
Abstract
This work evaluated a commercial fallback planning workflow designed to provide cross-platform treatment planning and delivery. A total of 27 helical tomotherapy intensity-modulated radiotherapy plans covering 4 anatomical sites were selected, including 7 brain, 5 unilateral head and neck, 5 bilateral head and neck, 5 pelvis, and 5 prostate cases. All helical tomotherapy plans were converted to 7-field/9-field intensity-modulated radiotherapy and volumetric-modulated radiotherapy plans through fallback dose-mimicking algorithm using a 6-MV beam model. The planning target volume (PTV) coverage (D 1, D 99, and homogeneity index) and organs at risk dose constraints were evaluated and compared. Overall, all 3 techniques resulted in relatively inferior target dose coverage compared to helical tomotherapy plans, with higher homogeneity index and maximum dose. The organs at risk dose ratio of fallback to helical tomotherapy plans covered a wide spectrum, from 0.87 to 1.11 on average for all sites, with fallback plans being superior for brain, pelvis, and prostate sites. The quality of fallback plans depends on the delivery technique, field numbers, and angles, as well as user selection of structures for organs at risk. In actual clinical scenario, fallback plans would typically be needed for 1 to 5 fractions of a treatment course in the event of machine breakdown. Our results suggested that <1% dose variance can be introduced in target coverage and/or organs at risk from fallback plans. The presented clinical workflow showed that the fallback plan generation typically takes 10 to 20 minutes per case. Fallback planning provides an expeditious and effective strategy for transferring patients cross platforms, and minimizing the untold risk of a patient missing treatment(s).
Keywords
Introduction
Modern radiotherapy treatment planning and delivery provide high conformity in target coverage and tissue sparing for adjacent organs at risk (OARs), thus improving tumor control probability and decreasing morbidity. 1,2 The 2 radiotherapy treatment modalities that can achieve advanced plan complexity include conventional L-shape linear accelerators, that is, Elekta (Stockholm, Sweden) and Varian (Palo Alto, California), and O-shape linear accelerators, that is, Tomotherapy (Accuray, Sunnyvale, California), and Halcyon (Varian, Palo Alto, California). The helical tomotherapy (HT) Hi-Art model combines a 6-MV linear accelerator and a helical Mega-voltage computed tomography (MVCT) scanner for delivering highly conformal intensity modulated helical beams. The technical details and clinical efficacy of HT have been well described in medical physics literature. 3 –5 The TomoEDGE (Accuray, Sunnyvale, California) series features dynamic jaws that open and close when tracking the target boundary as it enters and exits the treatment field. 6 –10 This feature reduces the dose penumbra along the superior and inferior direction, thus improves conformity. 6 –10 In the helical delivery, dose delivered to the target volume depends on the dose rate, multi-leaf collimator (MLC) delivery sequence, pitch, speed of gantry rotation, and total number of rotations. 11 Tomotherapy has demonstrated its ability to create high-quality plans that are comparable and/or superior to L-shaped linacs that deliver multifield intensity-modulated radiotherapy (IMRT) or volumetric-modulated radiotherapy (VMAT) plans for various cancer sites. 11 –14 Tomotherapy systems have significantly improved their reliability and reduced system downtime since their early installations. However, it remains a concern to those clinics that do not have twined systems to account for any downtime. At our institution, we treat about one-third of our patients on 1 Tomotherapy HDA (TM) unit, mostly using the helical IMRT delivery with the dynamic jaw feature. In an unintended machine down event, it is highly desired to have backup plans to continue those patients’ treatment on other L-shape linacs in the department. Treatment continuity is crucial for radiotherapy patients, especially for those with concurrent chemotherapy regimens, to avoid significant loss in local tumor control. 15 –18
Manual creation of a conventional backup plan for every tomotherapy plan might double dosimetrists’ planning time and physicians’ reviewing time. In response to the need of autoplanning, RayStation treatment planning system (RaySearch Laboratories AB, Stockholm, Sweden) has released its automated planning function, with the name fallback (FB) planning. The FB converts a given reference plan to plans that can be delivered on a different platform using dose-mimicking algorithm, that is, converting from an HT plan to a multifield IMRT or VMAT plan. This commercial software allows for automated creation and optimization of coplanar/noncoplanar 3D conformal radiotherapy (3DCRT), IMRT, and VMAT FB plans from reference plans’ dose–volume histogram (DVH) of any modality. 19 For clinics with only 1 tomotherapy unit, this solution can serve as a clinical treatment alternative when the tomotherapy unit is unavailable. So far there has been only 1 publication on the FB planning, which only evaluated clinical performance for converting HT plans to 3DCRT for lung and 9-field IMRT plans for lung, head and neck (HN), and prostate site. 20 Herein, we provide a more comprehensive evaluation of FB planning in generating multiple plan options, including 7-field IMRT, 9-field IMRT, and VMAT, for brain, HN, prostate, and pelvis patients. The goals of this study are to evaluate FB plan quality and its clinical workflow efficiency in the event of machine breakdown.
Methods
Plan Selection
From our patient database, a total of 27 previously treated HT patients were identified for this internal review board (IRB) (protocol no. CCRO050) approved retrospective study. The study included 7 brain, 5 simple HN, 5 complex HN, 5 pelvis, and 5 prostate cases. For 7 brain cases, disease sites included frontal, occipital, parietal lobes, and ventricles, with different levels of prescription dose varying between 25 and 55.8 Gy. For HN cases, 5 simple ones were unilateral and 5 complex ones were bilateral simultaneous integrated boost (SIB) targets. For simple HN plans, the planning target volume (PTV) was prescribed to receive at least 95% of 60 Gy in 30 fractions/66 Gy in 33 fractions. For SIB complex plans, the highest PTV dose was 70 Gy in 33 fractions. The pelvis cases were prescribed to at least 95% of the PTV receiving 45 Gy in 25 fractions. Among the 5 pelvis plans, 4 were considered complex with the para-aortic lymph nodes involvement. Among the 5 prostate cases, 2 were prescribed such that at least 95% of the PTV receives 70 Gy in 28 fractions, and the other 3 cases (intermediate/high risk) with proximal seminal vesicles involvement were treated to a total dose of 79.2 Gy in 44 fractions.
Fallback Planning Protocol
The predefined protocols are beam energy/treatment type specific and include information on beam angles, couch, and collimator angles. In this study, 2-arc VMAT and 7- and 9-field IMRT protocols were generated for FB plan creation. All VMAT plans were optimized further with 60 iterations in Raystation, while no additional optimization was made for FB IMRT plans. The dose-mimicking algorithm used for FB plan optimization uses an objective function to minimize the difference between the reference plan and FB plans generated for another treatment platform in terms of their DVH curves. Unit weight is given to the objective functions for OARs and targets are weighted based on user-defined target priority. 20 In our study, a target weight priority of 100 was used for all FB plans.
Clinical Workflow
Steps involved in a clinical implementation of an FB system are explained as follows: (1) Technique-specific protocols have been established at the time of commissioning, as explained in “Fallback Planning Protocol” section; (2) patients needing FB plans are identified by the physician at the time of treatment start; (3) on the day that FB plans are needed, as cases are prioritized, dosimetrists create FB plans and request physicians’ evaluation and approval; (4) approved plans are then transferred to Record and Verify (R&V) system, and second checked by a physicist per departmental policies and procedures; and (5) patient-specific quality assurance (QA) has to be performed for plan dose verification on the same day of the first fraction being delivered. Finally, the prescription is updated to account for the fractions delivered via FB plans before proceeding with the rest of the treatment.
Figure 1 depicted the timeline of generating an FB plan on the day when it is needed. DICOM files for CT, structures, and dose need to be transferred from HT to Raystation TPS. Plan preparation takes approximately 2 minutes for defining CT-density table, cleaning region of interest (ROI) types, creating external ROI, and inserting couch. Fallback plan creation based on the existing protocol takes approximately 5 minutes for IMRT plans and 10 to 15 minutes for VMAT plans, which require extra 40 to 60 iterations to achieve desired dose distribution. The overall plan creation time is 10 to 20 minutes. Depending on the planning workload or preference, an alternative workflow is to generate FB plans within a reasonable timeline after the original plans are done, that is, 1 week after treatment starts, in order to further reduce plan preparation time on the day of machine down and improve efficiency.
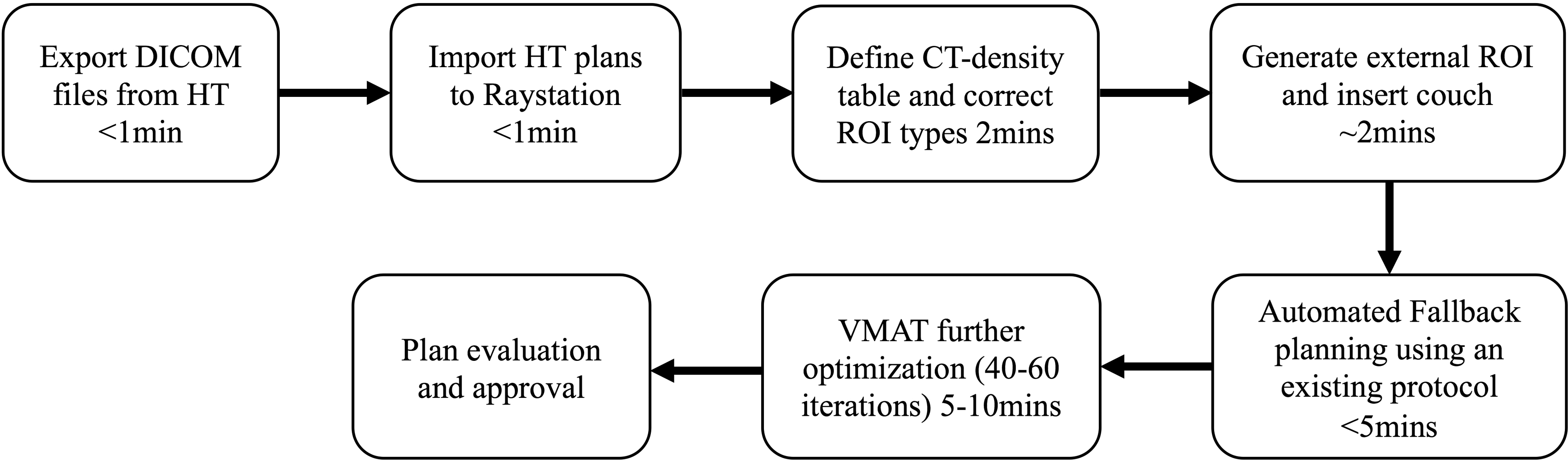
Flow diagram depicting the fallback plan creation and execution at our clinic. The approximate time taken during each step is illustrated.
Dosimetric Analysis
Plans are evaluated quantitatively for their dosimetric performance. For PTV coverage, the ratio of D 99 to prescription dose DRx , D 1 to DRx , and homogeneity index (HI), are compared. The HI analyzes the uniformity of dose distribution in the target volume and is defined as
where D 2 and D 98 are the dose to 2% and 98% of the PTV volume, respectively.
For the OAR avoidance comparisons, max-point (D max) or mean-point doses (D mean) are evaluated when applicable. For the pelvis plans, the OAR doses are evaluated using V45: V45 <80% (bladder), V45 <80% (rectum), and V45 <50 cc (small bowel), where VD is the percentage volume receiving a dose of at least D Gy. Prostate plans use mean point dose (D mean) for the penile bulb, V50 <40% for bladder, and V40 <50% for rectum. Final comparison tables for OARs are made showing ratios of dose points obtained from FB plans with respect to the reference plan (HT).
Results and Discussion
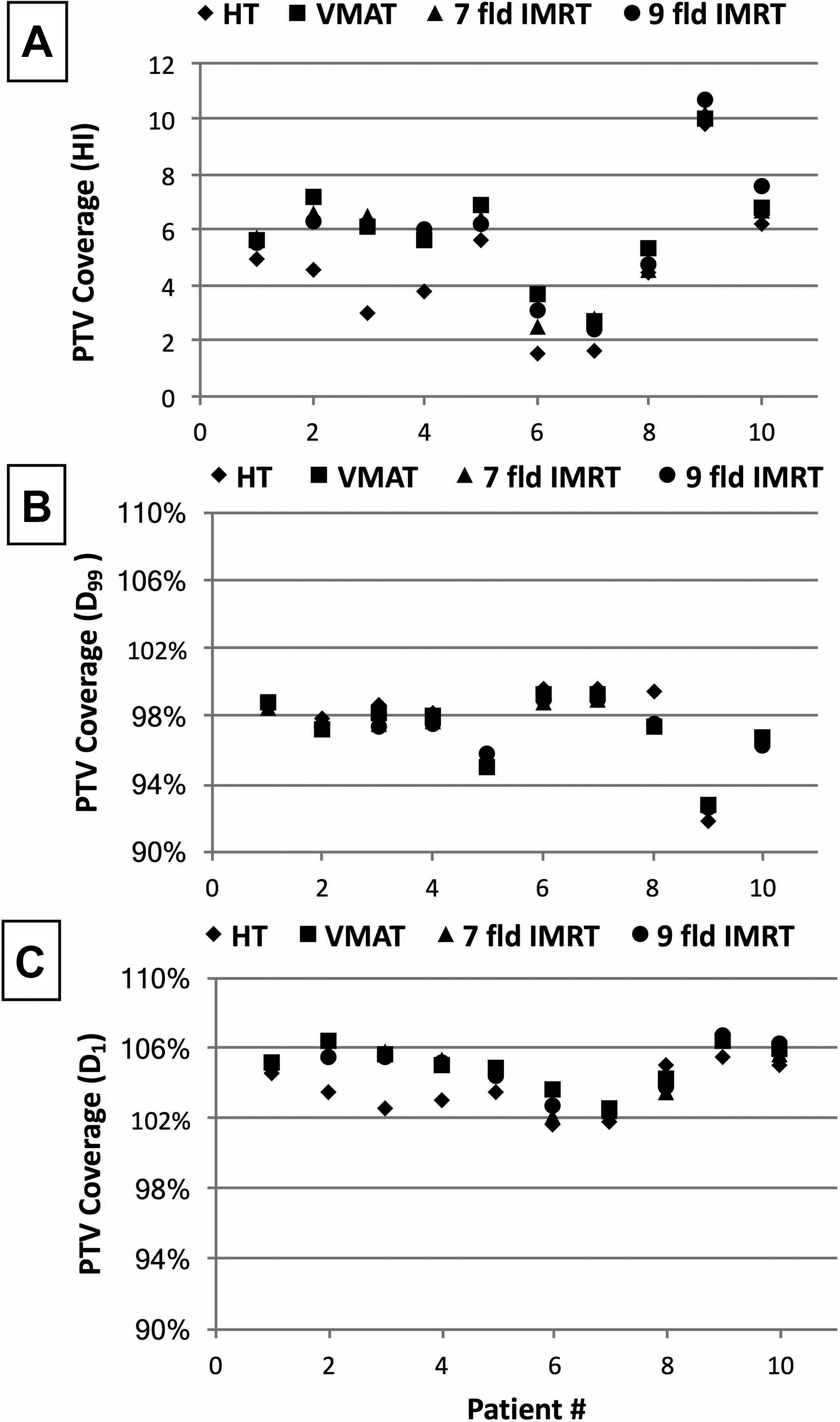
The dose mimicked plans are generated in the context of replacing entire treatment fractions and compared against their corresponding original HT plans for both PTV coverage and OAR avoidances. All plans studied here are physician-approved plans. The average values of HI, D 99/DRX , and D 1/DRX for brain, HN simple/complex, and pelvis/prostate plans in terms of the PTV coverage are listed in Table 1. For brain cases, all 3 FB plan techniques are comparable in terms of the PTV coverage, with slightly higher HI values compared to HT plans. For HN simple cases, although HT plans still show superior target coverage, the FB plans are acceptable with VMAT and 9-field IMRT demonstrating better PTV coverage conformity compared to 7-field IMRT plans. For the complex HN plans, all 3 FB techniques are comparable, with slightly inferior values to HT plans. Similar results are also seen in pelvis and prostate cases. PTV coverage metrics for individual case in terms of HI, D 99/DRX , and D 1/DRX for brain, HN, and pelvis/prostate plans are presented in Figures 2 to 4. Each HT plan (diamond) has its corresponding FB plans including VMAT (square), 7-field (triangle), and 9-field IMRT (circle) techniques. The HI, D 99/DRX , and D 1/DRX values are plotted in a scale of 0 to 12, 90% to 110%, and 90% to 110%, respectively. For brain cases (Figure 2), HI values (panel A) of the 3 FB techniques are slightly higher than the values of HT plans, residing in the range of 2 to 7. The D 99/DRX and D 1/DRX values (panel B and C) of the FB plans in each case are mostly overlapping with those of the HT plans. For simple/complex HN cases (Figure 3), HI values (panel A) cover a wider range, with most cases <10 for all FB plan options, except for 1 complex case. The D 99/DRX values (panel B) of all 3 FB options are −0.2% to 1.6% higher than the HT plan, while the D 1/DRX values (panel C) are 3.5% to 4.3% higher than the HT plans. For prostate and pelvis cases (Figure 4), HI values (panel A) of HT plans are averaged at 4.5 with a range of 1.6 to 9.8, while FB plans are average at 6.0 with a range of 2.5 to 10.7. Comparable values are seen in D 99/DRX and D 1/DRX .
Planning target volume (PTV) Coverage Comparisons of the VMAT and IMRT Plans Versus HT Plans.
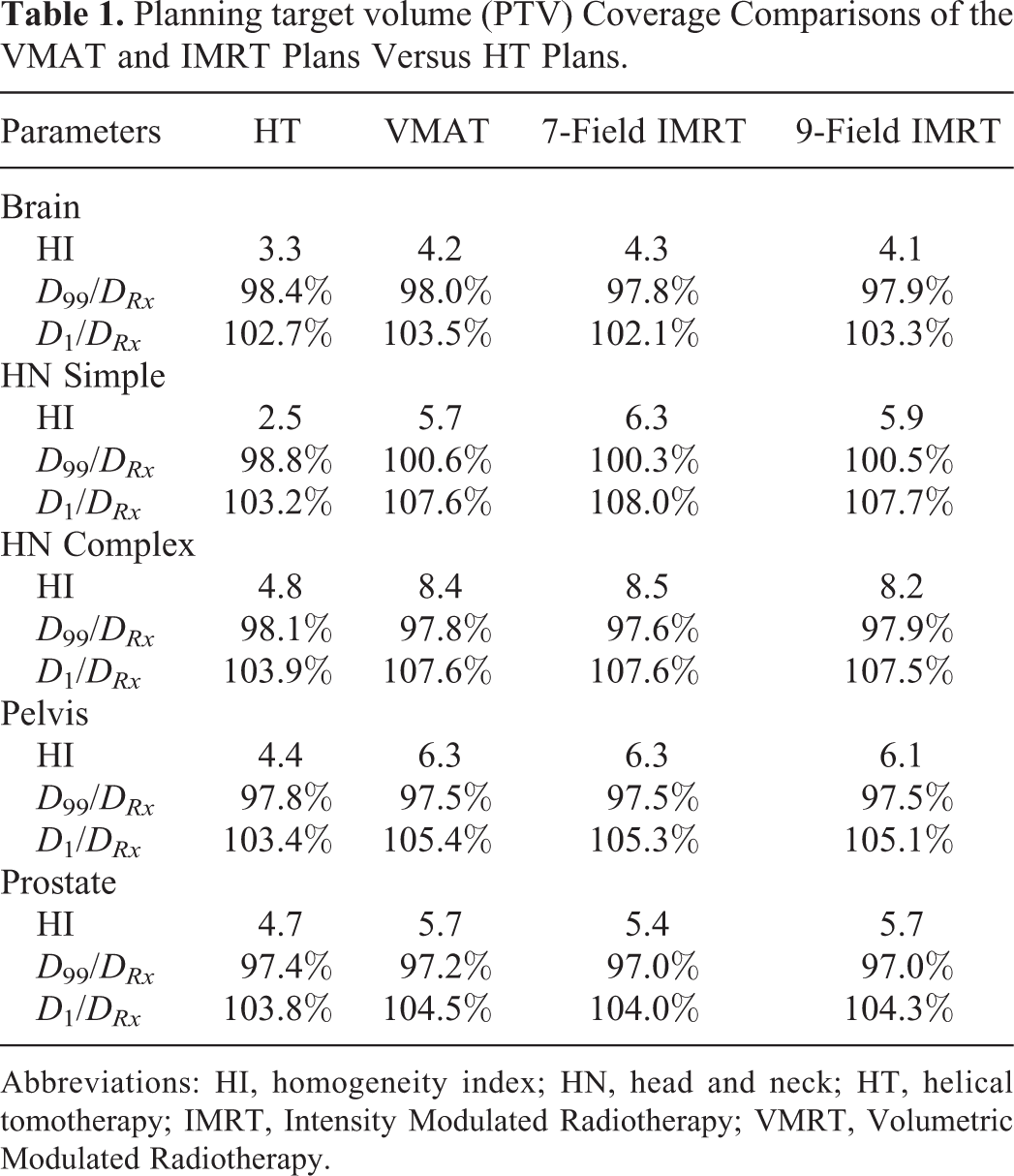
Abbreviations: HI, homogeneity index; HN, head and neck; HT, helical tomotherapy; IMRT, Intensity Modulated Radiotherapy; VMRT, Volumetric Modulated Radiotherapy.

Planning target volume (PTV) coverage of the brain fallback plans compared to the helical tomotherapy (HT) plans. The homogeneity index (HI), D 99/DRX , and D 1/D RX values are shown in panel (A), (B), and (C), respectively.

Planning target volume (PTV) coverage of the head and neck (HN) fallback plans compared to the helical tomotherapy (HT) plans. The homogeneity index (HI), D 99/DRX , and D 1/DRX values are shown in panel (A), (B), and (C), respectively.
Planning target volume (PTV) coverage of the pelvis/prostate fallback plans compared to the helical tomotherapy (HT) plans. The homogeneity index (HI), D 99/DRX , and D 1/DRX values are shown in panel (A), (B), and (C), respectively.
The OAR dose constraints for all HT treatments depend on the complexity of the plan and strictly follow the guidelines per our physicians. Dose constraints for brain treatment are applied to various OARs, including left and right lens/eye/optic nerve/cochlea, optic chiasm, and brain stem during plan optimization. Table 2 listed the OAR dose comparison ratios of VMAT/HT, 7-field IMRT/HT, and 9-field IMRT/HT for brain cases, in terms of D avg and D max for 15 structures. Overall, VMAT shows on average 11% (range: −13% to 36%) higher dose compared to HT for those 15 OARs, while 7-field IMRT and 9-field IMRT show on average 13% (range: −23% to 1%) and 10% (range: −21% to 1%) lower dose compared to HT. The OAR dose comparisons for HN simple/complex plans are listed in Table 3. The dose constraints are applied to brainstem, cord, larynx, upper esophagus, left and right parotid during plan optimization. Results show that for simple HN cases, the 3 FB plan options provided OAR doses comparable to the original HT plans, with VMAT plans being slightly superior (average: −3%; range: −13% to 5%) to HT plans. For complex HN cases, only VMAT plans are equivalent to HT plans, with an average dose ratio of 1.01 and a range of 0.92 to 1.09. The other 2 IMRT plans are shown slightly inferior to HT plans, with the same dose ratio of 1.08 and a range of 0.98 to 1.20. The OAR dose ratios of FB plans versus HT plans for pelvis/prostate are provided in Table 4. Compared to HT plans, all 3 options show lower OAR doses, that is, VMAT −11% to 0%, 7-field IMRT −9% to 1%, and 9-field IMRT −8% to 2%. For prostate, typical dose constraints followed the RTOG 0815 protocol and the institution-specific guidelines, including D ave <52 Gy for penile bulb, V50Gy <40% for bladder, and V40Gy <50% for rectum. Results show superior dose on the OARs in FB plans compared to HT plans, with VMAT ranging from −12% to −1%, 7-field IMRT −15% to 1%, and 9-field IMRT −19% to 2%.
OAR Dose Comparisons of VMAT and IMRT Plans Versus HT Plans for Brain.

Abbreviations: HT, helical tomotherapy; IMRT, Intensity Modulated Radiotherapy; OAR, organs at risk; VMRT, Volumetric Modulated Radiotherapy.
OAR Dose Comparisons of VMAT and IMRT Plans Versus HT Plans for HN Cases.
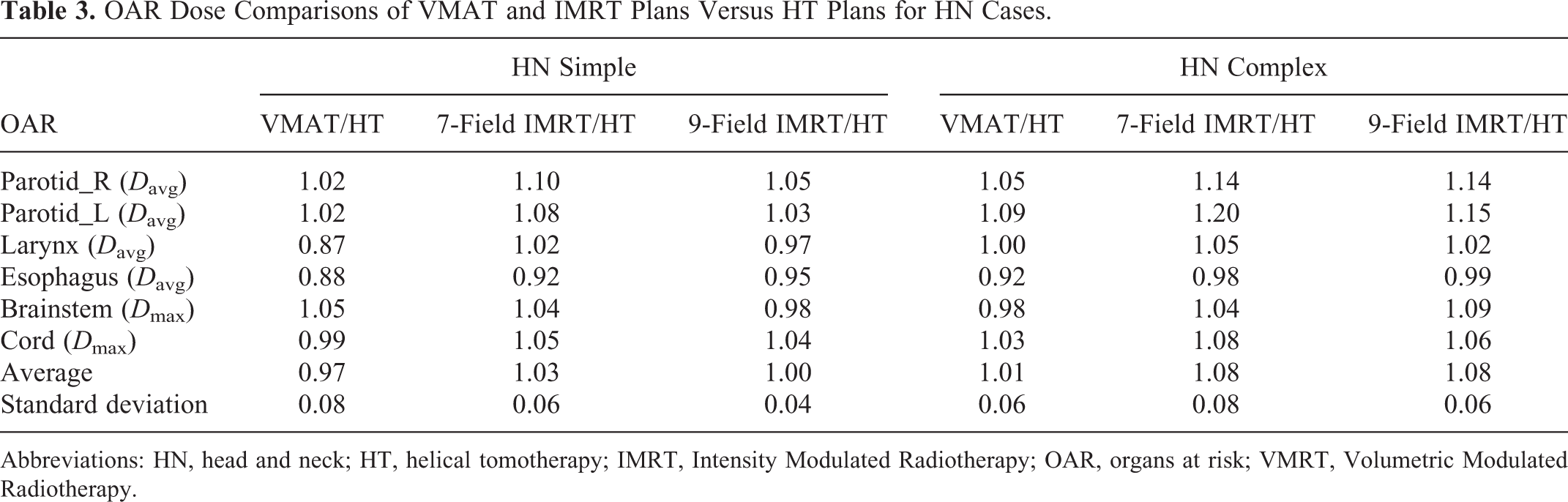
Abbreviations: HN, head and neck; HT, helical tomotherapy; IMRT, Intensity Modulated Radiotherapy; OAR, organs at risk; VMRT, Volumetric Modulated Radiotherapy.
OAR Dose Comparisons of VMAT and IMRT Plans Versus HT Plans for Pelvis and Prostate Cases.

Abbreviations: HT, helical tomotherapy; IMRT, Intensity Modulated Radiotherapy; OAR, organs at risk; VMRT, Volumetric Modulated Radiotherapy.
Note that the plan comparisons are performed for all fractions of the original HT and their FB plans. For the actual clinical scenario, we experienced so far, the maximum fractions that we had to supplement with the FB plan was 2. Under this circumstance, the overall dosimetric differences between all 3 FB plans and original HT plans are considered negligible and not clinically significant. For plan delivery verification, patient specific QA was performed on all plans included in this study using Sun Nuclear’s ArcCHECK or MapCHECK 2 devices. All QA plans achieved >95% pass rate using the 3%/3 mm γ analysis criteria.
In this study, 2-arc VMAT, 7-, and 9-field IMRT plans were generated for each HT plan studied. Once the protocol is created, all FB plans can be generated within 10 to 20 minutes depending on the plan type, using a dose-mimicking algorithm based on the DVH imported from the original HT plan. As for physician’s evaluation and plan approval, it varies significantly depending on physician’s availability. In a rare scenario of a machine breakdown in our center, most physicians would make these plans first priority. Therefore, plan evaluation and approval time is roughly 30 minutes. As we mentioned previously, FB plan QA is performed after the first treatment fraction; therefore, it is not taken into account in the pressuring timeline of FB plan preparation. In terms of the target coverage, no clinically significant differences were observed within 3 FB options, with all of them being slightly inferior to the HT plans considering the entire prescribed fractions. For brain OARs, VMAT gives on average 11% higher doses compared to HT, while both IMRT techniques give on average 9% lower doses. For HN OARs, all 3 techniques are equivalent to the HT plans for simple HN cases, while for complex cases, both IMRT techniques have on average 8% higher doses compared to HT. For both pelvis and prostate cases, all 3 techniques result in on average 5% and 8% lower doses compared to HT, respectively. Zhang et al also studied the performance of 9-field IMRT for HN and prostate cases and presented similar findings with inferior target coverage and comparable OAR dose sparing compared to HT. 20 Our study further explored the performance of 7-field IMRT and VMAT for all 4 anatomical sites, which provided a more practical solution to the clinic considering much shorter treatment delivery time with 7-field IMRT or VMAT.
The FB planning module provides the automated plan optimization and creation ability for efficiently generating conventional linac-based plans mimicking the dose distribution from the initial HT plans. The dose mimicking optimization process seeks to create a similar DVH of an HT plan with an alternative treatment technique (ie, IMRT or VMAT) by maintaining target conformity and penalizing dose falloff outside the target. Overall, for all 4 anatomical sites, FB plans are inferior in target coverage but within ±10% for OAR avoidance in the context of the entire prescribed treatment. Considering the actual need for these FB plans is mostly <10% of the prescribed fractions, the dose deviation caused by supplementing with the FB fractions should be <1%. When choosing an FB technique, VMAT is comparable to IMRT plans in terms of the dose coverage for HN, pelvis, and prostate cases. Yet VMAT delivery would be faster than IMRT, with the cost of extra 10 minutes in plan optimization when creating the FB plan. For brain, no clinically significant dose differences were observed between 7-field and 9-field IMRT, while VMAT is inferior in OAR sparing. Therefore, 7-field IMRT may be a better option than 9-field considering the time efficiency in plan delivery.
Conclusion
Transferring and mimicking treatment plans across platforms from an O-shaped linac to an L-shaped linac have been automated by a commercial program which requires modest time and effort from planners. Dosimetric evaluation of the mimicked plans has been performed, which demonstrated that FB plans are deliverable and clinically comparable to the overall treatment plan when utilized as a backup option. The overall workflow can be a practical and efficient alternative for patient treatment in the event of machine down. Further efforts are underway to optimize the quality and flexibility of FB planning for potential use in a wider array of treatment delivery options and cross-platform technologies.
Footnotes
Authors’ Note
Z.Y. and C.K.N. contributed equally to the manuscript.
Acknowledgments
We would like to thank Peter Paetzold and Jay Markham from RaySearch Laboratories, Stockholm, Sweden for their help and training with the software.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors Zilong Yuan and Jianfeng Qiu were supported by the China National Key Research and Development Program (2016YFC0103400).