
Abstract
Purpose:
To explore the clinical value of ultrasound in the diagnosis of medullary thyroid carcinoma by comparing with enhanced computed tomography.
Methods:
This retrospective study was performed on 62 patients with pathologically confirmed medullary thyroid carcinoma. All patients underwent ultrasound and enhanced computed tomography examinations before surgery. The findings of the pathologic examination of resected specimens were considered as gold standard and were compared with the results of these 2 methods.
Results:
There were 73 medullary thyroid carcinoma lesions and 29 benign lesions in 62 patients. In all, 55 of 73 medullary thyroid carcinoma lesions and 27 of 29 benign lesions were correctly diagnosed by ultrasound; and 45 of 73 medullary thyroid carcinoma lesions and 24 of 29 benign lesions were correctly diagnosed by enhanced computed tomography. The accuracy of ultrasound and enhanced computed tomography was 80.4% and 67.6%, respectively. There was significant difference between 2 methods (P < .05).
Conclusions:
Ultrasound can be used to observe the location, number, size, shape, border, internal echo, calcification, and blood flow of the lesion. It is a convenient, inexpensive, and nonradiative method with higher accuracy than enhanced computed tomography.
Introduction
Thyroid cancer is one of the most common malignant tumors of the neck. The incidence of the disease is increasing in recent years. Medullary thyroid carcinoma (MTC) is a rare form of thyroid cancers, originating from thyroid follicular C-cells and accounts for approximately 5% to 8% of all thyroid malignancies. 1,2 The growth of MTC is relatively slow, but if metastasized or relapsed, it becomes very aggressive causing more than 13% of all thyroid cancer-related mortality. 3 Therefore, it is important to diagnose MTC prior to surgery.
The ultrasound (US) characteristics of thyroid malignancies have been recently accumulated, but most reports are basically focused on the diagnosis of papillary thyroid carcinoma (PTC), and only limited data are available regarding the US criteria for possibly malignant MTCs. 4 -7 Moreover, the studies of enhanced computed tomography (CT) on MTC are rare and there is no report about the comparison of US and enhanced CT. In this retrospective study, we compared the accuracy of US and enhanced CT to explore the diagnostic value of US for MTCs.
Materials and Methods
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Research Ethics Committee of our Hospital. Informed consent was obtained from all patients.
Patients
Between January 2008 to June 2018, 91 consecutive patients were diagnosed with MTC in our hospital. The inclusion criteria for the study were: (1) not treated with radiotherapy previously, (2) underwent both US and enhanced CT examinations, and (3) results were confirmed by surgery. The final study group consisted of 62 patients (36 females, 26 males, mean age 49.3 ± 8.1 years [range 29-72]) with 73 MTC nodules and 29 benign nodules. All cases complained of masses found in the neck. Calcitonin increased (>300 pg/mL) in 49 cases; 25 cases presented hoarseness; and 10 cases had endocrine symptoms such as diarrhea.
Ultrasound Technique
Ultrasound examinations were performed with HDI 5000 (Philips Medical Systems, Bothell, Washington) or GE E8 (GE Healthcare, Wauwatosa, Wisconsin) scanner. The probe frequency ranged from 5.0 to 12.0 MHz. Transverse, longitudinal, and oblique plane sonographies of the thyroid and the cervical lymph nodes were obtained. These preoperative images were analyzed by 2 sonographers. Both of them had more than 10 years of experience and were blinded to the patients’ clinical data, other imaging findings, and pathology results at the time of the analysis. When the diagnosis of the 2 sonographers differed, the final diagnosis was decided after discussion.
The 2-dimensional gray-scale images were used to observe the location, number, size, border, shape, internal echo, and calcification of the lesion. The color-flow Doppler (CFD) was used to observe the blood flow of the lesion. According to the American Association of Clinical Endocrinologists/Associazione Medici Endocrinologi /European Thyroid Association guidelines, 8 nodular US classification was made by size (≥1 cm or <1 cm), height/width ratio (≥1 or <1), echogenicity (hypoechoic, isoechoic, hyperechoic), nodule margins (regular or irregular), presence of microcalcifications (defined as hyperechoic spots <2 mm), and macrocalcifications. The patterns of nodular vascular signal were assessed by CFD and defined as follows: (1) CFD-1, as absent signal; (2) CFD-2, as a perinodular signal; and (3) CFD-3, as an intranodular signal. 9 Malignant sonographic features were defined as an irregular margin, marked hypoechogenicity, microcalcifications, and taller-than-wide shape. 10 The MTC nodules were solid, hypoechoic, absent of peripheral halo, presenting calcification, and cervical lymph node metastasis. Compared with PTC nodule, MTC nodule was characterized by larger size, clear boundary, less taller-than-wide shape, coarse calcification, and enhanced intranodular blood flow. 11
Computed Tomography Technique
Computed tomography examinations were performed on a Philips Brilliance 16-slice spiral CT (Philips Medical Systems). The scanning parameters are as follows: collimation width 0.625 × 16 mm, pitch 1.0, tube voltage 120 kV, tube current 130 to 200 mAs, thickness of 3 mm, and reconstruction layer thickness of 1 to 2 mm. Contrast agent was iopromide injection 370 (iodine concentration 370 mg/mL). After routine scanning, 80 to 100 mL contrast agent was injected at a velocity of 3 mL/s. Arterial and venous enhancement was performed at 25 and 65 seconds after injection. The MTC nodules were hypodense solid masses with rare necrosis, usually demonstrated coarse calcifications and metastasized to lymph nodes in the neck and mediastinum. After injection of contrast agents, most MTC nodules were slightly nonuniformly enhanced or not enhanced. All the preoperative images were analyzed by 2 radiologists. Both of them had more than 10 years of experience and were blinded to the patients’ clinical data, other imaging findings, and pathology results at the time of the analysis. When the diagnosis of the 2 radiologists differed, the final diagnosis was decided after discussion.
Statistical Analysis
The findings of the pathologic examination of resected specimens were considered as gold standard and were retrospectively compared with the results of US and enhanced CT. Data analysis was made by using SPSS version 22.0 software. The change of diagnostic accuracy rate from US to enhanced CT was assessed by McNemar test, P < .05 was considered to indicate a statistically significant difference.
Results
There were 73 medullary carcinoma lesions and 29 benign lesions in 62 patients. Malignancy invaded 1 lobe of thyroid in 49 cases, invaded 2 lobes in 13 cases, involved the isthmus in 9 cases. The size of the maximal malignant lesion was 5.2 × 2.8 × 3.9 cm, the size of the smallest one was 0.8 × 0.6 × 0.6 cm; 26 (41.9%) cases combined with other kinds of nodules; 34 (54.8%) cases had cervical lymph node metastasis; 11 (17.7%) cases had distant metastasis, including 8 cases with bone metastasis and 3 cases with lung metastasis.
A summary of the sonographic findings of MTCs is presented in Table 1. Of all 73 MTC nodules, 32 nodules located in the left lobe of the thyroid and 41 nodules located in the right lobe; 31 nodules located in the upper pole of the lobe of thyroid gland, 29 nodules in the middle, and 13 nodules in the lower pole. The majority of the MTCs had an irregular shape (67.1%), a height/width ratio of <1 (76.7%; Figure 1), a clear border (64.4%), no peripheral halo sign (83.6%), hypoechogenicity (91.8%; Figure 2), heterogeneous echotexture (71.2%), calcification (61.6%), and perinodular vascular signal pattern (71.2%; Figure 3). The majority of calcification in the MTCs was macrocalcification (62.2%; Figure 4).
The Sonographic Findings of 73 MTC Nodules.

Abbreviations: CFD, color-flow Doppler; MTC, medullary thyroid carcinoma.

Ultrasound image of medullary thyroid cancer (MTC) from a 37-year-old man. The tumor showed predominantly solid, ovoid shape, iso- to hypoechoic echogenicity, well-defined margin, and height/width ratio <1.

A 49-year-old woman with medullary thyroid cancer (MTC) located in the left lobe of thyroid. The tumor was solid, round in shape, and had hypoechoic echogenicity compared with the normal thyroid parenchyma.

A 52-year-old man with medullary thyroid cancer (MTC) located in the right lobe of thyroid. The color-flow Doppler (CFD) showed hypervascularity as perinodular vascular signal pattern.

A 57-year-old woman with medullary thyroid cancer (MTC) located in the right lobe of thyroid. A, The gray scale sonography showed the macrocalcification presented in the mass(arrow). B, The color-flow Doppler (CFD) showed there is no obvious vascular signal in the lesion.
Enhanced CT findings of MTCs: 73 nodules were all performed as hypodense masses in thyroid gland before enhancement. The density was homogeneous in 54 cases. The density was heterogeneous in 19 cases; 24 nodules were obviously enhanced and became hyperdense relative to the anterior cervical muscles after administration of contrast agents, other nodules were not enhanced or slightly enhanced (Figure 5). Calcification was found in 44 nodules, of which coarse calcification presented in 29 nodules and psammomatous calcification presented in 15 nodules.
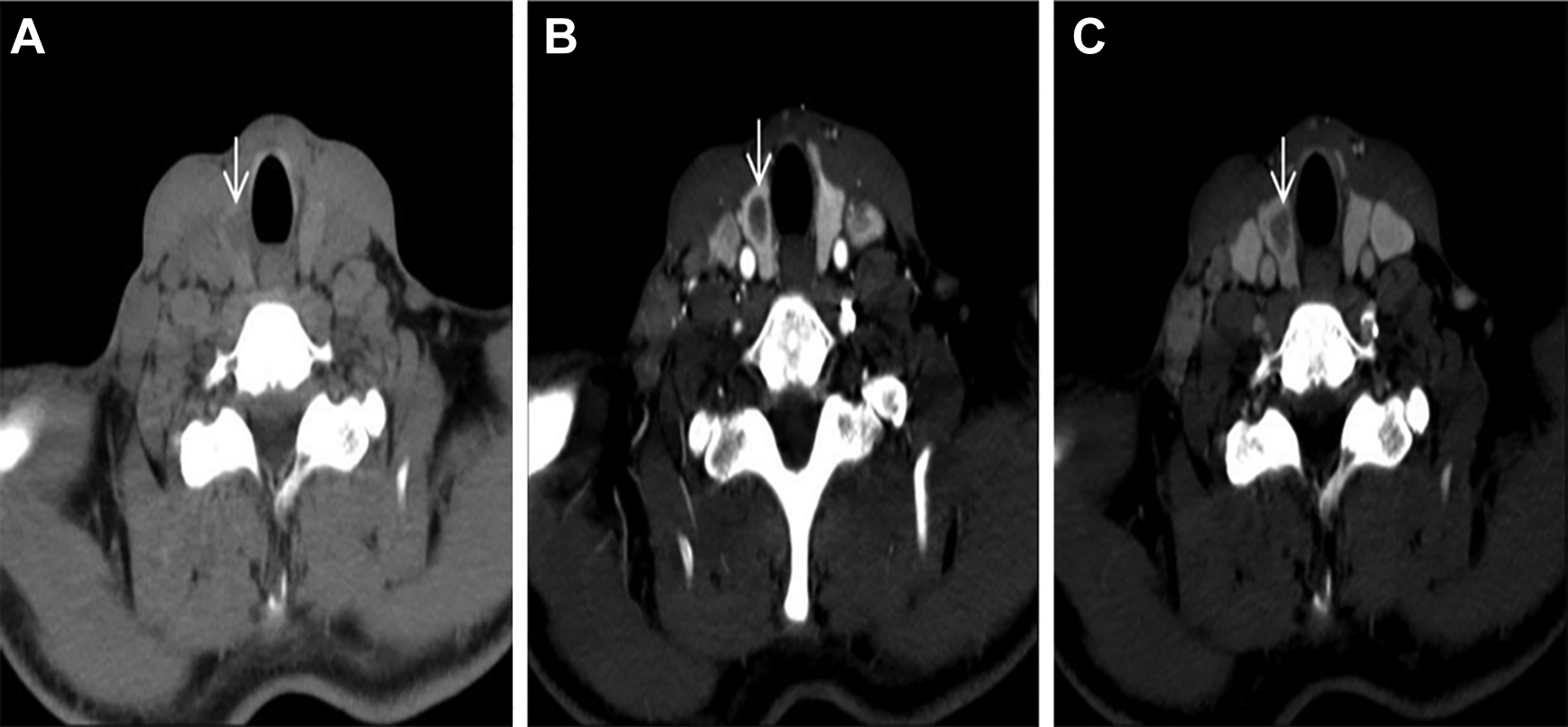
Computed tomography (CT) images of medullary thyroid cancer (MTC) in right thyroid gland. A, Axial CT scan without contrast through the thyroid gland revealed a hypodense mass. B and C, Axial enhanced CT showed the lesion (arrows) was slightly enhanced during the arterial phase and delayed phase.
In all, 55 of 73 MTC lesions and 27 of 29 benign lesions were correctly diagnosed by US. The sensitivity of the sonographic classification was 75.3%, specificity was 93.1%, positive predictive value was 96.5%, negative predictive value was 60.0%, and the overall accuracy was 80.4%. In all, 45 of 73 MTC lesions and 24 of 29 benign lesions were correctly diagnosed by enhanced CT. The sensitivity of the classification based on enhanced CT was 61.6%, specificity was 82.8%, positive predictive value was 90.0%, negative predictive value was 46.2%, and the overall accuracy was 67.6% (Table 2). There was significant difference between the accuracy of 2 methods (P = .015; Table 3).
Diagnostic Index of US and CT for Diagnosing MTC.

Abbreviations: CT, computed tomography; MTC, medullary thyroid carcinoma; NPV, negative predictive value; PPV, positive predictive value; US, ultrasound.
Comparison of the Accuracy of US and CT.a

Abbreviations: CT, computed tomography; US, ultrasound.
a P = .015.
Discussion
The most common cancer of the endocrine system is thyroid carcinoma. Thyroid carcinoma is classified into several subtypes: papillary, follicular, medullary, and undifferentiated (anaplastic). 12 Each histological subtype of thyroid carcinoma has its different and varied biologic behavior. Medullary thyroid carcinoma is a poorly differentiated, neuroendocrine tumor which arises from the C-cells of the thyroid gland. It is a relatively slow-growing malignancy, but at the time of initial diagnosis, a locoregional metastasis has already taken place, and a distant metastasis is present in 13% to 35% of patients. 11,13 -16 The most common sites of distant metastasis include the lungs, liver, and bones; and metastasis rarely presents in the brain, skin, and breast. 17,18 So early detection and early diagnosis are essential. Many imaging modalities can be used to detect MTCs and provide radiologic evaluation, including US, CT, magnetic resonance imaging, and nuclear scintigraphy. In this article, we compared the accuracy of 2 imaging methods (US and enhanced CT) in the diagnosis of MTCs according to the results of postoperative pathology. And we found that the accuracy of US was 75.3%, which was better than that of enhanced CT.
The MTC has some general sonographic features which are associated with a higher likelihood of malignancy, including irregular infiltrative margins, an absent halo sign, hypoechogenicity, and the presence of calcification. Lai et al 19 reported that 96.9% of the MTC nodules were hypoechoic, 72.4% of the nodular shape were irregular, 93.7% of the nodules had no peripheral halo, and 63.8% of the nodules presented calcification. Saller et al 20 compared the ultrasonographies of 19 MTC nodules and 139 benign nodules. They found that 89% of the MTC nodules were hypoechoic, absent of peripheral halo, and presenting calcification; and only 6% of benign nodules had these 3 characteristics as a control group. In agreement with the results of the previous reports, we found in this study that 91.8% of the MTCs were hypoechoic, 67.1% exhibited irregular shape, 83.6% had no peripheral halo, and 61.6% presented calcification. That is to say, MTC has some ultrasonographic characteristics which are similar to PTC. But MTC has its special sonographic performance according to this study: More than half of the MTCs had clear boundary (64.4%); most of MTCs height/width ratio were less than 1.0 (76.7%); and macrocalcification presented more common than microcalcification in MTCs (62.2% vs 37.8%).
Computed tomography is the preferred modality in the investigation of the neck including thyroid tumors. 21 Axial sections 3- to 5-mm thick should be obtained. The CT evaluation should include assessment of marginal definition, cyst formation, hemorrhage, necrosis, calcification of the lesion, extraglandular extension, and metastatic lymph nodes. 22 The MTCs are hypodense solid masses on CT and may demonstrate coarse or psammomatous calcifications and metastasize to lymph nodes in the neck and mediastinum in up to 50% of cases. 23 Necrosis of the MTCs is rare. Distant metastases may settle in the lungs, liver, and bone. After administration of contrast agents, the majority of the MTCs were slightly enhanced or not enhanced in this study. The MTCs originate from the C-cells and do not usually take up iodine, 23 so these tumors are hypodense to the surrounding normal thyroid tissues which can absorb iodine. Relatively abundant blood supply may contribute to the rarity of necrosis of the tumors. These characteristics of the MTCs are different from those of the PTCs (isodense; obviously enhanced; necrosis is common).
In our study, 18 of 73 MTCs were misdiagnosed by US, 28 of 73 MTCs were misdiagnosed by enhanced CT. The special performances of the MTCs which differ from general malignancy on US and enhanced CT are the possible reasons for the MTCs being misdiagnosed as some benign lesions.
There are some limitations of our study. As our study was a retrospective study, evaluating the sonographic findings in real time, which might provide more information, was impossible, and the interpretive results of images might vary among different sonographers or radiologists. Second, elastography and contrast-enhanced ultrasonography of MTCs were not contained in this study and this is the subject of ongoing research.
Conclusions
In conclusion, US examination is a convenient, inexpensive, and nonradiative method with higher accuracy than enhanced CT. It can be used to observe the location, number, size, shape, border, internal echo, calcification, and blood flow of the MTC. It should be used as the first choice of imaging modality to guide the treatment algorithms.
Footnotes
Acknowledgments
We would like to thank Dr Fuguang Huang for his help in finishing this study. And we wish to thank our colleagues in the Department of Radiology and the Department of Pathology for their cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.