
Abstract
Purpose:
The purpose of the present study was first to apply the progressive optimization algorithm based automatic volumetric modulated arc therapy (POA-VMAT) technology to accelerate and improve the radiotherapy of cervicothoracic esophageal cancer (CTEC). We comprehensive analyze the feasibility, normal tissue complication probability (NTCP) and dosimetric results of POA-VMAT, manual based VMAT and step-shoot intensity-modulated radiation therapy (IMRT) plans in the treatment of CTEC.
Methods:
Sixty patients with CTEC with or without concomitant chemotherapy at our institution between 2017 and 2019 were retrospectively identified. The manual 7field-IMRT (7f-IMRT), Single-arc-VMAT and Double-arc-VMAT (Single-Arc/Double-Arc) plans were generated in all cases. The POA-VMAT was designed using the automatic dual-arc VMAT technology of Pinnacle3 9.10 planning system based on progressive optimization algorithm. Specially, it includes the selection of treatment techniques, the running of automated planning scripts, and the evaluation of the final radiotherapy regimen. Subsequently, quantitative evaluation of plans was performed by means of standard dose–volume histograms, homogeneity index (HI) and conformity index (CI).
Results:
Target dose conformity of the 7f-IMRT plan was inferior to all plans, whereas the Double-Arc plan was slightly inferior to the POA-VMAT but superior to the Single-Arc and 7f-IMRT plan. The HI for 7f-IMRT, Single-Arc, Double-Arc and POA-VMAT were 0.17 ± 0.08, 0.28 ± 0.06, 0.29 ± 0.06 and 0.28 ± 0.03, respectively. For the NTCP results, there was significant statistical difference among POA-VMAT, IMRT and VMAT plans. The total MU was reduced by 48.3% and 42.1% in Single-Arc and POA-VMAT plans compare to IMRT plans.
Conclusions:
By comprehensive consideration, POA-VMAT efficiently generate acceptable treatment plans for CTEC without dose escalation to OARs and overall superior to manual planning which is a good option for treating CTEC.
Keywords
Introduction
Neoadjuvant chemo-radiation is currently considered as a standard treatment modality for locally advanced esophageal cancer patients who are not surgical candidates or surgery is refused by them. 1 -3 Squamous cell carcinoma of the cervical-thoracic esophagus is comparatively rare and accounting for 2%-10% of all esophageal cancers. 4,5 A major concern for cervical-thoracic esophageal cancers (CTEC) is radiation-associated toxicities due to complex anatomic features and organ at risk (OAR) shape variability. The best radiation therapy technique for CTEC that can reduce toxicities while delivering the appropriate target coverage has not been clinically determined.
As a novel form intensity-modulated radiotherapy (IMRT) technique, volumetric-modulated arc therapy (VMAT) owns more freedom delivery degrees during gantry rotation which accompanied by dynamic multi-leaf collimator with variable dose rates and gantry speed modulation. 6 -8 Investigations have demonstrated VMAT can produce dosimetrically better plans with adjacent OARs sparing and PTV coverage, while reducing the overall monitor units (MUs) and shorten the therapists time, thereby overcoming the primary shortcomings of IMRT. 9 -13 Moreover, the shorter delivery time of VMAT technique may result in better local disease control due to its biological advantages for cancer cell killing, the fewer delivered MUs could reduce the undesirable irradiation of healthy tissues and lower the probability of suffering from secondary cancer. 14 -19
However, the approach of manual optimization parameter tuning and re-optimization is inefficient and very time-consuming. So the prescriptive and data-driven technique has accumulated popularity in that can help automate the treatment planning process. 20 -24 Recently, various Automated planning techniques including Rapid-Plan (Varian Medical Systems, Palo Alto, CA), Multi-Criteria Optimization (RaySearch Laboratories, Stockholm, Sweden), and Pinnacle 3 Auto-plan (Philips Medical Systems, Best, The Netherlands) have been explored to speed up the planning process using clinical plans templates, and reduce planner variability and drastically improve the RT planning quality and efficiency of the treatment plans. 25 -28 Wang et al used Auto-plan technique for whole brain RT planning and found that Auto-plan was capable of meeting PTV dose coverage and OARs constraint objectives while sparing the planning time. 28 Breedveld et al proposed a novel multi-criterion optimization approach which using a quadratic objective function with voxel-dependent importance factors to automatically calculation for beam profile optimization. 20 In another retrospective study performed by Nawa et al. 27 They retrospectively analyzed prostate cases of Auto-plan and previously delivered clinical plan, which found that the plan quality was equal, and better than manual plans in some cases.
To the best of our knowledge, no investigation had applied the Auto-plan approach to CTEC patients and compared to VMAT and IMRT techniques. Furthermore, the investigations for CTEC are limited due to the scarcity of this disease. In this work, we first to apply the automatic volumetric modulated arc therapy (POA-VMAT) technology to accelerate and improve the radiotherapy of CTEC. The POA-VMAT was designed using the automatic dual-arc VMAT technology of Pinnacle 3 9.10 planning system. Specially, the progressive optimization based auto-planning engine was induced to automatically adapt objectives, constraints, and auxiliary structures during optimization. It includes the selection of treatment techniques, the running of automated planning scripts, and the evaluation of the final radiotherapy regimen. Subsequently, quantitative evaluation of plans was performed by means of standard dose–volume histograms (DVH), homogeneity index (HI) and conformity index (CI). Then we conducted a comprehensive scientific comparison among POA-VMAT, VMAT and IMRT to determine the most efficient treatment modality for CTEC based on the dosimetric comparison using statistical analysis methods. The study was approved by our institution’s review board (IRB). Since this study was done retrospectively and we did not apply any of these virtual treatments to patients, this study did not require written or verbal consent. Additionally, the study is done on anonymized patient data.
Materials and Methods
Patients and Simulation
Between 2017 and 2019, 60 patients with CTEC were treated at the first affiliated hospital of Nanchang university. Table 1 listed the patient specifics. All patients were staged according to the 7th edition of the AJCC–UICC staging system. Treatment planning was based on a 4D KV-CT scan with slice thickness of 2 mm and performed using Pinnacle treatment planning systems (clinical version 9.10; Philips, Fitchburg, WI). Patients were scanned with a computed tomography simulator in the supine position with arms above the head.
Patient Specifics (n = 60).

Target Definition, Contouring and Planning Objectives
CT, MRI and PET-CT were used to delineate the target volume by radiotherapy physician and radiologist. The clinical target volume (CTV) included the esophageal tumor, with a margin for microscopic tumor extension, and the adjacent lymph nodes. For the PTV, a 3-dimensional margin of 5 mm was added to the CTV to account for the variability in patient setup, uncertainty in target definition, and organ motion. The following OARs including lungs, heart, spinal cord and the healthy tissue were defined as the patients’ volume covered by the body volume excluding the PTV.
To avoid any bias or rescaling effect in the comparison, the prescription percentage for all plans were normalized to 95% and all plans were normalized to respective mean dose to PTV. Various planning objectives were imposed. The plan objectives were: For PTV, plans aimed to achieve 57 Gy (−5% to +7%); for spinal cord, maximum dose no more than 45 Gy; for heart, Dmean ≤ 35 Gy, V30Gy < 40%, V40Gy < 30%. For lungs, normalized mean total dose of 20 Gy was associated with a normal tissue complication rate of 13–14%, which was deemed acceptable. The mean dose was limited to <20 Gy in combination with other 2 complementary constraints: V20Gy < 40% and V30Gy < 18%. Total lung V5Gy < 45% and V10Gy < 35%; the mean dose was kept <40 Gy with an additional constraint of D35% <38 Gy.
Dose Prescription, Treatment Planning and Delivery
The prescription dose was 2Gy×30 fractions for a total dose of 60 Gy. Step-and-shoot technique was adopted for each patient, with intensity level 20, dose rate 300 MU/min, and 7 coplanar fields (7f-IMRT) were oriented at 0°, 51°, 102°, 153°, 204°, 255° and 306°, beam energy of 6MV X-ray was used. Two VMAT plans were generated. The Single-arc-VMAT (Single-Arc) was planned with start and stop angles of 179° and 181°, respectively, delivered with counter-clockwise rotation. The Double-arc-VMAT (Double-Arc) comprised of a counter-clockwise and a clockwise arc from gantry angles 179.9–181.1° and 181.1–179.9°, respectively. The collimator was rotated (20–250°) in the present study, allowing it to cover the entire tumor and minimize the contribution of tongue and groove effect during the arc rotation. All plans were optimized by one senior medical physicist to reach clinically acceptable PTV coverage and OAR sparing. At least 95% of the PTV had to be covered by 95% of the prescription dose.
In the present study, an inverse optimizer plugin named POA-VMAT module was installed in Pinnacle 3 version 9.10. The POA-VMAT engine was applied to a 2 coplanar disjointed arcs technique which consists of 2 full coplanar arcs, and the optimization parameters of POA-VMAT including creating auxiliary ROIs according to the configuration file, adding isodose lines for POA-VMAT and adjusting objectives during optimization. It is worth noting that the optimizer plugin will check the hard constraint list and add corresponding objectives then optimize again if the actual index is not pass the hard constraint. The template of POA-VMAT plays a critical role in the inverse optimizer plugin outcome. Specifically, we created the template with the same isocenter, machine, arc length, collimator angle, couch angle, and energy based on the parameters of previously manually optimized plan; the DVH information of previous 40 plans was extracted to construct the constraints of OARs for plan optimization. According to previous planning experience, the template optimization parameters were assigned referring to the quantitative analysis of normal tissue effects (QUANTEC) in the clinic values for OARs sparing and target coverage with priority values.
Plan Evaluation and Comparison
Quantitative evaluation of plans was performed by means of standard DVH, MUs, HI and CI.
13
Doses to OARs and coverage of the PTV were evaluated using a DVH. Given the superior location of tumor, interest for critical structure sparing only included dose to esophagus, dose to heart, mean dose to the total lung, volume of the total lung receiving 20 Gy, maximum dose to the spinal cord. To evaluate PTV coverage, minimum, maximum and mean dose to the PTV as a percentage of the prescribed dose were compared among the 3 methods. The HI of the treatment was expressed in terms of D1%-D99%
Results
Target Dosimetric Parameters
The dose distributions of one patient with corresponding cumulative DVHs for both PTV and OAR are shown in Figure 1 and Figure 2. In Tables 2 -4, an overview of the numerical findings from average DVH analysis on OARs and PTV are reported to assess for the relative inter-patient variability.

The transverse, coronal and sagittal dose distributions in one representative patient of for the 3 treatment plans: (A) 7f-IMRT, (B) Single-Arc, (C) Double-Arc, d) POA-VMAT.

Representative normalized, cumulative dose–volume histogram (DVH) comparison in one representative patient of for the 3 treatment plans: (A) 7f-IMRT, (B) Single-Arc, (C) Double-Arc, (D) POA-VMAT.
The Summary of Numeric Analysis From DVH for Target Volumes.

Statistically significant differences (p < 0.05) of paired t-test analysis for 4 plans; a: 7f-IMRT vs. Single-Arc; b: 7f-IMRT vs. Double-Arc; c: 7f-IMRT vs. POA-VMAT; d: Single-Arc vs. Double-Arc; e: Single-Arc vs. POA-VMAT; f: Double-Arc vs. POA-VMAT. *: using 2-paired Wilcoxon’s signed ranks test. NS: Not significant.
OARs Dose Calculated From The DVHs.
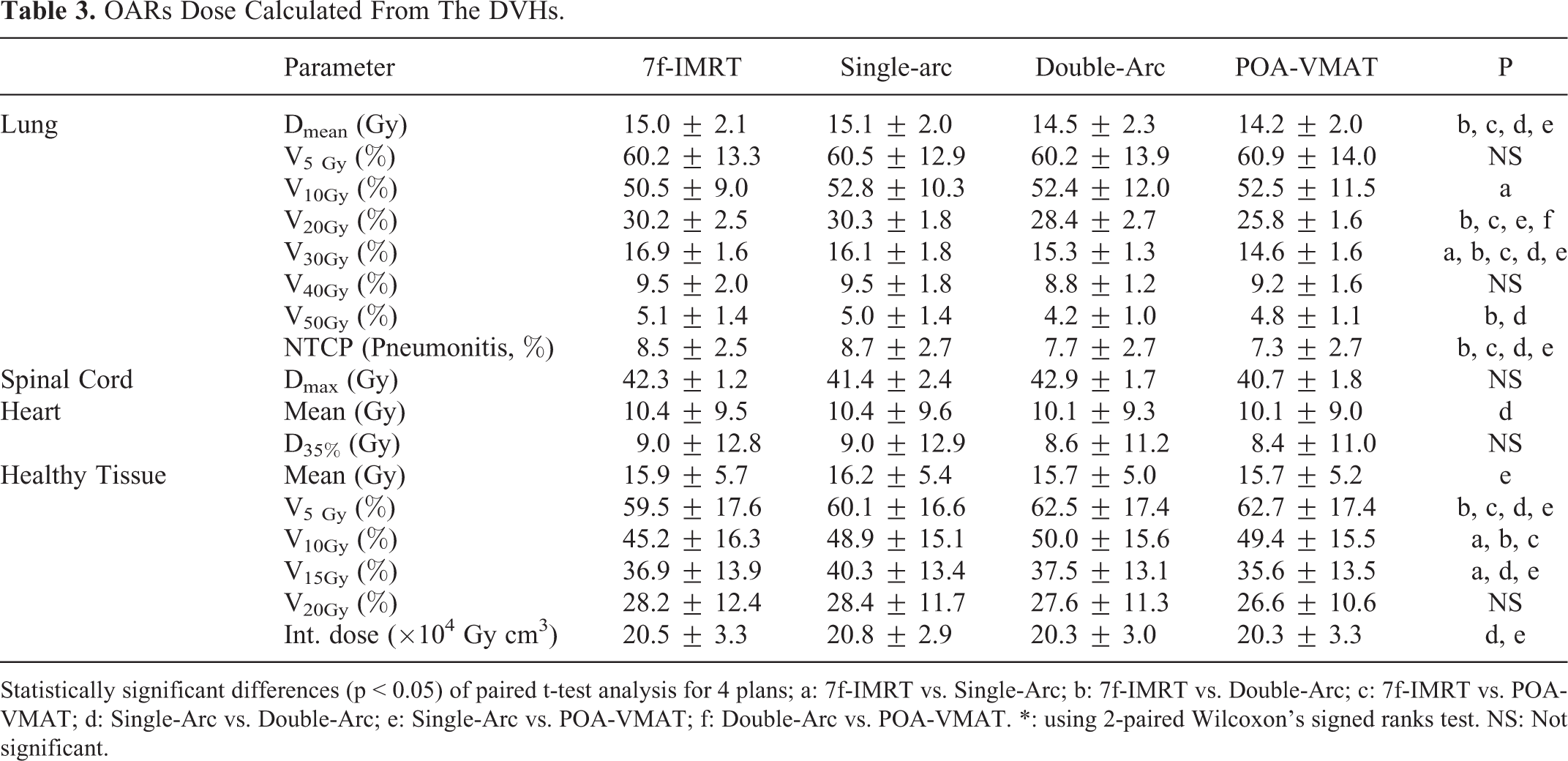
Statistically significant differences (p < 0.05) of paired t-test analysis for 4 plans; a: 7f-IMRT vs. Single-Arc; b: 7f-IMRT vs. Double-Arc; c: 7f-IMRT vs. POA-VMAT; d: Single-Arc vs. Double-Arc; e: Single-Arc vs. POA-VMAT; f: Double-Arc vs. POA-VMAT. *: using 2-paired Wilcoxon’s signed ranks test. NS: Not significant.
Total MU and Delivery Time.

Statistically significant differences (p < 0.05) of paired t-test analysis for 4 plans; a: 7f-IMRT vs. Single-Arc; b: 7f-IMRT vs. Double-Arc; c: 7f-IMRT vs. POA-VMAT; d: Single-Arc vs. Double-Arc; e: Single-Arc vs. POA-VMAT; f: Double-Arc vs. POA-VMAT. *: using 2-paired Wilcoxon’s signed ranks test. NS: Not significant.
Clinically acceptable plans of 7f-IMRT, Single-Arc, Double-Arc and POA-VMAT were completed for all 60 patients. Specific results for PTV are shown in Table 2. The POA-VMAT results in better PTV coverage than IMRT and VMAT plans. The target dose conformity of the 7f-IMRT plan was inferior to all plans. The Double-Arc plan achieved the best conformity, whereas the Single-Arc plan was slightly inferior to the POA-VMAT but superior to the 7f-IMRT plan. But there were no statistically significant differences between the plans. The HI for 7f-IMRT, Single-Arc, Double-Arc and POA-VMAT were 0.17 ± 0.08, 0.28 ± 0.06, 0.29 ± 0.06 and 0.28 ± 0.03, respectively. The target coverage of PTV for 4 modalities was with a V95 of 95.8 ± 3.2, 95.4 ± 2.3, 99.4 ± 0.3 and 99.8 ± 0.1 for 7f-IMRT, Single-Arc, Double-Arc and POA-VMAT, respectively. For V107%%, significant differences were observed between 7f-IMRT vs. POA-VMAT, Single-Arc vs. POA-VMAT and Double-Arc vs. POA-VMAT.
OARs Dosimetric Parameters
As summarized in Table 3, Dmean, V20 and V30 for lung in VMAT plans were lower than in IMRT plans (p < 0.05). V20 reduced from 30.2% ± 2.5% in 7f-IMRT and 30.3% ± 1.8% in Single-Arc to 28.4% ± 2.7% in Double-Arc and 25.8% ± 1.6% in POA-VMAT. V30 reduced from 16.9% ± 1.6% in 7f-IMRT and 16.1% ± 1.8% in Single-Arc to 15.3% ± 1.3% in Double-Arc and 14.6% ± 1.6% in POA-VMAT. Dmean reduced from 15.0 ± 2.1 Gy in 7f-IMRT and 15.1 ± 2.0 Gy in Single-Arc to 14.5 ± 2.3 Gy in Double-Arc and 14.2 ± 2.0 Gy in POA-VMAT. V5 and V40 showed no difference among all plans. Lung V50 in Double-Arc was lower than that of 7f-IMRT, while there was no statistical difference among 7f-IMRT, Single-Arc and POA-VMAT. NTCP results were also shown in Table 3. There was significant statistical difference among POA-VMAT, IMRT and VMAT plans. VMAT plans reduced the NTCP of lung pneumonitis by 1% compared to IMRT plans.
All plans complied with the planning objective of 45 Gy as maximum dose to the spinal cord (Table 3). The POA-VMAT plans were significantly improved the dose for spinal cord among all the plans and superior in sparing the heart in terms of Dmean and D35%. The mean dose to heart for VMAT plans was better than IMRT plans by a marginal percentage variation. Similar results were for D35% heart doses. However, there was no statistical significance between these 4 plans, except that Double-Arc plan showed a significant difference in heart mean dose when compared with Single-Arc plan. Details were in Table 3.
The IMRT and VMAT plans presented similar results in the DVH of the healthy tissue (Table 3). However, the difference are significant in low dose-volumes (volume receive 5-20 Gy). The VMAT plans increased V5 by 2.8% when compared to IMRT plans. Similar situation was seen in V10, the value was 2.6%. Contrary results happened to V15 and V20, the VMAT plans confer a reduction by 2.1% and 1.2%, respectively. For the mean dose of healthy tissue, there are no substantial statistic difference between 4 plans except for Single-Arc and POA-VMAT. And for integral dose, POA-VMAT plans were slightly better than Double-Arc. As displayed in Table 4, compared with IMRT plan, the total MU was reduced by 42.1% in VMAT plan. For Single-Arc plans, the value was 49.6% and 34.6% for POA-VMAT plans. Similarly, the total MU for the 7f-IMRT, Double-Arc and POA-VMAT plans were 868.2 ± 182.0 MU, 870.0 ± 225.3 MU and 548.8 ± 47.2 MU, respectively.
Discussion
Radiotherapy plays a predominant role within multimodal treatment concepts for CTEC because of protecting esophageal shape and function. 31 In recent years, clinical studies have shown that IMRT and VMAT based techniques are better than conventional 3-dimensional conformal radiation therapy with respect to improved PTV coverage and OARs sparing in the treatment of CTEC. 32 -34 Currently, manual-based treatment plans were widely used in clinical practice where the approach of manual optimization parameter tuning and re-optimization is inefficient and time-consuming. Such the desire for a prescriptive and data-driven technique has accumulated popularity in that can help automating the treatment planning process. Auto-plan technique has improved plan quality and consistency and drastically reduced treatment planning workload compared to manual trial-and-error planning. 35 -38 In this work, the automatic volumetric modulated arc therapy technology was used to improve the radiotherapy of CTEC which designed by the automatic double arc VMAT technology. Specially, the progressive optimization based auto-planning engine was induced to automatically adapt objectives, constraints, and auxiliary structures during optimization. We evaluated and qualitative analyzed the feasibility, NTCP and dosimetric results of POA-VMAT, VMAT and IMRT plan in the treatment of CTEC.
The results of this study show that the PTV Dmean, D2% and V107% of POA-VMAT was significantly improved compared to 7f-IMRT, Single-Arc, Double-Arc. It is mainly attributed to the progressive optimization algorithm to automatically create auxiliary structures and iteratively adjusts objectives based on the desired target coverage and OAR sparing during optimization. Significant differences were observed for PTV V95% from the comparison between any 2 techniques of the 4 methodologies except for Double-Arc vs. POA-VMAT. In this study, 7f-IMRT (p < 0.05) resulted a lower HI compared with other 3 methods, indicating a better dose homogeneity. Double-Arc and POA-VMAT had higher conformity indices compared to 7f-IMRT and Single-Arc plans, but there were no significant difference observed.
The results also indicate that Double-Arc and POA-VMAT plans yielded significantly lower lung Dmean, V30 and NTCT than the 7f-IMRT and Single-Arc plans, while the 7f-IMRT could achieve optimal lower lung V10 and similar V5 compared to other 3 methods. This was consistent with the study of Wuet al. 35 To further evaluate differences in risk of toxicity, LKB based NTCP model was assessed, the model parameters used in the LKB model were: a volume exponent n, the dose for 50% complication probability TD50 and a steepness parameter m with values of n = 1, TD50 = 31.4 Gy, m = 0.45, respectively, according to QUANTEC publication. POA-VMAT plans achieved the best with NTCP (7.3% ± 2.7%), whereas Single-arc plans were worst with NTCP (8.7% ± 2.7%). POA-VMAT plans reduced NTCP of lung pneumonitis nearly 1% compared to 7f-IMRT plans. And Double-Arc plans (7.7% ± 2.7%) were superior to 7f-IMRT (8.5% ± 2.5%). Although NTCP models were theoretical values, it could predict risk of toxicity to a certain extent. POA-VMAT decreased the maximum dose to spinal cord, but no significant difference was observed. Similar results for heart Dmean and D35% among the 4 methodologies had been observed in Table 3. Although it was of minor improvement for our comparison, the cardiac dose may become more important as cure rate improves, it was still desirable to reduce cardiac dose as much as possible. Radiation-associated cardiac diseases were slowly progressing until 10-20 years after radiation.
By stratifying the planning techniques in terms of sparing of the healthy tissue, the mean dose and the integral dose for the 4 methods showed similar dosimetric results. However, at low dose levels (5-10 Gy), POA-VMAT and Double-Arc plans showed increase in dose by 2-3% compared with 7f-IMRT plans, while with the dose levels escalation (15-20 Gy), POA-VMAT and Double-Arc plans showed reduction in dose by 1-2% compared with 7f-IMRT plans. VMAT was performed simultaneously with rotation by a dynamic MLC adaptation to the target volume during the rotation thus reduced the number of required MU. In this study, POA-VMAT offered a clear benefit in terms of reduction in MU compared with 7f-IMRT and the reduction on MU in turn leaded to reduce treatment delivery time. Theoretically, the significant reduction of MU may reduce the risk of secondary malignancies. It is well known that esophageal cancer patients treated with their arms extended above their head and require the patient immobilized in supine position, which make the patient very uncomfortable. This POA-VMAT method offered a lesser treatment time can relieve a lot of discomfort in patients and reduced the likelihood of patient activity during treatment. In addition, lesser MU improved the utilization of machine.
Conclusions
For the treatment of CTEC, POA-VMAT efficiently generates acceptable plans for CTEC without dose escalation to OARs while maintaining PTV coverage, POA-VMAT technology is a feasible planning method for CTEC.
Footnotes
Authors’ Note
Yongqiang Zhou and Xiaojun Xiang contributed equally to this study. The study was approved by First Affiliated Hospital of Nanchang University’s Institutional Review Board (IRB) as part of an ongoing quality improvement investigation. Since this study was done retrospectively and we did not apply any of these virtual treatments to patients, this study did not require written or verbal consent. Additionally, the study is done on anonymized patient data. The First Affiliated Hospital of Nanchang University has determined this falls under a global Institutional Review Board (IRB) approval to use these data sets for clinical improvements in treatment planning without a specific IRB approval.
Acknowledgments
The authors would like to thank Dr Zhao jingxin for generously providing consultation and software support for this study. We would also like to thank Philips Medical Systems for the Auto-Planning research license.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to acknowledge the financial support for this work from Natural Science Foundation of Jiangxi Province Youth Fund Project (20202BABL211015) and Science and technology research project of Jiangxi provincial department of education (GJJ190136) and Wenzhou Municipal Science and Technology Bureau (Y20180760).