
Abstract
Irreversible electroporation and electrochemotherapy are 2 innovative electroporation-based minimally invasive therapies for the treatment of cancer. Combining nonthermal effects of irreversible electroporation with local application of chemotherapy, electrochemotherapy is an established treatment modality for skin malignancies. Since the application of electrochemotherapy in solid organs is a promising approach, this article describes a novel electrode configuration and field generating method. For the treatment of hepatic malignancies, the shape of the electric field should resemble a spherical 3-dimensional geometry around the target tissue inside the liver. To adapt the actual shape of the field, the probe is designed in computer-aided design with a live link to a computer simulation software: Changes in design can be revalued quickly, regarding different quality criteria for field strength inside and outside the tumor. To rate these criteria, a set of formulas with weighting coefficients has been included. As a result of this design process, a needle-shaped prototype applicator has been built, designed for an intracorporal electroporation-based treatment. It can be used as percutaneous, image-guided, minimally invasive treatment option for malignant liver tumors. The shaft of the probe is used as central electrode and fitted with additional 4 expandable electrodes. These satellite electrodes are hollow, thus serving as injectors for chemotherapeutic agents within the area of the electric field. This configuration can be used for electrochemotherapy as well as irreversible electroporation. By placing 5 electrodes with just one needle, the procedure duration as well as the radiation dose can be reduced tremendously. Additionally, the probe offers an option to adapt the field geometry to the tumor geometry by connecting the 5 electrodes to 5 individually chosen electric potentials: By fine-tuning the ablation zone via the potentials instead of adjusting the location of the electrode(s), the procedure duration as well as the radiation dose will decrease further.
Keywords
Introduction
With about 8.2 million cancer-related deaths per year, 1 malignant tumors belong to the most relevant causes of death. In numerous tumor diseases, the occurrence of metastases is the major limiting factor of patients’ life expectancy. While surgical resection of the primary tumor and its metastases is the treatment method of choice in case of demonstrating resectability, this option is only suitable for about 25% of patients in our department because of tumor spread and/or comorbidities. For these patients, various alternatives to systemic chemotherapy, for example, transarterial chemotherapies and ablation-based thermal (such as radiofrequency ablation [RFA] and microwave ablation [MWA]) and nonthermal (such as irreversible electroporation [IRE]) tumor treatments, have gained clinical acceptance.
The clinical treatment modality IRE is named after the biological effect (IRE) and is a quite new, nonthermal ablation procedure employing multiple short-termed electrical pulses that irreversibly destroy cells in the application area. 2 -5 This technique has certain advantages compared to thermal ablation techniques such as RFA or MWA, notably the preservation of vulnerable structures such as blood vessels, bile ducts, and bowel. Electroporation (EP)-based methods can induce apoptosis instead of necrotic cell death, which can result in a superior immune effect; additionally, IRE may invoke a systemic response beyond the targeted ablation region. 6 Furthermore, IRE is not susceptible to the heat sink effect of major blood vessels, which could impair the efficacy of thermal ablation methods. Accordingly, for tumors close to major blood vessels and other heat-sensitive structures IRE seems to be the ideal ablation technique. 2,3,7 -9 With preoperative computer simulations of the electric field shape and density, IRE is also favorable since it can be planned precisely prior to the intervention. However, there is a growing body of evidence that IRE is more prone to induce needle tract seeding compared to thermal ablation methods. 10,11
Mahmood and Gehl designed an expandable applicator for electrochemotherapy (ECT) for brain tumors 12 and then Agerholm-Larsen et al used it for the treatment of brain tumors in mice. 13 Neal et al used bipolar needles for the treatment of breast cancer in mice, 14 but for liver tumors, the resulting ablation volume is too small and the ellipsoid geometry does not fit the desired spherical shape. Currently, the NanoKnife System by AngioDynamics (Latham, New York) is the only approved device for IRE in Europe. Although several applicator designs have been developed for use with the NanoKnife system (eg, also bipolar needle electrodes 15 ), this device together with straight monopolar needles is the only clinically licensed IRE system for liver tumor ablation. Accordingly, it is the reference design for this project.
Another nonthermal tumor treatment procedure is called ECT and is an established, highly effective method for the local treatment of malignant skin tumors. This technique also is based on the application of electric pulses, but in this case to temporarily increase diffusion processes through cell membranes (reversible electroporation). This increased cell membrane permeability facilitates the intracellular uptake of the chemotherapeutic agent. By means of an applied electric field, a much higher rate is channeled inside the tumor cells. 16 -20 However, ECT is also being a promising treatment method for deep-seated tumors of organs such as the liver or pancreas, offering the advantages of IRE with an increased antitumoral effect due to local chemotherapy administration. 21 -24
In both IRE and ECT, the success of the procedure highly depends on an appropriate application of the electric field in order to induce membrane permeability in the predefined area only. 25,26 Parameters that affect the applied electric field are: geometry and positions of electrodes, the tissue-specific electrical properties, and electric pulse parameters, that is, pulse length, amplitude (see Figure 1), quantity, frequency, slopes, shape. 18,27,29

The aim of this research project is the development of a minimally invasive, intracorporal application for IRE and ECT: From an engineering’s point of view, curved electrodes with different potentials leads to much more opportunities to adapt the field geometry to a specific patient’s tumor geometry, than straight ones with 2 potentials. Additionally, the duration of an IRE procedure is dominated by the time-consuming placement of multiple applicators, so an EP system consisting of a single needle bears the potential of significantly reducing intervention time.
As there are different opinions for the definition of IRE and ECT (IRE also contains regions of reversibly electroporated tissue, which could incorporate adjuvant chemotherapy for a combined therapy versus ECT also contains regions of irreversible electroporated tissue; therefore, this proposed setting is also included in the definition of ECT versus IRE with ECT combinatorial treatment), the following definition is used to simplify the description: When the applicator is connected to a pulse generator only, the treatment is referred to as “IRE.” If the applicator is used for applying both, pulses and chemotherapeutic drugs, it is referred to as “ECT.”
Materials and Methods
We designed a needle-shaped multipolar probe with telescopic electrodes for percutaneous image-guided IRE as well as ECT in solid organs. The applicator was designed in a computer-aided design environment (SolidWorks 2014, Massachusetts) with a live link to a finite element method (FEM) simulation software (COMSOL Multiphysics 5; COMSOL AB, Stockholm, Sweden). The alternating current/direct current (AC/DC) module was used to build up the model, the calculation was performed with a “physics-controlled mesh” with element size “extra fine.” No other than the default AC/DC equations and no additional simplifications were used. Three-dimensional design of the electric field is necessary because we focus on malignant liver tumors, whereas, for example, malignant melanoma is surface-bound and thus can be approximated with a rectangular 2-dimensional field. 30 ) We analyzed different geometries in reference to the geometry of the generated electrical field and optimized the best one in different parameters (ie, electrode radius and length, distance to main electrode, length of insulating layer).
The thresholds for IRE and reversible EP depend on quantity, frequency, and pulse width as well as on the tissue type. For the ECT treatment of malignant skin lesions, a field strength of about E = 1.3 kV/cm (with 8 pulses, 100 µs, about 1-5 Hz) has been established as a working threshold. 31 In liver tissue of rats, reversible EP could archived with approximately E rev = 360 V/cm, IRE with approximately E irrev = 640 V/cm (8 pulses, 100 µs, 1 Hz). 32 For the ECT of brain tumors in mice, Agerholm-Larsen used E > 280 V/cm (8-32 pulses, 100 µs, 1 Hz). 13 During an IRE ablation with the NanoKnife, the target tissue is typically exposed with E IRE_STD = 1.5 kV/cm, up to E IRE_2 = 1.7 kV/cm (with 70 pulses, 100 µs, about 1 Hz in sync of the heart rate; values are taken from treatments in our department and the NanoKnife Guide. 28 ) With these values, the magnitude for ECT and IRE can be assumed, but the exact thresholds have to be determined experimentally.
For a spherical, simplified setup (where Q is the field generating charge), the electrical field is defined by
In contrary to plate electrodes, which are often used for ECT treatments of skin tumors, in a spherical setup E decreases with r 3 in the distance r from the center of Q. This causes the tumor to be electroporated irreversibly at the inside and reversibly at an outer spherical shell. Note that through different electrical parameters for tumor and healthy (surrounding) tissue, the electric field is discrete at these boundary layers.
Besides geometry, the electrical field depends on electrical parameters: The relative permittivity ∊ r and the electrical conductivity σ for healthy tissue generated in ex vivo measurements is referenced, 33,34 most data based on the study by Gabriel et al. 35 Recent works provide variations up to 25% for ∊ r for normal liver tissue in vivo versus ex vivo. 36 To our knowledge, for electric parameters of tumorous liver tissue, there are only few publications with reference values available, 36 -40 which also provide data from ex vivo measurements only. Based on this reference data, we appraised the difference between tumorous and healthy liver tissue to use it as input parameters for our simulations, knowing that these values are still underexplored. Since the conductivity increases with the time of the EP process, the tissue conductivity has to be included as a time-dependent function 41 (COMSOL: step function, 42 location 50 000 [V/m], from 0.1 to 0.3 [S/m]; this function has also been used for healthy liver tissue at the Electroporation-Based Technologies and Treatments–International Scientific Workshop and Postgraduate Course. 43 )
With the results of the simulation process (sectional plane of electric field distribution in a tumor between liver tissue is shown in Figure 2A and B), a complete new probe for percutaneous application has been designed and built up as a fully functional prototype (see Figure 3): The needle-shaped applicator has a shaft diameter of 3.2 mm. The top of the shaft is the central electrode (length: 9 mm), the remaining length of the shaft is insulated with Teflon. It contains 4 expandable satellite electrodes with a diameter of 0.6 mm each, which can be pushed out from their rectilinear position into the surrounding tissue. They deploy retractable in a predefined radius of 35 mm and up to 70 mm in length. In this field-generating arcuate position, they can span an electrical field with almost spherical borders (see Figure 2B). For the insulated parts, a Teflon-coating is used also. In their semicircular configuration, these hollow satellite electrodes were used for the generation of a defined electric field as well as the interstitial injection of the chemotherapeutic agent inside the outer spherical shell of the electric field. All 5 electrodes are wired individually.


Prototype for intracorporal application of IRE or ECT to malignant liver tumors, used for in vivo trials (dimensions, see Figure 2A; an earlier version of the prototype, which had nearly the doubled size, was shown in the study by Ritter et al 44 ). Complete view with drug delivery and electrical supplies. In the upper probe, the satellite electrodes are inside the shaft (for punctuation and placement); in the lower probe, the satellite electrodes are expanded. ECT indicates electrochemotherapy; IRE, irreversible electroporation.
All geometry parameters can be adapted to special tumor geometries. For just the shape of the geometry, the pulse protocol is subsidiary. For the thresholds referring to IRE and ECT, we assumed a pulse protocol taken from the NanoKnife for typical IRE treatment of the liver (70 pulses, 100 µs, about 1 Hz), as this prototype is also designed for IRE.
Results
With the results of the electric field simulation processes and our experience in electrode design, we built a new fully functional needle-shaped prototype with a shaft diameter of 3.2 mm (see Figure 3). The applicator contains 4 expandable hollow electrodes in a semicircular configuration used for both interstitial injection of the chemotherapeutic agent and generation of the electric field. Results of the first ex and in vivo tests show that the purposed treatment can be archived with this design: First we did ex vivo trials in explanted beef livers, no macroscopic burnings could be observed (done with the BTX-Harvard Apparatus ECM 830 Electroporation Generator with 70 pulses, 100 µs, 1 Hz, 1.5 kV; electrode fully extruded). During an in vivo study, we compared ECT and IRE treatments made with this version of the prototype inside swine liver. 45 The ablation zones do match the simulated field geometry and the volume is nearly 2 times bigger with ECT. The complete in vivo study is work in progress and will be published soon.
During an IRE intervention, its common use is to correct the placement of all used electrodes several times. Instead of changing the position of this electrodes in the tissue, it is also possible that an electroporator will correct small deviations in the intended location of each electrode by adapting the potential of all electrodes time-dependent individually. A simplified example with just 2 potentials is shown in Figure 2B. Changes in design can be revalued quickly within FEM simulation, regarding different quality criteria for field strength inside and outside the tumor. To rate the direct effect, a Q factor model with weighting coefficients has been included to optimize the geometric and electric parameters dispassionately:
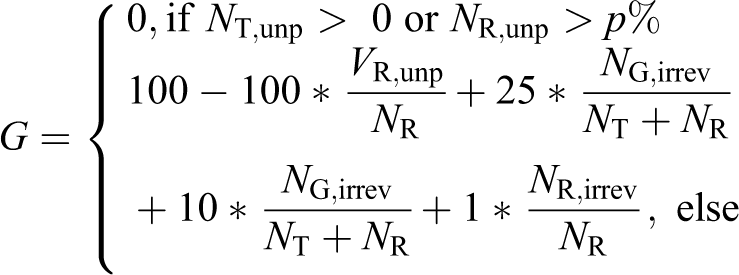
The variables used are described in Table 1. This quality factor is a sum of weighted coefficients (marked with *), which describe events that should not occur. These events—respectively these coefficients—decrease the quality factor down from G max = 100. Table 1 shows relevant different cases for calculating G, subdivided in the different volume segments, with preselected weighting coefficients. With the calculated value of G, effects of different geometry parameters, different wiring of the electrode, and different voltages can be determined and compared to each other objectively. The value of G therefore allows to optimize the electrode to different tumor geometries and provides an estimation on how precisely the (later) commercial production line must maintain the geometric parameters. In clinical applications, this will enable the physician to adapt the desired ablation zone to the patient individual 3D tumor geometry to ensure complete ablation of the target tumor. By this preinterventional adaption of the electric field to the patient-specific tumor geometry, the healthy tissue can be spared as far as the physician thinks it is medically sensible. Also, when using ECT for the outer area, this more tumor-specific method can save healthy tissue.
Volume Segments for Computing the Quality Factor and Preselected Associated Weighting Coefficients (WC).

Discussion
Based on the results of the FEM simulation, we developed a fully functional probe for intracorporal use, which can be used for both IRE and ECT as percutaneous, image-guided, minimally invasive tumor ablation treatment. 46 With this prototype, it is possible to place 5 independent electrodes doing a single stitch only, which also has main advantages for IRE (time of the intervention, patient’s radiation load, accuracy, risk of needle tract seeding).
Neal et al performed similar numeric simulation with regular IRE straight needle electrodes 47 : They compared the predicted volume of the ablation zone in canine brain when treating with ECT instead of IRE and confirm our result of a significant increase (ECT: 2.1-3.2 times larger compared to IRE. 47 )
The promising results for ECT legitimate the redesign of a multipole EP system to vary tumor coverage per software, even after the electrodes were positioned. The prototype already covers this concept: All 5 electrodes are wired individually and all 5 are simultaneously active during EP pulsing. The NanoKnife ablation system makes use of up to 6 connected electrodes, alternating two of which are used for pulse delivery simultaneously. 28 With the system presented here, up to 5 electrodes may be used simultaneously at different potential levels, which overcomes 2-electrode field design limitations and allows more complex electric field shapes.
Simplified electrostatic simulations indicate the influence of the electrical parameters we used 33 -39 : Inside tumor tissue, the electric field strength decreases about 5% to 20%. Thus, for a simulation model applicable to clinical practice, more basic research in the topic of electric tissue parameters is essential and current research by other groups. 48 However, these values are independent from the geometrical model which is shown here. If simulations are used for preinterventional patient-specific planning, it should also be considered how to measure the patient-specific electrical tissue parameters, which increase the simulation accuracy. Nevertheless, the accuracy is limited through the physicians and the computed tomography (CT): Image-guided interventions are done in the CT, and currently, the placing accuracy for a treatment like this is not better than ±1 mm. An improved CT combined with robotic needle placement might increase the accuracy, but after all the patient’s movements and breathing are the limiting factors.
Independently, Županiĉ et al did optimizations for EP similar to our model 49 : Both studies made use of similar assumptions and similar simplifications, independently. Because of the crossover from tumorous to healthy tissue inside this area, consequently the crossover of the electrical parameters, our model additionally includes a separate boundary area. Furthermore, because of the combined consideration of IRE and ECT, an explicit discrimination between irreversible and reversible EP was made, especially in this boundary area. Furthermore, the effect of reversible EP is not limited to ECT, it can also be used for, for example, calcium EP. 50
Next steps are to specify the used values for the electrical parameters and to prove the simulation results in vivo. Currently, we work on finalizing an in vivo study made with this electrode (Figure 3) in swine liver 45 : It will prove that an IRE treatment can be done successfully with this prototype and will also show the advantages when using the device for ECT with the same pulse protocol.
Long-term aims for bringing a device like this into medical usage, more simulations studies are needed: The current flow and the thermal distributions for this design have to be evaluated, both with focus on the edges of the electrical active parts of the probe. A numeric simulation together with pathological images has to prove that the tissue is not ablated through thermal issues. The other way around could also have a therapeutic impact: As RFA does not have that much issues with tract seedings as current IRE has, 11 it might be a new objective to ablate the tissue nearby the probe specifically with thermal heating. Also, the comparison of reversibly/irreversible electroporated tissue volumes versus various pulsed electromagnetic field parameters can help making a treatment like this more precise.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded through the Deutsche Forschungsgemeinschaft e.V. MA 4030/3 -1, BR 3912/1 -1.