
Abstract
Aim:
We sought to determine the epidemiology of mucinous ovarian tumors, the correlation between serum biomarkers and tumor status, and the outcomes of the management in different subtypes of mucinous ovarian tumors in a Chinese surgical cohort.
Methods:
A total of 513 patients were enrolled from January 2009 to May 2017. The number of patients who had benign mucinous ovarian tumor, borderline mucinous ovarian tumor, or malignant mucinous ovarian tumor was pathologically quantified. All patients underwent surgery with or without postoperative adjuvant therapy. Prognosis was analyzed based on clinicopathological characteristics and the type of treatment received. Hyperthermic intraperitoneal chemotherapy efficacy and adverse effects in patients were also explored.
Results:
In all, 383 (75%) patients were diagnosed as having benign mucinous ovarian tumor, 76 (14%) patients with borderline mucinous ovarian tumor, and 54 (5%) patients with malignant mucinous ovarian tumor. Levels of serum biomarkers increased as the tumors became more malignant. Patients with stage IA and IC (unilateral) malignant mucinous ovarian tumor who underwent fertility conserving surgery did not experience poorer prognoses when compared to those who received non-fertility conserving surgery. Hyperthermic intraperitoneal chemotherapy followed by chemotherapy significantly influenced survival rates in patients with a ruptured malignant mucinous ovarian tumor.
Conclusions:
Levels of serum tumor markers, carbohydrate antigen 125, carbohydrate antigen 199, carbohydrate antigen 242, and carcinoembryonic antigen may be useful in monitoring for malignant transformation. Fertility conserving surgery might be a preferable surgical procedure for patients with malignant mucinous ovarian tumor at early stage (IA and IC [unilateral]). Hyperthermic intraperitoneal chemotherapy appears to be a well-tolerated and promising postoperative adjuvant.
Keywords
Introduction
Ovarian tumors originating from the epithelial cell layer makes up about 65% to 75% of all types of ovarian tumors. 1 Histological variants of epithelial ovarian tumors include benign cystadenomas, borderline ovarian tumors (with low malignant potential), and invasive ovarian tumors. Of interest in this study are mucinous ovarian tumors, a subtype of epithelial ovarian tumors.
Mucinous ovarian tumors are rare types of gynecologic neoplasms. They exist along a spectrum ranging from benign mucinous ovarian tumors (BMOT), borderline mucinous ovarian tumors (BLMOT) to malignant mucinous ovarian tumors (MMOT). Primary MMOT accounts for 3% to 10% of all primary epithelial ovarian cancers. 2 Malignant mucinous ovarian tumor is classified as a type I tumor that has an unfavorable progression. Previous research has documented its progression from premalignant status to noninvasive status and its final manifestation as a full-blown invasive malignancy (Supplementary document 1).
All types of ovarian tumors have the risk of rupturing, while the subtype of mucinous tumor has a relatively big dimension enhancing the spillage risk. 3 Moreover, BMOT and BLMOT are unique, given their potential to behave in a malignant manner by leaking or rupturing intraperitoneally. This results in a complication known as pseudomyxoma peritonei, which is defined as the localized or ‘disseminated’ deposition of mucin in the peritoneal cavity. Abdominal and pelvic cavity seeding or ‘dissemination’ of mucin generally implies poorer outcomes. Previous reports 4 showed that women with stage III-IV MMOT had worse prognoses in contrast to women with other subtypes of epithelial ovarian cancers, after being matched for stage and other factors. Due to the rarity of this histopathologic type, the medical management of mucinous ovarian tumors and other types of ovarian tumors has historically been identical. Previous clinical trials regarding the use of chemotherapy in epithelial ovarian cancer involved patients with all types of ovarian tumors, without distinguishing between pathological subtypes. Mucinous ovarian tumors have only accounted for a small percentage of the study cohorts. Gynecologic Oncology Group (GOG) trials 111 only documented 14 (3.7%) of 410 enrolled patients with mucinous ovarian tumors. Similarly, the intergroup trial IV-10 (4.4%), GOG 132 trial (2.6%), and the GOG 186 trial (1.6%). 5
However, considering the differences in pathological characteristics, clinical behavior, and prognosis of mucinous ovarian tumors, many researchers have sought to uncover more effect means of managing patients with this tumor subtype.
Surgical removal of this tumor remains the gold standard of treatment. 6 Nevertheless, tumor recurrence rates are high, especially in the malignant subtype. Besides chemotherapy for MMOT, hyperthermic intraperitoneal chemotherapy (HIPEC) as a novel treatment has become an acceptable form of postoperative management in patients with peritoneal tumors. 7 Hyperthermic intraperitoneal chemotherapy has been used for ruptured BMOT/BLMOT, peritoneal pseudomyxomas, and MMOT for many years 7 and has been demonstrated to produce an affirmative cure.
Our objectives of this study were to determine the clinicopathologic characteristics, serum biomarkers, and prognosis of patients with mucinous ovarian tumors. Furthermore, we also recorded a different HIPEC protocol used in MMOT.
Materials and Methods
Data Collection
Clinical data from all patients that were diagnosed with mucinous ovarian tumor at the Henan province People Hospital from January 2009 to May 2017 were collected and reviewed retrospectively. A total of 513 patients with mucinous ovarian tumors were collected through the hospital pathology registry system. Standardized clinical data obtained from the hospital’s health record office were reviewed by clinicians. This study was approved by the Hospital Institutional ethics committee. Ovarian tumor diagnoses were made either by ultrasound and by computerized tomography (CT) or positron emission tomography scans combined with tumor biomarkers (carbohydrate antigen 125 [CA125], carbohydrate antigen 199 [CA199], and carcinoembryonic antigen [CEA]) pre-operation. The final diagnosis was confirmed by histopathological examination during and after surgery. Types of surgery performed included cystectomy, ovarectomy, tumor-debulking surgery, or comprehensive/non-comprehensive staging surgery. Staging was based on the International Federation of Gynaecology and Obstetrics (FIGO Staging System, 2015), which takes into consideration surgical findings and histopathological results.
Surgical results were categorized as optimal residual (satisfactory tumor-debulking) disease <1 cm or incomplete residual (unsatisfactory tumor-debulking) disease ≥1 cm for comprehensive cytoreduction.
After undergoing surgery, patients with late malignant stage disease were offered chemotherapy, while those who diagnosed with advanced disease (including having a ruptured tumor cyst or peritoneal pseudomyxoma) were recommended HIPEC (Cisplatin: doses of 90 mg at first day, 60 mg at third day, 60 mg at fifth day—all at precise controlled temperature of 42 °C, for 60 minutes). In these cases, a part of patients underwent HIPEC, while others refused these therapeutic strategies due to low economic status, older age, and any other personal consideration. Moreover, 3 consecutive HIPEC treatments were scheduled by doctors’ experience: The main reason was the tubes of HIPEC might be blocked with fibrous obstacles (such as fibronectin and red cells) if more HIPEC cycles undertaken, and the safety of harboring the tubes and the tolerance of HIPEC.
Parameters that were recorded included the histopathological subtypes, age, serum biomarkers, stages for malignant and BLMOTs groups, surgical procedures, postoperative management, tumor recurrence, and survival time. All computerized and written records were thoroughly reviewed, with the final cutoff for chart review of HIPEC treatment evaluation set between December 2012 and May 2017. All patients who received intravenous chemotherapy and HIPEC were monitored routinely for adverse events, such as myelosuppression, impairment of kidney, and liver function. Patients who were lost to follow-up after the initial operation were excluded in the analysis of prognosis. Patient status on the last follow-up session was classified as disease free, recurrent disease, or died.
Statistical Analysis
Data were analyzed by the Statistical Package for Social Sciences software (SPSS 19). Descriptive analysis was described as median ± SD for continuous variables. The difference between the groups was analyzed by analysis of variance or t test. Noncontinuous variable data were reported as median (interquartile range), and comparison between groups was done via nonparametric rank sum test. All enumerated data were presented as frequency, with comparison between groups done via the χ2 test or Fisher exact test. Survival rates were compared by log-rank test, and COX proportional hazards model was used to analyze the effect of multiple factors on survival time and survival outcome. A P value of <.05 was defined as statistically significant.
Results
Baseline Characteristics of Study Cohort
Table 1 displays the baseline characteristics of our patient cohort based on mucinous ovarian tumor subtype. The patients with MMOT had significant older age and higher rate of bilateral involving, tumor rupture, dissemination, and unsatisfactory tumor-debulking surgical procedures than BMOT and BLMOT (Table 1 and Figure 1B).
Baseline Patient’s Characteristics According to Tumor Subtype.
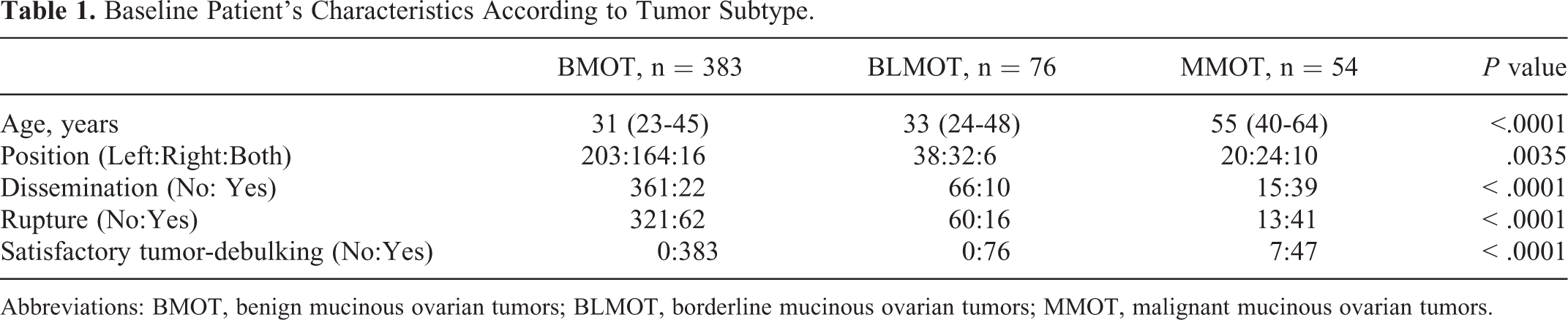
Abbreviations: BMOT, benign mucinous ovarian tumors; BLMOT, borderline mucinous ovarian tumors; MMOT, malignant mucinous ovarian tumors.

Frequency, patient age ranges, laterality, and size of different subtypes of mucinous ovarian tumor. A, Frequency of different subtypes of mucinous ovarian tumor. The pie chart on the left depicts the frequency of each subtype of mucinous ovarian neoplasm. The pie chart on the right depicts pathologic status of different subtypes of mucinous ovarian neoplasms. (a) BMOT; (b) BMOT with local hyperplasia active; (c) BMOT with partial of borderline neoplasm; (d) BLMOT; (e) local carcinogenesis; and (f) broad MMOT. B, Age ranges of different subtypes of mucinous ovarian tumor. C, Frequency of unilateral and bilateral mucinous ovarian neoplasms. D, Tumor sizes of different subtypes of mucinous ovarian neoplasms. Values of P < .05 are deemed to be statistically significant.
Frequency, Patient Age Ranges, Laterality, and Size of Different Subtypes of Mucinous Ovarian Tumors
Figure 1 depicts the frequency, patient age ranges, laterality, and size of different subtypes of mucinous ovarian tumors. A total of 74.66% of all the patients were found to have BMOT (Figure 1A, left), with 7.80% of those patients displaying active local hyperplasia (Figure 1A, right). A total of 14.81% cases were found to be BLMOT (Figure 1A, left). In all, 10.53% patients were found to have MMOT (Figure 1A, left), with 3.31% of those patients presenting with local carcinogenesis (Figure 1A, right, E). Benign mucinous tumors that were detected in our study ranged from between 2 and 30 cm in diameter (BLMOT: range 4-44 cm; Figure 1D). A large majority of mucinous ovarian neoplasms across all 3 subtypes are typically unilateral (Figure 1C).
Serum Biomarkers and Their Correlations With Different Status of Different Subtypes of Mucinous Ovarian Tumor
Figure 2 depicts the levels of serum biomarkers across different subtypes of mucinous ovarian tumors. It is clear that the serum biomarkers of CA125, CA199, CEA, and CA242 were gradually increasing due to the grade of ovarian mucinous lesion. The level of CA153 in serum was higher in cohort with malignancy than that in patients with BMOT and BLMOT subtypes. The levels of different serum biomarkers across different subtypes were also quantified (Table 2).

Serum levels of (a) CA125; (b) CA199; (c) CA153; (d) CA242; and (e) CEA for patient with different subtypes of mucinous ovarian tumor.
Tumor Marker Levels According to Tumor Subtype.a,b

Abbreviations: BMOT, benign mucinous ovarian tumor; BLMOT, borderline mucinous ovarian tumor; MMOT, malignant mucinous ovarian tumor.
a A, BMOT; B, BMOT with local hyperplasia active; C, BMOT with partial of borderline neoplasm; D, BLMOT; E, local carcinogenesis; F, broad MMOT.
b Values in italics indicate P values of less than < .05.
Surgical Procedures for Mucinous Tumors
In evaluating patient prognosis in this study, surgery was classified as either satisfactory or unsatisfactory tumor debulking.
In our patient cohort, 92.4% patients with benign tumor underwent fertility preserving surgery. Of these, 67% of patients selected cystectomy: 74.8% of those who chose cystectomy were subsequently diagnosed as disease free, with 17.9% lost follow-up. In all, 8.3% (33 patients) of our total patient cohort had recurrent disease. Two mortalities were recorded in this subgroup. Ruptured tumor or ‘metastatic’ mucinous tumor cells were found to be responsible for 22 of these 33 patients who were found to have recurrent disease. Of those who were diagnosed with recurrent disease, 25.4% chose to repeat surgery (unilateral salpingo-oophorectomy), with 3.4% of these patients again experiencing recurrent disease. Rates of recurrence of patients with BLMOT limited to ovarian and MMOT at stage I according to types of surgery are depicted in Table 3.
Rate of Recurrence According to Tumor Subtype.a

Abbreviations: BLMOT, borderline mucinous ovarian tumor; MMOT, malignant mucinous ovarian tumor.
a The patients with BLMOT and MMOT: The tumor was limited in ovarian, A: limited to unilateral ovarian, B: both ovarian involved, C: tumor ruptured.
In the group of patients diagnosed with early-stage malignant disease, 5 patients opted for unilateral salpingo-oophorectomy, and 3 patients received hysterectomy and bilateral salpingo-oophorectomy. All of the patients in this group were subsequently declared disease free.
Of 54 patients who were diagnosed with advanced stage MMOT, 44 underwent complete surgical resection per standard ovarian cancer surgery protocol. Two patients received incomplete surgical resection, as they were either unwilling to undergo total resection or experienced other logistical issues. All patients were followed up in a timely manner and were subjected to meticulous clinical examination by the attending clinicians.
Adjunctive Postoperative Management
Among the 22 patients with secondary recurrent BMOT, 14 were found to have peritoneal pseudomyxomas: 3 of these patients with recurrent disease underwent HIPEC and had disease-free interval times of 22.2, 30.2, and 36 months. Meanwhile, 11 patients with no further treatment had disease-free intervals that ranged between 6 and 18.5 months. One of these patients died 3 months after surgery.
All 46 of our patients with stage III-IVA MMOT received oxaliplatin-based chemotherapy given intravenously. The basic characteristics of stage III-IVA patients are presented in Supplementary document 2, and 20 of them received 1 cycle of HIPEC prior to commencing chemotherapy.
Evaluation of Efficacy and Toxicity of HIPEC
Investigations for the presence of HIPEC toxicity are shown in Supplementary document 3. Only the number of red blood cells reached a significantly worse difference in patients with HIPEC than that in cases without HIPEC. A promising overall survival trend of patients with advanced MMOT who received HIPEC was observed (Figure 3).

Survival curves of patients with advanced stage malignant mucinous ovarian tumor (MMOT) with/without HIPEC.
Prognosis for Patients With Mucinous Tumors
The 5-year survival rate for all subtypes of mucinous ovarian carcinomas was about 54%. This was increased to 93.7% in those with BLMOT. Laterals ovarian involving tumor dissemination, rupture, and unsatisfactory tumor-debulking were worse prognostic factors for survival rate (Table 4).
Survival Results.a

Abbreviations: BMOT, benign mucinous ovarian tumors; BLMOT, borderline mucinous ovarian tumors; MMOT, malignant mucinous ovarian tumors; N, Number.
a Statistical analysis was done via log-rank test. Values in italics Indicate P values of less than <.05.
Discussion
In this study, we sought to determine the epidemiology of mucinous ovarian tumors and its different subtypes in a Chinese surgical cohort. We investigated for possible correlations between cancer serum biomarkers and the tumor status. We also looked at different types of surgery and their respective patient outcomes and survival rates. Finally, we also sought to determine the safety profile of HIPEC when used as a postoperative adjuvant.
There exist many discrepancies in the literature regarding the epidemiology of primary ovarian mucinous tumors. Seidman et al 8 reported that 3.4% patients had primary mucinous ovarian cancer in a cohort of 220 patients with epithelial ovarian cancers in the United States. On the other hand, Shimada et al 9 found a low percentage of invasive primary mucinous ovarian tumor at 4.9% in a cohort of 1400 patients with epithelial ovarian cancer in 14 Japanese centers.
In our study, a total of 383 patients with BMOT were identified with a median age of 31 years. On the other hand, a total of 76 patients were found to have BLMOT, with a median age of 33 years. The age of patients with BLMOT in our data (13-79 years) was similar to ranges reported in Loizzi et al 10 (13-79 years). However, the median age for BLMOT in our study cohort was lower than reported in previous studies. Romeo et al 11 and Loizzi et al 10 both reported a median age for patients with BLMOT at 47.7 and 40 years, respectively. These differences may be attributed to intrinsic demographic or population characteristics.
We noted from our observations that patients with local mucinous ovarian carcinoma are rare and are more often detected in those younger than 30 years of age. On the other hand, patients with malignant ovarian mucinous tumors were more likely to be elderly. In all, 71% of our patients with this subtype of ovarian tumor were found to be over the age of 55 years. Based on these findings, we conclude that increasing age is associated with an increased risk of developing advanced lesions.
Both BMOT and BLMOT that were detected in our study ranged from 2 to 44 cm in diameter. Jubilee et al 4 reported a slightly larger average size of primary MMOT between 16 and 20 cm in diameter (range, 5-48 cm). Mucinous ovarian tumors have the ability to grow into large sizes. 3 However, a large tumor volume does not necessarily imply malignancy, as many may remain clinically asymptomatic. It is not uncommon for smaller cysts to be discovered incidentally during caesarean sections.
Our data also showed that 95.84% of BMOT diagnosed in our cohort were unilateral, with only 4.18% bilateral tumors were detected. This is lower than previous studies that reported a 10% occurrence of bilateral tumors. 12 There exists a previously proposed algorithm that aims to determine the type of mucinous ovarian tumors based on laterality and size. 3,13 It predicts a mucinous ovarian tumor as primary if it is unilateral and more than 10 cm and as metastatic if there are bilateral tumors or if tumors are unilateral and less than 10 cm. However, our data do not appear to fully support this algorithm.
In our study, 6 serum biomarkers were measured and their concentrations analyzed with respect to the various histological status in the benign to malignant progression of mucinous ovarian tumors. Our results revealed significantly different levels of 4 biomarkers among these subtypes. Levels of CA125, CEA, CA199, and CA242 were significantly increased in patients with malignant ovarian cancer. There appeared to be an increasing trend of serum biomarker concentrations, as ovarian lesions progressed from benign to malignant. Levels of CA125 levels were found to increase significantly, as mucinous ovarian tumors progressed toward malignancy. The median values for BMOT, BLMOT, and MMOT were found to be 11.78 µ/mL, 15.83 µ/mL, and 63.27 µ/mL, respectively. Similar increasing trends were noted to be statistically significant in CA199, CEA, and CA242 values but not in CA153.
Pretreatment concentration levels of serum biomarkers have been regarded as a potential predictive tool for distinguishing between malignant and nonmalignant lesions. These biomarkers have also been investigated as a method of surveillance during postoperative follow-up. Generally, CEA is used as a serum biomarker for MMOT. As in our study, CEA has previously been found to be elevated in 88% of patients with MMOT but not in their non-mucinous counterparts. 14 -16 Other serum biomarker that has been explored is human epididymis protein 4 (HE4). 17,18 However, existing data on HE4 are scarce and was not investigated in this study.
CA199 has been reported to correlate well with borderline and malignant subtypes of ovarian tumors but not with BMOT. Previous studies have reported that it is more useful as a tumor marker in the presence of a normal CA 125 level. 19 CA242 is a diagnostic biomarker for pancreatic and colorectal cancers, and its overexpression can be detected from tumor cell surfaces and serum. 20 Our data suggest that CA242 might be a novel biomarker associated with the progression of mucinous ovarian tumors. Nevertheless, its sensitivity, specificity, and prognostic values in distinguishing between primary and metastatic ovarian tumors require further exploration.
In our study, we were unable to thoroughly investigate the trends of serum biomarkers in patients during follow-up. The relationship between serum biomarkers and patient prognosis requires further exploration in future studies.
The surgical managements of mucinous and non-mucinous ovarian tumors are similar due to the rarity and lack of clinical evidence in mucinous ovarian tumors. Surgical managements can be categorized into fertility-sparing and non-fertility sparing surgery.
Fertility-sparing surgery revolves around removing the tumor and the affected ovary only while aiming to conserve the uterus and at least one ovary and its adnexa. Meanwhile, non-fertility sparing surgery involves removal of the tumor and comprehensive tumor staging. Comprehensive staging surgery consists of total hysterectomy, bilateral salpingo-oophorectomy, omentectomy, appendicectomy, and lymph nodectomy, including pelvic and para-aortic lymph nodes. 21
Laparotomy is generally the preferred surgical method (regardless of whether it is fertility sparing or non-fertility sparing) in the removal of ovarian tumors. This is due to the large size of most mucinous ovarian tumors. Furthermore, an open laparotomy allows better visualization and clearance of the entire abdominopelvic cavity in the event of a cyst rupture. Factors that influence the choice of surgery include tumor grade, tumor location, and whether the tumor affects one or both ovaries as well as patients’ desire for fertility. 22,23
Patients with BMOT can experience high survival rates if detected and managed appropriately. In a study comparing both fertility-sparing and non-fertility sparing procedures, Melamed et al 24 found that fertility-sparing surgery was a favorable option for younger patients with stage IA or unilateral IC mucinous epithelial ovarian cancer and was not associated with an increased risk of death.
Our results mirrored findings by another study that demonstrated no significant difference in 5-year overall survival rates and disease-free survival rates among patients with IA and IC stage that were both treated with fertility sparing surgery (Overall survival, P = .180, disease-free survival, P = .445). 25 The same study revealed that patients with stage IA and IC disease who underwent fertility-conserving surgery did not experience poorer prognoses when compared to those who received non-fertility conserving surgery. 25 In our study, a total of 5 patients with stage I disease received fertility-sparing surgery. No recurrence of disease was observed in this cohort upon follow-up.
It appears that the different choice of fertility-sparing surgery has an impact on patient prognosis. Koskas et al 26 demonstrated that women with BLMOT who received unilateral salpingo-oophorectomy experienced significantly higher 5-year disease-free survival rates compared to those who received a cystectomy. Women who received unilateral salpingo-oophorectomy also experienced lower risk of recurrence. This procedure has been found to not affect fertility. 26
Like other non-mucinous ovarian tumors, the first-line treatment for patients with MMOT has been platinum-based chemotherapy. 27 However, recent evidence has demonstrated significantly lower response rates in patients with advanced stage primary MMOT who were treated with platinum-based chemotherapy. Shimada et al recorded a 12.5% response rate in their cohort of patients with invasive MMOT compared to the 67.7% response rate in those who had serous ovarian adenocarcinoma. 9 Similarly, Pectasides et al also observed a 38.5% response rate in those with MMOT compared to a 70% response rate in those with serous ovarian carcinoma. 28 However, both studies did not report survival differences between the 2 types of ovarian carcinomas. 9,28
Recurrent MMOT has also been shown to be platinum resistant. Pignata et al 29 demonstrated that recurrent MMOT were less responsive to platinum-based regimens compared to their nonmucinous counterparts (36% vs 63%, respectively, P = .04). Progression-free survival of those with recurrent MMOT and nonmucinous carcinomas was 4.5 months and 8 months, respectively (P < .05). Additionally, those with MMOT had a shorter overall survival time of 17.9 months, compared to the 28.8 months of those with non-mucinous carcinomas (P = .003). 29
Advanced mucinous ovarian carcinoma has been documented to be highly chemoresistant. However, we do not agree with previous authors who have suggested complete resection of peritoneal metastasis does not reverse poor prognosis. 30 While tumor debulking procedures may be beneficial in terms of symptom control for late stage BLMOT and MMOT, the lack of HIPEC administration may result in poorer prognoses despite the presence of complete cytoreduction. 31 Our results show that combined HIPEC and chemotherapy administration significantly enhanced survival rates of those with advanced MMOT. These findings are congruent with those found by Tewari et al. 32 Moreover, previous study indicates HIPEC combined cytoreductive surgery improves survival in patients with diffuse peritoneal ovarian carcinomatosis (including primary and recurrent epithelial ovarian cancer). 33 -36 Concurrent cytoreductive surgery and HIPEC administration have also been shown to improve the survival rates in patients with pseudomyxoma peritonei (PMP), although the pathological subtype of PMP remains a crucial factor that influences outcomes. 31,37,38 Very recently, a multicenter, open-label, randomly controlled, phase 3 trial study demonstrates that the addition of HIPEC to interval cytoreductive surgery resulted in longer recurrence-free survival and overall survival than surgery alone in the patients with epithelial ovarian cancer at stage III (median overall survival, 45.7 months vs 33.9 months). The percentage of patients who experienced adverse side effects of grade 3 or 4 was similar in these 2 groups. 39 Our data are consistent with previous reports indicating that HIPEC is well tolerated by patient cohort 33 even when administered concurrently with chemotherapy in our cohorts. Furthermore, the literature demonstrates novel techniques, such as minimally invasive route and hybrid CO2 system, which might enhance the efficacy of HIPEC. 40,41
Mucinous ovarian tumors have been shown to have a poorer prognosis and higher rate of recurrence compared to other subtypes of ovarian tumors. In this study, the median follow-up period for patients from all 3 subtypes of ovarian cancer was between 6 and 101 months.
Finally, we also depict the correlation between tumor rupture and recurrence to its diameter in centimeters (Supplementary document 4). Most of our study patients presented with unruptured cysts. Some of these cysts had reached large sizes without rupturing. We conclude from our observations that there is no significant correlation between whether a tumor is ruptured or recurrent and its diameter. Even benign tumors that were between 15 and 30 cm in diameter displayed promising survival rates during our period of observation. The 5-year survival rate for all subtypes of mucinous ovarian carcinomas was about 54%. This was increased to 93.7% in those with borderline mucinous tumors (Table 4). If treated early or in its unruptured state, benign ovarian mucinous tumors have an overall survival rate of almost 100% and a much lower recurrence rate.
Patients with BMOT and BLMOT tended to present at a younger age compared to invasive MMOT. A large tumor volume was not shown to be predictive of its malignant potential. However, it was noted that patients with BLMOT and BMOT had larger tumor sizes. Bilateral ovarian involvement was more common in patients with MMOT. Serum biomarkers CA199, CA125, CEA, and CA242 displayed increasing trends that correlated with increasing tumor malignancy. Patients with advanced MMOT experienced longer survival times, possibly due to the combination of cytoreductive surgery, HIPEC, and chemotherapy administration. Postoperative HIPEC administration should be considered as it has been shown to impart tolerant toxicity and higher overall survival times. Follow-up periods should be sufficiently long to cater to the high recurrence rates of mucinous ovarian tumors.
Study Limitations
One of the major limitations of this study is the lack of patients with MMOT, despite the large sample size. Furthermore, our study was performed retrospectively with patients collected only from a single center. The formation of a multi-institutional registry would greatly facilitate future research. Other limitations include our focus on HIPEC administration only in those with advanced stage MMOT. We were unable to obtain sufficient numbers of patients with ruptured or ‘disseminated’ BMOT and BLMOT that received HIPEC. Finally, future studies would benefit from having longer patient follow-up times in order to thoroughly document the effects of HIPEC.
Supplemental Material
Supplemental Material, Supporting_Informations - Retrospective Study of the Epidemiology, Pathology, and Therapeutic Management in Patients With Mucinous Ovarian Tumors
Supplemental Material, Supporting_Informations for Retrospective Study of the Epidemiology, Pathology, and Therapeutic Management in Patients With Mucinous Ovarian Tumors by Yuanyuan Zhang, Chunmei Li, Suiyu Luo, Ying Su, Xiaoqing Gang, Peiyuan Chu, JuXin Zhang, Henghui Wu and Guangzhi Liu in Technology in Cancer Research & Treatment
Footnotes
Abbreviations
Authors’ Note
Yuanyuan Zhang and Chunmei Li contributed equally to this article. This study was approved by the Ethics Committee of Henan Provincial People’s Hospital (approval no. STIP144200510027). All patients provided written informed consent prior to enrollment in the study. The attachment states that this study has passed the ethical examination and approval by Ethics Committee of Henan Provincial People’s Hospital; the written informed consents of this study were signed by all involved patients and documented in their medical records.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research funding from the Science and technology innovation project of Henan province. (No.144200510027); National Natural Science Foundation of China (No. 81601261).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.