
Abstract
Purpose:
This article compares the dosimetric differences between jaw tracking and no jaw tracking technique in static intensity-modulated radiation therapy plans of large and small tumors.
Methods:
Eight plans with large tumor (nasopharyngeal carcinoma, volume range: 510.9 to 768.0 cm3) and 8 plans with small tumor (single brain metastasis, volume range: 5.3 to 9.9 cm3) treated with jaw tracking on Varian EDGE LINAC were chosen and recalculated with no jaw tracking to study the dosimetric differences. We compared the differences of organ-at-risk doses (Dmax, Dmean), monitor units, and γ passing rate of plan verification (3mm/3%, threshold 10%; 2mm/2%, threshold 10%) between the 2 techniques.
Results:
The organ-at-risk doses of nasopharyngeal carcinoma cases having jaw tracking are all less than those with no jaw tracking. The Dmax and Dmean of organ-at-risks reduced 0.61% to 17.65% and 2.17% to 19.32%, P < .05, respectively. In cases with single brain metastasis, the organ-at-risk doses with jaw tracking were also lower than no jaw tracking. The Dmax and Dmean of organ-at-risk doses reduced 0.84% to 1.52% and 0.90% to 1.86%, P < .05, respectively. The monitor units for the large tumor and small tumor were increased by 2.41% and 1.1%, respectively. The γ passing rates (3mm/3%, th10%; 2mm/2%, th10%) of nasopharyngeal carcinoma plans are 99.89% ± 0.06% (jaw tracking) versus 99.56% ± 0.19% (no jaw tracking; P = .127); 97.15% ± 0.98% (jaw tracking) versus 91.90% ± 1.40% (no jaw tracking; P = .000), and the γ passing rates (3mm/3%, th10%; 2mm/2%, th10%) of brain metastasis plans are 99.97% ± 0.05% (jaw tracking) versus 99.44% ± 1.24% (no jaw tracking; P = .251), 98.65% ± 1.27% (jaw tracking) versus 93.35% ± 2.72% (no jaw tracking; P = .000).
Conclusion:
Jaw tracking can reduce the dose of organ-at-risks compared to no jaw tracking, and the effect is more significant for plans with large tumor. The γ passing rate of plans with jaw tracking is also higher than the plans with no jaw tracking. Although the monitor units in plans of jaw tracking will increase slightly, it is recommended to use jaw tracking in static intensity-modulated radiation therapy both in large and in small tumors.
Introduction
Jaw tracking (JT) is a technique that was provided by Varian TrueBeam series, where the jaw can track the aperture of the multileaf collimator (MLC) to reduce the leakage and transmission and thus reduce doses of normal tissues around the tumor. 1,2 Most publications discussed the dose changes in several kinds of tumors, but very few articles studied the impact of tumor sizes and very few compared the intensity-modulated radiation therapy (IMRT) quality assurance (QA) verification results. Therefore, this study investigated the dose change in organ-at-risks (OARs), and the verification results of plans with JT both in large and in small tumors were compared to no JT (NJT), expecting the results can be beneficial for clinical treatment. In this study, we investigated the impact of JT on dose to OARs and the verification results (γ passing rates) of plans with large and small tumors.
Materials and Methods
Varian EDGE with HD120 MLC is used in the study, and the maximum field size with MLC is 40 × 22 cm. The width of MLC is 2.5 ´ 32 mm at the center and 5 ´ 28 mm at the peripheral. Portal Vision AS1200 with portal dosimetry (PD) is used for plan verification. AS1200 detector has an active area of 40 × 40 cm2 with 1190 × 1190 pixel arrays and pixel pitch of 0.336 mm which is suitable for both large- and small-field verification. 3 -5 The treatment planning system is Eclipse v13.6.
In this study, 8 static IMRT cases of nasopharyngeal carcinoma (NPC) and 8 static IMRT cases of single brain metastasis were chosen. All plans used sliding window technique with 6 MV photon beam. For NPC cases, 9 coplanar fields with 40° separation were used, and for brain metastasis cases, 10 to 12 noncoplanar fields were used. In each case, the JT IMRT plan was first designed, and the NJT plan was obtained from the JT IMRT plan by recalculating MLC sequence with no JT. The target doses of the 2 techniques were normalized to 95% volume of target received prescription dose in order to ensure the same target coverage. Meanwhile, the total monitor units (MUs) and doses of the normal tissues with the 2 techniques were compared by paired t test using SPSS22 Statistics Analysis Software. P < .05 was considered statistically significant.
All plans were verified with Varian PD. Composite fluence of all fields in one plan was used for γ analysis and 2 criteria were used for γ analysis: 3 mm, 3%, threshold 10% and 2 mm, 2%, threshold 10%. 6
Results
Target Volume
For NPC cases, all planning target volumes (PTVs) were combined to one target for volume measuring, and the target volume of brain metastasis was the PTV. All the target volumes are listed in Table 1.
Target Volumes of NPC and Brain Metastasis.

Abbreviation: NPC, nasopharyngeal carcinoma.
Dose of OARs
By comparing the dose–volume histogram (DVH) of OARs in JT and NJT plans for NPC, we found that both the maximum and mean doses of OARs in JT plans are lower than in NJT plans. Figure 1 shows the DVH comparison of OARs between JT and NJT of a representative patient (P1). The statistical analysis results are shown in Table 2.

Dose–volume histogram (DVH) comparison of nasopharyngeal carcinoma (NPC) organs at risk (OARs) of jaw tracking (JT) and no JT (NJT).
OAR Dose Comparison of Cases With NPC Between JT and NJT.

Abbreviations: JT, jaw tracking; NJT, no jaw tracking; NPC, nasopharyngeal carcinoma; OAR, organs at risk.
The maximum and mean doses of OARs in JT are smaller than in NJT, as shown in Table 2. The dose of lens reduced the most in JT plans, with the Dmax and Dmean reduced by 17.65% and 19.32%, respectively, while the impact on dose to larynx was not as significant, where Dmax and Dmean reduced by 0.61% and 2.17%, respectively. The reason could be that most part of the larynx is within the target volume, and the JT won’t impact the dose as significant as out-of-field OARs. For all the OARs assessed in Table 2, it is demonstrated that JT technique has a significant reduction in all OAR doses (Dmax and Dmean) when compared to NJT technique (P < .05).
In the single brain metastasis cases, the dose of OARs is also reduced in JT compared to NJT, but not as significant as that in NPC cases. Figure 2 shows the DVH comparison of OARs in the JT and NJT plans for single brain metastasis of a representative patient (P1). Although the DVH curve of each organ in JT is lower than NJT in Figure 2, the difference is not obvious. This trend can also be observed in Table 3.

Single brain metastasis dose–volume histogram (DVH) comparison of jaw tracking (JT) and no JT (NJT).
OAR Doses Comparison of Single Brain Metastases Between JT and NJT.

Abbreviations: JT, jaw tracking; NJT, no jaw tracking; OAR, organs at risk.
From Table 3, the OAR dose difference in JT and NJT plans is small: The reduction in Dmax ranges from 0.84% to 1.52% and the reduction in Dmean ranges from 0.9% to 1.86%, with P values all <.05. For the single brain tumor, the field size is small and the jaw size will not change much between JT and NJT, so the differences in the MLC leakage and transmission will be very small.
Verification Results and MU Comparison
Plans with either technique must be verified to ensure the deliver accuracy. This study verified all JT and NJT plans, and the results are shown in Table 4.
γ Pass Rate Comparison Between JT and NJT.

Abbreviations: JT, jaw tracking; NJT, no jaw tracking; NPC, nasopharyngeal carcinoma.
The γ pass rates of JT and NJT are slightly different at the 3 mm, 3%, and th10% γ pass criteria. Although the pass rates of JT are a little higher than NJT, the P values are >.05. Therefore, there is no significant difference between the 2 plans with the 3 mm, 3%, and th10% criteria. With the criteria of 2 mm, 2%, and th10%, the pass rates of JT plans are significantly higher than NJT technique both in large and in small tumors, with all the P values <.05.
We also compared the total MUs of JT and NJT plans. Table 5 shows the statistical results. The MUs of JT plans increased slightly compared to those of NJT plans, with the mean MU of NPC plan increased by 2.41% and the mean MU of brain metastasis plan increased by 1.10%.
MU Comparison between JT and NJT.
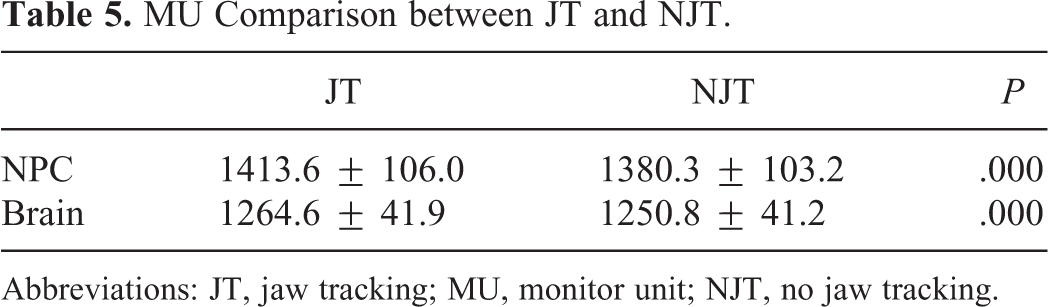
Abbreviations: JT, jaw tracking; MU, monitor unit; NJT, no jaw tracking.
Discussion
The article compared the doses of OARs (mean and maximum) and the plan verification results between JT and NJT static IMRT plans in small and large tumors. We found that the mean and maximal doses of OARs in JT plans were all lower than NJT plans with the same target coverage that is consistent with the results of other articles. 7 -11 The transmission of Varian HD MLC is about 1.2% for 6MV, 12 and the jaw transmission is <0.5%, so it is easier to reduce the OAR dose with JT. For small lesions, the field size is small, so the leakage to the OARs is also small. The impact of JT is more obvious in large tumor because the JT technique can block more MLC transmission in large field and reduce dose to out-of-field OARs. This finding is very helpful for plan design and can be specially applied in cases where low-dose sensitive normal tissues, such as the lung, 13 -15 are close to the treatment target. At the same time, JT technique can reduce the risk of secondary tumors in patients with longer survival periods, such as patients with breast cancer. 16
Plans with JT technique must be verified before treatment. In this study, we found that there was no significant difference in the γ passing rate between JT and NJT at the criteria of 3mm/3%, th10%, which is consistent with the result of Feng et al. 17 At the criteria of 2mm/2%, th10%, the pass rates of plans with JT are higher than NJT plans, with the P value <.05. The γ passing rate can be affected by many factors, such as MLC dose leaf gap (DLG), MLC leakage and transmission factor, output factor, jaw moving speed, and position accuracy. In the Varian TPS model, DLG and MLC leakage and transmission factor can be tweaked a little from the measurement value. The DLG is a parameter that accounts for Varian’s rounded MLC leaf ends and can affect the plan verification results a lot. The DLG value needs to be optimized at the stage of machine commissioning. The MLC leakage and transmission factor is an average value measured with large-volume ion chamber, 18–19 such as PTW30013 with a sensitive volume of 0.6 cm3. However, it actually varies with different positions of the MLC. 20 The difference cannot be discovered with the criteria of 3mm/3%, th10% due to its small influence, but with the criteria of 2mm/2%, th10%, the difference shows up. The JT technique can minimize the jaw size and reduce the MLC leakage and transmission so that the pass rates will increase.
Field size is smaller in JT than in NJT, and the output factor is much more difficult to measure in small field. Swinnen et al reported that it was more accurate with the fixed field 3 × 3 cm2 than JT in the very small tumor treatment. 21 Our study showed good γ passing rates in brain metastasis with small fields. It could be that the volumes of our brain metastasis in this study are not so small. Because there is no output factor of field size <3 × 3 cm2 in our PD model, PD can only measure the field size ≥3 × 3 cm2, so the verification results are still good in our brain metastasis plans. However, the smaller the tumor volume, the lesser the advantage of JT in dose reduction of OARs. So, when treating very small volume tumor with the field size less than 3 × 3 cm2, JT may not be a good choice.
In addition, we found that the MUs of JT plans were slightly higher than NJT, which was different from the article of Wu. 7 Target dose can also decrease with the decrease in the MLC transmission in JT; in order to compare the dose differences in OARs with the same tumor coverage, we renormalized the target dose. Meanwhile, the output factor is smaller in JT than in NJT due to the smaller jaw size, so the MU in JT should also be higher than NJT in order to get the same tumor dose. However, the increase in MU is very slight when using JT. The increase percentage of MU in NPC and single brain metastasis is 2.41% and 1.10%, respectively, which has little effect in the efficiency of treatment. Although the total MU is more in JT plan, the jaw size is smaller, most part of OARs is outside the field, and the jaw transmission is <0.5%, so increase in MU has little impact on OAR doses.
Conclusion
Jaw tracking technique can reduce the doses of OARs in static IMRT plans both in large and in small tumors, and the effect is more obvious in large tumors. The pass rates of plans with JT technique are also higher than NJT technique both in small (field size ≥3 × 3 cm2) and in large tumors. Although the MU of JT plan slightly increases, the effect in the efficiency of treatment is little, so it is recommended to use JT in static IMRT plan with the field size ≥3 × 3 cm2.
Footnotes
Acknowledgments
The authors would like to thank all study participants for their cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.