
Abstract
Due to the critical role of inflammation in nasopharyngeal carcinoma, we aim to investigate the correlation between nasopharyngeal carcinoma prognosis and the levels of tumor necrosis factor α and macrophages for the development of new prognostic models. The levels of tumor necrosis factor-α and CD68-positive macrophages were measured in 111 primary nasopharyngeal carcinoma specimens by immunohistochemistry. Kaplan-Meier analysis showed that, compared with nonelevated tumor necrosis factor-α levels, elevated tumor necrosis factor α levels were correlated with poorer 10-year distant metastasis-free survival (24.5% vs 5.2%, P = .004) and bone metastasis-free survival (17.0% vs 0.0%, P = .001). Multivariate analysis revealed that tumor necrosis factor α level was an independent prognostic factor for distant metastasis-free survival (hazard ratio = 16.765, P = .001), while the level of CD68-positive macrophages was a favorable independent prognostic factor for cancer-specific survival (hazard ratio = 0.481, P = .023) and disease-free survival (hazard ratio = 0.403, P = .010). Additionally, several prognostic models that considered tumor-node-metastasis stage alone or in combination with tumor necrosis factor α and/or CD68-positive macrophage levels were compared by receiver operating characteristic curve analysis. Interestingly, the T_score model, which considered the tumor necrosis factor α level alone, could better predict the distant metastasis-free survival and bone metastasis-free survival, whereas the MT model, which considered the combination of T stage and CD68-positive macrophage level, could better predict the cancer-specific survival and disease-free survival of patients with nasopharyngeal carcinoma. Elevated tumor necrosis factor-α levels and decreased CD68-positive macrophage levels in primary nasopharyngeal carcinoma tissues are unfavorable prognostic indicators in nasopharyngeal carcinoma. The T_score model or the MT model could be better prognostic models than those currently available for nasopharyngeal carcinoma and could be used to select high-risk patients and aid in the design of individualized immunotherapy.
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is a malignant cancer arising from epithelial cells of the nasopharynx. Southern China and Southeast Asia are the major epidemic areas of NPC, 1 with an incidence rate of 17.3 females and 43.3 males per 100 000 people in China during 2015. 2 These tumors are highly invasive, resulting in a high potential for metastasis. 3 Although NPC is sensitive to radiotherapy and chemotherapy, patients with distant metastatic disease show very poor prognoses, with a median survival time of only 13 months. 4 Although the tumor-node-metastasis cancer staging system summarized by the American Joint Committee on Cancer and the Union for International Cancer Control (AJCC/UICC) can aid in prognosis evaluation and the development of more effective treatment strategies, limitations in this system still exist due to its failure to account for biological characteristics and the heterogeneity of cancer cells. Therefore, it is important to identify new biomarkers that could be employed to generate a more rational model for improved prognostic predictions, thereby conferring the ability to identify high-risk patients and stratify them for treatment.
A great deal of evidence has demonstrated the role of tumor necrosis factor α (TNF-α) in the inflammatory process associated with carcinogenesis. 5 As it is produced by many types of cells, including macrophages, neutrophils, fibroblasts, keratinocytes, natural killer cells, T cells, B cells, and tumor cells, TNF-α is involved in the growth, differentiation, and survival of various cells. 6 In particular, TNF-α plays a critical role in the progression of cancers by enhancing angiogenesis and increasing the invasion and migration of cancer cells. 7 -9 It has been reported that elevated levels of serum TNF-α were associated with poor prognoses in patients with many types of malignancies, including lymphoma and prostate cancer. 10 -13 Similarly, we have reported in a previous study that serum TNF-α was an independent unfavorable prognostic factor for distant metastasis-free survival (DMFS) in patients with NPC. 13 However, because uncertainty remains regarding the sources of TNF-α in the tumor microenvironment and serum, we sought to evaluate the local expression of TNF-α in primary NPC tissues and to assess its prognostic value.
Macrophages are innate immune cells that differentiate from monocyte precursors upon arrival into tissues. 14 Macrophages that infiltrate the tumor microenvironment, also called tumor-associated macrophages (TAMs), were reported to be involved in the initiation and progression of cancers. Tumor-associated macrophages play a role in promoting angiogenesis, increasing the survival and migration of tumor cells, and suppressing the antitumor effect of the adaptive immune system by secreting growth factors, cytokines, and chemokines in the tumor microenvironment. 15 -19 Based on the majority of previous studies, macrophages play a protumor factor in many cancers and are correlated with a poor outcome in patients. However, a beneficial role of macrophages in cancers has also been reported. For instance, peritumoral infiltration of macrophages in colorectal cancer showed a positive correlation with patients’ overall survival (OS). 20 Moreover, TAMs in the tumor nest positively correlate with the frequency of tumor cell apoptosis, the abundance of CD8 cells in the tumor nest, and the 5-year disease-free survival (DFS) rate of patients with gastric cancer. 21 Most recently, TAMs were shown to suppress the proliferation of tumor cells in colorectal cancer by producing proinflammatory cytokines and chemokines and by promoting type 1 T-cell responses. 22 Notably, a study by our colleagues reported that patients having NPC with higher TAM levels in primary NPC specimens showed a higher OS rate. 23 Collectively, TAMs play a dual role in the development and inhibition of cancer; this role is dependent on cancer type, histology, and stage as well as on macrophage phenotype and other factors in the tumor microenvironment.
In particular, macrophages are the major producers of TNF-α and are also highly responsive to TNF-α. The engagement of Toll-like receptors on macrophages induces macrophage activation and TNF-α production, and TNF-α can inversely promote macrophage proliferation and differentiation. 24 However, neither the relationship between TNF-α and macrophages in primary NPC tissues nor their combined prognostic values in patients with NPC has been investigated. Hence, in this study, we measured the expression of TNF-α and the level of CD68-positive macrophages in primary NPC tissues by immunohistochemistry (IHC) and further evaluated the prognostic values of these 2 parameters either alone or in combination for predicting the survival of patients with NPC. Furthermore, we also compared the effectiveness of several models that account for both the clinical stage of NPC and these 2 remarkable biomarkers in predicting the outcome of patients with NPC.
Patients and Methods
Case Selection
After the study was approved by the institutional ethics board of Sun Yat-Sen University Cancer Center (SYSUCC), the slides from 111 patients diagnosed between February 1, 1999, and March 30, 2000, with histologically confirmed NPC but without distant metastasis were searched from the pathology archive of SYSUCC. All cases were restaged according to the AJCC/UICC cancer staging system (2002 edition) for NPC. The clinical and demographic characteristics of the patients are listed in Table 1.
Clinical Characteristics of Patients With NPC in Whom TNF-α Expression and CD68-Positive Macrophages Level Were Quantified by IHC Staining.

a P values were calculated using the chi-squared test or Fisher’s exact test if indicated
bII, differentiated nonkeratinizing carcinoma; III, undifferentiated nonkeratinizing carcinoma.
cAccording to the American Joint Committee on Cancer and the Union for International Cancer Control (AJCC/UICC) staging system (2002 edition).
dI, T1N0M0; II,T2N0-1M0, T1N1M0; III, T3N0-2M0, T1-2N2M0; IVa-b, T4N0-3M0, T1-3N3M0.
Abbreviations: CRT, chemoradiotherapy; ICT, induction chemoradiotherapy; NP, nasopharynx; RT, radiotherapy; TNF-α, tumor necrosis factor α; WHO, World Health Organization.
Treatment and Follow-Up
All patients received 2-dimensional radical radiotherapy with a daily fraction of 2.0 Gy and 5 fractions per week; the average radiotherapy dose to the nasopharynx and to the neck was 70.29 Gy (range, 60-80 Gy) and 60.58 Gy (range, 50-80 Gy), respectively. A total of 29 (26.1%) patients received 2 to 3 cycles of induction or concurrent platinum-based chemotherapy. Among these patients, 19 (17.1%) received induction chemotherapy (5-fluorouracil, 4.0 g/m2; and cisplatin, 80 mg/m2) alone, 5 (4.5%) received concurrent chemotherapy (cisplatin, 100 mg/m2), and 5 (4.5%) received both induction and concurrent chemotherapy (Table 1). Patients were followed up as previously described. 25 The median period of follow-up was 63.8 months (1-104 months).
Immunohistochemistry
Briefly, paraffin-embedded tissue specimens were deparaffinized and rehydrated. Antigen retrieval was performed with sodium citrate using a high-pressure boiler for 20 minutes. The sections were then incubated in H2O2 (3%) for 10 minutes, blocked in goat serum at room temperature for 30 minutes, and incubated with anti–TNF-α (25 µg/mL; R&D Systems, Minneapolis, Minnesota) and anti-CD68 (1:80; Boster, Wuhan, China) antibodies overnight at 4°C. The primary antibodies were detected by an EnVision kit (DAKO, Carpinteria, California) according to the manufacturer’s instructions. For TNF-α staining localized in cytoplasm and extracellular matrix, we scored the expression according to the intensity and stained area around tumor cells by 2 pathologists using a semiquantitative immunoreactive score. 26 The intensity and area of staining were classified into 0, 1, 2, 3, and 4 grades, and the staining was scored by the product of the 2 grades. Then, the median IHC score (score = 8) was used as the cutoff value to divide the patients into groups with high or low levels. For CD68 staining, macrophages with tawny to clay-colored particles were considered to be CD68 positive. The CD68-positive macrophages in 3 to 5 fields as viewed under a ×400 objective were enumerated, and the mean values were recorded. The evaluation of CD68-positive macrophages was repeated after 1 month, and the mean value of 2 enumerations of CD68-positive macrophages was ultimately used. The IHC score of CD68 was from 20 to 135. And the median IHC score (score = 70) was used as the cutoff value to divide the patients into groups with high or low levels of CD68. We had set the positive controls for TNF-α and CD68 IHC with neck inflammatory lymph node sections (Supplemental Figure 1A and C). And the negative controls for them were NPC section with the same IHC process but changed primary antibody diluents into pure diluents (Supplemental Figure 1B and D).
Statistical Analyses
All analyses were performed with the SPSS 22.0 software (SPSS, Chicago, Illinois). Student t test, 1-way analysis of variance, the χ2 test or Fisher exact test, and linear correlation analysis were performed as indicated for comparisons between the groups. The survival duration was calculated from the first day of NPC diagnosis. The primary end point was the DFS rate; the secondary end points were the rates of cancer-specific survival (CSS), DMFS, lung metastasis-free survival (lung-MFS), liver metastasis-free survival (liver-MFS), and bone metastasis-free survival (bone-MFS). The actuarial survival rates were calculated using the Kaplan-Meier method, and the differences were compared using the log-rank test. Adjusted Cox proportional hazard models were used to identify the significant independent variables with a backward (conditional) method. The area under the receiver operating characteristic (ROC) curve was used to compare the prognostic models. A 2-tailed P value of less than .05 was considered significant.
Results
Clinical Characteristics of Patients
Among the 111 patients, 42 (37.8%) died as a result of cancer, and 1 died from a non–cancer-related disease. Sixteen (12.6%) patients had distant metastases, with 9, 6, and 4 patients experiencing bone, liver, and lung metastases, respectively (Table 1). Among the patients with metastasis, 3 (18.7%) of 16 had multiple metastases. The 10-year CSS and DMFS rates were 62.2% and 85.6%, respectively.
Expression of TNF-α and Level of CD68-Positive Macrophages in Primary NPC Tissues
To determine the relationship between disease progression and the expression of TNF-α or the level of CD68-positive macrophages in primary NPC tissues, we evaluated both of these biomarkers in primary NPC tissues using IHC. However, neither the expression of TNF-α nor the level of the CD68-positive macrophages in primary NPC tissues was significantly different between patients with different T stages, N stages, or clinical stages (Figure 1A-C, all P > .05). Notably, patients with stage N2/3 disease showed a lower level of CD68-positive macrophages than those with stage N0/1 disease, but this difference was not statistically significant (Figure 1B, P = .072).

Baseline TNF-α expression or CD68-positive macrophage level in primary NPC tissues of the patients. The IHC scores for TNF-α (A) were not significantly different between patients with different T stages (left), N stages (middle), or clinical stages (right). The levels of CD68-positive macrophages (B) were not significantly different between patients with different T stages (left), N stages (middle), or clinical stages (right). The IHC scores for TNF-α in patients with or without distant metastasis (C). P values were calculated using Student t test or 1-way ANOVA. The lines in the box plots indicate the means and the upper or lower quantiles. ANOVA indicates analysis of variance; IHC, immunohistochemistry; NPC, nasopharyngeal carcinoma; TNF-α, tumor necrosis factor α.
Additionally, we sought to explore the relationship between the expression of TNF-α in primary NPC tissues and distant metastasis. As we expected, the average expression of TNF-α was higher in patients with bone metastases than in those without bone metastasis or with metastasis to other organs, but this difference was not statistically significant (Figure 1C, all P > .05).
Previous studies revealed that macrophages were a major producer of TNF-α. Thus, we explored the correlation between CD68-positive macrophages and TNF-α in primary NPC tissues. Linear correlation analysis revealed a lack of correlation between the expression of TNF-α and the level of CD68-positive macrophages in primary NPC tissues (Figure 2, P = .552).

The linear correlation analysis of CD68-positive macrophage level and TNF-α expression in the primary NPC specimens. NPC indicates nasopharyngeal carcinoma; TNF-α, tumor necrosis factor α.
High Expression of TNF-α in Primary NPC Tissues Correlated With Poor DMFS and Bone-MFS of Patients With NPC
To further explore the relationship between the expression of TNF-α and patient outcomes, patients were stratified based on low TNF-α versus high TNF-α expression or low CD68-positive versus high CD68-positive macrophage levels, according to the median value found by quantification of the IHC results (Figure 3). Kaplan-Meier survival analysis was performed on the cohort of 111 patients. Patients in the high TNF-α group showed a shorter 10-year DMFS and bone-MFS time (Figure 4A and B); no significant difference was observed in the baseline clinical characteristics between the 2 TNF-α groups (Table 1).
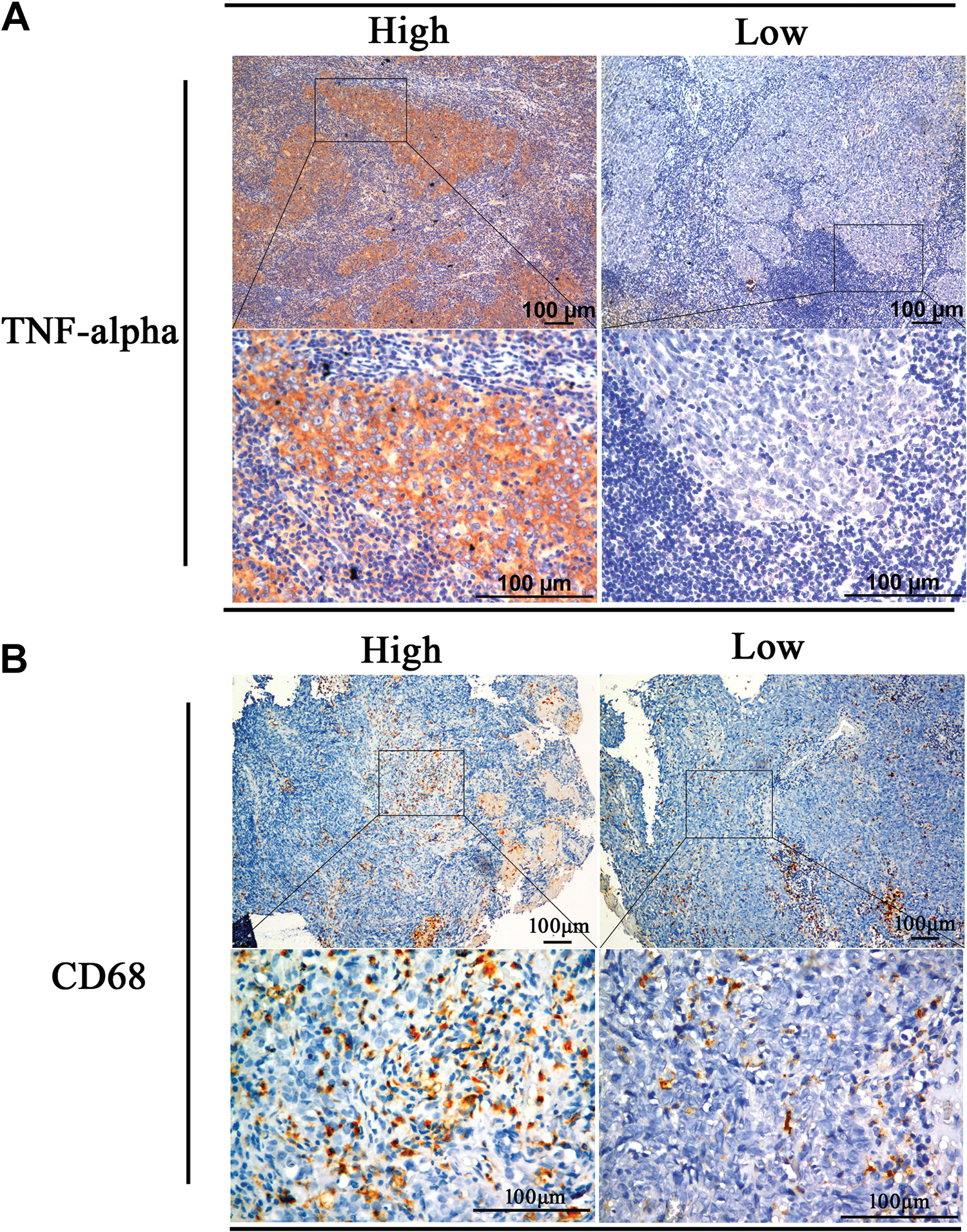
Representative images of high and low expression of TNF-α (A) and CD68 (B) in primary NPC tissues. Scale bar, 100 µm. NPC indicates nasopharyngeal carcinoma; TNF-α, tumor necrosis factor α.

Elevated expression of TNF-α positively correlated with poor outcomes in patients with NPC. Kaplan-Meier survival analysis showed that patients with NPC with high TNF-α expression had decreased rates of 10-year distant metastasis-free survival (A) and bone metastasis-free survival (B). Kaplan-Meier survival analysis showed that patients with NPC with fewer CD68-positive macrophages had poorer 10-year rates of overall survival (C, D) and disease-free survival (E, F). P values were calculated using unadjusted Kaplan-Meier survival analysis. NPC indicates nasopharyngeal carcinoma; TNF-α, tumor necrosis factor α.
Low Levels of CD68-Positive Macrophages in Primary NPC Tissues Correlated With Poor CSS and DFS of Patients With NPC
As the age distribution between the 2 CD68-positive macrophage groups was not equal, we performed Kaplan-Meier analyses in 2 subgroups (
Independent Prognostic Factors for Survival of Patients With NPC
To gain insight into the independent prognostic factors associated with the survival of patients with NPC, an adjusted multivariate analysis using a Cox proportional hazard model was performed. The clinical characteristics of age (
After adjusting for the differences in clinical characteristics, the level of CD68-positive macrophages was found to be a favorable prognostic factor for CSS and DFS (hazard ratio [HR] = 0.481, P = .023 and HR = 0.403, P = .010, respectively), while TNF-α was found to be an unfavorable independent prognostic factor for DMFS (HR = 16.765, P = .001; Table 2).
Multivariate Analysis of Prognostic Factors for Survival of Patients With NPC.

Abbreviations: CI, confidence interval; CRT, chemoradiotherapy; CSS, cancer-specific survival; DFS, disease-free survival; DMFS, distant metastasis-free survival; HR, hazard ratio; NP, nasopharynx; NPC, nasopharyngeal carcinoma; RT, radiotherapy; TNF-α, tumor necrosis factor α; WHO, World Health Organization.
a P values were calculated using an adjusted Cox proportional hazard model. The following parameters were included in the Cox proportional hazard model (backward method; conditional): age (≤50 vs > 50), sex (male vs female), type of histology (WHO classification III vs WHO classification II), T classification (T3-4 vs T1-2), N classification (N2-3 vs N0-1), RT dose to NP (discrete variate), RT dose to neck (discrete variate), use of induction chemotherapy (with vs without), use of concurrent chemotherapy (with vs without), TNF-α expression (high vs low), and CD68-positive macrophage level (high vs low).
b Statistically significant P values are indicated.
Comparison of the Different Models for Predicting the Outcomes of Patients With NPC
Upon discovering that both the expression of TNF-α and the level of CD68-positive macrophages were independent prognostic factors for survival of patients with NPC, we sought to determine the predictive capacity of these 2 parameters in different models that account for both clinical stage, and TNF-α and/or CD68-positive macrophage levels through the use of ROC curves. As shown in Figure 5, the MT model, which accounts for both CD68-positive macrophage levels and T stage, was the best model for predicting cancer-specific death and disease progression; this model had the highest area under the curve (Figure 5A and B). Intriguingly, the T_score model, which accounts for the expression of TNF-α, had the highest area under curve for the prediction of distant metastasis and bone metastasis (Figure 5C and D). Indeed, these results were consistent with those of the multivariate analysis, indicating that CD68-positive macrophage levels were more accurate in predicting cancer-specific death and disease progression, whereas TNF-α expression was better at predicting distant metastasis.

Comparison of prognostic models combining TNF-α expression and/or CD68-positive macrophage level and TNM stage in patients with NPC. The ROC curves were performed to compare the predictive ability among of models accounting for the AJCC (sixth) staging system score, T_score (TNF-α expression only), TT (TNF-α expression and T stage), TN (TNF-α expression and N stage), TC (TNF-α expression and clinical stage), M-score (CD68-positive macrophage level only), MT (CD68-positive macrophage level and T stage), MN (CD68-positive macrophage level and N stage), MC (CD68-positive macrophage level and clinical stage), and TMC (TNF-α expression, CD68-positive macrophage level, and clinical stage) in cancer-specific death (A), disease progression (B), distant metastasis (C), or bone metastasis (D) in 111 patients with NPC over a monitoring period of 10 years. AJCC indicates American Joint Committee on Cancer; bone-MFS, bone metastasis-free survival; CSS, cancer-specific survival; DFS, disease-free survival; DMFS, distant metastasis-free survival; NPC, nasopharyngeal carcinoma; ROC, receiver operating characteristic; TNF-α, tumor necrosis factor α; TNM, tumor-node-metastasis.
Discussion
As reported previously, the inflammatory cytokine TNF-α has a dual role in the initiation and progression of cancers. 27 Acute local TNF-α administration was shown to exert cytotoxic effects in tumors, whereas persistent TNF-α expression results in a strong protumor effect on the progression of many cancers. 28 Recently, TNF-α–expressing tumor cells were reported to inhibit the growth of primary and metastatic melanoma and Lewis lung carcinoma. 29 However, TNF-α could induce the invasion and migration of papillary thyroid cancer cells mediated by epithelial–mesenchymal transition. 30 Hence, the role of TNF-α in cancer may depend on its concentration and exposure duration, the tumor type, and the presence of other chemokines or cytokines in the tumor microenvironment. Notably, we previously reported that the level of serum TNF-α was positively correlated with a higher frequency of bone invasion and post-treatment distant metastases in patients with NPC as well as a poorer OS. 30 Consistent with these findings, we have verified in this study that the expression of TNF-α in primary NPC tissues was an unfavorable prognostic factor for DMFS. Taken together, these results indicate that the expression of TNF-α in either primary NPC tissues or in serum can predict the risk of distant metastasis in patients with NPC, indicating that TNF-α likely acts as a protumor factor in this setting. In addition, the use of TNF-α as a potential therapeutic target for NPC treatment warrants further investigation.
Notably, many studies have shed light on the mechanism of TNF-α-induced tumor progression. For instance, studies in gastric cancer and osteosarcoma suggest that TNF-α/TNFR1 signaling can maintain tumor cells in an undifferentiated state through the induction of NADPH oxidase organizer 1 or the activation of Gna14 and ERK. 31,32 Moreover, leukemia-initiating cells were found to exhibit constitutive nuclear factor (NF)-κB activity through autocrine TNF-α signaling, forming a NF-κB/TNF-α positive feedback loop. 33 In particular, the TNF-α/TNFR1 signaling pathway can directly stimulate lymphatic endothelial cell activity, leading to lymphangiogenesis and tumor metastasis. 34 Based on these findings, we could speculate that TNF-α might play an important role in metastasis through its effect on the lymphatic system. However, the role of TNF-α and its underlying mechanism of action in NPC remain unclear and need further investigation.
Likewise, the bidirectional correlations between patient survival and macrophage levels have been reported in many malignancies. Increased numbers of CD68-positive macrophages were shown to correlate with decreased progression-free survival and an increased likelihood of relapse in classic Hodgkin lymphoma 35 as well as with decreased survival in patients with breast cancer and advanced thyroid cancer. 36,37 However, in the setting of nonsmall cell lung cancer, the outcome was better in patients with a higher density of islet macrophages than in those with a lower density of these cells. 38 Moreover, a high density of macrophages in the invasive front positively influences prognosis in patients with colon cancer. 39 Herein, we have shown that the level of CD68-positive macrophages in primary NPC tissues was positively correlated with increased DFS and could be used as a favorable prognostic factor for CSS and DFS.
Although macrophages are the major producers of TNF-α, elevated TNF-α production could not be observed in TAMs stimulated with supernatant from NPC cell lines compared with a positive control. 23 Furthermore, herein, we could not find an association between the expression of TNF-α and the level of infiltrating CD68-positive macrophage in primary NPC tissues. Consistently, high levels of TNF-α in tonsil carcinoma did not correlate with an increase in macrophage and mast cell numbers, suggesting that this cytokine may be synthesized by other cells present in the tumor microenvironment, including the tumor cells themselves. 40
Additionally, the protumor or antitumor effects of macrophages may also be dependent on the type of macrophages present. Indeed, the densities of TAMs and stromal macrophages of the M1 phenotype were positively correlated with survival in nonsmall cell lung cancer, but this correlation was not observed for M2 macrophages. 41 However, we evaluated only macrophages that were positive for CD68, which is a common marker for both M1 and M2 macrophages. This limitation may explain why no correlation between TNF-α and macrophage levels was found.
Furthermore, comparison of our predictive models showed that the MT model was the best predictor of CSS and DFS, while the T_score model was the best predictor of DMFS and bone-MFS in patients with NPC. These results suggested that compared with patients with a lower T stage and higher levels of tumor-infiltrating CD68-positive macrophages in primary NPC tissues, patients with a higher T stage and lower levels of tumor-infiltrating CD68-positive macrophages in primary NPC tissues had a higher rate of tumor progression and a lower survival rate. Likewise, a higher expression of TNF-α in primary NPC tissues was associated with a higher risk of distant metastasis, particularly bone metastasis; this result was consistent with the result of our previous study.
We acknowledge that the small sample size of 111 NPC specimens was the main limitation of this study; however, it could also reveal the phenomenon to some extent. Further prospective clinical trials in larger population are warranted.
In conclusion, the expression of TNF-α and the level of CD68-positive macrophages in primary NPC tissues could be used as prognostic indicators for identifying high-risk patients who may require a more intensive therapeutic strategy. However, the clinical application of these models in terms of their capacity to predict disease progression should be validated in prospective clinical trials.
Availability of Data and Material
The authenticity of this article has been validated by uploading the key raw data onto the Research Data Deposit public platform (http://www.researchdata.org.cn), under the approval number RDDA2018000432.
Supplemental Material
Supplemental Material, supplementary_Fig1 - Elevated Levels of TNF-α and Decreased Levels of CD68-Positive Macrophages in Primary Tumor Tissues Are Unfavorable for the Survival of Patients With Nasopharyngeal Carcinoma
Supplemental Material, supplementary_Fig1 for Elevated Levels of TNF-α and Decreased Levels of CD68-Positive Macrophages in Primary Tumor Tissues Are Unfavorable for the Survival of Patients With Nasopharyngeal Carcinoma by Yahui Yu, Liangru Ke, Wei-Xiong Xia, Yanqun Xiang, Xing Lv and Junguo Bu in Technology in Cancer Research & Treatment
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.