
Abstract
Background and Objective:
Claudin-7 is a component of tight junctions and plays important roles in maintaining cell polarity and tightly connecting the barriers between cells. Abnormal claudin-7 protein expression is closely related to tumor occurrence, development, and metastasis. This study aimed to investigate the correlation between claudin-7 expression and carcinogenesis or metastasis in colorectal cancer and the clinical significance of these relationships.
Materials and Methods:
In this study, enzyme linked immunosorbent assays (ELISA) were used to measure the claudin-7 levels in serum from patients with colorectal cancer. Immunohistochemical staining and Western blotting were used to measure claudin-7 expression in colorectal cancer tissues, paracancerous tissues, and metastatic tissues.
Results:
Serum claudin-7 levels were significantly lower in patients with colorectal cancer than in healthy controls. Immunohistochemistry indicated that claudin-7 expression was lower in colorectal cancer tissues than in normal colorectal tissues, and its expression level was positively correlated with the degree of colorectal cancer tissue differentiation. Claudin-7 expression levels were significantly reduced or undetectable in metastatic tissues compared to primary tumor tissues, but there were no significant differences in claudin-7 expression among different metastatic tissues.
Conclusion:
We confirmed that claudin-7 downregulation was associated with colorectal cancer and metastasis. Claudin-7 could be a tumor suppressor gene for colorectal cancer and may thus serve an early diagnostic marker and a novel therapeutic target.
Introduction
Colorectal cancer (CRC) is one of the most common malignant tumors of the digestive system and is a serious threat to human health. Colorectal cancer incidence is the third highest in the world, second to only lung cancer and breast cancer incidence. 1 With improvements in living standards and changes in diet structure, the incidence of CRC continues to increase. 2 In developed regions such as Europe and United States, the incidence and mortality of malignant CRC tumors rank fourth and second, respectively. 3 Colorectal cancer invasion and metastasis are important causes of postoperative recurrence and poor prognosis, and one of the most common CRC metastasis sites is liver. 4 More than 50% of patients with CRC have liver metastases during the disease, and approximately 20% to 25% of patients have CRC and liver metastases simultaneously; finally two-thirds of patients with CRC die of liver metastasis. 5
The abnormality and destruction of tight junction structure and function between cells are important contributors to the distant invasion and metastasis of malignant tumor cells. Tight junctions comprise membrane proteins, such as occludin, claudin, and junctional adhesion molecules, and cytoplasmic proteins, such as zona occluden (ZO)-1, ZO-2, and ZO-3. 6 Claudin-7 (Cldn7) is one of the main members of the claudin family. In recent years, abnormal Cldn7 expression has been closely related to the development of various malignant tumors. 7 -10 The downregulation or deletion of Cldn7 and other tight junction proteins is considered to be the mechanism of intercellular adhesion loss and an important step in tumorigenesis and metastasis. 11
To investigate the relationship between Cldn7 and CRC carcinogenesis and metastasis, we used double-antibody sandwich enzyme linked immunosorbent assays (ELISA) and immunohistochemical (IHC) staining to determine Cldn7 levels in patient serum and CRC tissues. We also measured Cldn7 expression in tissues with different degrees of CRC differentiation and liver metastases by Western blotting.
Materials and Methods
Patients and Samples
Blood samples were obtained from 31 patients with a definitive diagnosis of CRC. All of these patients were diagnosed at the Cancer Center of Beijing Shijitan Hospital (Beijing, China) between 2016 and 2017. Blood samples from 9 healthy people were collected for a control group. Serum samples were separated from the cellular elements by centrifugation (3000 r/min × 15 minutes) within 2 hours of collection. A double-antibody sandwich ELISA was used to determine the levels of Cldn7 in the samples. The patient data were collected from the electronic database at Beijing Shijitan Hospital. The data included age, sex, tumor location, differentiation grade (low, median, high), perineural invasion status (yes or no), p53 gene (p53) mutation status (mutant or wild type), carcinoembryonic antigen (CEA) level, carbohydrate antigen (CA)19-9 level, and α-fetoprotein (AFP) level. 5
Tissue microarrays were collected from 75 patients with CRC who did not have preoperative radiotherapy or chemotherapy. Postoperative specimens were proven to be colorectal adenocarcinoma by pathology. For each patient, adjacent tissues more than >5 cm away from the tumor were also collected. All of these samples were confirmed to be normal colorectal tissues by pathology. Tissue microarrays were conducted with 75 CRC tissue samples and corresponding paracancerous and metastatic tissue samples. The IHC staining was used to determine Cldn7 expression. The patient data included age, sex, tumor diameter, grade of differentiation, lymphatic metastasis, other organ metastasis, tumor invasion depth, tumor, lymph node, metastasis (TNM) stage, and survival time.
A total of 30 fresh CRC tissue specimens were collected at our hospital from 2013 to 2015. None of the patients were treated with radiotherapy or chemotherapy before the operation. The postoperative specimens were confirmed as colorectal adenocarcinoma by pathology. Among them, there were 10 cases of well-differentiated adenocarcinoma, 10 cases of moderately poorly differentiated adenocarcinoma, and 10 cases of CRC liver metastasis. Normal intestine tissues were used for the control group. The Cldn7 expression for different CRC differentiation levels and liver metastases was detected by Western blotting. All assay protocols for patients were reviewed and approved by the Medical Ethics Committee of the Beijing Shijitan Hospital Affiliated Capital Medical University Institutional Review Board.
ELISA
A double-antibody sandwich ELISA kit (cat. HG38912; Bio TSZ, USA) was used to determine Cldn7 levels in patients and healthy controls. Fifty microliters of standards or samples was added to the appropriate well of an antibody-precoated microtiter plate and then mixed gently. After incubation at 37°C for 45 minutes, the liquid was removed. Diluted biotinylated anti-Immunoglobullin G (IgG) and streptavidin-horseradish peroxidase (HRP) were added to all wells and incubated for 30 minutes at 37°C. Then, chromogen solution was added to each well. After incubation for 15 minutes at 37°C, a stop solution was added to each well, and the blue to yellow color change indicated that the reaction stopped. The blank well was set to zero, and the colored reaction product was measured using an automated ELISA microplate reader at 450 nm. The results are expressed as picograms per milliliter.
Immunohistochemical Staining Assay
For hematoxylin and eosin (HE) staining, tumor, paracancerous, and metastatic tissues were labeled. All tissues were embedded into wax blocks and cut into paraffin sections. Xylene was used to dewax the paraffin slices. Different concentration gradients of alcohol were then used for hydration. Tissue sections were incubated for 10 minutes in 3% H2O2 and washed with 0.01 mol/L phosphate buffered saline (PBS). Then, the sections were incubated with a diluted rabbit polyclonal anti-Cldn7 antibody (ab27487, 1:200; Abcam, USA), followed by incubation with the corresponding secondary antibody (ab175780, 1:1000; Abcam). After that, the proteins were developed in diaminobenzidine (DAB) for coloration. Hematoxylin was used to stain the nuclei, and different concentration gradients of alcohol were used for dehydration. Neutral gum was used to seal the slides.
Western Blotting
Appropriate amounts of CRC, normal colorectal, and liver metastasis tissues were added to eppendorf (EP) tubes. Then, equal amounts of grinding beads and 1 mL of total protein extraction reagent containing various protease inhibitors were mixed with the tissues. Next, the total protein was extracted by grinding with a tissue homogenizer. The proteins were separated by sodium dodecyl sulfate (SDS)-polyacrylamide gel electrophoresis and transferred onto a nitrocellulose (NC) membrane. The membrane was blocked with Tris Buffered saline Tween (TBST) solution containing 5% skim milk for 1 hour. Next, the membrane was incubated with a diluted rabbit polyclonal anti-Cldn7 antibody (ab27487, 1:1000; Abcam) at 4°C overnight, followed by incubation with a donkey anti-rabbit IgG antibody (1:10 000, ab175780; Abcam). Finally, a Western blot scanner was used to visualize the blots. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used as the internal reference.
Immunohistochemical Staining Classification
Brown granules on the cell membrane indicated positive results. A semiquantitative method was used to score the samples. Colorless, light yellow, light brown, and deep brown staining intensities were recorded as 0, 1, 2, and 3, respectively. The number of positively stained cells was determined as follows: 5 visual fields were observed for each section, and the percentage of positive cells was recorded. The total score was the product of the staining intensity score and the percentage of positive cells; ≤10% was scored as 1, 11% to 50% as 2, 50% to 75% as 3, and ≥75% as 4. A total score ≥3 was positive, and a total score <3 was negative.
Follow-Up
In total, 63 of 75 patients whose tissues were IHC stained were followed up. The median survival time was 45 months, and the patients were divided into 2 groups according to different survival periods. The relationship between IHC staining results and survival times was then analyzed.
Statistical Analyses
Statistical analyses were performed using IBM SPSS version 17.0 for Windows and GraphPad Prism version 6.0 for Windows. The measurement data are expressed as the mean (standard deviation). The Mann-Whitney U test was used to compare differences in Cldn7 serum levels. The correlation between Cldn7 expression and clinical pathological parameters was analyzed using the χ2 test. Claudin-7 expression determined by Western blot was analyzed using Student t test. Differences were considered significant when P < .05.
Results
Clinical Characteristics of Patients Included in the ELISA Experiment
In this study, blood samples from 31 patients with CRC who were diagnosed at our hospital from 2016 to 2017 were collected. The personal information and disease characteristics of these patients are shown in Table 1.
Clinical Characteristics of Patients Included in the ELISA Experiment.
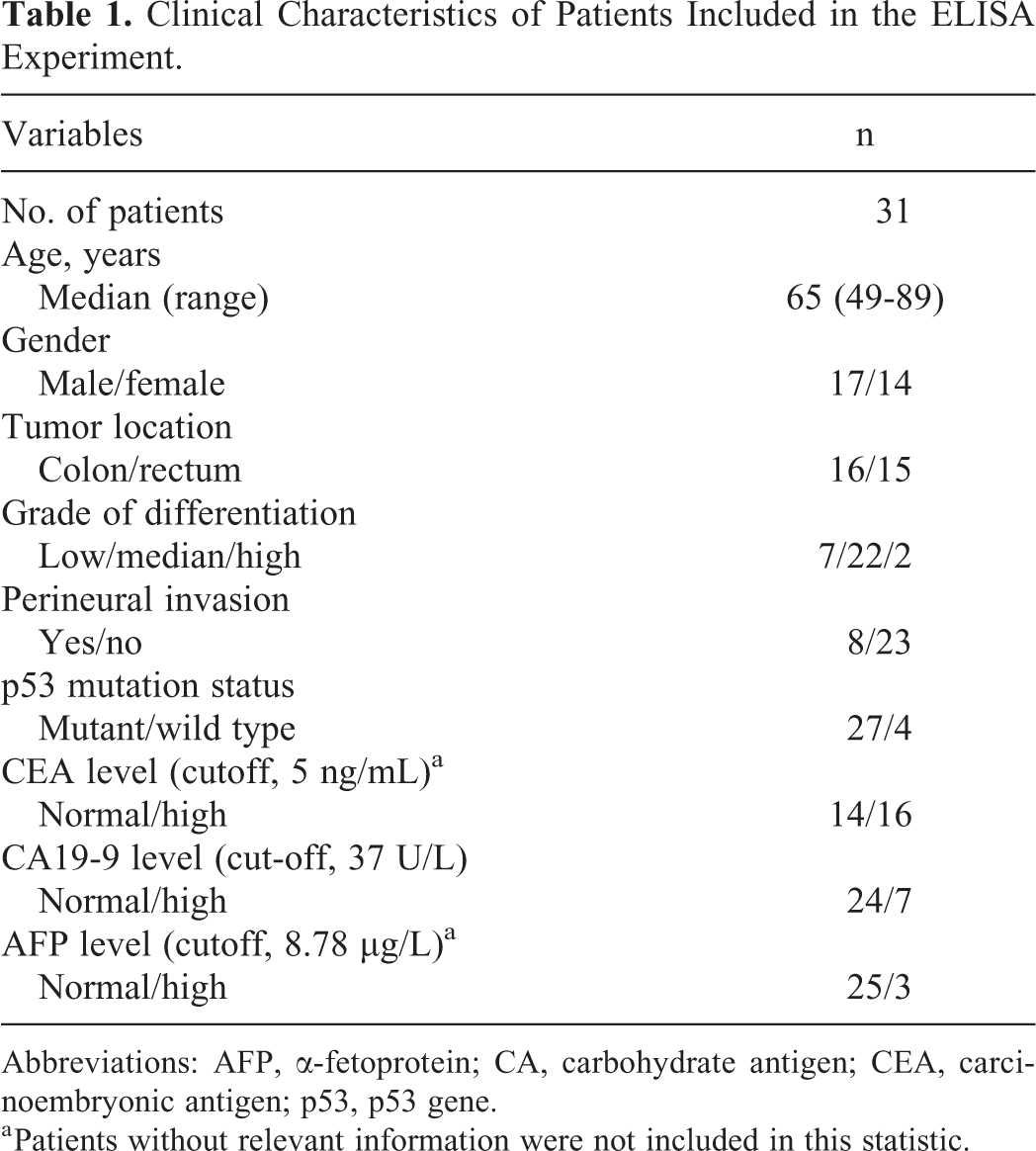
Abbreviations: AFP, α-fetoprotein; CA, carbohydrate antigen; CEA, carcinoembryonic antigen; p53, p53 gene.
a Patients without relevant information were not included in this statistic.
The overall median age was 65 years (range, 49-89 years), with a male predominance (n = 17, 54.8%). The tumors were located in the colon (n = 16, 51.6%) and the rectum (n = 15, 48.4%). According to the World Health Organization (WHO) histological grade, there were 2 cases of high-moderate adenocarcinoma differentiation (6.4%), 22 cases of moderate adenocarcinoma differentiation (71%), and 7 cases of moderate-low or low adenocarcinoma differentiation (22.6%). Laboratory examination showed that there were 4 patients with the wild-type p53 and 27 patients with the mutant type. There were 14 patients with normal serum CEA levels (<5 ng/mL) and 16 patients with elevated CEA levels (46.7% vs 53.3%). The CA19-9 levels were normal (<37 U/L) in 24 patients and increased in 7 patients (77.4% vs 22.6%). Serum AFP levels were normal (<8.78 μg/L) in 25 patients and increased in 3 patients (89.2% vs 10.7%). Patients without relevant information were not included in this analysis.
Comparison of Serum Cldn7 Levels Between Patients With CRC and Healthy Controls
The serum Cldn7 levels of patients with CRC and healthy controls are shown in Table 2. Serum Cldn7 levels were significantly lower in patients with CRC than in healthy controls (15.25 vs 72.1 pg/mL; P = .04; Figure 1A). Repeated tests indicated that the average serum Cldn7 level in some patients with CRC (n = 4) was below 0.01 pg/mL or too low to be detected. When the serum Cldn7 levels of these 4 patients were all counted as 0.01 pg/mL and incorporated into the statistical analysis, the difference in serum Cldn7 levels between patients with CRC and healthy controls was more significant (8.92 vs 72.1 pg/mL; P = .02; Figure 1B). We also depicted a receiver operating characteristic (ROC) curve of serum Cldn7 levels of patients with CRC which was detected by the ELISA method (Figure 1C). When the experimental group included 27 patients with CRC, the area under the curve (AUC) was 0.731, and the P value was .04. When 31 patients with CRC were included, the AUC was 0.763, and the P value was .017. The ROC curve indicated that the use of ELISA to detect serum Cldn7 levels in patients with CRC had a good accuracy for the diagnosis of patients with CRC. And when patients whose serum levels of Cldn7 were too low to be detected were included, this method had a better diagnostic effect. Because low Cldn7 levels in the serum indicated a positive result, these data were used in the later analyses of the relationship between serum Cldn7 levels and the disease characteristics.
Comparison of Serum Cldn7 Levels Between Patients With CRC and Healthy Controls.

Abbreviations: Cldn7, claudin-7; CRC, colorectal cancer.
a Patients whose serum levels of Cldn7 were too low to be detected were not included.
b Patients whose serum levels of Cldn7 were too low to be detected were included.
c Statistically significant (P < .05).

Serum claudin-7 (Cldn7) levels in patients with colorectal cancer (CRC) and healthy controls. A, Patients whose serum Cldn7 levels were too low to be detected were not included (P = .04). B, Patients whose serum Cldn7 levels were too low to be detected were included (P = .02). C, The receiver operating characteristic (ROC) curve of serum Cldn7 levels of patients with CRC was detected by enzyme linked immunosorbent assay (ELISA) method.
Correlations Between Serum Cldn7 Levels and the Disease Characteristics
Correlations between serum Cldn7 levels and the disease characteristics are shown in Table 3. Age, sex, tumor location, grade of differentiation, and other disease characteristics were not correlated with serum Cldn7 concentrations.
Comparison Between Serum Cldn7 Levels and the Disease Characteristics.

Abbreviations: AFP, α-fetoprotein; CA, carbohydrate antigen; CEA, carcinoembryonic antigen; p53, p53 gene.
a Patients without relevant information were not included in this statistic.
Clinical Characteristics of the Patients Included in the Immunohistochemistry Experiment
Clinical characteristics of the 75 patients with CRC are shown in Table 4. The median age of the patients with CRC was 63 years. There were 37 patients older than 63 years and 38 patients aged 63 years or younger. The number of males and females was similar (38 vs 37). Tumor diameters were larger than 5 cm in 39 cases and ≤5 cm in 36 cases. According to the WHO histological grade, there were 10 cases of highly differentiated adenocarcinoma (13.3%), 47 cases of moderately differentiated adenocarcinoma (62.7%), and 18 cases of poorly differentiated adenocarcinoma (24%). The number of patients with lymph node metastases was 37, and the number of patients without lymph node metastases was 38. The most frequent metastatic sites were the liver (n = 18) and lung (n = 9). The infiltration depth was also included in this study. Tumor infiltration reached the serous layer or below in 51 patients and reached the serous layer or higher in 24 patients. According to the clinical stages of TNM, there were 40 cases of stage III and higher (53.3%) and 35 cases below stage III (46.7%). The median survival time was 45 months, with times ≥45 months in 33 cases and <45 months in 30 cases.
Clinical Characteristics of the Patients Included in the Immunohistochemistry Experiment.
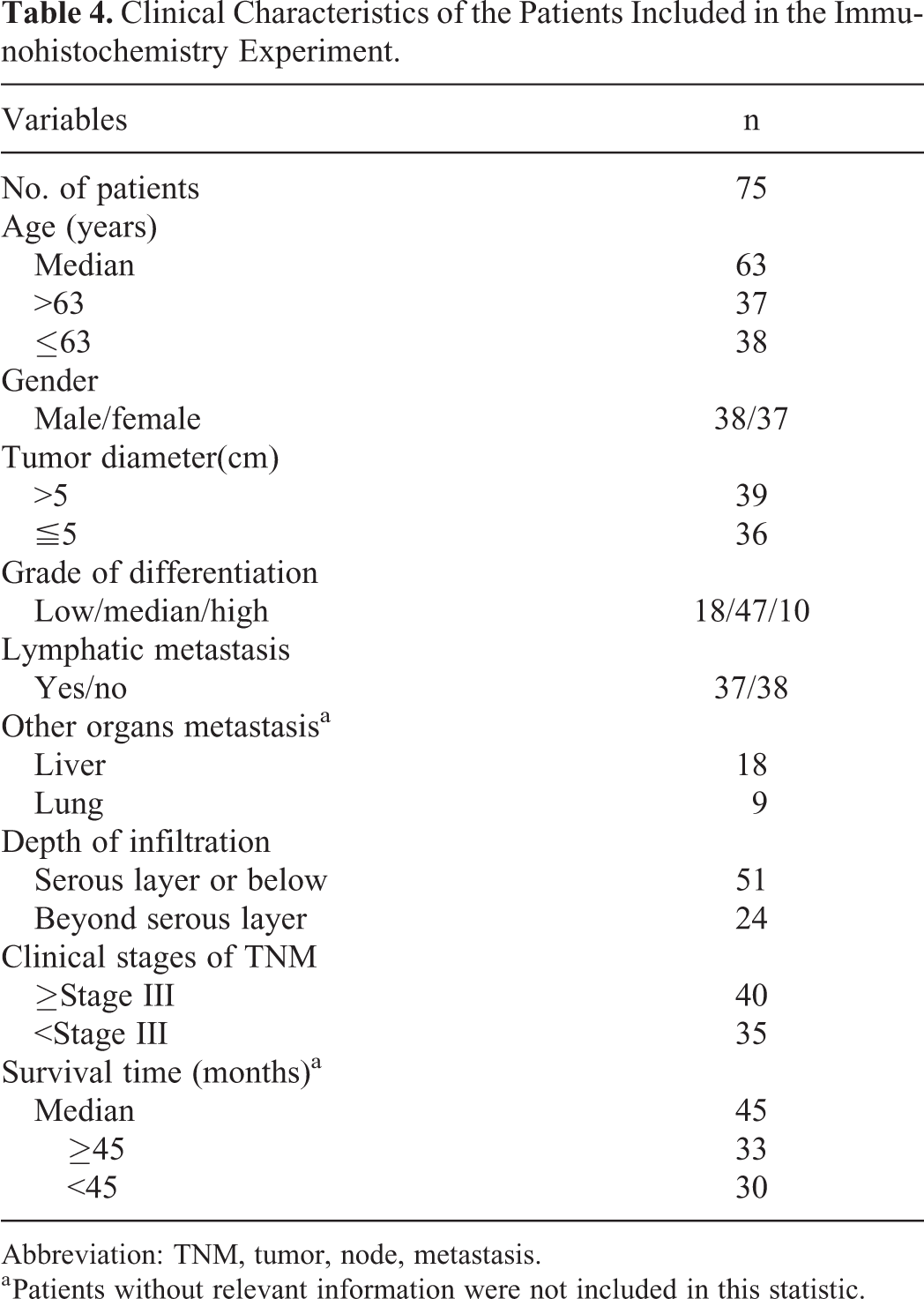
Abbreviation: TNM, tumor, node, metastasis.
a Patients without relevant information were not included in this statistic.
Comparison of Cldn7 Expression Between CRC Tissues and Paracancerous Tissues
The rate of positive Cldn7 expression in paracancerous tissues was 0.96, and the expression was located primarily in the cell membrane. The rate of positive Cldn7 expression was significantly lower in CRC tissues than in paracancerous tissues (0.52 vs 0.96, P =.000; Table 5).
Comparison of Cldn7 Expression Between CRC Tissues and Paracancerous Tissues.

Abbreviations: Cldn7, claudin-7; CRC, colorectal cancer.
a Statistically significant (P < .05).
Correlations Between the Rate of Positive Cldn7 Expression in CRC Tissues and the Disease Characteristics
Correlations between the rate of positive Cldn7 expression in CRC tissues and the disease characteristics are presented in Table 6. The grade of differentiation was related to the rate of positive Cldn7 expression. The rates of positive Cldn7 expression in high, moderate, and low adenocarcinoma differentiation were 0.85, 0.55, and 0.28, respectively; these rates decreased with decreasing tissue differentiation (P = .019; Figure 2). However, Cldn7 expression was not correlated with gender, age, tumor invasion depth, lymph node metastasis, tumor size, TNM stage, or survival time (P > .05).
Comparison Between the Rate of Positive Cldn7 Expression in CRC Tissues and the Disease Characteristics.

Abbreviations: Cldn7, claudin-7; CRC, colorectal cancer.
a Statistically significant (P < .05).
b Patients without relevant information were not included in this statistic.

Immunohistochemical staining shows claudin-7 (Cldn7) expression at different stages of colorectal cancer (CRC) and in adjacent normal tissues. The arrowheads show that Cldn7 expression was strongly positive in paracancerous tissues (A-C), downregulated in well-differentiated tissues (D-F), further downregulated in moderately differentiated tissues (G-I), and significantly downregulated in poorly differentiated adenocarcinoma tissues (J-L). The rates of positive Cldn7 expression in well, moderately, and poorly differentiated carcinomas are presented (P = .019) (M). Magnification: (A, D, G, J) ×20, (B, E, H, K) ×100, (C, F, I, L) ×200.
Comparison of the Rate of Positive Cldn7 Expression Between CRC Tissues and Metastatic Tissues
Claudin-7 was located on the cell membrane of lymph node, liver, and lung metastases, and its expression was weakly positive (Figure 3A-I). The rates of positive Cldn7 expression in CRC tissues and metastatic tissues are presented in Table 7. The rates of positive Cldn7 expression were significantly lower in lymph node metastases, liver metastases, and lung metastases than in primary tumors (P = .000, .034, and .031, respectively; Figure 3J). However, Cldn7 expression levels were not significantly different among metastatic tissues (P = .625).

Immunohistochemical staining for claudin-7 (Cldn7) in lymphatic metastases (A-C), liver metastases (D-F), and lung metastases (G-I). Claudin-7, as indicated by the arrowheads, was located on the cell membrane, and its expression was weakly positive or negative. Rates of positive Cldn7 expression were significantly lower in lymphatic metastases, liver metastases, and lung metastases than in primary colorectal cancer (CRC) tissues (P = .000, .034, and .031, respectively) (J). Magnifications: (A, D, G) ×20, (B, E, H) ×100, (C, F, I) ×200.
Comparison of the Rate of Positive Cldn7 Expression Between CRC Tissues and Metastatic Tissues.
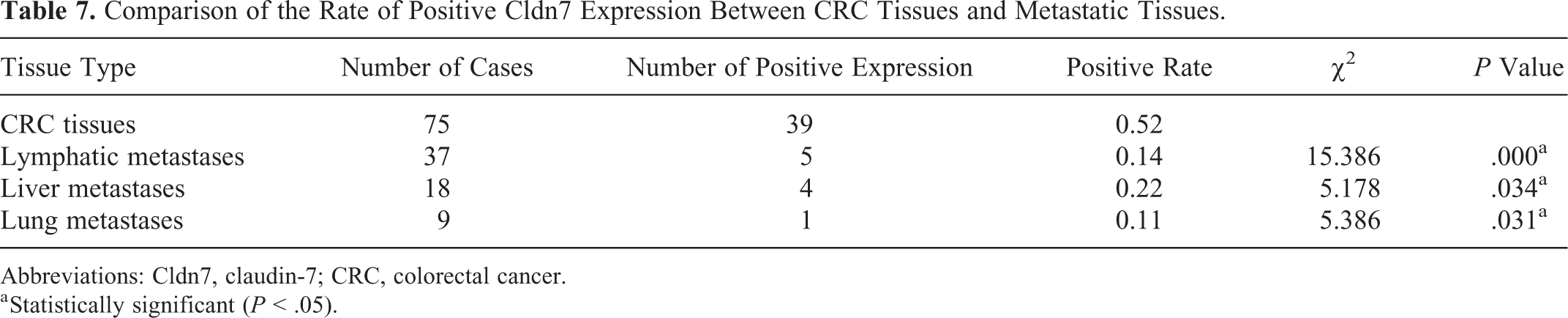
Abbreviations: Cldn7, claudin-7; CRC, colorectal cancer.
a Statistically significant (P < .05).
Claudin-7 Protein Expression in Fresh and Metastatic CRC Tissues
Western blot analyses showed that Cldn7 was highly expressed in adjacent tissues of CRC, and the relative expression was decreased in high-medium differentiated, medium-low differentiated, and liver metastatic CRC tissues (P < .0001). The relative expression levels decreased with the degree of differentiation and were barely detectable in liver metastasis of CRC (Figure 4).
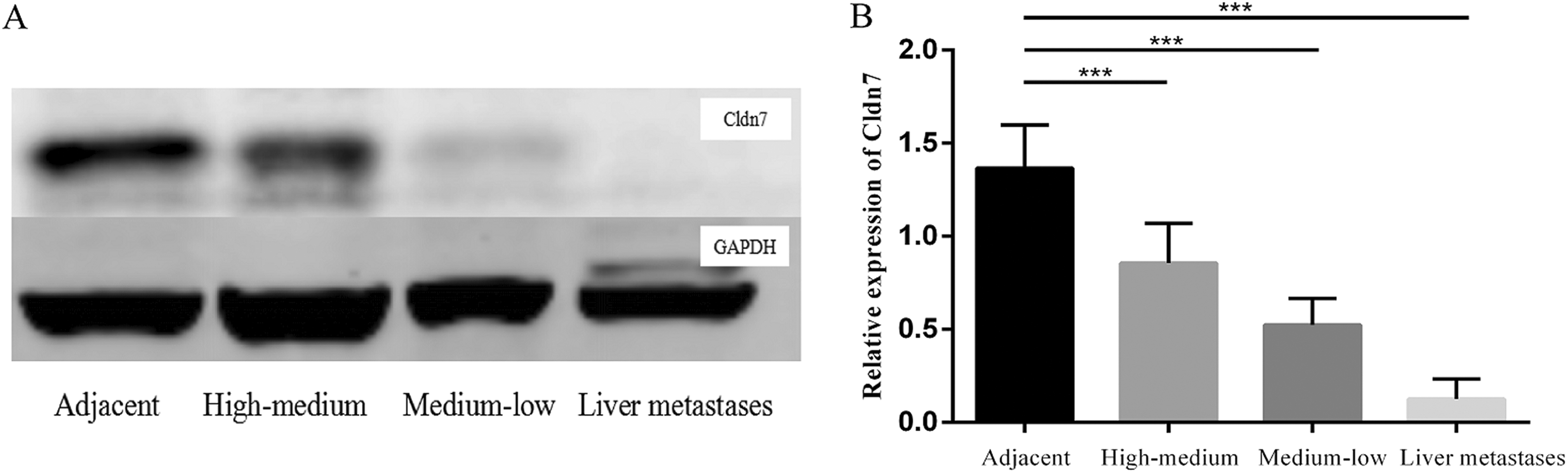
Claudin-7 (Cldn7) expression levels were lower in CRC tissues than in normal tissues; the relative Cldn7 expression levels decreased with decreasing differentiation degrees, and Cldn7 expression was barely detectable in liver metastases (P < .001).
Discussion
The occurrence, invasion, and metastasis of CRC is a complex process involving multiple genes and processes, including oncogene activation, tumor suppressor gene inactivation, mismatch repair gene mutation, and other genetic mutations. 12 Among these, the tumor suppressor genes have received increasing attention because they can be used as therapeutic targets for CRC.
Claudin is the main skeletal protein composing the tight junctions between epithelial cells. In addition to the classic barrier and fence functions of tight junctions, claudin also plays an important role in regulating cell proliferation and differentiation. 13,14 Abnormal claudin protein expression changes the normal structure and function of tight junctions to cause the loss of cell polarity and the diffusion of nutrients and other factors necessary for the survival and growth of tumor cells; these effects play an important role in the metastasis and nutrition supply of tumor cells. 15 Claudin protein expression is different in several types of cancer tissues, and some claudin proteins are downregulated or not expressed in cancer tissues.
Claudin7 is an important member of the claudin family and plays an important role in maintaining tight junction integrity, epithelial cell polarity, and ion permeability between cells. 16 In recent years, increasing attention has been paid to the role of Cldn7 in tumorigenesis, development, invasion, and metastasis. Lioni et al 17 used RNAi to knock out Cldn7 in esophageal squamous cell carcinoma cells. The results showed that E-cadherin expression levels decreased and that cell growth and infiltration increased. These findings suggest that Cldn7 expression is closely related to tumor progression. Lu et al 11 transfected Cldn7 into the NCI-H1299 lung cancer cell line, which does not express Cldn7 protein. Proliferation and invasion were significantly lower in these transfected cancer cells than in the control cells, suggesting that Cldn7 plays an anticancer role in lung cancer cell lines. In addition, Kominsky et al 18 found that Cldn7 expression was significantly lower in breast invasive ductal carcinoma than in normal breast tissue.
Some studies have suggested that Cldn7 expression may be related to the degree of tumor differentiation. Decreases in Cldn7 levels in breast cancer are related to the histological malignancy of carcinoma in situ and invasive ductal carcinoma; the higher the degree of malignancy, the lower the expression of Cldn7. 18 Usami et al 19 reported that Cldn7 expression was negatively correlated with the differentiation degree, invasion depth, and lymph node metastasis in esophageal carcinoma. However, there are also reports of increased Cldn7 expression. Johnson et al 10 found that Cldn7 expression was higher in gastric cancer tissues than in paracancerous tissues. It has been suggested that Cldn7 overexpression may be an early event in gastric carcinogenesis. Claudin-7 expression is apparently different in different types of tumor tissues.
Bornholdt et al 20 found that the Cldn7 messenger RNA (mRNA) level in CRC tissue decreased by 270% compared with that in normal colorectal tissue, and the decreased Cldn7 mRNA levels were also found in early-stage CRC. These data suggest that decreased Cldn7 expression occurs in the early stage of CRC. Nakayama et al 21 found that promoter methylation may lead to Cldn7 silencing in the CRC cell line Colo320; this action may affect the progression of CRC. In addition, the expression of Cldn7 protein in patients with CRC seems to be more important for the recognition and diagnosis of CRC. In a study by Süren et al, 22 Cldn1, Cldn4, and Cldn7 expression levels were detected by immunohistochemistry in 70 patients with CRC. 22 The results demonstrated that Cldn1, Cldn4, and Cldn7 expression levels were related to tumor invasion depth, lymph node status, disease stage, and tumor grade. Oshima et al 23 found that the absence of Cldn7 expression is associated with venous infiltration and liver metastasis in CRC. Previous studies have investigated the role of Cldn proteins on different cancer types using IHC or Western blotting, while Karabulut et al 24 used the ELISA method to detect patient serum for the first time. A series of important findings such as the significant reduction of Cldn1 and Cldn7 expression in patients with CRC and the correlation between high T stage and CEA level and low Cldn1/Cldn7 expression were found. 24 Because ELISA is easy to operate and blood is easy to collect, the expression of Cldn proteins in the serum of patients can be used to determine if the CRC has occurred and to predict the stage of disease and prognosis. Therefore, the application and effect evaluation of the ELISA method will facilitate the transformation of Cldn7 research into clinical applications.
In this study, we integrated traditional IHC and Western blotting methods, as well as rare ELISA methods. Similar to the results of previous studies, our IHC staining results showed that the rate of positive Cldn7 expression was significantly lower in CRC tissues than in paracancerous tissues and Cldn7 expression was positively correlated with CRC differentiation. In addition, we found the rates of positive Cldn7 expression were decreased in lymphatic metastases, liver metastasis, and lung metastasis, but there were no significant differences in Cldn7 expression among metastatic tissues. We also used Western blotting to measure Cldn7 protein levels in CRC tissues with different differentiation degrees and liver metastases. The results were consistent with those obtained by immunohistochemistry. Our ELISA results confirmed that serum Cldn7 levels were significantly lower in patients with CRC than in the control group. We also found that serum Cldn7 levels in some patients with CRC (n = 4) were too low to be detected, but the low expression of Cldn7 in these patients also had research and clinical significance. However, we did not find a significant correlation between serum Cldn7 levels in patients with CRC and disease characteristics such as tissue differentiation and prognosis. This result may occur because the expression of Cldn7 in serum is different from that in tissues, and the ELISA technique is relatively limited compared with the IHC technique. Therefore, Cldn7 may be more suitable for the preliminary determination of disease stage and distant metastasis by IHC method, that is, Cldn7 may be a factor to determine the severity of the disease and a potential therapeutic target and to rely on ELISA to detect serum Cldn7 for disease prevention and the forecast is still to be verified.
Conclusion
In this study, serum and tissue samples were collected from many clinical patients with CRC; Cldn7 expression levels were significantly lower in the CRC samples according to ELISA, immunohistochemistry, and Western blot results. Decreased Cldn7 expression levels were correlated with CRC differentiation; hence, we speculated that Cldn7 could inhibit the occurrence of CRC. Claudin-7 expression was significantly decreased or not detectable in distant metastatic tissues, such as lymphatic metastases, liver metastasis, and lung metastasis, suggesting that Cldn7 downregulation may be related to the invasion and metastasis of CRC. Because the ELISA method is convenient and patient blood samples can be routinely obtained, the ELISA detection of Cldn7 could be developed into a clinical diagnostic method for CRC. Blood Cldn7 levels may be a new marker for diagnosing CRC.
In conclusion, Cldn7 is a tumor suppressor gene for CRC. Therefore, it is expected to be an early diagnostic marker and a new therapeutic target for CRC.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant nos. 81372585 and 81772557) and Beijing Health System High Level Training Plan of Health Technical Personnel (2014-3-048).