
Abstract
Oral squamous cell carcinoma is a common malignancy in the head and neck region. Brachytherapy after radical surgery has achieved much progress as a cancer adjuvant treatment. This study focused on the pathologic characteristics of the patients with oral squamous cell carcinoma who underwent seed implantation after radical surgery, and the relationship of these characteristics with prognosis. Thus, 76 patients with oral squamous cell carcinoma, who were treated with surgery and subsequently with iodine 125 (125I) radioactive seed implantation, were recruited in this study. We summarized the demographic information, tumor size, location, clinical stage, prognosis, and pathologic characteristics, and discussed the correlations between prognosis and histologic features of oral squamous cell carcinoma after seed implantation. The data showed that the median age was 64 years old, the male/female ratio was 47/29, and the frequent location of the carcinoma was the tongue (35.5%). The median follow-up time was 126 months, and of the patients, 52 (68.4%) exhibited recurrent tumors. The 5-year survival rate was 81.5%, and the local control rate in 6 months was 95.3%. Microscopically, 25 cases demonstrated lymph node metastasis, there was obvious necrosis in 13 cases, and 55 cases exhibited confirmed adjacent tissue invasion including muscle, gland, vessel, nerve, and bone infiltration. Among those, vascular infiltration (13 cases) was significantly correlated with tumor recurrence (P < .05). This study suggests that detailed pathologic diagnosis and microscopic description, especially of vascular infiltration, was valuable in the prognosis prediction of brachytherapy.
Introduction
Oral cancer is a common cancer worldwide, and 90% of oral cancers are squamous cell carcinoma. Even with the numerous basic and clinical research and reports that have emerged, the overall 5-year survival rate for patients with oral squamous cell carcinoma (OSCC) is still poor. It is necessary to look for more effective treatments for OSCC.
The main therapeutic choices of OSCC are surgery, radiotherapy, and/or chemotherapy. Several published studies have suggested the feasibility of radiotherapy with curative intent for every type of head and neck cancer. Recently, computed tomography (CT)-guided 125I brachytherapy after radical surgery has received much attention in the field of cancer adjuvant treatment. Brachytherapy is a treatment that escalates the dose of radiation to the primary tumor while minimizing the dose to critical organs at risk. Computed tomography-guided 125I brachytherapy uses the 125I radioisotope, and the seed implantation is guided by CT. The major advantage of brachytherapy is its accurate delivery of a high dose that is localized to the target areas, with a relatively low dose in the adjacent tissues. It has been used to treat early invasive breast cancer, early stage endometrial cancer, vaginal cancer, advanced cervical cancer, prostate cancer, anal canal cancer, brain tumors, and lung cancer. Brachytheraphy is also effective in head and neck carcinoma. Promising prognoses have been obtained when these tumors have undergone brachytherapy. Brachytherapy has been shown to have excellent local control rates and acceptable side effects. It has been demonstrated as a supplementary method for oral cancer, it could be used alone for oral cancer therapy as well.
For the surgeon or radiologist, the pathologic term or diagnosis is more important than the detailed microscopic description when they choose the treatment modality or predict the prognosis. However, several clinicopathologic parameters, including metastasis, invasion, and necrosis, are all related with tumor recurrence, disease progression, and survival of oral cancer. Unfortunately, there are no reported clinicopathologic studies related to OSCC of patients who underwent brachytherapy to highlight the significance of detailed microscopic descriptions of OSCC after brachytherapy until now. At the same time, it has been recently found that patients with the same cancer may exhibit different clinical progress and prognosis even after the same treatment due to tumor heterogeneity. Herein, this study aims to (1) analyze the relationship between clinicopathologic parameters and recurrence, tumor progression, and survival after brachytherapy; (2) valuate the microscopic descriptions in the prognosis prediction; and (3) provide the detailed morphological implications needed for personalized or accurate treatment.
Materials and Methods
Patients
We retrospectively analyzed 76 patients (median age, 64 years; range, 37 to 90 years) who were treated with 125I seed implantation guided by ultrasound or CT in Peking University School and Hospital of Stomatology from 2004 to 2013. The criteria for eligibility were as follows: (1) squamous cell carcinoma in the oral cavity confirmed by 2 professional pathologists; (2) tumor resection surgery performed before seed implantation; (3) both primary and recurrent tumors confirmed by pathologic diagnosis; and (4) the follow-up time is equal to or more than 5 years. The investigated parameters included the gender and age distributions, anatomic location, clinical stage, pathological grade, histologic characteristics, treatment before implantation, and postoperative outcomes.
New Stage Classification
The American Joint Committee on Cancer (AJCC) published the 8th AJCC Cancer Staging Handbook in 2016, and the revision will be valid from January 01, 2018. We used this new classification to redefine the clinical stages of the above patients. In the 8th AJCC Cancer Staging Handbook, the T stage of the tumor is defined by its size, the depth of invasion (DOI), and the involvement of vital structures. Lymph node metastasis conditions determine the N stage, and distant metastasis defines the M stage. In particular, the new T stage emphasizes the (DOI) and extra-nodal extension (ENE). The classification is as follows: T1: tumor size ≤ 2 cm and DOI ≤ 5 mm; T2: tumor size ≤ 2 cm and 5 mm ≤ DOI < 10 mm or 2 cm ≤ tumor size < 4 cm and DOI < 10 mm; T3: tumor size > 4 cm or DOI > 10 mm; T4: the involvement of vital structures. Any lymph node metastasis with evident ENE(+) is defined as the N3b.
Surgical Treatment and Seed Implantation
Each patient underwent primary surgery before 125I radioactive seed implantation. The aim of the primary surgery was to obtain the maximal tumor excision with tumor-negative margins, which was judged by frozen section examination. In addition, 10 patients underwent traditional radiotherapy after surgery. Radioactive seed implantation was performed by a seed implanting brachytherapy system (Beijing Astro Science and Technology Development Limited Company, China). The seed activity was 0.7 mCi with a half-life of 59.6 days. The prescribed dose was 60 to 160 Gy. The space between seeds was maintained at approximately 1.0 cm (center-to-center), and the seeds were implanted at a depth of 1 cm.
Follow-Up
We obtained the follow-up information through clinical interviews, patients’ medical records, or telephone interviews. Overall survival rate was calculated from the date of implantation to the last recorded reexamination date or death. Local control rate (recurrence-free survival rate) was calculated from the date of implantation to the time of recurrence or death.
Pathology
An immediate pathological examination of specimens collected intraoperatively was conducted for testing surgical margins or lymph node metastasis. In addition, the surgical specimens were fixed, processed, embedded, sectioned, and stained in hematoxylin and eosin after surgery. Two professional pathologists diagnosed these cases.
The histologic grade of the tumor was classified as follows: Gx (grade of differentiation cannot be assessed), G1 (well differentiated), G2 (moderately differentiated), G3 (poorly differentiated), and G4 (undifferentiated). This grade was based on the comprehensive evaluation of the following histologic features: mitoses, nuclear pleomorphism, and the amount of keratinization.
Invasion included vascular infiltration, perineural invasion, and muscle/gland/bone invasion. Necrosis and lymph node metastasis were observed, consisting of intranodal extension and extranodal extension. Other morphologic signs such as clear cytoplasm, basaloid-squamous carcinoma, spindle cell carcinoma, and epithelial–mesenchymal transition (EMT) were also viewed.
Statistical Analysis
The SPSS 17.0 software was used for statistical analyses . Survival and disease-free survival rates were calculated using the Kaplan-Meier functions. Chi-squared test was performed to analyze the relationship between clinical or histologic characteristics and recurrence. The level of statistical significance was considered at P < .05.
Results
Clinical Data
We reviewed a total of 77 patients aged from 37 to 90 years (median age was 64 years old) who underwent 125I radioactive seed implantation after primary tumor resection. The median follow-up duration was 126 months (from 2 to 167 months). Among those, gender distribution was: male 47 (61.8%) persons, female 29 (38.2%) persons. As for the primary tumor location, 35.5% cases occurred in the tongue, 25% in the gingiva, 10.5% in the bucca, 10.5% in the floor of the mouth, and 18.5% in other regions. Before brachytherapy, 42.1% of masses (32 cases) were less than 2 cm and 57.9% (44 cases) were greater than 2 cm. The clinical stage distributions were stage I, 27 cases (35.5%); stage II, 24 cases (31.6%), and stage III, 25 cases (32.9%).
There were 52 patients with recurrent tumors (68.4%). Among those, the clinical stage was upgraded in 9 (17.3%) cases, 21 (40.4%) cases were downgraded, while 22 (42.3%) cases remained at the same stage. Thus, 82.7% (40.4% + 42.3%) of recurrent cases had downgraded or were at the original clinical stage (Table 1).
Clinical Data for the 76 Cases.

In our sets, 12 patients were dead. The median overall survival time was 18 months (from 2 to 146 months). The survival rate in 24 months was 88.3%, and the 5-year survival rate was 81.5%. The median local control time was 8.5 months (from 1 to 123 months) and the local control rate in 6 months was 95.3%.
The survival rate between tumor size < 2 cm and ≥ 2 cm was different, and the larger tumor size suggested poorer survival rate (data not shown). Patients with a high clinical TNM stage exhibited an inferior survival rate (data not shown). However, the tumor size, primary location, and clinical stage did not statistically correlate with recurrence.
Pathologic Features
All tumors were G1 (well-differentiated) or G2 (moderately differentiated) squamous cell carcinomas before brachytherapy. Keratin pearls and individual cell keratinization were evident in the G1 tumors. Although we could find keratin pearls and individual cell keratinization in the G2 tumors as well, they were less evident than those in the G1 lesions. The numbers of cell mitoses and nuclear pleomorphisms were more frequent in G2 tumors than those in G1 cases. In the recurrent cases, the pathologic grade changes were: 4 cases (10.8%) upgrade, 2 cases (5.4%) downgrade, and 31 (83.8%) cases remained at the same stage (Table 2).
Pathologic Features of the 76 Cases.

a Only 37 cases had pathologic diagnoses both before and after brachytherapy.
Microscopically, 55 (72.4%) cases exhibited invasion to adjacent tissue. Invasion suggested a poorer survival rate than noninvasion, but had no statistical significance (data not shown). Muscle invasion appeared in 42 cases (55.3%), vascular invasion in 13 cases (17.1%), nerve invasion in 20 cases (26.3%; Figure 1), and bone invasion in 6 cases (7.9%). Noticeably, vascular infiltration was significantly related with recurrence (P = .025, χ2 = 5.046; χ2 test). In addition, there was necrosis in 13 (17.1%) cases (Figure 2).

The squamous cell carcinoma nests circled the nerve and vessels. Hematoxylin and eosin staining; original magnification was 4× and 20×.
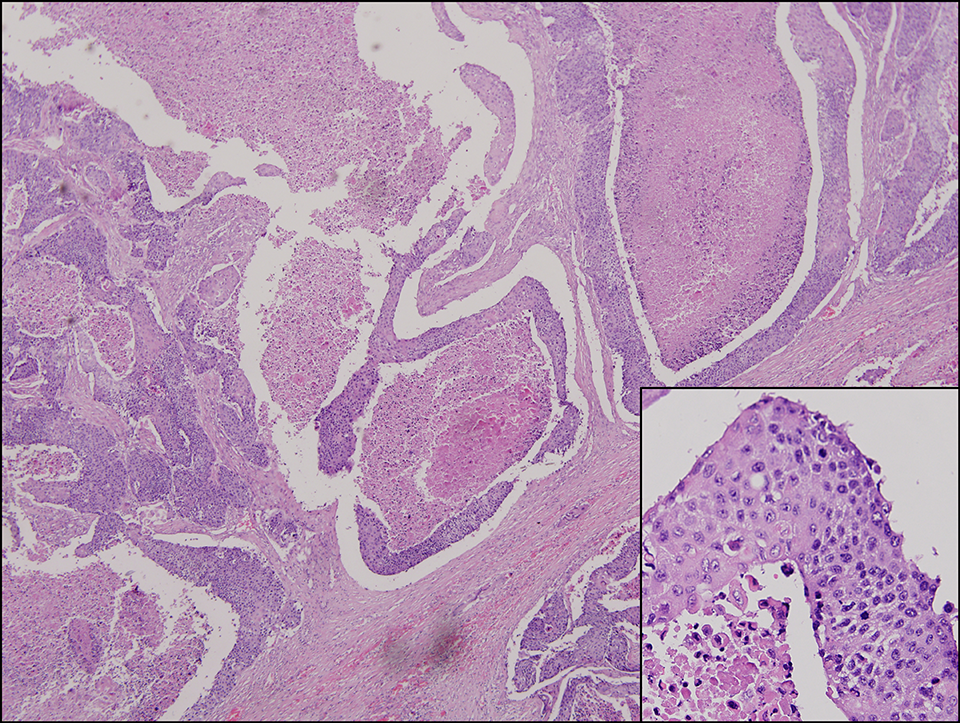
The tumor cells were basaloid and uniform. The central part demonstrated necrosis and formed a pseudoglandular cavity. High karyoplasmic ratio and pathological mitosis were frequent. Hematoxylin and eosin staining; original magnification was 4× and 20×.
There were 25 patients with lymph node metastasis. Among them, extranodal extension appeared in 16 cases, while intranodal extension was observed in 11 cases. Two cases had both extranodal and intranodal extension (Figure 3). Some other morphologic signs such as clear cytoplasm, basaloid-squamous carcinoma, spindle cell carcinoma, and EMT conditions were also observed in recurrent tumors under the microscope.
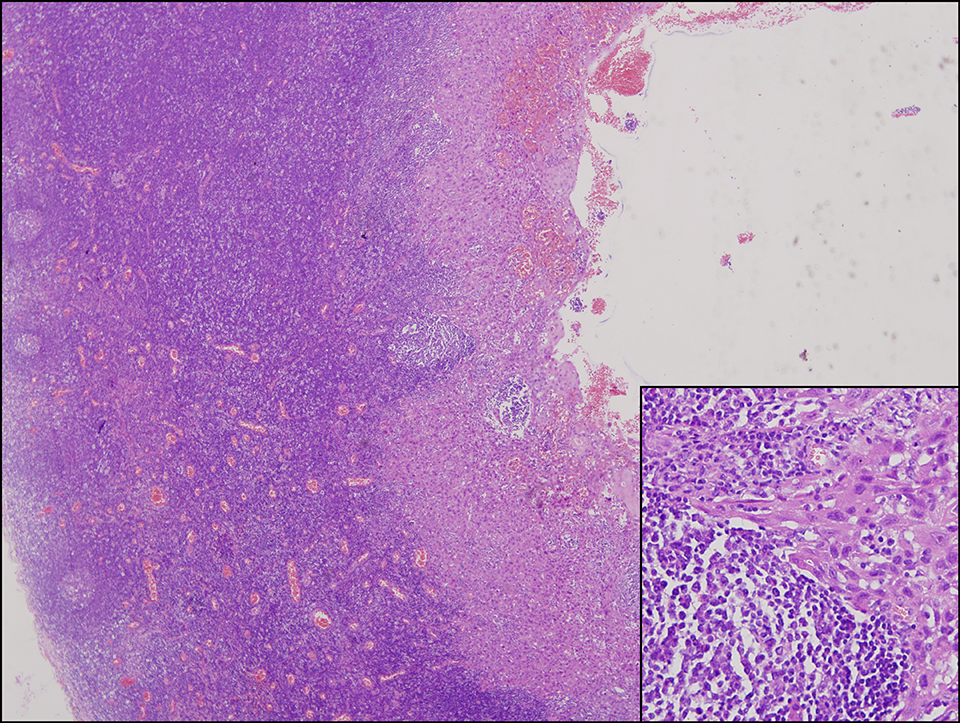
Typical squamous cell carcinoma metastasis into the lymph node; original magnification was 4× and 20×.
The primary tumor of case No. 45 was characterized by clear cytoplasm, and it recurred 16 months after implantation. The recurrent tumors of cases No. 5 and No. 32 were also characterized by clear cytoplasm.
The primary tumors of cases No. 2 and No. 67 were basaloid-squamous carcinoma, and recurred 26 months and 17 months, respectively, after implantation. The patient from case No. 34, who had a basaloid-squamous carcinoma together with vascular invasion, died. In addition, the recurrent tumor of case No. 38 was also characterized by basaloid-squamous carcinoma.
Case No. 55 was characterized by spindle cell carcinoma before implantation. Its recurrent mass demonstrated evident EMT, which suggested the development of metastatic disease after implantation.
Discussion
We summarized the pathologic characteristics and clinical outcomes of 76 cases after radical surgery and seed implantation, and found that the vascular infiltration was significantly correlated with tumor recurrence. These data suggested that detailed pathologic diagnosis and microscopic description should be valuated in the choice of therapeutic strategy and prognosis prediction.
In this study, the median overall survival time was 18 months after surgery and brachytherapy. The 24-month survival rate was 88.3%, and the 5-year survival rate was 81.5%. The median local control time was 8.5 months, and the local control rate in 6 months was 95.3%. An Iranian study by Ali Kazemian et al researching brachytherapy in oral cavity cancer also obtained a 5-year survival rate of 80%. In our study, the survival rate between tumor size < 2 cm and ≥2 cm was different, and the larger tumor size suggested poorer survival rate. The following clinical factors of tumor size, primary location, primary clinical stage, and treatment before implantation had no correlation with recurrence in our sets. These results are different from the result obtained by Jerjes et al. They concluded that recurrence was associated with clinical N stage disease. Dantas et al believed that a lower patient survival rate was correlated with a more advanced stage of disease. Our data showed that 82.7% of recurrent cases had downgraded or original TNM stages, and high clinical TNM stage exhibited an inferior survival rate. However, there was no significance associated with these data according to statistical analysis.
As for the pathologic parameters, 89.2% of recurrent tumors remained at the primary histologic grading or were downgraded. Invasion suggested a poorer survival rate than noninvasion, but had no statistical significance. The vascular infiltration was significantly correlated with recurrence, although this result was inconsistent with the conclusion of Adel et al. Our conclusion was consistent with that made by Michikawa et al, who reported that the blood vascular invasion was associated with recurrence. This similar conclusion was also made by other authors. Seki et al analyzed 90 specimens of patients with previously untreated OSCC and determined that the presence of vascular invasion or lymph node metastasis was significantly associated with poor prognosis in the univariate analysis. Grimm reviewed the records of 429 consecutive patients after primary radical R0 tumor resection and 55 patients after brachytherapy and concluded that patients with increased microvascular invasion had a significantly poorer prognosis.
The perineural invasion rate in the current study was 26.3%, which was less than the reported perineural growth rates of 63% in head and neck squamous cell carcinoma. Limited sampling may have led to this discrepancy and ultimately concealed some invasion. It suggested that both clinician and pathologist should pay more attention to the detailed pathologic descriptions, especially those of invasion features. Importantly, precise and comprehensive pathologic diagnosis and description require more tissue blocks in representative areas. Multisite tumor sampling is necessary and efficient in this situation. At the same time, this could provide morphological implications for personalized and accurate treatment in instances of tumor heterogeneity.
Conclusion
Clinicopathologic parameters are important information for patients with OSCC who have undergone brachytherapy. Comprehensive pathologic diagnosis and microscopic description, especially for vascular infiltration, was valuable information that could be used to predict the prognosis. Surgeons and radiologists should pay more attention to detailed microscopic descriptions rather than only focus on pathologic terms or diagnoses. The pathologists should make the utmost detailed microscopic descriptions as well.
Footnotes
Authors’ Note
This study was approved by the ethical committee of Peking University School and Hospital of Stomatology. The approval number is PKUSSIRB-201732006.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by Program for New Clinical Techniques and Therapies of Peking University School and Hospital of Stomatology (PKUSSNCT-17A10).