
Abstract
Chronic myeloid leukemia is a myeloproliferative neoplasm that occurs more prominently in the older population, with a peak incidence at ages 45 to 85 years and a median age at diagnosis of 65 years. This disease comprises roughly 15% of all leukemias in adults. It is a clonal stem cell disorder of myeloid cells characterized by the presence of t(9;22) chromosomal translocation, also known as the Philadelphia chromosome, or its byproducts BCR-ABL fusion protein/messenger RNA, leading to the expression of a protein with enhanced tyrosine kinase activity. This fusion protein has become the main therapeutic target in chronic myeloid leukemia therapy, with imatinib displaying superior antileukemic effects, placing it at the forefront of current treatment protocols and displaying great efficacy. Alternatively, nanomedicine and employing nanoparticles as drug delivery systems may represent new approaches in future anticancer therapy. This review focuses primarily on the use of organic nanoparticles aimed at chronic myeloid leukemia therapy in both in vitro and in vivo settings, by going through a thorough survey of published literature. After a brief introduction on the pathogenesis of chronic myeloid leukemia, a description of conventional, first- and second-line, treatment modalities of chronic myeloid leukemia is presented. Finally, some of the general applications of nanostrategies in medicine are presented, with a detailed focus on organic nanocarriers and their constituents used in chronic myeloid leukemia treatment from the literature.
Introduction and Clinical Features
Chronic myeloid leukemia (CML) is a neoplasm that affects mature myeloid cells, especially granulocytes and their precursors. It results from the reciprocal translocation of the ABL gene on chromosome 9 to the BCR gene on chromosome 22, that is, t(9;22) forming the Philadelphia chromosome (BCR-ABL gene fusion). 1,2 Consequently, tyrosine kinase activity is expressed constitutively, leading to the phosphorylation and activation of various downstream proteins that promote cellular proliferation and simultaneous inhibition of apoptosis. 3
Chronic myelogenous leukemia represents roughly 15% of leukemias in the adult population, with an incidence of 1 to 2 new cases per 100 000 individuals 4 and a median age of diagnosis of 60 to 65 years. 5
The most common clinical presentation of CML is an incidental finding in an asymptomatic patient, representing 50% of patients with CML. 6 Additionally, even in symptomatic patients, symptoms are largely nonspecific.
They can range from dyspnea on exertion or fatigue due to anemia, to left upper quadrant pain and early satiety from splenomegaly. Rarely, 5% of patients may present with symptoms of headache, retinopathy, and vertigo among others, owing to the hyperviscosity syndrome from the large-scale leucocytosis. 7
Regarding treatment, the most widespread therapeutic approach for CML is the use of imatininb, a tyrosine kinase inhibitor (TKI). 8 Nonetheless, TKIs do not offer a cure for CML. Rather, a bone marrow transplantation is required for cure. 8 Additionally, current treatment protocols are hampered by drug resistance and cancer relapse. 9 For this reason, the combination of newer agents with existing ones offers a new prospect to address cancer cells’ resistance to drugs, cancer recurrence, and importantly a cure without the need for transplantation. Of these strategies, nanotechnology is emerging as a possible new approach in the management of CML. 10
Multidrug resistance (MDR) emerged as a major reason of chemotherapy failure and relapse in hematological neoplasms. Specifically, cancerous cells develop resistance against the cytotoxic effects of various drugs, through a complex mechanism involving different pathways. To note, resistance developed to one drug is not specific to that drug only and may involve multiresistance. 11 One pathway involved is the downregulation of the production of apoptosis-related proteins, such as Bax and B-cell lymphoma-2 (Bcl-2). 12 Other mechanisms affect recovery from drug-induced DNA damage, drug excretion, and alterations in the activity of enzymes functioning in drug metabolism. 13
Drug excretion via P-gp, the permeability glycoprotein, remains the most important mechanism of resistance. 14 In essence, it is an adenosine triphosphate–dependent transmembrane efflux pump encoded by the Mdr1 gene, which functions to decrease intracellular drug concentrations through active transportation of drugs out of the cells. 15 -17 This overexpression of Mdr1 increases resistance to drugs and consequently increases the chance of cancer recurrence, a sign of worse prognosis. 18
A promising new approach to combat resistance is through the use of nanoparticles (NPs) as drug delivery systems. This review aims to collect and discuss current advancements in organic nanomedicine, in which organic NPs are made to function as drug delivery systems for the treatment of CML, with a focus on both the chemical properties of NPs and their clinical applications.
Nanomedicine in CML Treatment
Designing a drug delivery system is a complex process requiring several steps be taken to ensure success. The delivery system must be developed in a way that balances efficiency in delivery and preservation of drug bioactivity.
Moreover, adequate loading and release of the drug must be ensured through the control of the kinetics of both drug loading and release. 19,20 Herein lies the advantage in using NPs as delivery systems, as they enhance the intracellular uptake of the drug, improve water solubility of the drug in cancer cells, and enhance circulation time of the drug. Importantly, NPs allow sparing of normal cells from the cytotoxic effects of drugs through their targeted delivery system. 21,22 As such, chemotherapeutic drugs loaded into NPs can resist degradation, display lower toxicity, and show enhanced solubility and efficacy. 23 -25
However, NP use is not without its own complexities. Both intrinsic properties, such as surface charge, particle size and shape, zeta potential, and surface area, as well as extrinsic properties, such as the activity of the reticuloendothelial system, and renal clearance affect toxicity, uptake, and half-life of NPs. 26 The reticuloendothelial system, mostly the macrophages, specifically mediates the half-life of NPs. 27 A method to circumvent this system is to coat NPs with a hydrophilic layer, using polymers such as polyethylene glycol (PEG) through a process called PEGylation. 28 Endocytosis is the last step through which NPs are transported into cells when they reach their target.
Classification of NPs
According to RSC Advances by Aula et al, 29 NPs can be divided into organic and inorganic. Inorganic NPs for CML treatment were detailed in a previous work. In this review, organic NPs are discussed and categorized as presented in Table 1 and below:
Summary of the Main Nanoparticles.
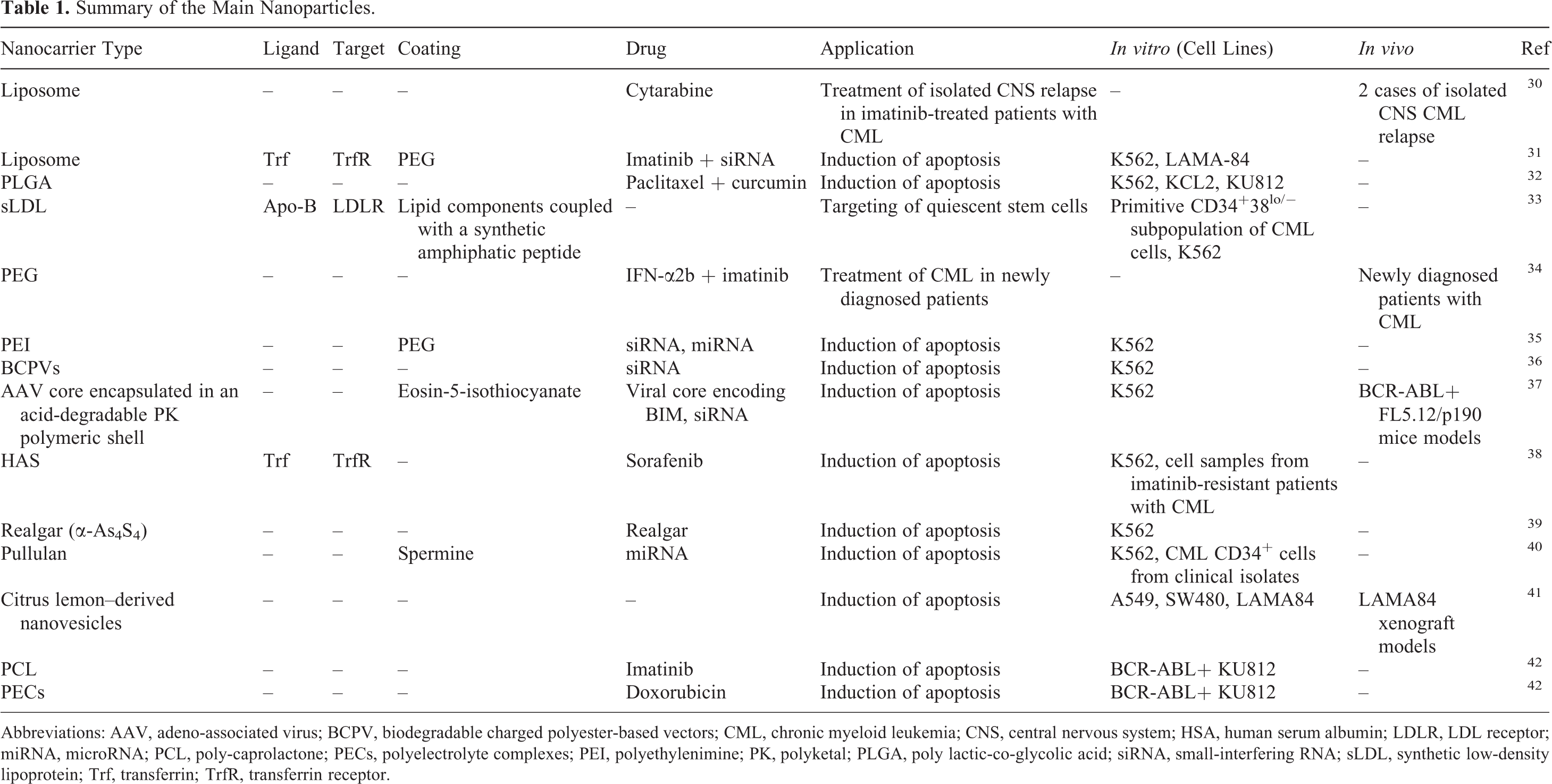
Abbreviations: AAV, adeno-associated virus; BCPV, biodegradable charged polyester-based vectors; CML, chronic myeloid leukemia; CNS, central nervous system; HSA, human serum albumin; LDLR, LDL receptor; miRNA, microRNA; PCL, poly-caprolactone; PECs, polyelectrolyte complexes; PEI, polyethylenimine; PK, polyketal; PLGA, poly lactic-co-glycolic acid; siRNA, small-interfering RNA; sLDL, synthetic low-density lipoprotein; Trf, transferrin; TrfR, transferrin receptor.
Lipid-based NPs (liposomes) Polymer-based NPs and micelles Poly lactic-co-glycolic acid (PLGA) NPs Micelles ▪ Multipurpose caniste-diisopropylamino)ethyl methacrylate deblock copolymers ▪ PEG Lipophilic polyethylenimines (PEIs) polymers Synthetic low-density lipoprotein (LDL) Dendrimers Biodegradable polyesters Biodegradable charged polyester-based vector (BCPVs) Poly-caprolactone (PCL) Albumin-based nanovectors Realgar NP Polysaccharide polymer Spermine-introduced pullulan (Ps) Citrus lemon–derived nanovesicles
Organic NPs for CML Treatment
Liposomes
Aichberger et al investigated the usage of liposomal cytarabine for the treatment of myeloid central nervous system (CNS) relapse in CML. 30 When compared to free drugs, the advantages of liposomes in drug vehiculation can be attributed to a reduction in drug toxicity, the ability to couple them with antibodies and other signaling molecules for further targeted delivery, as well improved altered bioavailability and pharmacokinetics.
Although considered an extreme rarity in the past, data show that a CNS relapse can appear in imatinib-treated patients with CML. 43,44 Although imatinib has been shown to be extremely effective in CML treatment, its chemical properties don’t allow for adequate crossing of the blood–brain barrier. This “anatomic” resistance may lead to a possible CNS relapse. This was demonstrated and studied on 2 patients who had a CNS relapse after being treated with imatinib for 4 years.
Both patients received intrathecal liposomal cytarabine. In the first patient, additional CNS radiation was performed, while a systemic relapse in the other patient was being concurrently treated with dasatinib. In both cases, symptoms resolved, and lumbar puncture revealed no leukemic cells in the CSF. Furthermore, 3 months of posttherapy monitoring showed no evidence of systemic or CNS relapse in either patient and both were shown to be in complete cytogenetic and molecular response. Therefore, liposomal cytarabine with/without radiation is effective as local therapy in patients with CNS relapse.
Furthermore, there is no concrete data regarding the efficacy of the newer BCR-Abl kinase inhibitors with regard to CNS relapse, implying that they cannot be regarded as standard therapy alone. These data suggest that liposomal cytarabine may be an effective therapeutic approach in such patients.
In addition to treating CNS relapses, liposomes have been used to coencapsulate anti-BCR-ABL small-interfering RNA (siRNA) and imatinib in CML treatment. 31 Overexpression of the transferrin receptor (TrfR) on tumor cell surface 46,47 and constitutive endocytosis 45,46 has made it a prime target for liposomal delivery into cancer cells. 48,49 Transferrin (Trf) is the ligand for this TrfR. 46,48
Small-interfering RNAs are small double-stranded RNA molecules composed of 20 to 25 base pairs that target messenger RNA (mRNA), leading to its cleavage. 50 -53 Nonetheless, the therapeutic use of siRNA is burdened by impediments such as degradation by enzymes, 51,54,55 a low uptake by cells, 54,55 as well as a rapid clearance by the kidneys, 49,52 leading to the observed poor pharmacokinetic properties in an in vivo environment. The vehiculation of siRNA in liposomes confers protection from nuclease degradation, leading to a sustainable plasma concentration while also allowing for targeting of tumor cells by these nucleic acids.
Mendonca et al 31 demonstrated an in vitro triple targeting strategy within a single system using TrfR-targeted liposomes to coencapsulate imatinib with anti-BCR-Abl siRNA. Cellular targeting was accomplished via Trf, molecular targeting of BCR-Abl mRNA was accomplished via BCR-Abl siRNA, and protein targeting was accomplished with imatinib. Not only is such a combination strategy a promising approach to the heterogeneity of tumor cells and their varying response to individual drugs, it is also an equally promising therapeutic approach to overcoming the resistance phenomena.
Rather surprisingly, imatinib encapsulation yields were improved by siRNA. This possibly owes to interactions between imatinib and siRNA, positively and negatively charged, respectively, which could promote further entrapment of imatinib in the liposomes.
Antileukemic activity against the K562 cell line was recorded for varying concentrations, with higher cellular toxicity being achieved with formulations carrying a higher siRNA to imatinib ratios. Furthermore, the highest siRNA to imatinib ratio was achieved at the lowest imatinib to lipid ratio. As such, it was possible to achieve therapeutic concentrations of each of imatinib and siRNA in a single liposome.
Poly Lactic-Co-Glycolic Acid
Polylactic acid as well as polyglycolic acid and their copolymer PLGA have been thoroughly explored due to their biocompatibility and biodegradability. 56 They manifest physical strength and biological compatibility while also possessing great flexibility. Moreover, their degradation can be modulated with control over the molecular weight (MW) of the NPs to fit the desired dose for sustained drug release. Loading the therapeutic drugs into PLGA provides many advantages, such as protecting the drug from enzymatic degradation and providing sustained release. 57 Recent reports demonstrate that PLGA NPs complexed to anticancer drugs can be used for efficient drug delivery and for reduced toxicity against normal cells. 58 -60
Acharya et al 32 explored an approach using PLGA NPs to simultaneously deliver 2 drugs to the Bcr-Abl fusion protein. In this study, paclitaxel, doxorubicin, etoposide, rapamycin, curcumin, and nutilin were encapsulated alone, and then paclitaxel was combined with each of the other drugs and encapsulation efficiency was calculated. When encapsulated alone, each of the drugs showed high encapsulation that slightly dropped when combined with paclitaxel. The lowered encapsulation efficiency may be due to differences in the partition coefficient between the drugs and their competition to occupy the NPs. Nevertheless, drug loading was still capable of reaching a therapeutically optimal concentration in vitro that requires further in vivo experimentation to prove its efficacy.
The highest therapeutic efficacy in vitro experimentation was observed with a paclitaxel/curcumin combination. When compared to their native equivalents, the encapsulated dual formulations used in this study showed better antileukemic effects on K562. When comparing the IC50 values of encapsulated dual formulations to their singly encapsulated counterparts, singly encapsulated formulations were effective only after 5 days versus 2 days when combined, showing that such drug combinations and their encapsulation in PLGA NPs could potentially reduce the treatment duration. Thus, NPs could potentially be used to codeliver drugs to the same target site and increase efficacy while decreasing treatment duration.
Synthetic LDL
Low-density lipoprotein is a lipoprotein in plasma responsible for the transport of cholesterol. This spherical particle has a diameter of approximately 22 nm. It’s use as a drug carrier in chemotherapy dates back to the 1980s when Gal et al 61 established an increase in the uptake of LDL in cancer cells of gynecological origin compared to normal cells. This observation has been shown to apply to many other types of cancer, including CML. 62 There is an elevation in LDL receptor activity leading to a higher LDL uptake and particularly in cases of CML with a worse prognosis related to lower concentrations of plasma lipids. 63
There is an overexpression of Bcr-Abl in CML stem cells. These cells do respond to imatinib therapy; however, this response is one of reversible block in proliferation and without a significant amount of apoptosis. Therefore, achieving a complete cure is hindered by the subsistence of leukemic quiescent stem cells (QSC) with the ability to initiate relapse. Zhou et al 33 have previously shown that intracellular levels of imatinib in CML progenitor cells (CD34+) and in other commonly used leukemic cell lines are remarkably higher than in primary primitive QSC (CD34+ 38 lo/−), which were significantly subtherapeutic. Achieving complete cure with imatinib and other TKIs, therefore, is dependent on targeting QSC.
Zhou et al 33 also aimed to determine whether drug delivery in synthetic LDL (sLDL) targeting QSC could overcome the subtherapeutic levels of drug concentrations in these cells. First, nondrug-loaded NPs were used to target BCR-Abl-positive cell lines, and an increase in the sLDL uptake by these cells compared to their BCR-Abl-negative counterparts was noted. Furthermore, compared to non-CML CD34+ cells, primitive CD34+ 38 lo/− cells were reported to accumulate significantly higher levels of sLDL. Therefore, loading sLDL NPs with drugs could present as a potential mechanism to enhance the level of intracellular drugs in primitive CML cells and aid in their elimination. Further studies, in vivo and with the inclusion of drugs in sLDL particles, must be carried out before a definitive conclusion that sLDL-loaded NPs may be beneficial in the therapeutic management of CML via the eradication of QSC.
Polyethylene Glycol
Polyethylene glycol is a water-soluble block used in forming polymer micelles. The advantages that PEG presents are that it makes micelles biocompatible and increases the bioavailability of certain drugs. 64 Simonsson et al 34 combined imatinib with pegylated interferon (IFN)-α2b (Peg-IFN-α2b) to potentially increase the molecular response rates in patients with CML.
Combining imatinib with IFN-α is an approach sometimes used in the management of CML. 65 -68 However, when using IFN-α, it seems that it is barely detectable after 24 hours of administration. Subsequently, a modification was necessary and 2 types of IFN-α have been developed: Peg-IFN-α2a and Peg-IFN-α2b, which involve the attachment of PEG. 34 Studies have compared the difference between the combination of imatinib with IFN-α2a and Peg-IFN-α2a on one side and IFN-α2b and Peg-IFN-α2b on another side. 69 The results indicated the efficacy of the pegylated form of IFN-α along with the combination of each with imatinib. 34,69
Newly diagnosed patients with CML were randomly chosen and either received a weekly dosage of 40 μg of Peg-IFN-α2b along with a daily dosage of 400 mg of imatinib or only a dosage of 400 mg of imatinib. 34 The results were remarkable in that the combination therapy showed much better results after 12 months, where major molecular response rate was greatly increased in the former than in patients receiving imatinib alone. Therefore, this combined therapy shows a promise for future CML therapy, keeping in mind that Peg-IFN-α2b appeared to have some toxicity levels leading to its discontinuation in 34 patients receiving the combined therapy. 34
Polyethylenimines
Polyethylenimine is a polycation used as a delivery system for DNA 70 and RNA carrying. Polyethylenimine has positively charged amine groups that complex with the negatively charged phosphate groups of nucleic acids. 71 -78 This modality is, however, limited by its toxicity 79 ; therefore, methods for lowering the toxicity levels have been enhanced and involve the linkage with nonionic/hydrophilic polymers such as the PEG. 35 With further modifications, the PEG could be rendered more hydrophobic and hence have a better interaction with the cell membrane making transfection much more feasible along with the endocytic uptake of the nucleic acids. 35 Consequently, modifying the hydrophobicity of the low-molecular PEI increases the safety as well as efficacy of drug delivery to cancer cells and induces silencing of the target protein.
RNA interference (RNAi) provides an alternative approach for the treatment of CML with acquired resistance. However, for RNAi to reach the cell and exert its actions, an efficient carrier must be provided. Therefore, Valencia-Serna et al 35 explored low-MW lipid-modified PEIs as potential carriers for therapeutic BCR-ABL downregulation. Results showed that palmitic acid–substituted PEI (1.2 kDa) was the most efficient (when compared to other lipid-substituted polymers) in delivering siRNA to the cells and silencing the reporter green fluorescent protein gene (GFP). In addition, PA-substituted PEI was able to reduce the mRNA levels in K562 cells when the BCR-ABL protein was targeted and was also able to induce apoptosis (early and late stages). Thus, low-MW PA-substituted PEI may be used as an efficient delivery system of siRNA for CML treatment.
Another strategy to transfect CML cells is the usage of PEG–PEI complex as nonviral carriers of microRNA (miRNA). 80 In CML, a beneficiary tumor suppressor miRNA is the miR-150 that functions as an inducer for the phosphoinositide-3-kinase, protein kinase B (AKT) pathway activation, pioneering telomerase activation, and immortalization of cancer cells. 81,82 One study showed that the usage of PEG–PEI-based NPs encapsulating the miRNA maintains a proper transfection of CML cells. 80 The high efficiency in miRNA transfection and the low cytotoxic effects make PEG–PEI a promising nonviral delivery system in CML treatment. The data indicate that PEG–PEI may be a promising nonviral carrier for the treatment of CML, with many advantages such as relatively high miRNA transfection efficiency and low cytotoxicity.
Phosphorus Dendrimers
Dendrimers are small NPs that have radial symmetry that make an efficient carrier for the delivery of a given drug. 83,84 Several types of dendrimers exist, and each has certain biological characteristics. These biological properties include electrostatic interactions, chemical stability, polyvalency, self-assembling, low cytotoxicity, and solubility. These properties allow for the wide usage of the dendrimers in the medical field. Phosphorus dendrimers are amphiphilic having a hydrophilic surface and a hydrophobic backbone, which facilitates their entry through the cell membrane. 83,85-86 The formation of dendriplexes with siRNA is favored due to the interaction between the negatively charged siRNA and the positively charged dendrimer surface. Moreover, the success of the formation of dendriplexes depends on external factors such as pH and temperature.
With regard to dendrimers potential usage in CML treatment, it was demonstrated that phosphorus dendrimers can be used to carry siRNAs specific for BCR gene, but no experiments were done to test their effect on CML cells. 87 Therefore, further investigations should be done.
Biodegradable Charged Polyester-Based Vectors
Yang et al 36 showed that BCPVs are efficient nonviral transfection NPs for gene knockdown of the BCR-ABL hybrid oncogene in K562 cell line. Their results showed that cancer cell proliferation can be decreased by enhancing cell apoptosis by downregulation of the oncoprotein (BCR-ABL) via RNAi. The significance of such results is that BCPVs may potentially be used as potential carriers of siRNA for CML treatment. The positive charge on the surface of the BCPV NPs allows for the penetration of the negatively charged cell membrane of the cells via electrostatic interactions. Furthermore, since the BCPV–siRNA complex is encapsulated, the obstacle of siRNA degradation is eliminated. When compared to Lipofectamine2000 (common transfection reagent), BCPV had a larger suppressive effect on K562 cells proliferation. This is due to the higher transfection efficiency of BCPV, subsequently leading to the enhancement of apoptosis. The mRNA expression knockdown-induced apoptosis is positively correlated with transfection efficiency. In summary, what makes BCPVs potentially successful carriers for siRNAs delivery is that they have low toxicity, high transfection efficiency, and manageable charge density. It is important to note that these studies were performed on adherent cells whereas leukemic cells are of nonadherent nature necessitating further research. 36
Viral/Nonviral Chimeric NPs
One interesting approach by Hong et al used viral/nonviral chimeric NPs to synergistically suppress leukemia proliferation via simultaneous gene transduction and silencing. 37 In this study, a dual-modal gene therapy was developed. 88,89 A new therapeutic approach to apoptosis-mediated gene therapy was led through analyzing the Bcr-Abl pathways, 90 -92 where it appeared to be directly regulated by the Bcl-2 family proteins, such as Bcl-2-interacting mediator (BIM) of cell death. 93,94 B-cell lymphoma-2 interacting mediator is responsible for the apoptosis of the leukemia cells, yet it is inactivated due to the presence of myeloid cell leukemia 1 (MCL-1). 95,96 Therefore, an important approach in CML targeting is the restoration of BIM expression and silencing the MCL-1 through a dual-modal gene manipulation. This study made use of NPs consisting of an adeno-associated virus (AAV) core encapsulated in an acid-degradable polymeric shell where proapoptotic BIM transduction was induced by the AAV core and silencing of prosurvival MCL-1 was achieved by siRNA encapsulated in the shell. The AAV was shielded in a nonviral chimeric NP that protected the virus from the immune system as well as encapsulating the siRNA responsible for the MCL-1 silencing. This, in turn, suppressed the proliferation of the Bcr-Abl-positive cells as was shown to occur in this study. 37
Albumin-Bound Paclitaxel to Treat Refractory CML
One of the challenges of using TKIs are point mutations in the kinase domain imparting drug resistance and contributing to future relapses. 97,98 Studies showed undesirable results due to point mutations in the tyrosine kinase–binding domain, the most critical being the tyrosine-isoleucine mutation at 315 position (T315I). 99 -101 One strategy is to target the other survival kinases; however, this might inflict damage to healthy cells where the pathway might also be present. 102,103 Therefore, Retnakumari et al developed a dual targeting method, where 2 pathways would be targeted at the same time in order to target the receptors of the refractory cancer cells along with their intracellular network of kinases. 38 The chemo drugs chosen needed to be transferred in a nontoxic manner and be readily bioavailable; therefore, a polymeric encapsulation for the drugs was chosen and that polymer was albumin-encapsulating paclitaxel (Abraxane), which is a key formulation of the human serum albumin (HSA). 104 Since albumin is part of the blood serum, it is a suitable integration of the delivery system due it is nonimmunogenic, nontoxic, and biocompatible nature. 105 This HSA-based NP was loaded with STAT5 inhibitor (sorafenib) designed to inhibit the phosphorylation of an activated secondary survival kinase (STAT5) and the surface was conjugated with Tf ligands to target TfR on the CML cells. 38 The results were promising when performed in vivo, where the dual targeting method led to the apoptosis of the leukemic cells without any side effects, inflammatory responses, or toxicity to the blood while showing maximal toxicity to the most resistant clinical samples. 38 This study demonstrates the potential of nanomedicines in tackling critical challenges such as drug resistance by engineering endogenous proteins abundant in our own body.
Realgar NPs
One of the methods to treat leukemia is by modifying the pathways involved in the cells’ life cycles, especially those concerned with cell apoptosis and autophagy. 106 One of the well-known pathways is the P13K/Akt/mTOR (class I phosphoinositide 3-kinase/protein kinase B mammalian target of rapamycin). 39 Such pathway appears to be enhanced when treated with As2S2 such as realgar; however, realgar has been demonstrated to be insoluble in water and most organic reagents. 107 These characteristics play a negative role in its utilization in biological applications and medicine due to its limitations and poor bioavailability. 108 Therefore, Shi et al 109 prepared realgar NPs with a minimum size of 100 nm and proved to have higher bioavailability compared to coarse realgar while degrading the oncoprotein involved (Bcr-Abl). Moreover, one of the known membrane proteins involved in the P13K/Akt/mTOR pathway, Caveolin-I (Cav-1), appeared to be enhanced when treated with the realgar NPs. 109,110
Pullulan/MiRNA NPs
Ma et al 40 aimed to modulate the growth and imatinib sensitivity of CML stem/progenitor cells using pullulan/miR-181a NPs in vitro. A miR-181a is a miRNA that has been shown to inhibit the proliferation of a CML cell line, K562 cells. Moreover, miR-181a binds to 3-UTR of RALA (an oncogene) and subsequently inhibit its expression. 111
Spermine-introduced pullulan were used as vectors to deliver miRNA to CML cells. Delivery efficiency and mean fluorescence intensity showed successful transfection of CML CD34+ cells by Ps miRNA in vitro. In CML, the expression of miR-181a is extremely low while the expression of RALA is very high compared to control cells. RALA is the direct target of miR-181a. The delivery of miR-181a induced a decrease in CML cells proliferation, while it had no effect on normal CD34+ cells. When TKIs were used in combination with miR-181a, a higher specific inhibition of CML cells growth was achieved, even in cells manifesting resistance. Consequently, Ps was presented as an efficient nonviral delivery system of miRNA to CML cells. The delivery of miR-181a not only inhibited the growth the CML cells (CD34+), but it also increased their sensitivity to imatinib mesylate. Overall, Ps provides an improvement in the treatment of CML.
Citrus Lemon–Derived Nanovesicles
Under specific circumstances, when some natural compounds are used in association with chemotherapeutic drugs, lower dose of drugs can be used without compromising efficiency. 41 Nanoparticles extracted from lemon by Raimondo et al induced apoptotic effects on the cancer cells via the TRAIL mechanism. These NPs express anticancerous properties since they inhibit cell proliferation. 112 -115 One of the main advantages of TRAIL lies in its specificity to induce apoptosis only in transformed cells and not in normal cells. 116,117 Subsequently, the therapeutic approach can overcome 2 main obstacles: drug resistance and toxicity on normal tissues. Based on morphology and size, the NPs extracted from the citrus lemon juice are exosome like. 118 According to data, citrus lemon nanovesicles reduced cell proliferation in vivo on CML (LAMA84) xenograft models in both time- and dose-dependent manner. 41 The nanovesicles were also active in vitro against the following cell lines: A549, SW480, and LAMA84. The nanovesicles were able to induce apoptosis via the TRAIL pathway in cancer cells without affecting the normal cells. Moreover, the nanovesicles inhibited angiogenesis by inhibiting the secretion of angiogenic cytokines (vascular endothelial growth factor A, interleukin [IL]-6, and IL-8).
Poly-Caprolactone
In order to maintain well-controlled drug delivery, NPs usage became important and studied more thoroughly; therefore, Palama et al 42 investigated the usage of coupled delivery of imatinib and doxorubicin carried using biodegradable pH sensitive core–shell PCL NPs and enzyme-sensitive polyelectrolyte complexes for a sustained downregulation of BCR-ABL in CML. The main purpose of the combination is to increase the therapeutic index of the drug by making it more target specific while simultaneously making it less toxic at increased concentrations. 119 The experimental results suggest that the nanoformulations maintained the biological activity of drugs for longer periods and led to a continuous release of active drug. Moreover, at low concentrations, the combined drug-loaded nanoformulation was relatively more efficient against CML cells than the single drug formulation. Western blot analysis was used to assess the effective inhibition of the BCR-ABL tyrosine kinase activity after 3 days of incubation with a low concentration (10 nM) of free combination drugs and same concentration of drug-loaded NPs. Cell viability of CML was permanently blocked, using the drug-loaded NPs cocktail, but BCR-ABL inhibition was only partially inhibited using the free combination, demonstrating this nanoformulation’s ability to improve drug kinetics and efficacy.
Conclusion
Chronic myeloid leukemia is a neoplastic proliferation of mature myeloid cells, especially granulocytes and their precursors. It is the result of the BCR-ABL fusion gene, leading to a constitutively active TK resulting in uncontrolled growth of myeloid cells. Imatinib and other TKIs are the most widespread treatment modalities available for CML treatment. However, as good as the response rates to these drugs are, they are not without their downfalls. For instance, imatinib fails to achieve cure status due to persistent QSC. Furthermore, resistance plays a major part in the decreased efficacy of imatinib and its sister drugs, with a functional “anatomic” resistance also being reported.
Therefore, nanomedicine and the use of NPs as drug delivery systems may provide an alternative and a superior treatment modality to CML. This review highlighted organic examples of such treatments in vitro and in vivo settings, with inorganic NPs highlighted in a previous study. Preliminary results are encouraging, with NPs displaying the ability to overcome both “anatomic” resistance and MDR, and successfully targeting the QSC. Additionally, these NPs demonstrated safety through specific targeting of CML cells with sparing of normal cells. However, the majority of these studies were conducted in a controlled laboratory environment, while only a few studies included clinical trials; therefore, further studies and clinical trials in this field are required.
Footnotes
Acknowledgments
The authors thank Ahmad El Mahmoud, Khodor Terro, Bachar El Baba, and Nadia El Harake for helping with revision of the text.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.