
Abstract
Purpose:
To evaluate the safety and efficacy of stereotactic body radiation therapy for primary lesion of renal cell carcinoma with long-term and regular follow-up of tumor size and renal function.
Methods:
This prospective study included 13 patients treated with stereotactic body radiation therapy for primary lesion of stage I renal cell carcinoma between August 2007 and June 2016 in our institution. Diagnosis of renal cell carcinoma was made by 2 radiologists using computed tomography or magnetic resonance imaging. A dosage of 60 Gy in 10 fractions or 70 Gy in 10 fractions was prescribed. The higher dose was selected if dose constraints were satisfied. Tumor response on imaging examination, local progression-free rate, overall survival, and toxicity were assessed.
Results:
The mean follow-up period was 48.3 months (range: 11-108 months). The tumors showed very slow but continuous response during long-term follow-up. Three cases (23.1%) showed transient progression during the short follow-up. The mean duration until the day on which partial response was confirmed among the partial or complete response cases was 22.6 months (95% confidence interval, 15.3-30.0 months). Local progression-free rate was 92.3% for 3 years and overall survival rate 91.7% for 2 years and 71.3% for 3 years. Twelve cases (92.3%) had impaired renal function at baseline. Renal function decreased slowly and mildly in most of the cases, but 2 cases of solitary kidney showed grade 4 or 5 renal dysfunction.
Conclusion:
All renal tumors decreased in size slowly but continuously for years after stereotactic body radiation therapy. Renal cancer can be treated radically with stereotactic body radiation therapy as a radiosensitive tumor, but careful attention should be given in cases with solitary kidney.
Introduction
Renal cell carcinoma (RCC) is the most common malignancy of the kidney. In 2016, approximately 63 000 patients were diagnosed with RCC, and 14 000 died of the disease in the United States. 1 In 2016 in Japan, approximately 9400 patients died of kidney cancer, which constituted 2.5% of all malignancy; moreover, the kidney cancer-related morbidity is increasing as Japan changes into an aging society. 2,3 Therefore, improving the diagnosis and treatment of RCC remains important.
Many guidelines recommend surgical resection as the standard strategy for localized, unilateral RCC. 4 –6 As an alternate and less invasive method, partial nephrectomy is considered in select patients with unilateral stages I to III tumors, uninephric state, bilateral renal masses, or familial renal cell cancer. In inoperable patients who have medical comorbidities, ablative techniques such as cryosurgery and radiofrequency ablation (RFA) can also be considered. Both of them need a percutaneous needle insertion for treatment. A meta-analysis showed that tumor progression was 12.9% with RFA and 5.2% with cryosurgery (P < .0001). 7 The use of these ablative techniques is limited to smaller tumors, those away from the ureter and renal pelvis, or patients without anticoagulative medications.
Radiotherapy is another nonsurgical definitive treatment option. Although the kidney surrounding the tumor in RCC is a radiosensitive organ, RCC has been thought to be radioresistant. 8 Therefore, palliative therapy is often the first step of radiation therapy for RCC. 9 As RCC is reported to have a lower α per β coefficient of the linear-quadratic model compared to other tumors, 10 high dose per fraction methods have shown good local control. The Gamma Knife, used for brain metastases, and stereotactic body radiation therapy (SBRT) for body metastases (eg, bone, lung, or kidney) have also shown good local control. 11 –14 Local control is reported as 82.6% to 95% for brain metastases and 91.9% for lung metastases. 11,12,14 In this SBRT era, in which the respiratory motion management or correction method enables stereotactic radiation therapy for body parts, hypofractionated radiation therapy and high-precision irradiation have the potential to maximize the treatment effect for the primary lesion of RCC, and minimize the adverse effect surrounding the tumors. 15 Although some studies have reported positive outcomes of SBRT for the primary lesion of RCC, it has not been clarified how the tumor size and renal function chronologically changes in a long-term follow-up. 16 –29 Therefore, this study aimed to evaluate the safety and efficacy of SBRT for the primary lesion of RCC with long-term and regular follow-up of tumor size and renal function.
Methods
We used a prospective study design, which was approved by the institutional review board at University of Yamanashi Hospital (approval number 525), and written informed consent was provided by every participant. Medical records were collected and analyzed for patients who were diagnosed with stage I (Union for International Cancer Control 8th) RCC and treated with SBRT for the primary lesion between August 2007 and June 2016 in our institution. All patients had been diagnosed as medically inoperable by urologists or had rejected surgical resection. Cases with a solitary kidney, cases with double cancer (cancer of another organ or previous RCC) were included. The diagnosis of RCC was made by 2 radiologists according to typical enhancement findings on dynamic contrast-enhanced computed tomography (CT). If a patient rejected the use of contrast material or had high serum creatinine levels, magnetic resonance imaging was performed as an alternative.
The planning of SBRT was carried out with the simulation CT in which contrast enhancement was used if possible. The slice thickness was 2 mm. The radiotherapy planning system that we used was XiO (Elekta AB, Sweden) or Pinnacle3 (Philips Medical Systems, Fitchburg, Wisconsin). The calculation algorithm for inhomogeneity correction was superposition. The patients were immobilized with the BlueBAG (Elekta AB) vacuum immobilization cushion. In each radiation therapy, the self-controlled breath-holding technique with Abches (APEX Medical, Japan) was used to manage respiratory movement. 15 Image-guided radiation therapy technique using the CT-on-rails system was performed before the delivery of each fraction. Target volumes were defined as follows: Gross tumor volume was equal to clinical target volume (CTV). Internal target volume (ITV) was defined as CTV with an internal margin (IM) of 2 to 4 mm. The IM depended on each patient’s reproducibility, which was evaluated with more than 3 CT series. Planning target volume (PVT) was defined as ITV with a setup margin of 3 mm. Non-coplanar static multiport (more than 5 ports) or dynamic arc (5 arcs, more than 400 degrees) was used for irradiation with a linear accelerator radiation therapy system. A dosage of 60 Gy in 10 fractions or 70 Gy in 10 fractions was prescribed to isocenter, 95% volume covering ITV or 95% volume covering PTV (Table 1). Higher dosage was selected if dose constraints around the target kidney were satisfied. Used dose constraints of organ at risk are listed in Table 2. The dose of contralateral kidney if existed was not concretely restricted but reduced as much as possible as far as it did not conflict with other dose constraints.
Details of Treatment.

Abbreviation: CT, computed tomography; CTV, clinical target volume; fr, fraction; GTV, gross target volume; ITV, internal target volume; PTV, planning target volume.
Dose Constraints.a
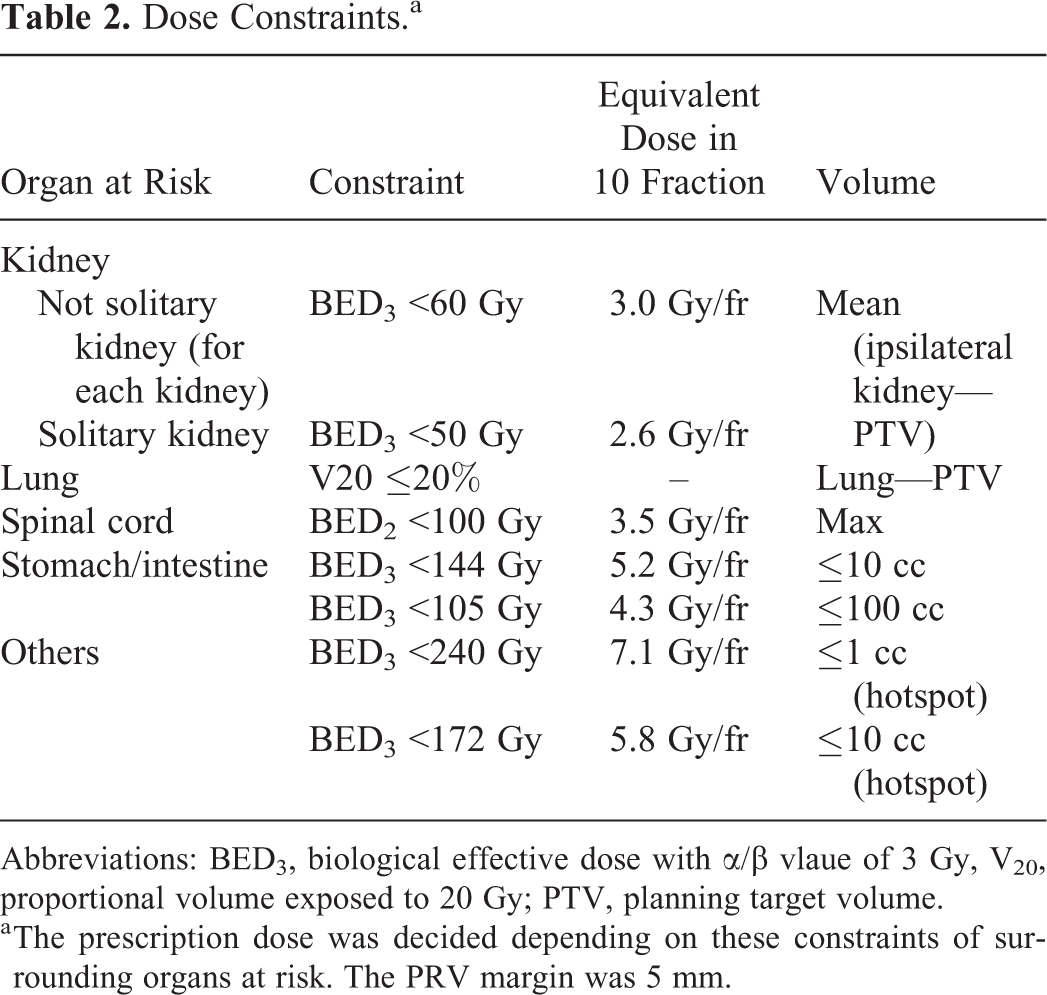
Abbreviations: BED3, biological effective dose with α/β vlaue of 3 Gy, V20, proportional volume exposed to 20 Gy; PTV, planning target volume.
a The prescription dose was decided depending on these constraints of surrounding organs at risk. The PRV margin was 5 mm.
The interval of follow-up was 2 to 3 months until 2 years after treatment, and 6 to 12 months after that. The follow-up duration was defined as the time between the first day of irradiation and the last follow-up. To evaluate adverse events, patient examination by a radiation oncologist and a blood test that included serum creatinine level were performed on each visit. Local progression-free rate and overall survival rate were assessed with the Kaplan-Meier method. Progression-free survival was not assessed in this study, as the progression of some of the cases was difficult to judge, particularly in cases of double cancer. Evaluation of tumor response was made by contrast-enhanced or non-contrast-enhanced CT according to the Response Evaluation Criteria In Solid Tumors. 30 Local progression was defined as complete response, partial response, or stable disease of the primary lesion treated with SBRT. Among the cases that showed partial response or complete response, the duration before the partial response was evaluated. Acute and chronic toxicities were assessed with Common Terminology Criteria for Adverse Events version 4.0. In particular, estimated glomerular filtration rate was used to investigate adverse events of chronic kidney disease (CKD). 31 The software for statistical analysis was R (version 3.3.2) and the “survival” library (version 2.39-5) for survival analysis.
Results
This study included 13 patients with stage I RCC. The baseline characteristics of patients, parameters of radiotherapy planning, and clinical course are shown in Table 3. The median age was 72 years (range: 59-81). Among 5 patients, reasons for past history of nephrectomy were the following: contralateral metachronous RCC (4 cases) and contralateral adrenal carcinoma (1 case). The stage was I in all of the cases (12 T1aN0M0 and 1 T1bN0M0). The median tumor size was 19 mm (range: 9-43). One operable patient rejected a proposal of surgery because postoperational initiation of hemodialysis was needed. Six patients were judged as high-risk operable for the following reasons: a necessity of initiation of dialysis after surgery (4 cases), a state of low liver function (1 case), and past history of esophagectomy and gastrectomy (1 case). Reasons for inoperable cases were as follows: uncontrolled type I diabetes mellitus, interstitial pneumonia, and current ongoing treatment of cholangiocarcinoma.
Patient Characteristics.

Abbreviations: CKD, chronic kidney disease; F, female; L, left; M, male; PR, partial response; PS, performance status; PTV, planning target volume; R, right; SBRT, stereotactic body radiation therapy; SD, stable disease.
The mean follow-up period was 48.3 months (range: 11-108 months). A case of dose distribution using static multiport SBRT and follow-up CT examination after treatment is shown in Figure 1. The tumors showed very slow response, and as a result most cases reported partial response with gradual, long-term reduction of size (Figure 2). Three cases showed transient progression during the short period of follow-up. Six patients showed partial response, and 6 had stable disease of the local lesion. The mean duration until the day on which partial response was confirmed among the partial or complete response cases was 22.6 months (95% confidence interval, 15.3-30.0 months).
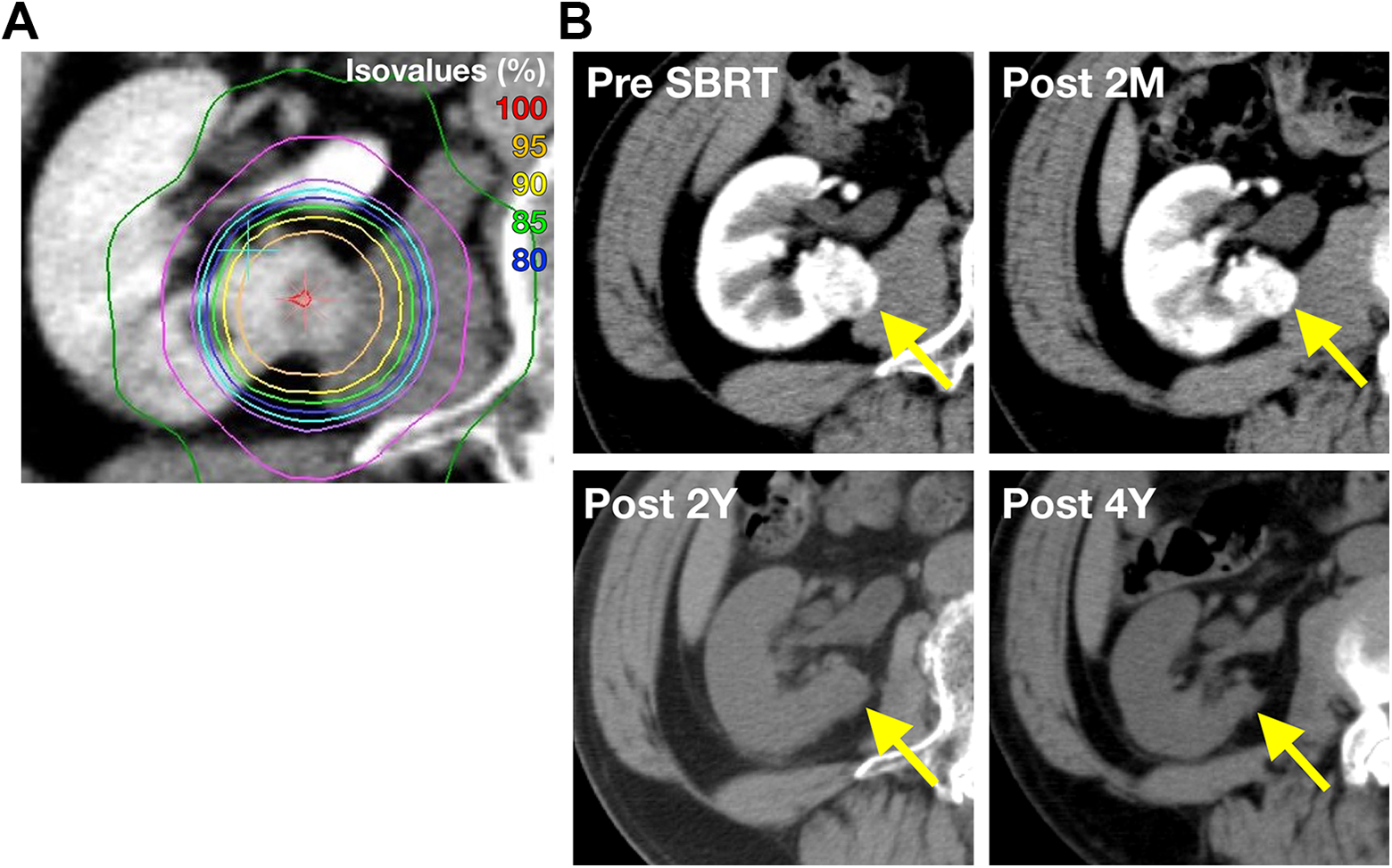
Case presentation. A, The dose distribution of case 1 treated with SBRT using static multiport. B, Follow-up CT examinations showed tumor response of partial response. The tumor showed very slow but continuing response. SBRT indicates stereotactic body radiation therapy; CT, computed tomography.

Tumor size change in percent of pre-SBRT is shown. Most tumors demonstrate very slow response. Three cases increased temporally and showed tendency to decrease in size. Only one case relapsed about 1 year after SBRT. SBRT indicates stereotactic body radiation therapy.
Case 4 was an autopsy case. 32 He died of progression of hepatocellular carcinoma and liver dysfunction. Histologically, almost the entire tumor showed hemorrhagic necrosis. In case 11, a local recurrence (progressive disease) was reported on contrast-enhanced CT images 1 year after treatment, and surgical resection was performed. On histopathological examination, necrotic tissue, which was thought to be a treatment effect, and residual tumor were confirmed.
In the survival analysis, local progression-free rate was 92.3% for 3 years (Figure 3). Overall survival rate was 91.7% for 2 years and 71.3% for 3 years. The causes of death were as follows: renal failure (1 case; grade 5), other cancer (2 cases; intrahepatic cholangiocarcinoma and hepatocellular carcinoma), infectious pneumonia (1 case), and acute subdural hemorrhage (1 case). Two adverse events excluding CKD were reported: acute dermatitis, grade 1 (1 case); and back pain, grade 1 (1 case).
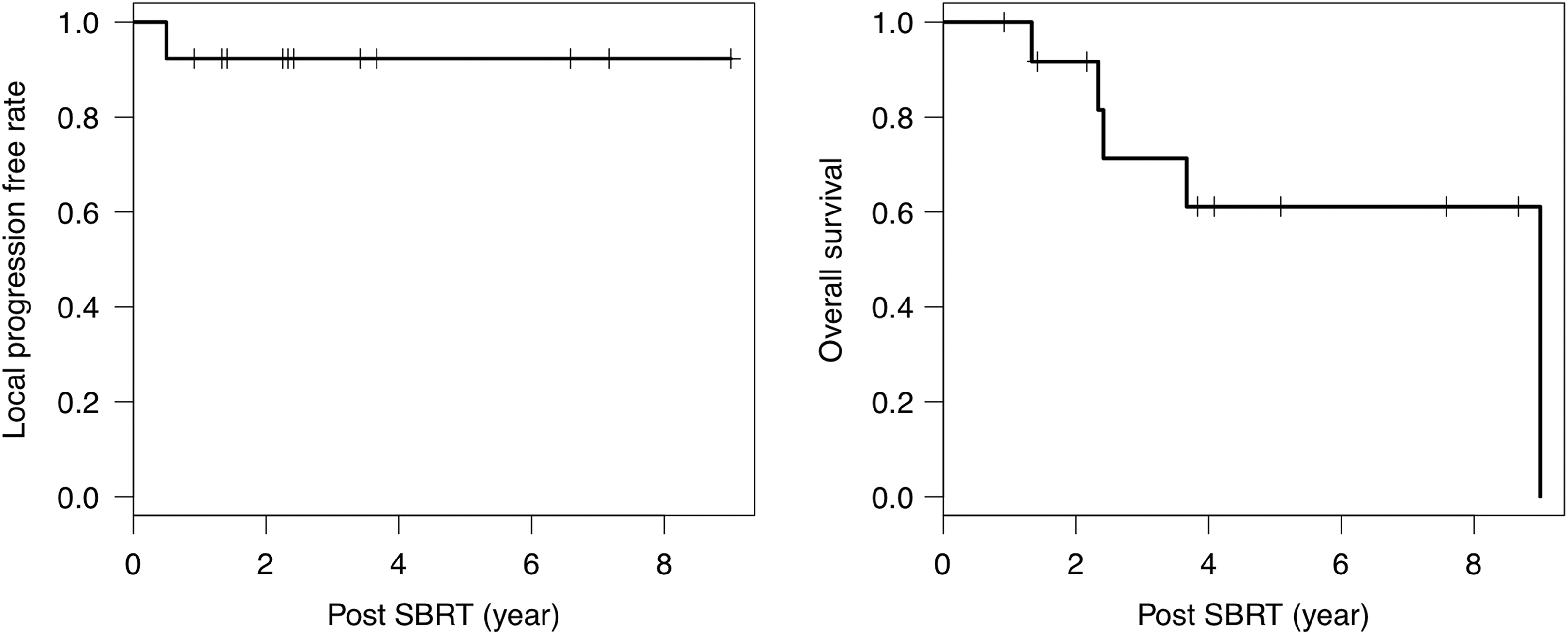
Survival analyses. The survival analyses using Kaplan-Meier method. Local progression-free rate was 92.3% for 3 years. Overall survival was 91.7% for 2 years and 71.3% 3 years.
Adverse events of CKD are shown in Figure 4. Twelve cases 13 (92.3%) had renal dysfunction at baseline: grade 1, 5 cases; grade 2, 5 cases; and grade 3, 2 cases. The CKD grade of 11 cases increased mildly after SBRT. In 2 cases, the CKD grade did not change between pretreatment and post-treatment.

Comparison of CKD grade. Comparison of eGFR (mL/min/m2) between pre-SBRT and post-SBRT. Grade of CKD are also colored. In most of cases, the serum creatinine level decreased after SBRT but mildly. One grade 5 event was reported, but the association between treatment and death was unclear because it occurred 9 years after treatment. CKD indicates chronic kidney disease; eGFR, estimated glomerular filtration rate; SBRT, stereotactic body radiation therapy.
One case of grade 5 CKD was reported after the treatment. This case had been affected with grade 2 CKD before SBRT due to contralateral nephrectomy for previous RCC. After treatment, creatinine level was stable, and hemodialysis was not initiated until the observation of an adverse event of grade 5 CKD, 108 months after SBRT. The onset of renal failure was sudden. Therefore, it was not clear whether the treatment for RCC caused grade 5 CKD in this case.
One additional case of initiation of hemodialysis (grade 4 CKD) was reported. This case showed grade 2 CKD before SBRT as a result of past history of contralateral nephrectomy. The creatinine level gradually increased after treatment. The follow-up CT images showed a trend of normal kidney parenchymal atrophy surrounding the tumor. The hemodialysis was initiated 1 year and 3 months after treatment.
Discussion
The present study demonstrated the efficacy and safety of SBRT for the primary lesion of RCC. The local progression-free rate for 3 years was 92.3%. This local control rate is similar to previous literature on the efficacy of SBRT for the primary lesion of RCC, ranging from 84% to 100%. 17 –19,24 –28,33 One in vitro study using a human RCC cell line showed a lower α per β based on the linear quadratic model (2.6 for A498 and 6.92 for Caki-1) and exponential cell decreasing above single 6 Gy irradiation. 10 This suggests the effectiveness of high dose per fraction for RCC. However, Siva et al conducted a prospective study of 37 patients treated with SBRT for the primary lesion of RCC and reported the local control rate was 100% for 2 years using a single fraction of 26 Gy for small (<5 cm) lesions, 29 which was equivalent to 251 Gy in BED3.0 and higher than our study. Siva et al presented a multiinstitutional consensus statement in regard to the indication and SBRT method for primary RCC based on a survey from 8 international institutions. 34 Five institutions applied size constraints of the tumor within 5 to 8 cm, the total PTV expansion was 3 to 10 mm around gross target volume, and the number of fractions used were 1 to 12 to a total dose of 25 to 70 Gy. They also reported that multifraction SBRT was more strongly associated with poorer progression-free survival than was single-fraction SBRT in a pooled analysis of SBRT for primary RCC. 35 The prescribed dose of our study was calculated as 180 Gy (60 Gy/10 fractions) or 233 Gy (70 Gy/0 fraction) in BED3.0, which is a high-dose prescription in a previously reported multifractionated regimen. 17,18,25 –28,33 We considered it was acceptable because the PTV margin was comparatively small by using a CT-on-rail system and breath-holding technique. However, we had 2 cases with severe chronic renal dysfunction in the study; therefore, lower BED in multifraction SBRT or single-fraction SBRT might be desirable. Further study is mandatory to clarify the ideal dose and fractionation regimen for RCC.
To our knowledge, this study is the first report concerning the time course of tumor size when treated with SBRT using an x-ray beam. The 2 key features of the time course of RCC response were a very slow but continuous shrinkage of tumor size and transient progression during short period follow-up. Mori et al reported that brain metastases of RCC, when treated with stereotactic radiosurgery, showed slow reduction is size of the tumor and occasionally enlarged on contrast-enhanced imaging before regression. 36 In another study of the initial experience of carbon ion radiotherapy for the primary lesion of RCC, Nomiya et al found that 4 (40%) cases among 10 tumors showed transient progression that reached a tumor size change of 120% temporally. 19 These reports are consistent with our results. Because of these features, attention should be paid when tumor response of RCC is evaluated. Siva et al reported the neutrophil-to-lymphocyte ratio as a predictor of tumor shrinkage in a prospective clinical trial of stereotactic ablative body radiotherapy for the primary lesion of RCC. 29 The pseudo-progression is occasionally reported in the field of immune check-point blockade. 37 These results suggest that immune reaction may contribute to tumor shrinkage or transient progression. It will be useful to distinguish transient progression from true progression of disease if a factor is detected for not only tumor shrinkage but also transient progression. Further study is needed in this area.
The evidence of kidney toxicity by SBRT is still limited. Staehler et al used CyberKnife for single-fraction SBRT 16 for initial treatment of primary RCC and reported the median creatinine clearance difference between pretreatment (76.8 mL/min) and post-treatment (70.3 mL/min) was not significant (P = .89). In this study, renal function decreased slowly and mildly in most cases, even in patients who had impaired renal function at baseline. Although comparison of toxicity with previous reports was difficult due to difference of renal function at baseline, late toxicity of SBRT for primary lesion of RCC with impaired pretreatment renal function seemed to be permissive. However, 2 cases of solitary kidney showed grade 4 or 5 renal dysfunction. Therefore, careful attention should be paid in cases with solitary kidney. Furthermore, additional examination of the appropriateness for a radical treatment would be necessary in such renal dysfunction cases. According to the NCCN guideline, 38 active surveillance is an option for the initial management stage T1 RCC in particular when the tumor is small (<2 cm) or the patient has a risk of severe morbidity from intervention.
The difficulty in predicting efficacy of SBRT for the primary lesion of RCC with impaired renal function at baseline still remains. In this study, the CKD grade of 4 cases increased (grade 2 -3, 3 cases; grade 3-4, 1 case). One case of grade 5 CKD adverse event was reported in our study. This case was affected by renal dysfunction at baseline, and the creatinine level was stable until the event occurred. In this case, it was difficult to identify the relation between the treatment and the event, as it occurred 9 years post-treatment. Yamamoto et al investigated the predictors for post-treatment kidney atrophy and reported that V20–V30 had strong correlation with post-treatment irradiation kidney volume (r < −0.70, P < 0.01). 8 These predictors for late adverse events of the kidney could perhaps contribute to improve and optimize the indication of SBRT for the primary lesion of RCC. However, to establish the dose constraints for impaired kidneys, further prospective study is needed.
There were some limitations in our study. First, no case had histological confirmation of the tumors. We set the study design for such patients in whom it was difficult to acquire pathological confirmation due to the patients’ poor condition or refusal to undergo a surgical procedure. Therefore, we allowed diagnosis of RCC by radiological imaging. However, it was possible that benign tumor might be included in the findings and there would be some difference of local response and prognosis among various histological types. Second, the number of cases was not sufficient to conclude late local effect and toxicity with high reliability. More cases with longer follow-up are mandatory to demonstrate the reliability.
In summary, all renal tumors decreased in size slowly but continuously for years after SBRT. Renal cancer can be treated radically with SBRT as a radiosensitive tumor, but careful attention should be paid in cases with solitary kidney.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI grant number JP16H05389).