
Abstract
Background:
The purpose of this preliminary study is to evaluate the feasibility of the excisional ultrasound (US) guided vacuum-assisted breast biopsy (VAE), followed by US-guided Laser Interstitial Thermal Therapy (LITT) in the treatment of unifocal ductal breast carcinomas ≤ 1 cm and estimate the ablation rate analyzing the final histopathological results after subsequent surgical excision.
Methods:
In a single session 11 female patients with unifocal less than a centimeter breast cancer underwent 2 different minimally invasive percutaneous US-guided techniques: a VAE breast biopsy with an 8 G needle to remove the lesion and, immediately after, a LITT ablation in the biopsy site. Four weeks later, all patients underwent radiological follow-up. Afterward, a systematic surgery was performed, the ablation rate was calculated, and iconographic and histological features were correlated.
Results:
Average maximum diameter of the lesions was 7.6 mm (5-10 mm). No patient reported pain or discomfort during procedure. 1/11 patient (9.1%) reported an early minor complication (a small superficial skin burn). After surgical excision, the histopathological evaluation reported in 10/11 cases (90.9%) complete ablation of the target lesion. In only one case (9.1%) residual cancer was detected. The necrotic-hemorrhagic cavities showed a mean maximum diameter of 27.3 mm (20-35 mm).
Conclusions:
Laser ablation performed after excisional biopsy could be considered a valid alternative to surgical excision for the treatment of lesions ≤ 1 cm, if carried out by expert radiologists. The association of these minimally invasive percutaneous methods has proven to be reliable, fast, and safe with an ablation rate of 90.9% and excellent aesthetic results. RM and CESM are potentially able to quantifying treatment results and to follow-up the ablation effects.
Introduction
Over the past decade, there have been extraordinary developments in breast cancer research, clinical management and therapy that changed the landscape of the disease presentation, allowing considerably more options for patients, particularly in the treatment of early breast cancer, with a transition from radical surgery to minimally invasive surgery. De facto, many randomized studies have shown that there is no evident advantage in overall survival in breast cancer patients treated with mastectomy and axillary dissection compared to those undergone conservative surgery. 1 -3
The evolution of minimally invasive techniques has been not only a consequence of the progress in diagnostic imaging to obtain an early diagnosis but also a need born from the pressing request of patients for conservative methods. 4 In the last few years, several radiologically guided percutaneous ablative treatments of breast lesions have been proposed, such as radiofrequency, cryo-ablation, microwave, high-intensity focused ultrasound (US), irreversible electroporation and laser interstitial thermal therapy (LITT). 5 -7 In fact, the increasing frequency of diagnosis of small tumors has led to improve the therapeutic path in this selected group of patients. Furthermore, the possibility of obtaining, as traditional surgery, the oncological radicality of breast cancer but with better aesthetic results, low cost, and reducing hospitalization time is a very attractive objective. The first method introduced in the minimally invasive treatment of breast lesions was laser thermal ablation with a study conducted by Harries in 1994. 8 Since then, several studies have been carried out but the results are limited because the different works have not assessed the adequacy of the ablation, but only the presence or absence of ablative changes. 8 -11
There are few studies in the literature evaluating the adequacy of laser thermal ablation treatment with anatomic-pathological evaluation after subsequent surgical excision, demonstrating an ablation rate between 50 and 100%. The ablation rate rises between 84 and 100% if only small breast lesions are considered. 12 -15
Moreover, there are also studies on the laser thermal ablation of benign lesions, such as fibroadenomas 16,17 or as palliative therapy in inoperable or refusing surgery patients. 18
It is also important underline that LITT has already been widely standardized in several studies in the literature, both ex-vivo and in-vivo, on brain, bone, skin, gastrointestinal, liver, lung, pancreas, thyroid, retinal lesions, prostate and uterus 19 -26 ; however the validation of tumor ablate therapy in breast clinical practice is still ongoing, more prospective studies addressing local failure rates, cosmesis, the effectiveness to detect residual untreated disease, and long-term patient satisfaction are required. 27
The purpose of this preliminary study is to evaluate the feasibility of the excisional eco-guided vacuum-assisted breast biopsy, also known as Vacuum-Assisted Excision (VAE), followed by eco-guided LITT in the treatment of unifocal ductal breast carcinomas, ≤ 1 cm in maximum diameter, and estimate the ablation rate analyzing the final histopathological results after subsequent surgical excision. A secondary aim is to assess the sensitivity of Contrast Enhanced Spectral Mammography (CESM) and Magnetic Resonance Imaging (MRI) in the evaluation of tumor ablation, using histopathological results as a benchmark.
Materials and Methods
The study was carried out at Tor Vergata University Hospital (Rome, Italy) between August 2018 and November 2019. It was approved by Tor Vergata Hospital Independent Ethics Committee (approval n° 70/18). All patients provided written informed consent before participating in the study.
Inclusion criteria were: women ≥ 18 years with a diagnosis of US-detectable ≤1 cm in maximum diameter, unifocal, invasive breast cancer lesion, at least 1 cm depth from the skin surface and pectoralis muscle. Patients with lobular carcinomas, multifocal or multicentric carcinomas, a prior history of breast carcinoma were excluded.
At first, a needle core biopsy was performed on all patients with a suspicious nodular lesion on conventional mammography and breast US. Histopathological results were classified in the diagnostic categories (B1-B5) according to the Fourth edition of the European guidelines in breast cancer screening and diagnosis. 28
Subsequently, a second-level imaging, as breast MRI or CESM, was performed on all patients with a diagnosis of invasive breast cancer, for loco-regional staging and to assess unifocal/multifocal nature of the tumor (Figure 1). The preferred imaging method for staging was MRI (Gyroscan Intera 1.5 T, Philips Healthcare, Best, the Netherlands), performed before and after the intravenous injection of 0.15 mmol/kg of gadobenate dimeglumine (Gd-BOPTA-Multihance; Bracco Imaging, Milan, Italy) and a 20-mL saline infusion. In case of inability to carry out MRI (incompatible metal devices or habitus, claustrophobia, contraindications to gadolinium) CESM was performed (Senographe Essential mammography, GE Medical Systems SCS, Buc, France). CESM is a mammographic technique utilizing a dual-energy exposure undertaken during a single breast compression, following the injection of an iodinated contrast agent (1.5 ml/kg body weight) and a 20-mL saline infusion. Two minutes after injection, standard mediolateral oblique (MLO), laterolateral (LL) and craniocaudal (CC) projections are undertaken on each breast.

The image shows bilateral mammography in cranio-caudal (A) and medio-lateral-oblique projections (B) demonstrating on inferior-external quadrant of left breast an irregular radiopacity. US evaluation confirm a solid hypoechoic lesion, with irregular shape, not parallel orientation, measuring 7 mm in maximum diameter (C). CESM (in left cranio-caudal and left medio-lateral-oblique projections), performed after the diagnosis of Ductal Infiltrating Carcinoma, indicates pathological enhancement of the known lesion and demonstrates its unifocality (D).
In the present preliminary study, 11 female patients met the inclusion criteria and, in a single therapeutic session in an ambulatory care setting, underwent 2 different minimally invasive percutaneous US-guided techniques: a VAE breast biopsy with an 8 Gauge (G) needle to remove the lesion and, immediately after, a LITT ablation in the biopsy site (Figure 2). Procedures were performed with a free-hand approach by a radiologist with 15 years of experience in breast interventional radiology and 20 years of experience in breast imaging.

The image shows US frame of the lesion in Figure 1 subjected to VAE breast biopsy (A), the moment of histological specimen collection (B), fiber introduction into the biopsy site (C), and an US image post LITT ablation (D).
The patient was positioned supine and the US examination was performed to identify the breast nodular lesion. After disinfecting the area and administering local anesthesia (10 ml lidocaine hydrochloride 2%), a 5 mm incision was performed using a scalpel to guarantee appropriate access for the needle insertion. The excision was achieved with a Mammotome vacuum-assisted system (Devicor Medical Products, Inc., Cincinnati, OH, USA) with an 8-G needle under the guidance of high-resolution US equipment (MyLabTM 9 XP, Esaote SpA, Genoa, Italy) with 5-13 MHz linear array transducer, obtaining a minimum of 12 samples, until there was no US evidence of the lesion. When US evidence of complete resection was achieved, the VAE device was removed and, afterward, LITT ablation started.
The optic fibers were connected to a multi-source laser system operating at 1.064 nm (EchoLaser X4, Elesta srl, Calenzano, Italy). A single fiber through a 21 G needle, was inserted in the biopsy site under US-guidance with the fiber tip placed in the center of the target area.
The position of the applicators was carefully controlled using a bi-planar ultrasound probe.
At this point, it was supplied a power of 6 W and an energy between 1200 J e 1800 J. Laser (Light Amplification by Stimulated Emission of Radiation) light comes out of the fiber tip and turns into thermal energy capable of destroying any remaining cancer cell. The temperature near the tip of the fiber reaches 100° C, causing vaporization in the target tissue area and cell death through protein denaturation and coagulative necrosis. The progress of ablation was monitored by US.
At the end of the laser ablation, the fiber was removed and the operator released a MR-compatible titanium clip. Thereafter, the biopsy site was compressed manually for at least 10 minutes until complete haemostasis. Sterile adhesives were placed on the incision site and locoregional therapy with ice and systemic antibiotics therapy were prescribed. Four weeks later, all patients underwent clinical examination and radiological follow-up, which included breast US evaluation and second-level imaging (MRI or CESM) that were compared to the ones performed before the procedures. During the radiological examinations, the size of the necrotic cavity was measured and, after contrast medium injection, the presence in the treated area of suspicious contrast-enhancement referable to residual tumor was evaluated. Rim enhancement around the cavity was considered inflammatory reaction.
Afterward, a systematic surgery was performed and histopathological examination evaluated presence of residual breast cancer and the size of necrotic cavity (Figure 3). The ablation rate was calculated, and iconographic features were correlated to histological results. Comparing radiological examination with histopathological results after surgery, patients were categorized into 4 groups: “true positive” (both imaging and histopathological evaluation showed macroscopic residual tumor), “true-negative” (neither imaging nor histopathological evaluation showed macroscopic residual tumor), “false-negative” (imaging showed no macroscopic residual tumor, whereas histopathological evaluation demonstrated the presence of cancer residue), “false-positive” (imaging showed macroscopic residual tumor, whereas histopathological evaluation did not).

The image shows left mammography in cranio-caudal (A) and medio-lateral-oblique projections (B) executed after LITT, demonstrating edema into the site of the previous procedure without contrast enhancement referable to residual tumor in CESM in cranio-caudal (C) and in medio-lateral-oblique projections (D). It is shown also the moment of systematic surgery (E), the surgical resection specimen with the measurement of the necrotic cavity (F), and the histological sections of hematoxylin-eosin stain without evidence of tumor residue (G).
The MRI- and CESM-negative predictive value and sensitivity rate were calculated.
Continuous variables are presented as the mean ± standard deviation. Pearson correlation index was used to compare differences between the size of the inflammatory collection, measured with CESM or MRI, and the size of the necrotic-hemorrhagic cavity resulting from the definitive pathological analysis. Schematic representation of the method is summarized in Figure 4.

Flow chart of the study phases.
Results
The study included 11 female patients, with mean age 61 years ± 6.1 (range: 54-70 years).
Average maximum diameter of the lesions subjected to treatment was 7.6 mm ± 1.4 (range 5-10 mm); all the lesions were Infiltrating Ductal Carcinomas (B5b).
Local staging was performed using MRI in 8/11 (72.7%) cases and CESM in 3/11 (27.3%) cases.
No patient included in our study reported pain or discomfort during VAE and LITT, and no one stopped the procedure before it ended. None of these patients experienced significant complications after the procedure (deep skin burns, infections or hematoma requiring aspiration). However, 1/11 patient (9.1%) reported an early minor complication represented by a small superficial skin burn.
The radiological follow-up, executed on average 32.6 days ± 9.2 (range 22-57) after treatment, with the same contrast imaging technique used pre-treatment, revealed, in each patient, the inflammatory collection in the site of percutaneous treatment (Figure 5), with a mean maximum diameter of 34.2 mm ± 4.9 (range 32-43).

The image shows a comparison between MRI before (A and B) and after (C and D) LITT. The T2 weighted (A) and the T1 weighted post-contrast dynamic sequences (B) performed before procedure show a mass enhancement in the external quadrants of left breast that appears replaced by a necrotic cavity (C) with only inflammatory rim-enhancement (D) after procedure.
Surgery was carried out on average 10 days ± 3.3 (range 2-16) from clinical examination and radiological follow-up after treatment. After surgical excision, the histological examination revealed in all cases the effects of laser-ablative therapy showing a central necrotic cavity containing fibrin-blood, material surrounded by an intense xantho-granulomatous inflammatory reaction with multinucleated giant cells, steatonecrosis and fibrosis. After macroscopic histopathological analysis, the necrotic-hemorrhagic cavities showed a mean maximum diameter of 27.3 mm ± 4.4 (range 20-35 mm).
The histopathological evaluation reported in 10/11 cases (90.9%) complete ablation of the target lesion with no tumor residue. In only one case (9.1%) (Figure 6), residual cancer, represented by 2 foci of Infiltrating Ductal Carcinoma (measured, respectively, in 1.5 and 2.0 mm), was detected.

The image shows CESM in medio-lateral-oblique (A) and in cranio-caudal projections before LITT (B) presenting a lesion in the external quadrants of left breast, CESM after LITT (C) and histological sections of hematoxylin-eosin stain showing at low magnification the central necrotic-hemorrhagic cavity with the 2 foci of Infiltrating Ductal Carcinoma (arrow heads) (D), and a detail of a focus of Infiltrating Ductal Carcinoma in image at high magnification (E).
Correlating radiological (MRI/CESM) and histopathological data, 8 true negatives, 1 true positive, 0 false negative and 2 false positives resulted. These data demonstrate 100% in both sensitivity and negative predictive value of MRI and CESM in assessing the effectiveness of LITT. Furthermore, as showed in Figure 7, a statistically significant correlation was observed between the size of the inflammatory collection, measured with CESM or MRI, and the size of the necrotic-hemorrhagic cavity resulting from the definitive pathological analysis (Pearson correlation index r = 0.649).
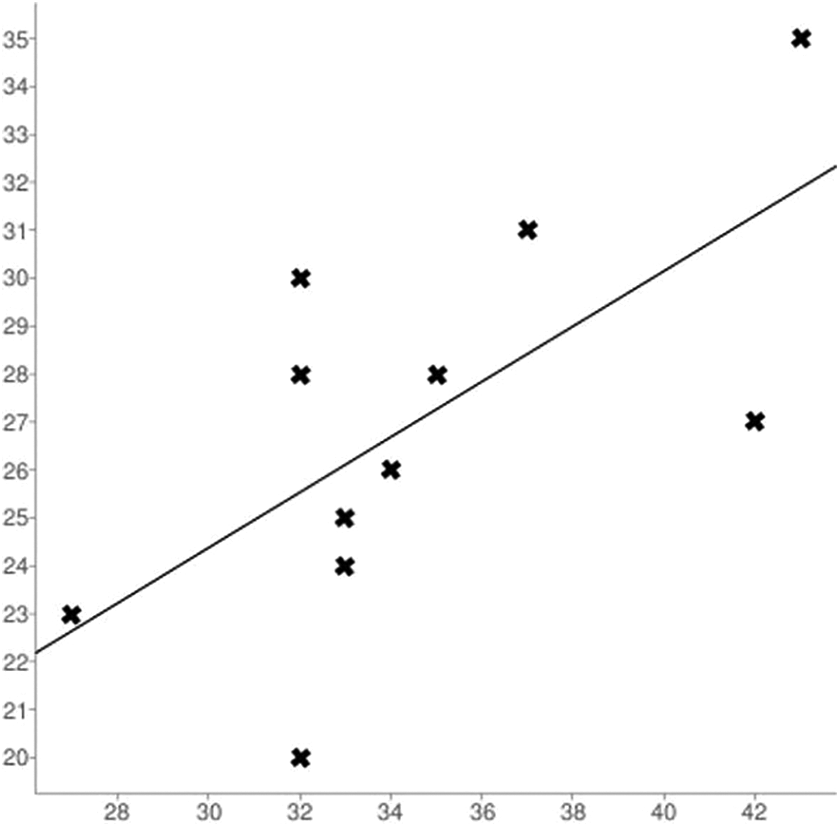
The graph shows a direct linear relationship between the size of the inflammatory collection measured with CESM or MRI (abscissas) and the size of the necrotic-hemorrhagic cavity evaluate on histopathological analysis after surgery (ordinates), resulting in a statistically significant correlation (Pearson correlation index r = 0.649).
Discussion
During last years, a series of minimally invasive ablative treatments of breast lesions with a radiological guide have been tested. 5 -7 These types of treatments allow the ablation of the lesion due to the percutaneous emission of different types of energy for destroying cancer cells. The laser radiation diffuses into the tissues as thermal energy able to determine tumor necrosis with both direct damage, caused by the increased temperature (thermo-ablation), and also indirect damage to the surrounding tissue. Indirect effects occur after thermo-ablation by progressive destruction of the tissue by vaporization, microvascular damage, necrosis and the activation of a strong immune reaction capable of attacking the residual tumor. 14,15 Compared to other methods, the main advantage of using laser light for thermal applications is its ability to focus a precise amount of energy in a restricted area, inducing a controlled and reproducible coagulative necrosis. In addition, the photo-coagulative effect reduces the bleeding risk. Like other percutaneous ablative therapies, aesthetic results are excellent, with a reduction of costs and hospitalization rate, compared to conventional surgical therapy. Furthermore, the procedure is outpatient, well tolerated by patients, and the adverse reactions rate is very low. Actually, we reported just one case of skin burn.
In our pilot trial LITT was performed immediately after VAE procedure within the residual biopsy site.
This is the first study in literature which combines, in an unique therapeutic session, 2 different minimally invasive techniques (VAE and LITT). These techniques, both widely validated by literature, do not have however an individually reliability comparable to the surgical resection, who represents the “standard of care.” Several Authors have confirmed that VAE represents a valid alternative to surgery thanks to the capability to remove nodules up to 3 cm in size by 8 G needles. 29 -31 Indeed, it has been widely validated for the treatment of some B3 (uncertain malignant potential) lesion. 32 -34 The proposal to associate VAE with a second minimally invasive percutaneous therapy such as LITT for the treatment of B5 lesions is interesting and totally innovative. The aim of the laser procedure would be to erase the residual tumor cells from the procedure cable.
In our opinion systematic VAE + LITT association offers great potential. Our results demonstrate the feasibility of this procedure with a success rate of 90.9%, complete lesion ablation occurred in 90.9% of cases. This value is far higher than the ablation rates found in literature about the exclusive use of LITT. 12 -15 Just in one case we observed a tumor residue (respectively, 2 foci of 1.5 and 2 mm). We would highlight that it was the first Patient of our trial, the reason why failed ablation could be related to the lesser confidence with the technique. In this regard, several studies have demonstrated that results improve with experience. 12 -14 The visualization of the target area during the procedure can be difficult due to tissue vaporization and an incorrect positioning of the laser needle-fiber can invalidate the treatment goal. Thus, the radiologist should have a long experience in breast interventional procedures and excellent manual skills. In 2 cases (18.2%), histological analysis showed the presence of a millimetric carcinoma far from the central cavity.
The main limit of this study is to miss further carcinomas in residual breast, not previously diagnosed by imaging due to their small size; this possibility could improve risk of local disease recurrence. In this regard, it is important to remind that the detection rate of new carcinoma foci is currently high in conventional breast conservative surgical therapy. According to Houssami et al., positive margins rate is 26% in patients treated with quadrantectomy or nodulectomy and there is also no clear evidence of correlation between negative margins and reduced risk of local disease recurrence. 35 Despite a surgical adequate resection, the possibility to find additional cancers in residual breast is high. However, the use of loco-regional radiotherapy and medical therapy reduces the probability of both local and systemic recurrence.
The laser ablation performed after excisional biopsy could therefore be considered a valid alternative to surgical excision for the treatment of lesions ≤ 1 cm. The small tumors detection is now increasingly frequent thanks to technological advances, the spread of large-scale screening programs and awareness-raising campaigns on the importance of early diagnosis which increases the survival rate. 6 The possibility of reducing the aggressiveness of the breast cancer therapeutic approach is a topic of great social interest, both economically and psychologically for patient, so VAE + LITT association could be the answer in this concern.
Finally, there was a statistically significant correlation between histopathological results and MRI/CESM findings that shows a negative predictive value of 100% for tumor residuals. RM and CESM are potentially able to follow-up the ablation effects and could be used in future studies as a reference parameter in quantifying treatment results and patient follow-up. This technique reachs the goal to measure the size of necrotic cavity compared to the histopathological analysis (p < 0.01). Nevertheless, CESM, as RM, has presented false positive cases. Post-treatment inflammation and edema could in fact limit the complete visibility of the neoplastic residue present. In future works could be interesting to use some statistical measurements, US/MRI co-registration or textural features to help radiologists characterize the enhancement. 36 -38
Conclusions
Although our results are based on a preliminary study on a small cohort of patient, we propose that Infiltrating Ductal breast Carcinomas (maximum diameter ≤ 1) could be treated with VAE + LITT, if carried out by expert radiologists. The association of these minimally invasive percutaneous methods has proven to be reliable, fast, safe and well tolerated with an ablation rate of 90.9% and excellent aesthetic results. MRI and CESM have shown high sensitivity and negative predictive value in monitoring the effects of the ablative procedure, with a strong radiological-pathological correlation between the size of the inflammatory collection radiologically detected and the histological necrotic-hemorrhagic cavity.
Further studies are necessary to standardize and validate this technique for treatment of small breast lesions, is important underline that only a close cooperation between different specialists in a multidisciplinary team, finalized to a correct selection of patients, will allow the success of this new minimally invasive therapeutic approach.
Footnotes
Abbreviations
Authors’ Note
Approved by the ethics committee of the University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.