax to the cord, cord PRV, and esophagus; Dmean and Dmax to and V50(cc) of the intestine, stomach, and duodenum; Dmean and Dmax to and V52(cc) of the colon; Dmean and Dmax to and V30 (%) and V40 (%) of the heart; and Dmean and Dmax to and V20 (%), V5 (%), and V30 (%) of the entire lung (Lung All) were also evaluated.
Statistical Analysis
The data were analyzed using SPSS 25.0 software. The data from the radiotherapy techniques could not conform to both positive distribution and χ2, so Friedman nonparametric test was used. The descriptive statistics were expressed as median (interquartile spacing) with P < .05. Then the multiple analysis used Wilcoxon paired signed-rank test, with Bonferroni correction P values. A significant level should be P < .0166 as the result with a statistical difference.
Results
Plan Comparison
Table 3 compares the dosimetric parameters of the 3 radiotherapy techniques about PTV and OAR parameters, and the descriptive statistics are presented as median and interquartile spacing. The 3 radiotherapy techniques regarding PTV were statistically different for D98%, D2%, CI and HI with χ2 = 9.692, 14.600, 8.600, and 12.600 and P = .008, .001, .014, and .002, respectively. Further multiple analyses showed that the D98% of N-VMAT was significantly higher than N-VMAT-Cage (P = .009), and the D98% of N-VMAT was significantly higher than VMAT (P = .011). The D2% of N-VMAT-Cage was significantly higher than N-VMAT (P = .013). The D2% of VMAT was significantly higher than N-VMAT-Cage (P = .007). The D2% of VMAT was significantly higher than N-VMAT (P = .005). The CI of N-VMAT was significantly better than VMAT (P = .013). The HI of N-VMAT-Cage was significantly better than N-VMAT (P = .007). The HI of VMAT was better than N-VMAT (P = .005). All other parameters were not statistically different. Overall, the dose parameters of PTV with all 3 radiotherapy techniques meet the clinical requirements, but it might not be possible to clearly compare the advantages and disadvantages.
Summarizes the Dosimetric and Plan Quality Results for All Patients.

Abbreviations: VMAT, volumetric modulated arc therapy; N-VMAT, noncoplanar volumetric modulated arc therapy; N-VMAT-Cage, noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system; PTV, planning target volume; Liver-GTV, liver minus gross tumor volume; CI, conformity index; HI, homogeneity index.
Statistically significant, P < .0166. Q1: first quartile, Q2: median, Q3: third quartile.
The differences in mean dose (χ2 = 15.800, P = .000), and V5 (χ2 = 15.000, P = .001) for Liver-GTV were statistically significant, respectively. Maximum dose for spinal cord (χ2 = 8.600, P = .014) and mean dose for stomach (χ2 = 15.000, P = .001) were statistically significant, respectively. Further multiple comparisons revealed that N-VMAT-Cage significantly reduced the mean dose (P = .005) and V5 (P = .005) of the normal liver, and the mean dose (P = .005) of the stomach compared to N-VMAT. N-VMAT-Cage significantly reduced the mean dose (P = .005) and V5 (P = .005) of the normal liver, V50 (P = .043) of the duodenum, and the maximum dose (P = .007) of the esophagus compared to VMAT. The results indicate that N-VMAT-Cage protects the normal liver, stomach, and lung better than N-VMAT and protects the normal liver, spinal cord, duodenum, esophagus, and lung better than VMAT.
The spread of dosimetric parameters in PTV of the 3 radiotherapy plan moderations is shown in Figure 1. The spread of mean and maximum dose in OAR of the 3 radiotherapy plan moderations relative to plan a prescription dose is shown in Figure 2.

Comparison of the dosimetric parameters of planning target volume (PTV) for the 3 different radiotherapy techniques.
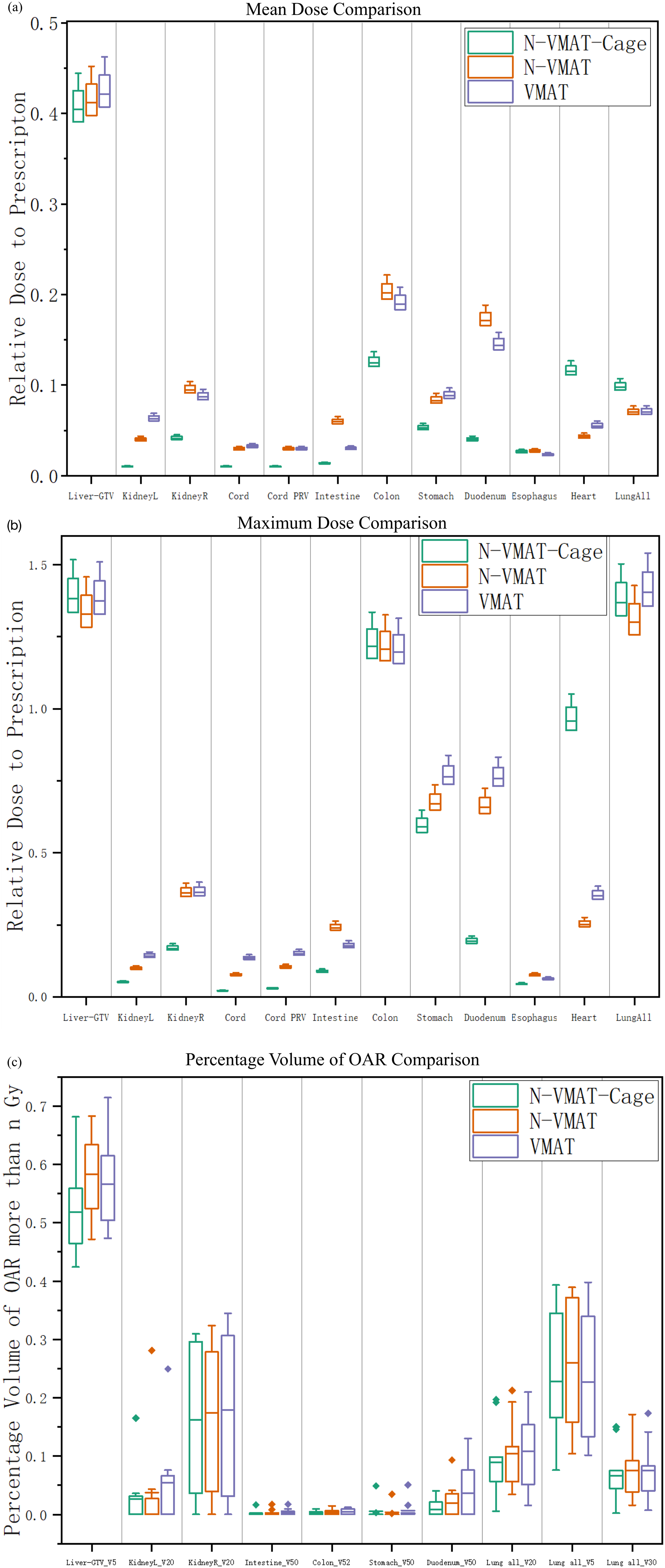
Noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system (N-VMAT-Cage) versus noncoplanar volumetric modulated arc therapy (N-VMAT) and volumetric modulated arc therapy (VMAT) dosimetric comparison, dose relative to the prescription dose (a) Max dose, (b) Mean dose, and (c) V%.
Dose Distribution
The dose distribution and beam arrangement for N-VMAT-Cage, N-VMAT, and VMAT of the representative patient (No.1) are shown in Figure 3. N-VMAT-Cage had the lowest V5 of Liver-GTV compared with N-VMAT and VMAT. The dose–volume histogram (DVH) of the representative patient is shown in Figure 4. These reductions in OAR dose were evident in the DVH.

Dose distribution and beam arrangement for (A) noncoplanar volumetric modulated arc therapy technique based on a cage-like radiotherapy system (N-VMAT-Cage), noncoplanar volumetric modulated arc therapy (N-VMAT), and volumetric modulated arc therapy (VMAT). (A) Transverse, (B) sagittal, (C) coronal slices (color wash: green, planning target volume PTV; red, gross tumor volume GTV).

Dose–volume histograms of planning target volume and organs at risk.
Discussion
In this study, we compared 3 radiotherapy techniques for HCC. Our study showed that the N-VMAT-Cage technique with the arrangement of noncoplanar arcs provided optimal dosimetric gains over the N-VMAT and VMAT techniques. By utilizing more freedom in the noncoplanar beam geometry solution space and beam orientation selection, N-VMAT-Cage achieved dose reductions to OARs, particularly the healthy liver, kidney, cord, colon, esophagus, stomach, and duodenum, as well as a significantly more compact dose distribution. N-VMAT-Cage was optimal in protecting the normal liver, which can reduce the incidence of radiation-induced liver injury and improve the local control and long-term survival rates of liver cancer patients. N-VMAT had advantages over VMAT in protecting the kidney, cord, intestine, stomach, and duodenum. However, the dosimetric advantage of N-VMAT with the finite noncoplanar arc was not obvious to avoid a collision. 25
There is a reason for the limited improvement in plan quality observed when using the N-VMAT technique as opposed to the VMAT technique. It is not guaranteed that arcs between anchoring beams will be optimal when using the N-VMAT technique. Because of the continuity of arcs, the range of favorable noncoplanar angles is restricted to avoid collision.26,27 It has been demonstrated that attempting to put arc angles in a rotational IMRT system that is not in the same plane as each other does not improve the plan. 28 In addition, the N-VMAT technique would simultaneously rotate arcs that need both the couch and gantry, which would be impossible to achieve in existing treatment implementation. 18 Internal organ motions, which may be significantly affected by couch rotation and are certainly more difficult to monitor, are another potential problem irrelevant to the current clinical investigation.
The N-VMAT-Cage technique, where the collision-free beam geometry solution space is individually mapped and the beam orientations are optimized, is an effective method for overcoming these restrictions. Two degrees of freedom are available for translating the X-ray head in the CRTS: it can rotate around as well as slide along with the longitudinal axis of the machine. This allows the body to be irradiated from different directions around the treatment volume as the machine rotates. 20 A patient does not need to be moved at any stage throughout the noncoplanar radiation treatment process. The X-ray head is moved immediately from one noncoplanar radiation position to another without moving the couch. Therefore, the N-VMAT-Cage technique eliminates the collision problem between gantry and couch/patient and internal organ motion caused by rotating the couch. Therefore, even though N-VMAT is currently available, it is not a reasonable substitution for N-VMAT-Cage. Due to the special setting of CRTS, it is convenient to design a noncoplanar plan. However, since the optimization algorithm is still under development, the preliminarily selected noncoplanar optimization trajectory has shown better dosimetric characteristics than VMAT. In the future, with the addition of mature optimization algorithms, caged plans will show better dosimetric characteristics than the present.
The common treatment methods include hepatectomy, liver transplantation, ablation therapy, TACE, radiotherapy, and systemic antitumor therapy. Choosing reasonable treatment methods for patients with different stages of HCC can maximize the therapeutic effect. Due to the deep location of liver, radiation is more damaging to normal liver cells, so radiotherapy is not a routine treatment for patients with liver cancer. However, for some patients with good liver function index, limited tumor, distant metastasis, and not suitable for surgical resection, radiotherapy is also one of the alternative treatments.
Moreover, N-VMAT-Cage demonstrates that the arrangement of noncoplanar arcs helped create safer treatment plans without compromising the PTV coverage. Our study was applicable to the Pinnacle 16.3 platform with 6-MV FFF photon beams and single liver lesions. There is a wide range of potential N-VMAT arc configurations examined for HCC, which is a significant strength of this work. Finally, we would like to highlight that our study was limited to single liver tumors and that the findings should not be extrapolated to more complex treatment situations, such as previous liver irradiation or multiple liver cancers. This study provides a novel noncoplanar field technique whose dosimetric advantage has been verified using the N-VMAT-Cage plan for HCC.
Because the CRTS is still a simulation study, there is currently no ready-made planning system that conforms to this accelerator structure. The CT was deflected 90° to enable the corresponding planning design in the Pinnacle 3 planning system. In the future, a TPS suitable for the cage system should be developed. One major drawback of N-VMAT-Cage may be prolonged treatment time. In HCC treatment, treatment delivery speed is very critical to reduce the impact of intrafraction motion on the treatment outcome. Although VMAT is a time-saving delivery technique, it may result in lower plan quality. N-VMAT-Cage is expected to achieve a higher plan quality than VMAT with only a minor and acceptable increase in delivery time, whereas N-VMAT-Cage with superior plan quality will have significantly shorter delivery times than N-VMAT, according to the theory of the CRTS. However, since no TPS is suitable for the cage system, specific delivery times have not been compared among the 3 radiotherapy techniques. The N-VMAT-Cage technique does not require couch rotation, which reduces movement between organs and the delivery time, compared with N-VMAT. Moreover, N-VMAT-Cage is superior to the 2 other techniques in terms of dosimetric advantages. In the future, we will further enhance the application of CRTS on different types of tumor and a greater number of patients. What's more, we will distinguish the difference between large PTV and small PTV in treating HCC patient with CRTS.
Conclusion
In this study, N-VMAT-Cage plans with the arrangement of noncoplanar arcs provided significant dosimetric gains over N-VMAT and VMAT plans, except for the heart and lung. N-VMAT-Cage significantly reduced the healthy liver dose compared with N-VMAT and VMAT and should be used in more clinically challenging cases.
Footnotes
Abbreviations
Authors’ Note
For this study, anonymized patient data was used. According to our local ethics committee this does not require ethics approval.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No.11875320).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the National Natural Science Foundation of China (No.11875320).
Appendix
A cage-like radiotherapy system (CRTS) has 2 stands, which are fixed to the ground in parallel, and their circular through-holes are located coaxially along with the longitudinal axis. A free treatment volume is formed between the 2 stands. Thereby, irradiating the body with sliding angle range of −45° to 45° can be done from different directions around the treatment volume. The structure of CRTS is shown in Figure A1. The sphere is constructed with the source axis distance as the radius. The stereoscopic irradiation angle achievable with the C-Linac is marked on the surface of the sphere with a thin line. The stereoscopic irradiation angle achievable with the cage radiotherapy unit is marked on the surface of the sphere with a thick line.