
Abstract
Objective:
To evaluate the diagnostic value of radial endobronchial ultrasound (R-EBUS) combination with rapid on-site evaluation (ROSE) guided transbronchial lung biopsy (TBLB) for peripheral pulmonary lesions.
Methods:
Peripheral pulmonary lesions identified by computed tomography underwent R-EBUS with or without ROSE randomly from February 2016 to August 2017. The diagnostic yield and the operation time were compared.
Results:
In total, 158 patients were involved in and completed this research, including 84 cases in the group of R-EBUS with ROSE, and 74 in the group without ROSE. The diagnostic yield of ROSE group was 85.7%. Among these positive cases, 69.4% cases were malignant tumors, and 30.6% cases were benign lesions. The operation time was (24.6 ± 6.3) min. In the group without ROSE, the diagnostic yield was 70.3%, including 35 malignant tumors (67.3%), and 17 benign lesions (32.7%). The operation time was (31.5 ± 6.8) min. There were significant differences between both groups in the diagnostic yield (χ2 = 5.556, P = 0.018) and in the operation time (t = 3.187, P < 0.01). No serious procedure related complications were observed, such as pneumothorax and hemorrhage.
Conclusion:
ROSE can improve the diagnostic yield, and shorten the operation time. R-EBUS combined with ROSE is a safe and effective technique for peripheral pulmonary lesions.
Keywords
The clinical diagnosis of peripheral pulmonary lesions is difficult because of its anatomic location far from segmental bronchus, which is difficult to reach by routine bronchoscopy. 1 Transbronchial lung biopsy (TBLB) guided by ultrasound image has been used in the diagnosis of peripheral lung diseases. In recent years, R-EBUS guided TBLB has been used to diagnose peripheral lung diseases, but it is not real time guided, so it is difficult to judge whether satisfactory samples are obtained. In order to solve this problem, the clinical application of rapid on-site evaluation (ROSE) has been used. 2 There are many reports showed that ROSE can improve the diagnostic yield and reduce the complications in transbronchial needle aspiration, which has a high clinical value, but there are few reports about its application in peripheral pulmonary lesions. 3 -5 In this study, R-EBUS combined with ROSE guided TBLB was used to assess the diagnostic yield, the operation time and safety of diagnosis of peripheral pulmonary lesions, and to analyze the validity of this method.
Materials and Methods
Patients
From February 2016 to August 2017, in the Clinical Center of Nanjing Respiratory Diseases and Imaging, 158 consecutive cases underwent R-EBUS-TBLB for peripheral pulmonary lesions, 84 of whom underwent R-EBUS-TBLB with ROSE (ROSE group) and the 74 patients without ROSE (Non-ROSE group). Inclusion criteria: the diameter of pulmonary peripheral lesions found by chest CT was less than or equal to 30 mm, and there were invisible lesions in the tube under bronchoscope. Exclusion criteria were severe emphysema, bullae in lung parenchyma near to pulmonary lesions, cardiopulmonary function insufficiency. hemorrhagic diseases or coagulation disorders. Our study was approved by The Affiliated Brain Hospital of Nanjing Medical University Ethics Committee (approval no. NJXK16208). Prior to inclusion in the study, all patients provided written informed consent.
Equipment
Patient underwent flexible bronchoscopy (BF-1T260, Olympus, Japan) 5.8 mm in external diameter for complete inspection of airways before echo endoscopy. The EBUS (EU-M30 S, Olympus, Japan) was integrated with a 20 MHz radial probe (UM-S30-20 R, Olympus, Japan) 2.0 mm in external diameter and guide sheath kit (K-203, Olympus, Japan). For ROSE, the Diff-Quick staining method (American Scientific Products, McGaw Park, IL) was used and cytological evaluation was processed with microscope (DM500, Lycra, Germany)
Procedures and Equipment
All patients were examined preoperatively by chest CT scan before operation to assess the size and lesions location. Bronchoscopy was applied under conscious sedation. Solid food and liquid fasting for 6 hours before operation and 2% lidocaine aerosol inhalation were routine procedure. During the operation, operators must observe and record blood pressure, saturation of pulse oxygen and clinical symptom. A biopsy forceps was inserted into guide sheath before procedure, location and fixed probe. The guide sheath -covered probe was inserted through the work channel of the bronchoscope and adjusted the lesions to get the EBUS images (Figure 1A). After achieving the EBUS image, the assistant helped to fix the bronchoscope, confirmed that the guide sheath entered to working channel entrance, then removed the probe and kept the guiding sheath in place. Biopsy forceps obtained specimen through the guide sheath.
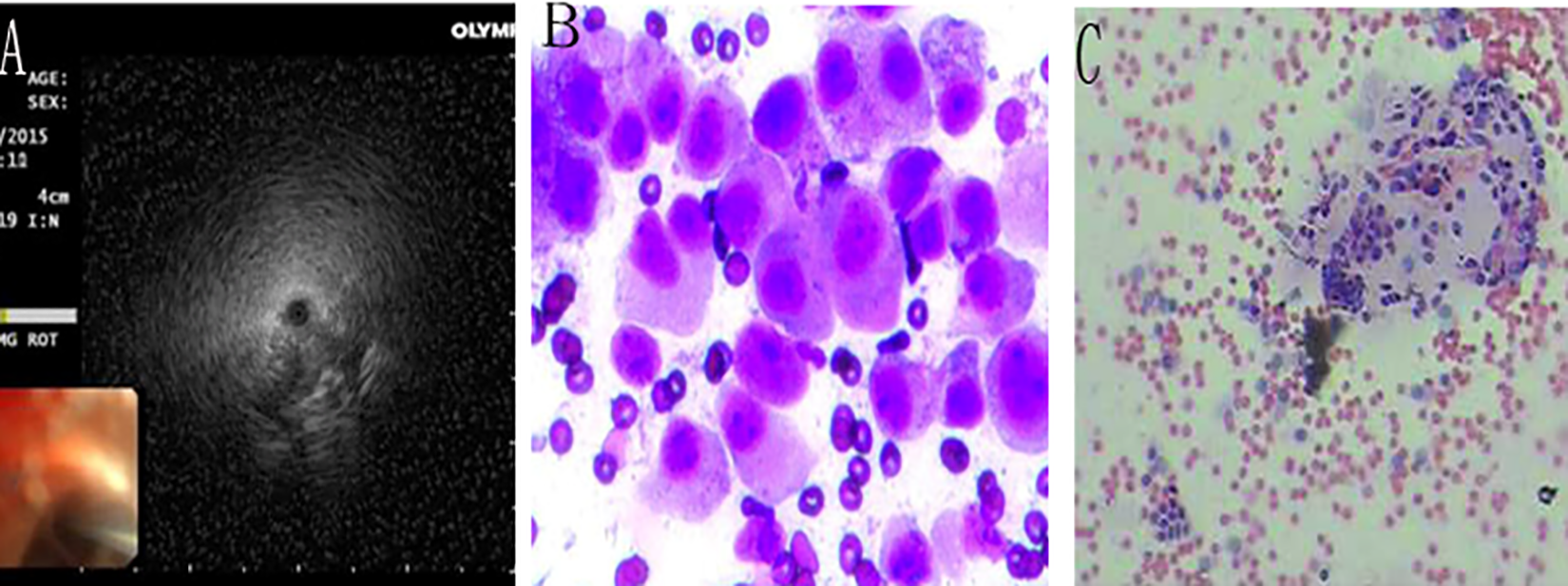
(A) Endobronchial ultrasound image with typical findings indicating peripheral pulmonary lesions; (B) Histopathological biopsy revealed a malignant lesion (adenocarcinoma) and (C) benign lesions (pneumonia).
Rapid On-Site Evaluation
The specimens were smeared on several glass slides. Air-dried smears were carried out with Diff-Quick staining for ROSE. 6 The reagent Diff-Quick A solution, Diff-Quick B solution and phosphate buffer solution were prepared by printing method. After fixation, the specimens were stained in Diff-Quick A solution for 5-10 s, then the Diff-Quick A solution was slowly soaked in phosphate and washed out, and the slides were dried gently and then put in Diff-Quick B solution for 5-10 s for staining. The diagnosis was made by washing, drying and optical microscopy. After reading the film, judge whether the puncture is effective and evaluate whether the lung biopsy to be continued.
If the ROSE results were positive (Figure 1B and C), the TBLB operation would be finished, otherwise, another biopsy site would be sampled. The number of R-EBUS attempts per lesion is less than 5 times. 7 The remaining specimens were fixed in 10% formalin by hematoxylin and eosin staining for histological diagnosis. The final pathological diagnosis was completed by 2 experienced pathologists. 8
Outcome Measures
The diagnostic yield, the operation time and the complication of ROSE group and Non-ROSE group were compared. The most common complication of TBLB is bleeding. The amount of bleeding is estimated by bronchoscopy doctors according to the microscopic manifestations. According to the literature, it can be divided into minimal bleeding (<5 ml), mild bleeding (5-20 ml), moderate bleeding (>20-100 ml) and severe bleeding (>100 ml). 9 The operation time: from the bronchoscope reaching the carina to exiting the glottis.
Final Diagnosis
R-EBUS-TBLB pathological results confirmed the final diagnosis definitely. In case of non-diagnostic patients, the final diagnosis was determined or confirmed through additional medical examinations and/or by clinical and radiographic follow-up for at least 6 months.
Statistical Analysis
All data analysis was performed using SPSS software version 20.0. Measurement data are expressed as mean ± S.D, enumeration data are expressed as a percentage. Differences in Continuous variables between 2 groups were compared by unpaired Student’s t-test while χ2 test was applied to compare the difference in percentages between groups. P < 0.05 was considered statistically significant.
Results
Clinical Characteristics
Studies have shown that, in Table 1. Of the 84 patients in ROSE group, 54 were male and 30 were female. The average age was (58.5 ± 11.4) years. The diameter of the lesion was (24 ± 5) mm. In the Non-ROSE group, there were 46 males and 28 females. The average age was (59.3 ± 10.3) years. The diameter of the lesions was (26 ± 3) mm. In ROSE group, there were 20 nodules in the right upper lobe (23.8%), 12 in the right middle lobe (14.3%), 22 in the right lower lobe (26.2%), 12 in the left upper lobe (14.3%), 18 in the left lower lobe (21.4%). In Non-ROSE group, there were 18 in the right upper lobe (24.3%), 10 in the right middle lobe (13.5%), 22 in the right lower lobe (29.7%), 10 in the left upper lobe (13.5%), and 14 in the left lower lobe (18.9%). There was no statistical difference between the 2 groups.
Demographics and Baseline Values.

Diagnosis of R-EBUS-TBLB
In ROSE group, the diagnostic yield was 85.7%, in which malignant tumor was 69.4%, benign disease was 30.6%, and in Non-ROSE group, the diagnostic yield was 70.3%, including malignant tumor 67.3%, benign disease 32.7%. Compared with ROSE group, the difference of diagnostic yield between the 2 groups was statistically significant (χ2 = 5.556, P = 0.018) (Table 2).
Diagnostic Yield According to Clinicopathological Characteristics.
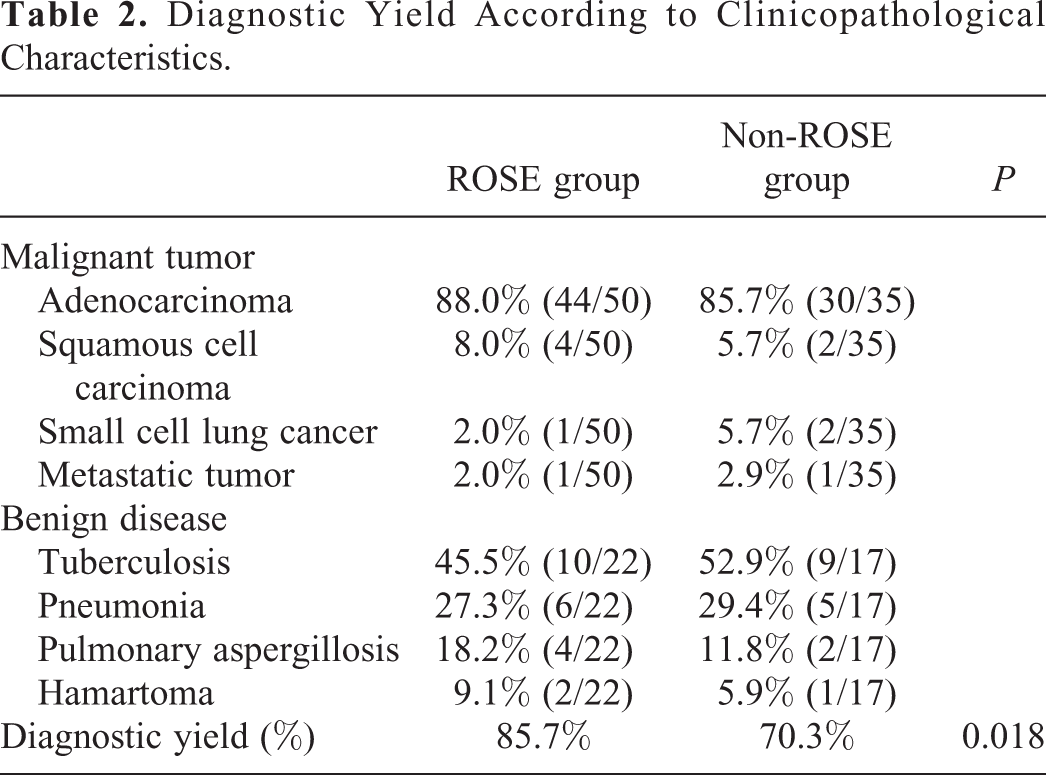
In ROSE group, there were 50 malignant tumors, including 44 adenocarcinoma, 4 squamous cell carcinoma, 1 small cell lung cancer and 1 metastatic tumor, 22 benign diseases, including 10 tuberculosis, 6 pneumonia, 4 pulmonary aspergillosis and 2 hamartoma; in Non-ROSE group, there were 35 malignant tumors, including 30 adenocarcinoma, 2 squamous cell carcinoma, 2 small cell lung cancer and 1 metastatic tumor, 17 benign diseases, including 9 tuberculosis, 5 pneumonia 2 pulmonary aspergillosis and 1 hamartoma (Table 2).
Effect of EBUS-TBLB on Diagnostic Yield
The diagnosis yield of peripheral lung lesions in different parts based on the combination of biopsy and ROSE was respectively, 90.0% in the right upper lung, 66.7% in the right middle lung, 86.4% in the right lower lung, 91.7% in the left upper lung, 88.9% in the left lower lung. The diagnosis yield of Non-ROSE group was respectively, 61.1% in the right upper lung, 60.0% in the right middle lung, 81.8% in the right lower lung, 50.0% in the left upper lung and 85.7% in the left lower lung. The diagnostic yield of right and left upper lung in ROSE group was higher than that of Non-ROSE group, and the difference was statistically significant (Table 3).
Effect of EBUS-GS-TBLB on Diagnostic Yield.

The diagnosis yields of ROSE group and Non-ROSE group were 88.0% and 77.6% respectively for the peripheral lesion diameter >20 mm. There was no statistically significant difference between groups (P > 0.05). Concurrently, the diagnosis yields of ROSE group were higher than that of Non-ROSE group in the lesion diameter ≤20 mm (P < 0.05, Table 3).
Results of Outcome Measures
In the Non-ROSE group, the number of biopsies, the hemorrhage rate and the operation times were all higher than that of ROSE group (Table 4). Mild bleeding occurred in 9 cases of ROSE group and 20 cases of Non-ROSE group. The hemorrhage was stopped after 1:1 000 ice saline, adrenaline or thrombin injected through endobronchial channel. No serious bleeding or complications such as pneumothorax occurred in this study.
Comparison of Index Between ROSE and Non-ROSE group.

Discussion
The diagnosis of peripheral pulmonary lesions is often affected by the stenosis of bronchus which is connected with them and difficult to enter by endoscopy. For lesions especially close to the chest wall, CT guided percutaneous lung biopsy can be used for diagnosis, but it is difficult to carry out because of the risk of pneumothorax and bleeding for lesions far away from the chest wall or with large blood vessels around.
R-EBUS technique uses a fine high-frequency radial ultrasound probe to reach the distal bronchial lesions through the bronchoscope working channel, which can clearly show the lesions in the distal airway, and detain the guiding sheath to carry out biopsy in the lesions. Since the use of EBUS-TBLB, a number of study results showed that the technology was safe and effective in the diagnosis of lung lesions. 10,11 In previous study, R-EBUS was used in the diagnosis of peripheral pulmonary lesions, but the application of R-EBUS combined with ROSE in the diagnosis of peripheral pulmonary lesions has not been reported.
Previous studies showed that, compared with the group without ROSE, the number of cases with unsatisfactory specimens in ROSE group decreased, and the diagnostic yield of malignant tumors was high, so it was demonstrated that ROSE could improve the diagnostic yield. 12 In this research, the diagnostic yield in ROSE group was 75.5%, and that of Non-ROSE group was 70.3%. There was statistical difference between the 2 groups, which was consistent with the above conclusions.
The characteristics of the lesion will bring out an influence on the diagnostic yield. Previous studies have suggested that the size of the lesion affects the diagnostic yield. Due to the technical and tracheal structure reasons, the sampling tools cannot approach the smaller focus and the smaller focus does not involve more bronchioles, thus affecting the diagnostic yield. 13,14 In this study, the diagnostic yield of the lesions with diameter >20 mm had higher than that of lesions with diameter ≤ 20 mm, the difference was statistically significant, suggesting that R-EBUS combined with ROSE had significance in improving the diagnostic yield for peripheral pulmonary lesions.
In the current research, the diagnostic yield of each lobe is not same, which is consistent with the previous study report that the location can affect the diagnostic yield and the relatively low diagnostic yield of the upper lobe of the right and left lung. 15 It may be the bending angle of the right upper lobe and the left upper lobe proper branch is too large without brush detection of ROSE, the ultrasound probe is difficult to stick to the focus and the tool for taking materials is soft, and the excessive bending occurs after extending to the distant focus, which leads to the failure to completely extend to the focus according to the path entered by the probe, leading to the dissatisfaction of taking materials. In the present study, under the guidance of ROSE, the extension path of biopsy forceps can be modified to reach the focus according to the probe extension path, so as to improve the diagnostic yield.
In this study, when ROSE was positive, the operation time could be reduced. Shortening the examination time can improve the efficiency of bronchoscopy and reduce the adverse physiological effects of carbon dioxide retention, blood oxygen and pH reduction, especially in reducing the operation time of patients with severe pulmonary diseases. 16 Because of the good consistency between ROSE and pathological results of biopsy, the positive result provides termination of procedure, lessening the hemorrhage and pneumothorax caused by biopsy.
To summarize, R-EBUS combined with ROSE has a high diagnostic value in the diagnosis of peripheral pulmonary lesions. It can lessen the operation time of bronchoscopy, the number of biopsy and complications, and provide a safely and feasible method for peripheral pulmonary lesions diagnosis.
Supplemental Material
Supplemental Material, CONSORT-2010-Flow-Diagram-MS-Word - Rapid On-Site Evaluation During Radial Endobronchial Ultrasound–Guided Transbronchial Lung Biopsy for the Diagnosis of Peripheral Pulmonary Lesions
Supplemental Material, CONSORT-2010-Flow-Diagram-MS-Word for Rapid On-Site Evaluation During Radial Endobronchial Ultrasound–Guided Transbronchial Lung Biopsy for the Diagnosis of Peripheral Pulmonary Lesions by Chunhua Xu, Wei Wang, Qi Yuan, Huidi Hu, Li Li and Rusong Yang in Technology in Cancer Research & Treatment
Footnotes
Authors’ Note
Chunhua Xu and Wei Wang contributed equally to this work.
Acknowledgments
We gratefully acknowledge Professor Like Yu and Xiuwei Zhang for technical assistance. We thank Ms Qian Zhang for advice and discussions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Medical Scientific Research Project of Jiangsu Provincial Commission Health and Family Planning (H2017048).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.