
Abstract
(1) Background:
The coexistence of chronic kidney disease (CKD) and cancer is common due to the increased incidence of cancer in patients with CKD. Glomerular filtration rate is the optimal way to measure kidney function. To date, little is known about the role preoperative renal function plays in the prognosis of NSCLC patients.
(2) Methods:
The study enrolled 140 patients who had been newly diagnosed NSCLC and received potential radical surgery for treatment from 2009 January to 2012 December. The detailed characteristics were collected including gender, age, smoking and drinking habits, KPS score, hemoglobin levels, tumor size, pathology type, differentiation, pTNM stage and serum creatinine before surgery. Univariate and multivariate analyses of overall survival (OS) and disease-free survival (DFS) were performed using Kaplan-Meier method and Cox model.
(3) Results:
The univariate analysis identified that the pTNM stage (p < 0.001), eGFR level (p = 0.006), and adjuvant treatment (p = 0.007) were prognostic factors for OS, while drinking habit (p = 0.032), pTNM stage (p = 0.002) and eGFR level (p = 0.006) were the prognostic factors for DFS. Further multivariate analysis found that pTNM stage (HR = 2.091, 95% CI 1.424-3.071; p < 0.001) and eGFR level (HR = 1.890, 95% CI 1.424-3.071; p = 0.004) were independent factors associated with OS. The pTNM stage (HR = 1.735, CI 1.215-2.479; p = 0.002) and eGFR (HR = 1.793, CI 1.193-2.696; p = 0.005) were independent factors associated with DFS. Further subgroup analyses found that in female patients/ no smoking patients/ patients younger than 60 years, better eGFR level was significantly associated with better OS and DFS.
(4) Conclusions:
Decreased preoperative eGFR was associated with poor clinical outcome of NSCLC patients.
Introduction
Lung cancer is the leading cause of cancer-related deaths around the world. 1 Non-small-cell cancer (NSCLC) accounts for approximately 85% of lung cancer cases. 2 Despite the development of surgical techniques, molecular targeted therapy and improvements of chemoradiotherapy in lung cancer treatments, the prognosis of NSCLC remains poor. 3 Some studies have shown that preoperative performance status such as sex, age, smoking behavior, disease stage, histology are prognostic factors of NSCLC patients. 4 -6 However, to date, the most commonly used method to evaluated the prognosis of NSCLC patients is tumor-node- metastasis (TNM) staging system. Finding a new method to evaluate the prognosis of NSCLC patients is important for clinical treatment.
The coexistence of chronic kidney disease (CKD) and cancer is common due to the increased incidence of cancer in patients with CKD. 7 Reduced kidney function leads to increased cancer mortality in breast and urinary tract cancers. 8 Glomerular filtration rate (GFR) is the optimal way to measure kidney function. Estimated Glomerular filtration rate Estimated (eGFR) is equal to total of the filtration rates of the functioning nephrons in the kidney. In most healthy people, the normal GFR is 90mL/min/1.73m2 or higher. eGFR is fundamental to several aspects of cancer therapy, including decision in surgical treatment, perioperative management, chemotherapy dose adjustment, and preparation of long-term care. 9
Currently, little is known about the role preoperative kidney function plays in the prognosis of NSCLC patients. The prognostic value of the preoperative eGFR in NSCLC patients is not clear. In this study, our aim is to evaluate if eGFR can serve as a prognostic marker for NSCLC patients.
Methods
Patients
The present study enrolled 140 patients who had been newly diagnosed NSCLC and received potential radical surgery for treatment in Qilu Hospital of Shandong University, China and Shandong Tumor Hospital, China from 2009 January to 2012 December. All the patients required a pathological confirmed diagnosis of NSCLC. The exclusion criterion in this study: lost to follow up, coexistence of other malignancies, resection not for curative intent, stage 0 disease or if they refused to attended the study. Over all, there were 95 men and 45 women enrolled in this study. The detailed general characteristics were collected including gender, age, smoking and drinking habits, Karnofsky Peformance Status (KPS). KPS score was categorized into low (sore 10-40), intermediate (50-70), and high (80-100). 10 Tumor characteristics included size, pathology type, differentiation, pTNM stage. In addition, serum creatinine (sCr), hemoglobin levels before surgery was collected for analyses.
The treatment of the patients was adherent to the national guideline. Surgery with systematic mediastinum lymph node dissection was performed in each patient. 6 (4.3%) patients were treated with neoadjuvant treatment and 134 (97.5%) patients underwent primary lung tumor resection without receiving any primary preoperative treatment. 62 (44.3%) patients were treated with adjuvant therapy after surgery, including chemotherapy, radiotherapy or a combination of the two.
Follow-Up
The primary endpoint was overall survival (OS) and the secondary endpoint was disease-free survival (DFS). The definition of OS was the time form surgery start to death by any cause or the last follow-up, while DFS was the time from surgery start to the date of relapse or death or the last follow-up. All patients were followed up every 6 months.
Kidney Function and Glomerular Filtration Rate
The National Kidney Foundation recommends using the 2009 CKD-EPI creatinine equation of estimate GFR in adults. Kidney function is estimated by Glomerular filtration rate (eGFR) based on sCr, age, gender, ethnic, where eGFR is expressed as mL/min/1.73 m2 of body surface area and sCr is expressed in mg/dL. 11
Statistical Analysis
A hospital-based retrospective cohort study was performed. Variables were compared using Chi-square test or student’s t-test. χ2 test was employed to investigate the correlation between the different variables and eGFR levels. Survival curves were constructed according to the Kaplan-Meier method. Multivariate analysis for the significant variables was performed using the Cox model, together with the corresponding 95% CI of HR. Analyses were carried out using SPSS software (version23.0.0.0, SPSS, Chicago, IL). Statistical significance was assumed if p < 0.05.
The pTNM staging was according to the eighth edition of the Lung Cancer Staging Guide set by the American Joint Committee on Cancer and the Union for International Cancer Control.
Results
Patient Characteristics
The preoperative characteristics of 140 NSCLC patients are list in Table 1. There were 95 males (67.9%) and 45 females (32.1%). The average age at the time of diagnosis of NSCLC was 60.21years (range, 35-84). 71 (50.7%) patients had smoking behavior and 53 (37.9%) patients had drinking behavior before the surgery. KPS scores of 134 (95.7%) patients are at high level (≥80). Histopathological examination revealed 47.9% of adenocarcinoma (AC) (67, 47.9%), followed by squamous cell carcinoma (SCC) (54, 38.6%), bronchioloalveolar carcinoma (BAC) (7, 5%) and other histology types (12, 8.6%). 6 (4.3%) patients were treated with neoadjuvant treatment and 134 (97.5%) patients underwent primary lung tumor resection without receiving any primary preoperative treatment. 78 (55.7%) patients underwent pneumonectomy alone, 2 (1.4%) patients received postoperative radiotherapy, 45 (32.1%) patients received postoperative chemotherapy, and 15 (10.7%) patients received postoperative chemoradiotherapy.
General Characteristics of the NSCLC Patients (n = 140).

The median serum creatine (sCr) is 0.775 mg/dL (range, 0.418 -1.368 mg/dL). The renal function of 77 (55.0%) patients is normal (eGFR ≥ 90 mL/min/1.73 m2), while other patients had reduced eGFR level (eGFR < 90 mL/min/1.73 m2), including 57 (40.7%) patients in second level group (60 mL/min/1.73 m2 ≤ eGFR ≤ 89 mL/min/1.73 m2) and 6 (4.3%) patients in third level group (30 mL/min/1.73 m2 ≤ eGFR ≤ 59 mL/min/1.73 m2). No patient’s eGFR was less than 30 mL/min/1.73 m2 in this study. Only 7 (5%) patients had anemia before the surgery.
Relationship Between the General Characteristics and Ovearall Survival (OS) and Disease-Free Survival (DFS)
The relationship between the general characteristics and OS/DFS are showed in Table 2. The 140 patients were categorized into the following 3 groups according to eGFR levels (Table 2). The mean OS of the first group (eGFR ≥ 90 mL/min/1.73 m2) is 58.325 months (95% CI: 54.011-62.638) vs. the second group (60mL/min/1.73m2 ≤ eGFR ≤ 89 mL/min/1.73 m2), 49.579 months (95% CI: 43.870-55.288) vs. the third group (30mL/min/1.73m2 ≤ eGFR ≤ 59mL/min/1.73 m2), 41.667 months (95% CI: 14.684-68.649) (p = 0.017). The mean DFS of the first group is 54.526 months (95% CI: 49.232-59.821 months) vs. the second group, 42.263 months (95% CI: 35.590-48.936 months) vs. the third group, 35.000 months (95% CI: 5.303-64.697 months) (p = 0.007). Kaplan-Meier survival curves of OS and DFS divided by eGFR level are showed in Figure1A and B respectively, which show higher eGFR level were significantly associated with longer OS and DFS (log-rank: p = 0.006 and p = 0.006, respectively) (Figure 1). Anemia has no significant relationship with both OS and DFS (p = 0.965 and p = 0.473, respectively).
Relationship Between the Patient Characteristics and OS/DFS.


Kaplan-Meier survival cures of differences of OS and DFS in different eGFR levels.
Univariate and Multivariate Analyses of Prognostic Factors and OS/DFS
The univariate analysis identified that the pTNM stage (p < 0.001), eGFR level (p = 0.006), and adjuvant treatment (p = 0.007) were prognostic factors for OS (Table 3), while drinking habit (p = 0.032), pTNM stage (p = 0.002) and eGFR level (p = 0.006) were the prognostic factors for DFS (Table 3). Further multivariate analysis found that pTNM stage (HR = 2.091, 95% CI 1.424-3.071; p < 0.001) and eGFR level (HR = 1.890, 95% CI 1.424-3.071; p = 0.004) were independent factors associated with OS (Table 3). Chemotherapy (HR = 0.428, 95% CI 0.203-0.903; p = 0.026) was a significant protective factor compared with no treatment after surgery. Multivariate analysis also found that pTNM stage (HR = 1.735, CI 1.215-2.479; p = 0.002) and eGFR (HR = 1.793, CI 1.193-2.696; p = 0.005) were independent factors associated with DFS (Table 3).
Univariate and Multivariate Analyses of OS/DFS.

Subgroup Analyses
Relationship between eGFR level and clinicopathological variables in NSCLC patients
Further analyses indicated that eGFR level was significantly correlated with gentle (p < 0.001), age (p = 0.017), smoking (p = 0.002) and histology type (p = 0.031). However, the level of eGFR was not significantly different in other clinicopathological variables (Table 4).
Comparison of Clinical Characteristics of Patients With Different eGFR Level (χ2 test).

Subgroup analysis according to sex, age, smoking and histology type
The patients were divided according to sex, age, smoking habits and histology type. In male patients, neither OS (p = 0.071, Figure 2A) nor DFS (p = 0143, Figure 2C) were significantly different with different eGFR levels, while in female patients, better eGFR level was significantly associated with better OS (p = 0.016, Figure 2B) and DFS (p = 0.015, Figure 2D). In patients younger than 60 years old, both OS (p < 0.001, Figure 3A) and DFS (p < 0.001, Figure 3C) were significantly different in different eGFR levels, but not for patients older than 60 years (p = 0.401, Figure 3B and p = 0.533, Figure 3D, respectively). Both OS (p = 0.030, Figure 4B) and DFS (p = 0.016, Figure 4D) were significantly different in different eGFR levels for patients who didn’t smoke before the surgery, but not significantly for smoking patients (p = 0.096, Figure 4A and p = 0.197, Figure 4B, respectively). In lung adenocarcinoma patients, eGFR was significantly associated with DFS (p = 0.027, Figure 5C) but not significantly associated with OS (p = 0.132, Figure 5A). In lung squamous cell carcinoma patients, eGFR was not significantly associated with OS or DFS (p = 0.378, Figure 5B and p = 0.981, Figure 5D, respectively). Patients who were diagnosed BAC or other Histology type were not subgroup analyzed because of the small sample.

Kaplan-Meier survival cures of Differences of OS and DFS divided by eGFR in male and female patients.
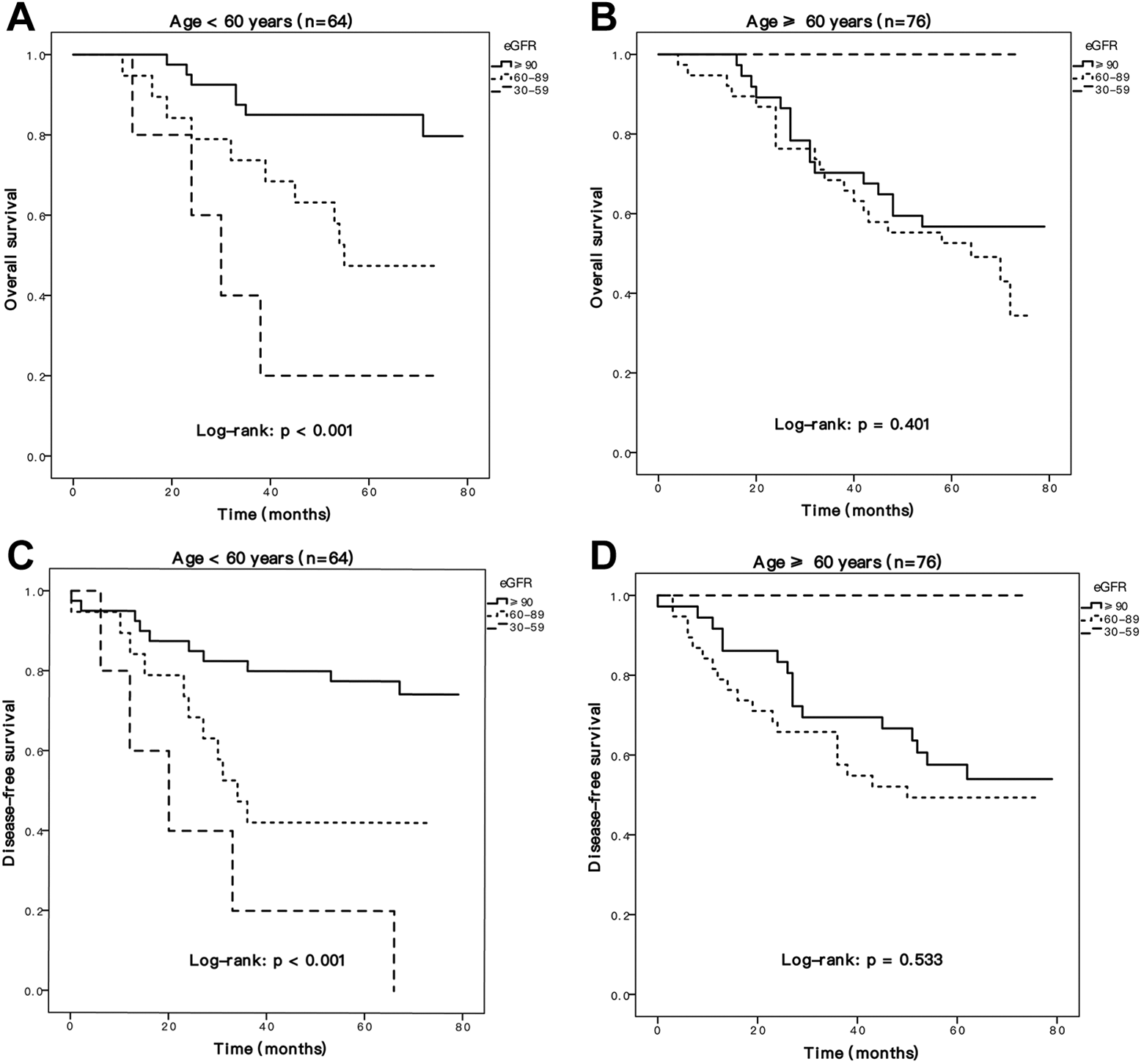
Kaplan-Meier survival cures of Differences of OS and DFS divided by eGFR in different age group.

Kaplan-Meier survival cures of Differences of OS and DFS divided by eGFR in smoking and no smoking group.

Kaplan-Meier survival cures of Differences of OS and DFS divided by eGFR in AC and SCC patients.
Discussion
To our knowledge, the present study is the first report to explore the association of preoperative eGFR level with general characteristics and survival outcome in NSCLC patients. Patients with cancer commonly present with impaired renal function 12 and eGFR is currently the standard measurement for determining renal function. We found that decreased preoperative eGFR was significantly associated with poor clinical outcome of NSCLC patients. Cox regression analysis showed eGFR was an independent prognostic factor of both OS and DFS. Studies found new equation to analyze eGFR in cancer patients 9,13,14 which needs further validation studies to support. In that we used the 2009 CKD-EPI, which is recommended by The National Kidney Foundation, to estimate GFR level.
There are limited studies investigating the relationship between eGFR and different cancers. Individuals with CKD seem to have higher risk of developing certain types of cancers and have increased mortality after development of malignancies in certain cancer categories. 7,15 -17 Ming-Shian found the survival was not significantly different between CKD and non-CKD lung cancer patients. 18 Another study found CKD was associated with a poorer OS in patients who undergo lung cancer resection for recurrent disease. 19 Different from these studies, our study divided the CKD patients to different groups according to eGFR levels, not only CKD and non-CKD group, and provided more detailed results.
Our study found preoperative eGFR is a simple potential prediction tool for prognosis of NSCLC patients that can be added to the clinical judgment. One reason might be the limited cancer therapy options for individuals with impaired renal function. Because of the increasing number of CKD patients, improved treatment of NSCLC and many other malignancies 20 according to different eGFR level would be important. Protective treatment for renal function may be a good choice during treatment for cancer.
In addition, to our knowledge, the greatest risk for developing lung cancer is cigarette smoking. In this paper, the general characteristics showed that those patients who smoke live longer than patients who do not in table 2 (p = 0.188 for OS, p = 0.024 for DFS) and figure 4. However, in univariate and multivariate analyses, smoking was not significant risk factor for OS and DFS. The accepted risk factors by far for lung cancer also include age, environment pollution, gender, race, age, genetic influences and so on. The limited sample number and the disadvantage of retrospective study might account for why smoking was not significant related with poor lung cancer prognosis. We hold the view that smoking is a risk prognostic factor for lung cancer patients as long as the study sample being enlarged.
Anemia is a common complication of CKD and Erythropoiesis-stimulating agent (ESAs) is a common drug used to manage anemia in CKD. 21 In this study, only 7 (5%) patients has anemia and results show anemia has no significant relationship with both OS and DFS. It needs a large prospective study to investigate if anemia and ESAs could influence OS and DFS in NSCLC patients with CKD.
There are certain limitations in our study, including the limited number of patients, the retrospective nature of the data collected and the CKD stages was based on the preoperative sCr level without consideration of chronicity. Meanwhile, this study did not enroll patients with eGFR < 30 mL/min/1.73 m2 because of limited sample number. Some other factors such as weight loss cerebrovascular disease and cardiovascular disease were not included because of the difficulty of collecting data. Further studies on treatment such as anti-cancer drug dose adjustments based on different eGFR level will be valuable. We call on large sample, prospective, randomized controlled studies on this field. Despite these, our work found preoperative decreased preoperative eGFR was related with poor prognosis of NSCLC patients.
Conclusions
We found a new predictor for the prognosis of NSCLC patients. Decreased preoperative estimated Glomerular filtration rate was related with poor prognosis of female, younger, no-smoking NSCLC patients.
Footnotes
Authors’ Note
This study was approved by the Ethics Committees of Qilu Hospital, Cheeloo College of Medicine, Shandong University (approval no.KYLL-2015-069). All patients provided written informed consent prior to enrollment in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Special fund for Taishan Scholar Project. NO.ts20190973.