
Abstract
Purposes:
The newly released Protura 6 degrees-of-freedom couch (CIVCO) has limited quality assurance protocols and pertinent publications. Herein, we report our experiences of the Protura system acceptance, commissioning, and quality assurance.
Methods:
The Protura system integration was tested with peripheral equipment on the following items: couch movement range limit, 6 degrees-of-freedom movement accuracy, weight test and couch sagging, system connection with Linac, isocentricity of couch and rotation alignment, kV and cone-beam computed tomography imaging of HexaCHECK with MIMI phantom (Standard Imaging), and an in-house custom 6 degrees-of-freedom quality assurance phantom. A couch transmission measurement was also performed.
Results:
The vertical, longitudinal, and lateral ranges of the 6 degrees-of-freedom couch pedestal are 43.9 to 0.0 cm, 24.6 to 149.5 cm, −20.6 to 20.7 cm, respectively. The couch movement accuracy was within 1 mm in all directions. The couch sagging with a 200 lbs (∼91 kg) evenly distributed object is 1.0 cm and 0.4° pitch in the distal end of the couch. The isocentricity of the couch was about 0.5 mm in diameter of all crosshair projections on the couch isocenter level, and the largest couch rotation alignment observed was (0.3°) at the couch angle of 90°. The deviation from the reference position (zero position) of the HexaCHECK phantom, measured by matching the cone-beam computed tomography with the reference planning computed tomography, was found to be below 0.2 mm in the anterior–posterior and right–left dimensions, 0.4 mm in superior–inferior dimension, and 0.1° in roll, pitch, and yaw directions.
Conclusions:
A 6 degrees-of-freedom quality assurance phantom is helpful for the commissioning and routine quality assurance tests. Due to the third-party integration with Linac, the system is prone to “double-correction” errors. A rigorous quality assurance program is the key to a successful clinical implementation of the Protura system.
Introduction
Accuracy and precision of radiotherapy are essential to a successful radiation treatment, which requires registering the target volume from the pretreatment kV/cone-beam computed tomography (CBCT) images to the planning computed tomography (CT) images and positioning the patient in their treatment location. Therefore, the quality assurance (QA) of localization and patient positioning systems is critical for accurately treating the patient in their exact treatment location. The previous version, Clinac, is subject to 4 degrees of freedom, which makes the patient alignment longer prior to treatment due to realigning and reimaging the patient without a rotation correction on a standard couch. For example, it is very common in clinics that some head and neck patients are subject to c-spine curvature alignment, and thorax patients are subject to body rotation in roll and pitch directions. For stereotactic radiosurgery/stereotactic body radiation therapy, a 6 degrees-of-freedom (6D) couch is an essential component of the program to ensure the patient receives the most accurate and precise treatment. 1 –7 Most modern Linacs (ie, TrueBeam) have an upgrade option to include a 6D couch from their own manufacturers. However, the 6D couch is not an upgradable option from the manufacturer for some older models of C-series Linacs. To achieve high precision localization on these older model machines, the alternative is to explore and acquire a 6D couch from a third-party vendor. A newly released Protura 6D couch (CIVCO Radiotherapy, Coralville, Iowa) was implemented in our clinic over a year ago. Because the system is relatively new to the community, few publications exist about acceptance testing and QA guidelines. The American Association of Physicists in Medicine (AAPM) has published QA guidelines about 6D couches, which can be found in the task group (TG) reports 40, 142, and AAPM MPPG#8a. 8 –10 The TG-142 report recommends a monthly test of treatment couch position indicators (2 mm/1°) and annual tests of couch rotation isocenter (±1 mm from baseline). The QA tests of the treatment couch include tabletop sag (2 mm from baseline), table angle (1°), table travel maximum range movement in all directions (±2 mm), and so on. Among these AAPM official reports on Linac QA, only the MPPG#8a explains the importance of frequent testing not only for the function of 4D to 6D couch alone but also for the accuracy of the device while interfacing with peripheral equipment such as the imaging system of the Linac. The report recommends monthly QA to test the absolute position of the 6D couch against the digital readout at the isocenter level. For relative measurements, the ability of the 6D couch to move a known amount to within 1 mm for translational moves and 0.5° for rotational moves over a clinical range should also be tested. In addition, the 6D couch with any positioning systems used clinically to set up the patient (eg, CBCT image guidance systems), and overall degrees of freedom should be checked. For example, a phantom (with a corresponding reference position/image of the phantom) could be shifted to an offset position, imaged, shifted back to the reference position via the positioning system, and reimagined or compared with reference marks to ensure that the table went to the correct location within the tolerance. 10
Due to lack of a well-defined acceptance test from the vendor that just ensures the installation is completed and functionality is enabled, we would include the verification of all mechanics within manufacturer’s specs as part of commissioning. There are several reports on the evaluation of 6D couches for radiation therapy. 11 –14 However, detailed commissioning and QA procedures are still unavailable for the third-party 6D couch systems, especially for the Protura system. Furthermore, the Protura system has several features that differ from the manufacturer 6D couch (Varian Medical Systems, Palo Alto, California). One such feature is “virtual pivot point” in which 6D corrections to the couch position are executed with the isocenter as the virtual pivot/reference point. The benefit of virtual pivot point is that the rotations will rotate according to the machine isocenter instead of the couch center.
To the best of our knowledge, this was one of the first few Protura systems installed in the United States, and there are few publications available for detailed QA guidelines and procedures of 6D couches, especially on the lack of procedures in dealing with a third-party 6D couch. Therefore, the present study can provide future users of the Protura system with a point of reference.
Methods
Specifications of Protura System and Tools
A Protura 6D couch was retrofitted and integrated to a Trilogy Linac equipped with OBI kV/CBCT (Varian Medical Systems) in 2017. The Protura 6D couch height was 15 to 20 cm and the weight was 84 kg (185 lbs). The readout of couch movement is in submillimeter or 0.1 mm resolution. There were 3 different speeds: slow, medium, and fast (4, 8, 16 mm/s) with a maximum patient load of 200 kg (440 lbs), which is similar to the typical Varian IGRT couch. However, when attached to the Varian Exact pedestal, the Protura weight limit was reduced to 163 or 169 kg (359 or 372 lbs), when using the UCT LE (Universal Couchtop Long Extension), or UCT 1 piece (Universal Couchtop 1 piece), respectively. Figure 1 shows the translational and rotational ranges of the couch. The crosshair of an LAP laser system (LAP Laser, Boynton, Florida) was used as the initial alignment reference for all tests that followed. A HexaCHECK MIMI phantom (Standard Imaging, Middleton, Wisconsin) and a custom-made cube (see section “Isocenter verification with a custom 6D QA phantom”) were used in the QA of the Protura system. A set of 30 × 30 cm2 solid water (Gammex RMI; Sun Nuclear Corp, Melbourne, Florida) slabs and an A12 ion chamber (Standard Imaging) were used in the couch transmission measurement as buildup material, and a regular ruler with millimeter resolution and digital water levels were also used.

Range of motion of a Protura 6 degrees-of-freedom couch.
Preinstallation Checklist
There is a checklist (see Table 1) that the site must provide to the vendor in advance to successfully integrate the couch to an existing clinical system.
Preinstallation Checklist.
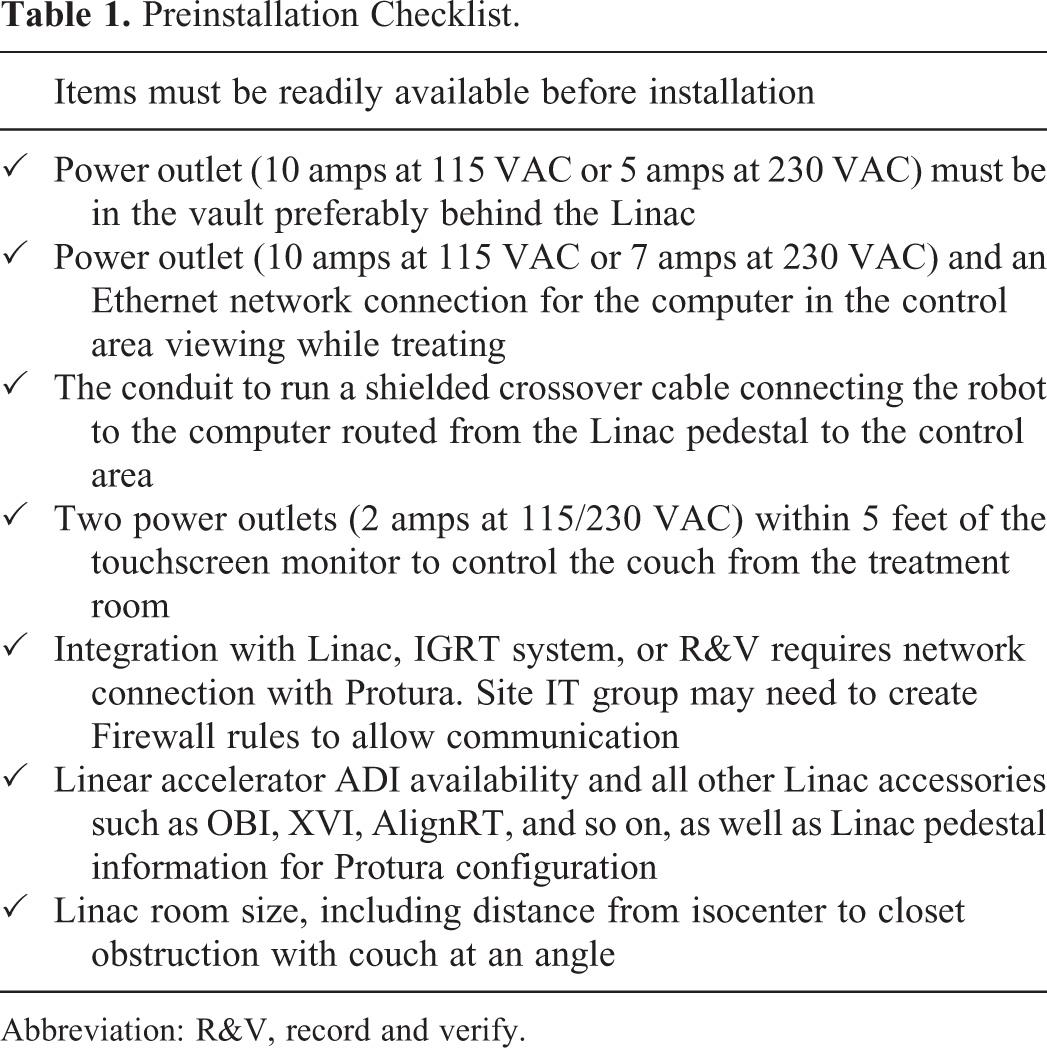
Abbreviation: R&V, record and verify.
On the other hand, the IT support team on-site must prepare to add the Protura system on the hospital network domain. Hospital-specific IT Security, Risk, and Control policies must be followed and communicated to the vendor prior to installation. For example, the vendor must allow the hospital IT to install the institution’s mandatory antivirus for the workstation to be joined to the network domain. Additional required information includes but is not limited to the maker, model, serial number, MAC address, segment, OS, RAM, and CPU of the Protura workstation. Figure 2 is the Deployment Architecture Diagram that shows network connectivities of the Protura system inside and outside of the Linac room.
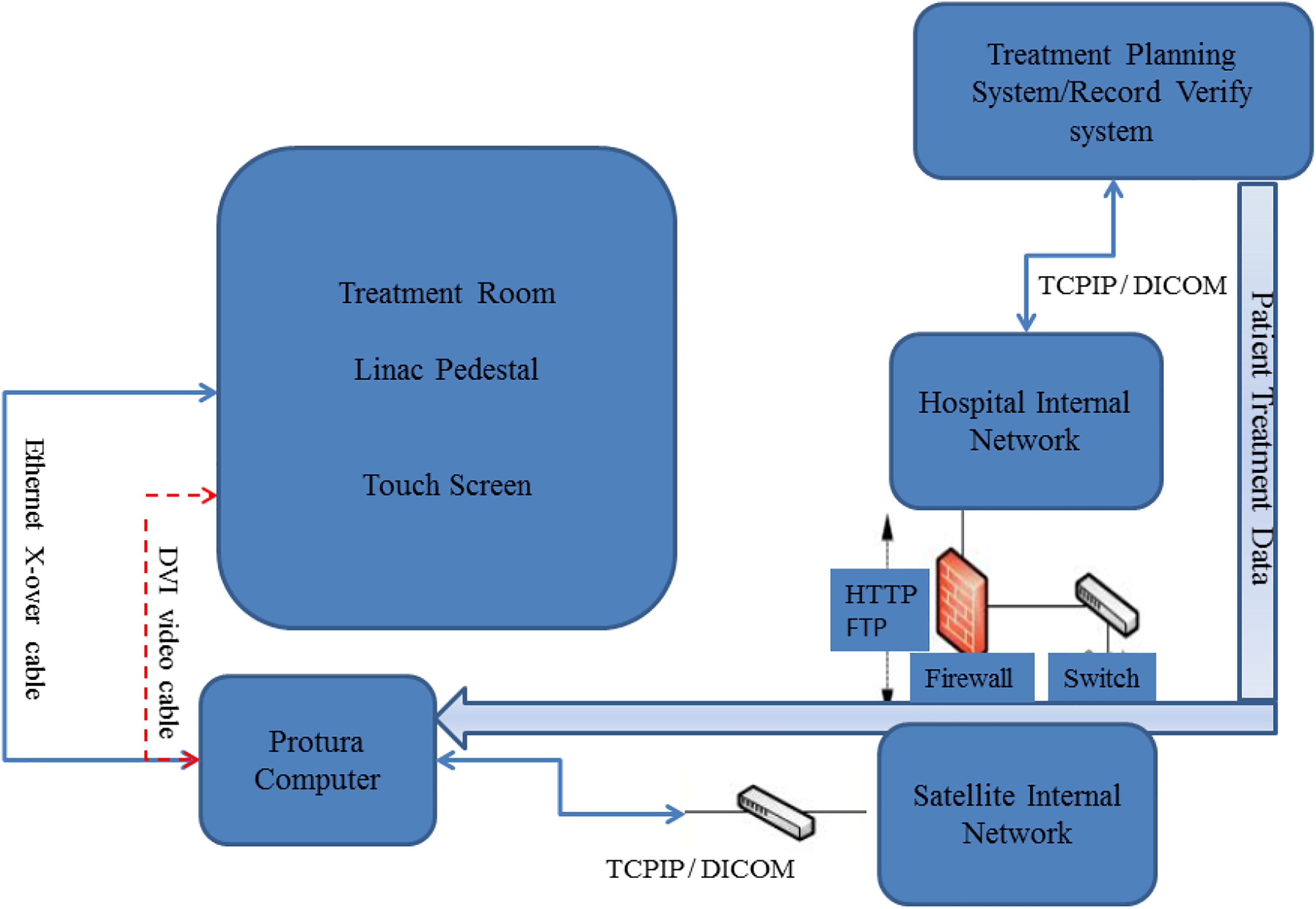
The deployment architecture diagram of the Protura system in connection with the Linac and hospital network.
Quality Assurance of Integration with Peripheral Equipment
The installation involved an invasive change to the clinical system. To ensure the integrity of the Linac, the acceptance test from the manufacturer involved performing Protura QA on image or CBCT acquisition, IGRT outputs, robotic couch shifts, and rotation corrections. The Protura system integration with the peripheral equipment, including integration with the record and verify, IGRT, and Linac couch systems, should be checked. An image transfer end-to-end test of the Protura system integration was carried out by a HexaCHECK MIMI phantom. First, the HexaCHECK phantom was scanned by CT, and the CT images were imported into the Eclipse treatment planning system (TPS). An external contour and a pair of 2-dimensional kV and CBCT setup fields were created and saved as a QA patient’s plan. The QA plan was scheduled in the record and verify system for imaging the phantom on the Protura 6D couch. The Protura couch was moved to the zero position before moving the pedestal with the phantom into the isocenter position using the laser marking system. Then, the couch was locked position in the Protura touchscreen before exiting the treatment room.
After kV images were taken, kV images of the HexaCHECK phantom should be displayed on the Varian OBI system. Image registration was performed to align the kV images with the CT images. The exact shifts recommended on the OBI system should be sent, and the exact shifts should be displayed on the Protura workstation. After the shifts were applied in the Protura system, the 6D couch should be moved automatically. Simultaneously, the shifts waiting on the OBI system should be canceled to avoid “double-shift.” Another CBCT imaging was acquired, and the images should be available in the off-line review (OLR). Note that after the shifts made through the Protura system, there should not be any shift shown in the OLR. A “Patient Move Report” should be automatically generated in Protura workstation at the completion of treatment.
Commissioning of Protura 6D Couch
Couch range limit
The Protura couch was leveled in all directions within 0.1° using a calibrated digital level. Besides level of couchtop and a Lok-Bar for correct fitting, the couch range limit of the Protura system was measured in 6 dimensions: longitudinal, vertical, lateral, and in 3 rotations: pitch, roll, and yaw. The Protura rotational limits are based on a number of factors, including the combination of the rotations, translations, magnitudes, directions, and isocenter position. The ranges were readout from the digital display of the Linac parameters inside the treatment room. The longitudinal, vertical, and lateral ranges that the 6D couch can travel are 24.6 to 149.5 cm, 43.9 to 0.0 cm, −20.6 to 20.7 cm, respectively. The maximum couch rotation for pitch, roll, and yaw are ±3° each. These values may increase/decrease based on translations (vertical having the largest impact), and other rotational shifts done in combination. The couch position values are defined exactly the same as those in the Varian couch coordinate system. Note that both longitudinal and vertical ranges were changed significantly from the IGRT couch due to the additional base volume of the Protura system on the Varian pedestal.
6 degrees-of-freedom couch position indicators
A ruler and a digital level were utilized to test the accuracy of the 6D movement. For absolute measurements, the absolute position of the couch was tested against the digital readout at the isocenter level. All measurements were performed without couch load. The tolerances of position indicators were 2 mm and 1 mm for absolute (Abs) and relative (Rel) values, respectively, that is consistent with the AAPM guidelines. 8 –10 At the isocenter level, the couch was programmed to move vertically, laterally, and longitudinally ±10.0 cm. The absolute couch shifts were compared against the digital readouts. Table 2 shows the couch position accuracy.
Sample of Couch Position Indicators Accuracy.

Isocentricity of couch pedestal and rotation indicators
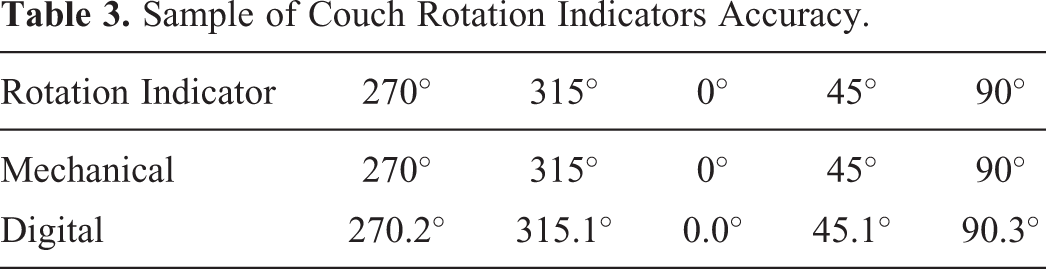
The isocentricity and rotation alignment tests used a piece of graph paper and pencil similar to the tests of the regular Linac couch. The graph paper was secured on the couchtop, and the couchtop was rotated at a different angle. Then, the mechanical versus digital indicators were compared. The tolerance of couch isocentricity was 2 mm diameter, and the tolerance of rotation indicators was 1° (<1 mm diameter and 0.5° for stereotactic radiosurgery/stereotactic body radiation therapy [SRS/SBRT] machine), according to the AAPM guidelines. 8 –10 Table 3 shows the measurement at the time of commissioning.
Sample of Couch Rotation Indicators Accuracy.
Couch sag and pitch baseline with approximately 200 lbs (∼91 kg) weight
The Protura couch sag was measured with a 200 lbs (∼91 kg) weight evenly distributed on the distal end (away from the pedestal) of the 6D couch. A ruler and a digital level were used to measure the sag in cm vertically and the degree in pitch rotation at the isocenter level when the couch was extended at the longitudinal position of 120 cm. The tolerance of couch sag was 2 mm from the baseline value, as determined at the time of commissioning (see Table 4).
Sample of Couch Sag Measurements.

Cone-beam computed tomography of a HexaCHECK MIMI Phantom
The HexaCHECK MIMI phantom tests multiple angular displacements at one time in pitch, yaw, and roll (see Figure 3). It serves as a surrogate for a patient who may or may not be perfectly localized on the treatment couch. The HexaCHECK determines the exact offset performance of the couch in millimeters and degrees and is used with Linac registration software (ie, OBI IGRT system). The phantom was exclusively designed to perform 6D couch commissioning and QA. 15 Refer to the white paper for more technical details. The HexaCHECK phantom was set at the laser isocenter with no rotations. The phantom is aligned to the offset marking on the MIMI phantom, and the rotations are applied in all 3 directions. Next, return to the OBI console and take an initial positioning image, the software should now have the new corrections to account for the applied rotations (ie, 1 -1.5° on pitch and roll each). Apply these couch corrections and once again reimage the phantom to ensure that the 6D couch went to the correct location within tolerances.

HexaCHECK MIMI phantom on the 6 degrees-of-freedom (6D) couch with laser alignment.
The tolerances should be 1 mm for translational moves and 0.5° for rotational moves over a clinical range. The CBCT images of the HexaCHECK MIMI phantom after 6D couch corrections are shown in Figure 4. The registration should only be performed on the MIMI phantom itself to avoid error from the geometric changes of the HexaCHECK portion. Keep in mind that the level should simply be removed before imaging.

Three orthogonal images of cone-beam computed tomography (CBCT) images of the HexaCHECK MIMI phantom after 6 degrees-of-freedom couch corrections.
Isocenter verification with a custom 6D QA phantom
Similar to section “CBCT of a HexaCHECK MIMI Phantom,” the isocentricity test can also be done using 2-dimensional kV imaging of a custom-made phantom. The HexaCHECK phantom provided by the Protura vendor at the time of installation can be used for commissioning, whereas the custom-made phantom can be used as a crosscheck of HexaCHECK and established baselines for subsequent routine QA tests when HexaCHECK phantom is not available in the clinic. The custom-made 7.5 × 7.5 × 7.5 cm cube with a 6-mm sphere at the center of the phantom was used for virtual and physics graticule alignment checks. The 2D kV images were taken with and without known rotations, such as 2° pitch and 1° roll. The isocenters with crosshair display on the kV images were compared with and without rotations. Figure 5 shows the display of Protura workstation that is interfaced with the Varian OBI system. The tolerance of crosshair centering was 1 mm. Figure 6 shows that the Protura system could accurately correct to the couch rotation position (2° pitch and 1° roll) executed with the isocenter as the virtual reference point. In routine monthly QA, a different combination of pitch and roll can be tested besides the commissioning values. For example, any 2 combinations of pitch, roll, and yaw could be sufficient if on a rotational basis (ie, different combination in even months and odd months).

Screenshots of the Protura workstation.

Custom-made phantom for isocentricity test. The crosshair indicates the isocenter position. AP indicates anterior–posterior; RL, right–left.
Couch attenuation measurement
An A12 cylindrical ion chamber with slabs of water-equivalent phantom was used for measuring the transmission factor of the Protura couch. The setup was 100 cm SAD, a field size of 15 × 15 cm and depth of 10 cm. With and without couch measurements were taken using the gantry angles of 0° and 180°. The purpose of this test was to identify the couch with the closest attenuation measurement to the couch (ie, IGRT couch) that was already built in the library in the Eclipse TPS. The transmission factors were measured and averaged to be 0.977 and 0.983 for 6 and 15 MV, respectively. Because the Varian IGRT couch is already available in the Eclipse TPS, and the transmission factors between 2 couches were similar, planners could insert the IGRT couch when planning on the machine with the Protura system.
Results and Discussion
The Protura system integration with the Varian Trilogy was verified. The Protura couch was shifted based on the image registration on the OBI system using the test plan of the HexaCHECK phantom, and the CBCT images were saved in the OLR. All functionalities were tested, and the results satisfied the manufacturer’s specifications. The Protura system can transfer correct translational and rotational shifts based on the OBI/CBCT system and therefore make the couch movement accordingly. The diameter of all crosshair projections on the graph paper at the couch isocenter level was within 1 mm (approximately 0.5 mm). The couch sag was 1.0 cm and 0.4° pitch rotation, which is larger than the typical IGRT couch sag (4-5 mm), probably due to the thinner couchtop. The couch sag (1.0 cm) will be used as baseline for a future QA test. The deviation from the reference position (zero position) of the HexaCHECK MIMI phantom, measured by matching the CBCT with the reference planning CT, was found to be below 0.2 mm in the anterior–posterior and right–left dimensions; 0.4 mm in superior–inferior dimension; and 0.1° in roll, pitch, and yaw directions.
The principle of this performance evaluation was to verify the requested shift by independent third-party methods. 11 We have reviewed all AAPM relevant TG reports and literature and adapted the recommended tolerances from the AAPM QA guidelines. Risk assessment has been performed, and a comprehensive commissioning and QA program have been compiled to ensure the safety and quality of precision radiotherapy for using this third-party 6D couch.
The overall process from searching for the product to acceptance of the Protura system was about 9 months and began with visiting sites with a third-party 6D couch. The evaluation team included a physician, physicist, and therapist to assess the workflow in their respective roles. Several follow-up visits from the prospective vendor followed to address questions, including the flexibility of mounting and indexing various patient immobilization devices on the couch, and concerns of all personnel on-site. Such sessions help facilitate the clinicians’ better understanding of the functionalities and safety features of the product. After the decision was made for purchase, hospital-wide IT safety assessment was required.
The installation of the Protura system was about 12 to 15 hours and required the site to schedule 1 day of downtime to complete installation and acceptance if the installation was not planned during a weekend. The coordination between the Protura installers, Linac engineers, facilities management, and IT is essential in the event the engineer requires access to information or resources. The Protura couch has the limitation of the total rotation magnitude being 3° because most other 6D couches can correct for 3° in each direction. Although the maximum pitch, roll, and yaw angle that can be compensated for by the Protura couch was 3°, the clinically achievable compensation could be significantly reduced depending on the longitudinal location of the couch.
Since the installation of the Protura couch, more than 500 data sets of translations and rotations have been generated and archived from the patients treated, most of who were prostate, head and neck, ablative gastrointestinal, and SRS brain patients. Although therapists and physicists have additional QA to perform daily and monthly, the therapists and physicians have been very pleased with the outcome of pretreatment image registrations. In addition, the patient setup time has been reduced significantly because the rotation can be automatically corrected with the 6D couch system.
The commissioning done in this work set the baseline for routine QA tests and verifies that the 6D couch is mechanically functional and operates within certain tolerances from absolute specified values. The absolute and relative tolerances for each of these 6D couches depend on the institution’s workflow and procedures. 10 Based on 1 year of experience of clinical implementation, the following QA regimen has been instituted, as shown in Table 5.
Routine Quality Assurance of Protura System.

Abbreviations: SBRT, stereotactic body radiation therapy; SRS, stereotactic radiosurgery; 6D, 6 degrees-of-freedom.
The functions and positioning accuracy of the Protura system have been evaluated. A 6D QA phantom is helpful for the commissioning and routine QA tests. Due to the third-party integration with Linac, the recommended shifts and rotation suggested on the OBI Console might be overdone by the therapists, which may result in double shifts/rotations by the OBI system. Thus, it is important to have a rigorous QA program to warrant the accuracy of the system. For example, a warning sign of “Cancel Shifts” could be placed nearby the OBI console to remind the therapists in case they are newly rotated to the 6D couch machine. Future work will include studies on long-term stability and overall performance with Linac.
Conclusions
A Protura 6D couch was accepted and commissioned successfully in our clinic. Quality assurance procedures for the third-party 6D couch were introduced. A 6D QA phantom is helpful for the commissioning and routine QA tests. Due to the third-party integration with Linac, the system is prone to “double-correction” errors. A rigorous QA program is the key to a successful clinical implementation of the Protura system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part through the NIH/NCI Cancer Center Support Grant P30 CA008748.