
Abstract
Braided suture made with different materials and sizes is commonly used in many surgical interventions. Their key properties include tensile strength during tightening, knot security, surface morphology, knot slippage, and behavior during healing period. We have developed different testing procedures to measure these properties, but selection of suture should be brought under simultaneous considerations of all preferred properties related to surgical interventions and surgeon requirement.
In this study, we propose a new approach for appreciation of surgeon satisfaction by using global quality index corresponding to simultaneous satisfaction of several suture properties such as organoleptic and mechanical properties. A global quality index was developed by using desirability functions. A statistical survey based on the evaluation of suture qualities by Tunisian surgeons allowed the determination of surgeon's requirement, weights, and objectives of individual desirability functions corresponding to each suture property. Braided sutures have been submitted to different developed tests for the evaluation of suture properties during healing and tying. The obtained results are converted to individual desirability index in order to evaluate satisfaction degree of each suture property. Finally, geometric and arithmetic mean aggregation are used to determine the global quality by attributing relative weight to each individual satisfaction degree. Global quality index of polyamide-braided sutures fabricated under different braiding conditions was determined. Obtained results allow the identification of optimal suture for specific surgical interventions.
Keywords
Introduction
Braided suture is commonly used in many surgical interventions. Several suture materials and sizes are available for surgical procedures [1]. However, it is essential for surgeons to be aware of the nature of suture material, the biologic processes of healing, and the interaction of the suture material with the surrounding tissues. This is a critical issue because surgeon must ensure that a suture will retain its strength and keep wound edges together during healing process [2,3]. In fact, skin-severed edges should be secured against each other to close any dead space between wound edges. However, excessive tightening could lead to suture breakage at the knot, and leave an unpleasant track scar [3]. Therefore, an optimal tightness must be reached to prevent suture failure by untying or breaking and to obtain an aesthetic look with no unpleasant track scars [2–4]. The handling characteristics of suture include pliability and suture friction coefficient. Sutures with a high coefficient of friction are more difficult to pass through tissue because of tissue drag and cause a greater degree of tissue injury. However, these sutures are easier to handle and better for knot tying. Sutures key properties include tensile strength (TS) during the critical wound healing period, knot security (KS), knot slippage, ease of sterilization, foreign body response, and handling characteristics [1,4]. Therefore, critical material properties, suture design, and optimal tightening force should be determined to insure secure and aesthetic wound closure.
Existing methods used to evaluate suture performances have been limited to straight pull and knot pull strength (KPS) [5], KS, foreign body response to sutures, wound infection, and absorption rate. Today, there are no available standards for theses tests, but many testing procedures developed to measure these properties are described in literature [6–12]. Given the confirmed dependency of suture performance on test conditions, Heward et al. [10] recommended the development of standardized test methods to provide a common platform to compare sutures. Hong et al. [5] and Tomia et al. [6] developed test methods to measure in vitro suture characteristics including bending stiffness and friction coefficient. We have developed in previous works new tests to measure knot slippage ratio (SR) and percentage of deformation recovery (DR) of a given suture [13]. However, selection of appropriate suture should be brought under consideration of all preferred properties related to surgical interventions and the requirement degree of surgeons.
When choosing suture, there is no ideal product, but a compromise permitting to best satisfy different points of view and desires of surgeons for each surgical intervention type has to be found. In fact, surgeon's satisfaction is a multi-criteria phenomenon that requires satisfaction in the same time of a set of qualities needed during wound healing and suture tying. In this study, we propose a new approach in order to estimate the surgeon's satisfaction using global quality index (GQI). The desirability functions are used for developing this index. Modeling surgeon's satisfaction allows to manufacture the best choice of suture-manufacturing conditions when several points of view, often contradictory, must be taken into account. The impact of braiding conditions on GQI of suture having similar sizes has been also investigated.
Materials and methods
Suture manufacturing
Manufactured braided sutures conditions.

Determination of suture properties
The developed suture GQI is a result of different components related to different suture properties: bending rigidity (BR), friction coefficient difference (FCD), lateral deformation (LD), TS, KPS, KS, percentage of DR, SR, and knot efficiency (KE). These characteristics were measured according to developed tests presented in previous works [13] and represent the database inputs. All tests were carried in a controlled environment of 21 ± 1 ℃ temperature and 65% ± 2% relative humidity according to ASTM D1776-04 [14]. Ten specimens were tested in each test type. A traction machine (dynamometer LLOYD, England) with a constant extension rate was used for tensile tests according to ASTM D76-99 standard test method [15].
Suture diameter
We measured the suture diameter according United States Pharmacopeia (USP) convention that attributes for each USP number a corresponding suture diameter interval. So, USP32-NF27 S2 < 861 > method described in USP32-NF27 S2 monograph are used for nonabsorbable sutures. A deadweight mechanical thickness gauge (SODEMAT- France), with grading precision of 0.02 mm divisions was used.
TS and KPS
In order to determine suture resistance from doctor's side, we have submitted suture to TS and KPS tests. Tests adopted from Instron® method and recommended by USP were used [16] with a strain rate of 300 mm/min and 150 mm initial gauge length [16] (Figure 1). A flat square knot with two throws was used.
Tensile tests from the doctor side. (a) Straight pull test and (b) knot pull test.
Suture KE
It is defined by loss percentage of TS, as a result of tying a secure knot. It is obtained from the ratio of TS and KPS suture (equation (1)).

Suture FCD (
)
The test method that closely simulates surgical knot tying is the twist method. In our tests, we adopted the method developed by Gupta [17] to simulate friction between threads warped together in the knot. Two test weights (0.2 N) are attached to each end of the sutures warped together and placed between different pulleys as shown in Figure 2(a). Upper sutures ends undergo a vertical displacement of 30 mm at a rate of 12.7 mm/min. Sutures displacement between each other produce a tension (T) recorded by the traction machine (Figure 2(b)). Different sutures were compared in terms of average ( (a) Experimental device used to measure friction coefficient by twist method and (b) recorded tension as function of yarns displacement.

Suture BR
Suture BR was measured by using the loop test method developed by Morton and Hearle [18]. The two ends of the specimen (10 cm of length) were clamped together. Then, a specimen is suspended and loaded by a rider, as shown in Figure 3. The BR was obtained from equation (3) developed by Peirce to determine fiber BR [18].
Bending rigidity device.

Suture LD caused by transversal pressure
In this study, suture compressibility was evaluated by the measurement of LD. The difference between measured diameter under pressure of 4.2 kPa and suture diameter measured by an image-processing procedure is then determined. This difference divided by suture diameter measured by image processing is considered as the LD caused by transversal pressure.
Suture KS
KS is defined as suture resistance during healing to break and untying. We have used test methods to determine tensile performances of knotted suture from patient side developed in our previous works [13]. Sutures are tied around two cylindrical sponges under a tying force of T0 during 3 s at 200 mm/min strain rate to simulate roughly surgeon's tying force. The tied suture is subjected to tensile test until failure (Figure 4). The distance between bottom of upper grip and the pin was set at 10 mm and the strain rate was 12.7 mm/min.
Experimental device for knot security measurement.
SR
SR expresses the amount of slipped materials from patient side. It was developed in previous works [13]. It is given by equation (4). EKP is the extension of the knotted suture from the patient side. ENKP is the extension of unknotted suture from the patient side. L is the specimen length equal to 145.7 mm. Fp is applied force from patient side chosen equal to 20 N. The amount of slipped length upon tying (AST) is obtained by the difference between the extension of the knotted suture from the doctor side and the extension of unknotted suture from the doctor side at an applied force of 10 N. All extensions are expressed in millimeter.

The percentage of DR
In order to determine the percentage of DR after wound healing, suture is subjected to a creep test in the traction direction by using a 12.7 mm/min strain rate. The hold time was set to 60 min and the load limit was set to 60% of KS. The percentage of DR was calculated according to equation (5) where EM is the maximal extension in mm, and EF the final extension in mm.

Methodology of GQI development
To develop the GQI of suture, we have used the design process presented in Figure 5.
Design process of the global quality index.
Definition of individual desirability functions
Appreciation of surgeon's satisfaction degree of each property requires the determination of individual desirability index “d
i
.” This index varies between 0, corresponding to a null satisfaction, and 1 corresponding to a total satisfaction. Individual desirability functions of Derringer and Swich were used [19–21]. Desirability functions are classified into three types: desirability function to minimize (Figure 6), desirability function to maximize (Figure 7), and desirability function to reach a property target value (Figure 8). When a property “Y
i
” has to be minimized, we use the desirability function shown in Figure 6, where “d
i
” is calculated according to equation (6). We use equation (7) when a property has to be maximized (Figure 7). If a property has to reach target value “Ytarget” as in the case of diameter, we use the desirability function shown in Figure 8, where “d
i
” is calculated according to equation (8).
Desirability function to minimize. Desirability function to maximize. Function of desirability to reach a target value.





The desirability functions depend on two factors: the surgeon's requirement degree “r i ” and satisfaction limits for each property: “Ymin,”“Ymax,” and “Ytarget.” The increase of surgeon's requirement degree “r i ” is proportional to the requirement increase. We consider that if r i = 1, surgeon's requirement degree is medium. On the other hand, if r i > 1, we consider that surgeon's requirement degree is too high, and finally when r i < 1, we can consider that surgeon's requirement is too low. In the case of desirability function to reach a target value (equation (8), Figure 8), we can have two different requirement levels: “r i ” level when measured value is lower than target value “Ytarget,” and a “t i ” level when measured value is higher than target value.
By calculating satisfaction degree (d i ) for each property, the initial database of suture properties, was transformed to a new database in which the outputs are represented by the individual indexes of each property.
Determination of objectives, weights, and surgeon's requirement degree
We have conducted a survey in seven Tunisian hospitals. Seventy-two surgeons having seven different specialty are asked to response to quiz about suture quality and encountered suture defect. In this study, we have only used statistical results related to response to the two following questions (a) and (b). Surgeons are invited to note on levels scale their appreciation from 0 to 10 for each suture quality.
Note the minimum accepted level of suture quality. What is the importance degree of each quality.
The weight and the surgeon's requirement degree of each property were determined using noted values on this scale levels. The average recorded values of the weight and the surgeon's requirement degree of each quality in different surgery interventions are determined by equation (9). Then, average recorded values are converted to weight and surgeon's requirement degree for each properties by using, respectively, equations (10) and (11).



GQI definition
After having corresponded to every property an individual desirability function, we have combined these individual desirability functions in order to obtain combined desirability, called GQI.
This index is obtained by multi-criteria decision analysis. We have organized properties by clustering them under high-level and low-level objective hierarchy. Geometric mean aggregation defined in equation (12) and arithmetic mean aggregation presented in equation (13) are used to combine individual desirability (di) on partial global satisfaction degree (PGSD) according to suture performances types. The weight of each property is taken into account in determination of the PGSD. Finally, different PGSDs are grouped into one global satisfaction degree designed by GQI by using Derringen and Suich desirability function [19–21] (equation 12) and with according relative weight, “w
i
= 1”, to each PGSD.


The GQI varies between 0 and 1, where the value 0 corresponds to a null satisfaction, and the value 1 corresponds to a full satisfaction for the global suture quality. By defining this GQI, the initial properties database is transformed to a new one, with a unique output represented by “GQI.” Finally using MATLAB R2014-a, we have developed a program permitting the calculation of GQI from measured values of property in each studied surgery intervention.
Results and discussion
Braided sutures are generally manufactured for many different surgeries, but suture performances requirements have to be related to future suture application. Particularly, mechanical properties determine how it will perform, and ultimately whether it will be accepted for its specific use. Suture success is affected by achievement of several mechanical properties. It is a multi-criteria phenomenon that requires the simultaneously satisfaction of a lot of properties.
In this study, we purpose to transform all measured performances in only one parameter permitting to estimate the surgeon's satisfaction by means of desirability functions.
Objectives of individual desirability functions
To determine the adequate desirability function for each property, we have to establish an objective, surgeon's requirement degree, and weight of each property. However, there are a diversity of surgeon's point of views due to diversity of surgery conditions. For this reason, we have conducted the survey in Tunisian hospitals and asked surgeons to give us an appreciation of main suture qualities. We have defined main qualities after literature examination [5,7,10,13,22–28]. In Table 2, we present summary of appreciated qualities and measured properties. Desirability functions related to each property were determined and appreciated qualities were correlated to measured properties as follows:
Suture size: suture having small diameter is generally appreciated by the surgeon, but suture diameter has to be in the intervals defined the USP. In fact, surgeon looks for the smallest diameter belonging intervals of the USP number. Tissue drag: A good slide is preferred for easy tissue penetration and minimal tissue trauma. FCD of suture is used to evaluate how easy suture penetrates tissue. Suture slide between surgeon's hands: For easy handling and reliable suture, suture has to gently slip on surgeon's hands. This property is estimated by the measurement of FCD. Sutures slippage between each other: Sutures has to slide against each other during tying. This property is evaluated by FCD. Flexibility: It expresses how the suture is bent. It is evaluated by measuring the BR. Pliability: It expresses how suture is compressed. Suture easily compressed is difficult to tie and has a nonuniform diameter. It is evaluated by LD. Resistance of suture during tying: It is a fundamental property because the suture has to be resistant during tying. It is estimated by TS and KPS. Limit values are defined by USP for each USP number. Knot packaging: It is defined by the stability of knot during tying without defect. It is evaluated by KE. Suture resistance during healing: knotted suture has to resist to defect by sliding or breaking during healing process. It is evaluated by KS. Wound edges adjustment just after implantation: knot has to be stable without slippage in order to have a stable loop size. It is appreciated by SR. Wound edge adjustment after healing: Suture loop has to recover its initial deformation after edema disappearing. It is determined by percentage of recovered deformation. No dead space: dead space is formed between non-adjusted wound edges. It is appreciated by SR. Correlation between estimated qualities and measured properties.

Weight and the surgeon's requirement degrees of each quality
Weights and surgeon's satisfaction degrees corresponding to measured proprieties in different surgical interventions.

Note: TS: tensile strength; KPS: knot pull strength; KE: knot efficiency; FCD: friction coefficient difference; BR: bending rigidity; LD: lateral deformation; KS: knot security; SR: slippage ratio; RD: recovery deformation.
Obtained results confirmed that surgeon's choice is related to type of surgical intervention. In fact, in every intervention, surgeon's preferences are influenced by operation difficulty and post healing exigency. From Table 3, it can be seen that, KS during healing and KE during tying are essential performances in all surgery. They are the most important performances in the case of cardiovascular surgery. LD properties have the lowest values in all surgery. For general surgery, percentage of recovered deformation is the most important properties because dermic suture has to keep wound edges adjusted after healing to obtain esthetic closure without track scar. In the case of urology surgery, knot performances during tying and percentages of DR are the main properties. Thus, knot has to be secure inhibiting to suture defect because defect may lead to remaking the intervention.
Limit values of individual desirability functions
There is no perfect suture for all surgical intervention. For this reason, the acceptance limits for each studied properties depend on surgery type. Consequently, surgeon has to define his preferred limits for the future desired surgical intervention. Suture manufacturer is also invited to determine the required limits according to their customer's desires.
Limits values correspond to tested properties at different suture size.

Note: USP: United States Pharmacopeia; TS: tensile strength; KPS: knot pull strength; KE: knot efficiency; FCD: friction coefficient difference; BR: bending rigidity; LD: lateral deformation; KS: knot security; SR: slippage ratio; RD: recovery deformation.
For diameter and KPS, the USP requirements corresponded to each USP number are respected. For SR, maximum and target values are chosen respectively equal to 4% and 2%. SR has not to exceed 4% (6 mm sliding materials) because according to literature, knot ear length is at maximum equal to 3 mm [8,29–31]. So, slippage of material higher than 6 mm (3 mm from each ear) involves suture defect. SR lower than 2% is considered as perfect (3-mm sliding materials) [32]. In fact, many researchers recommended a minimal knot ear length equal to 2 mm [32] and not exceed in preference 3 mm [8]. KE higher than 60% is considered to be ideal because in the most cases KE of square knot is near 50% [33]. KS, is extremely related to the type of surgery, but we did not found in literature the exact limit values because of diversity of used methods for measurement KS [8,23,32,34–36]. Chu et al. [1] reported that in classical conditions, the maximum force applied to suture during healing is 20 N. Thus, for all suture diameters, we used a minimum value “Ymin” of KS equal to 20 N for all surgery. A minimum recovery deformation is chosen equal to 50% and a value of 70% is considered as ideal. For properties related to suture performances during tying (BR, LD, and FCD), limit values are chosen as restricted as possible for studied sutures because of lack of preferred values related to tying performances in literature.
Development of GQI
The main objective of this study is the development of GQI that permits to compare overall sutures quality of and determine best ones. This index could simplify the surgeon choice of preferred suture. Furthermore, appreciation of GQI facilitates manufacturer decision when choosing optimum suture manufacturing conditions.
Calculation of GQI that includes all requirements imposed on suture properties is described in the flowchart presented in Figure 9. The program principle encloses, in first step, the calculation of individual satisfaction degree “di” of each suture property by using individual desirability functions defined in Table 2 and using limits and surgeon's requirement degrees presented, respectively, in Table 4 and Table 3. In the second step, individual satisfaction degrees are combined together by type. There are three types of suture properties: fundamental properties having values required by USP, suture-tying properties, and properties related to postimplantation performances (Table 2). All fundamental properties have to be non-null. So, geometric mean aggregation is used to determine fundamental PGSD (F-PGSD) (equation (14)). Consequently, if individual satisfaction degree of diameter, TS or KPS is equal to zero, F-PGSD will be zero. For determination of PGSD of tying properties (T-PGSD) and PGSD during healing (H-PGSD), we have used arithmetic mean aggregation. So equations (15) and (16) are respectively used for determination T-PGSD and H-PGSD. In fact, these types of properties are preferred but not fundamental. So, for example, if FCD exceeds maximum limit, suture is accepted but global quality degree will have non-null low value.
Flowchart of global quality index design.


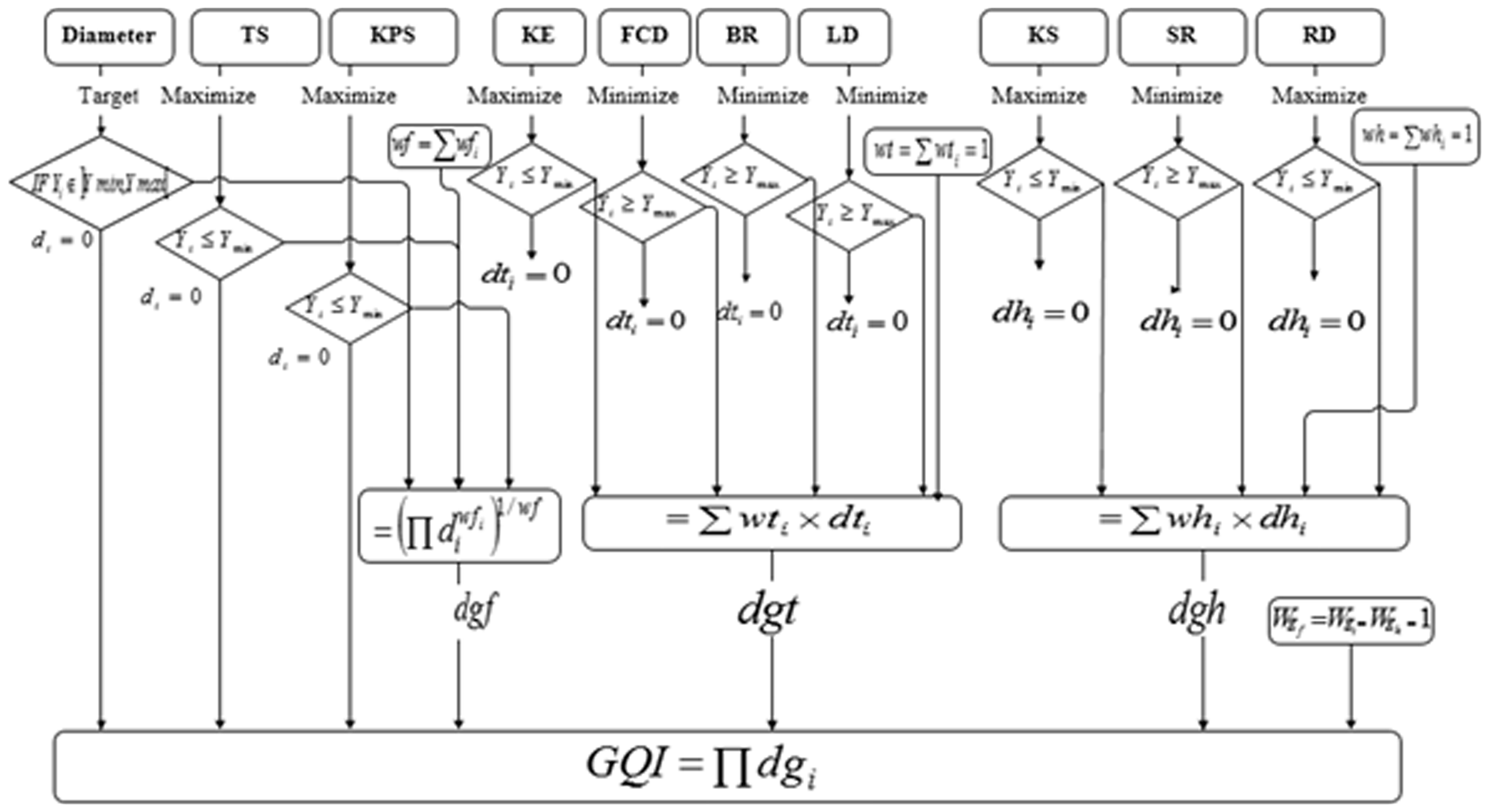
Finally, Derringen and Suich global desirability function is used to calculate GQI. If one type of PGSD is null, the overall desirability is equal to zero and suture is rejected. All PGSDs are considered having the same weight in GQI. Thus, the compromise between the different properties is better when GQI increases. It is considered as perfect when GQI is equal to 1.
Investigation of GQI of braided sutures
Braided sutures properties.
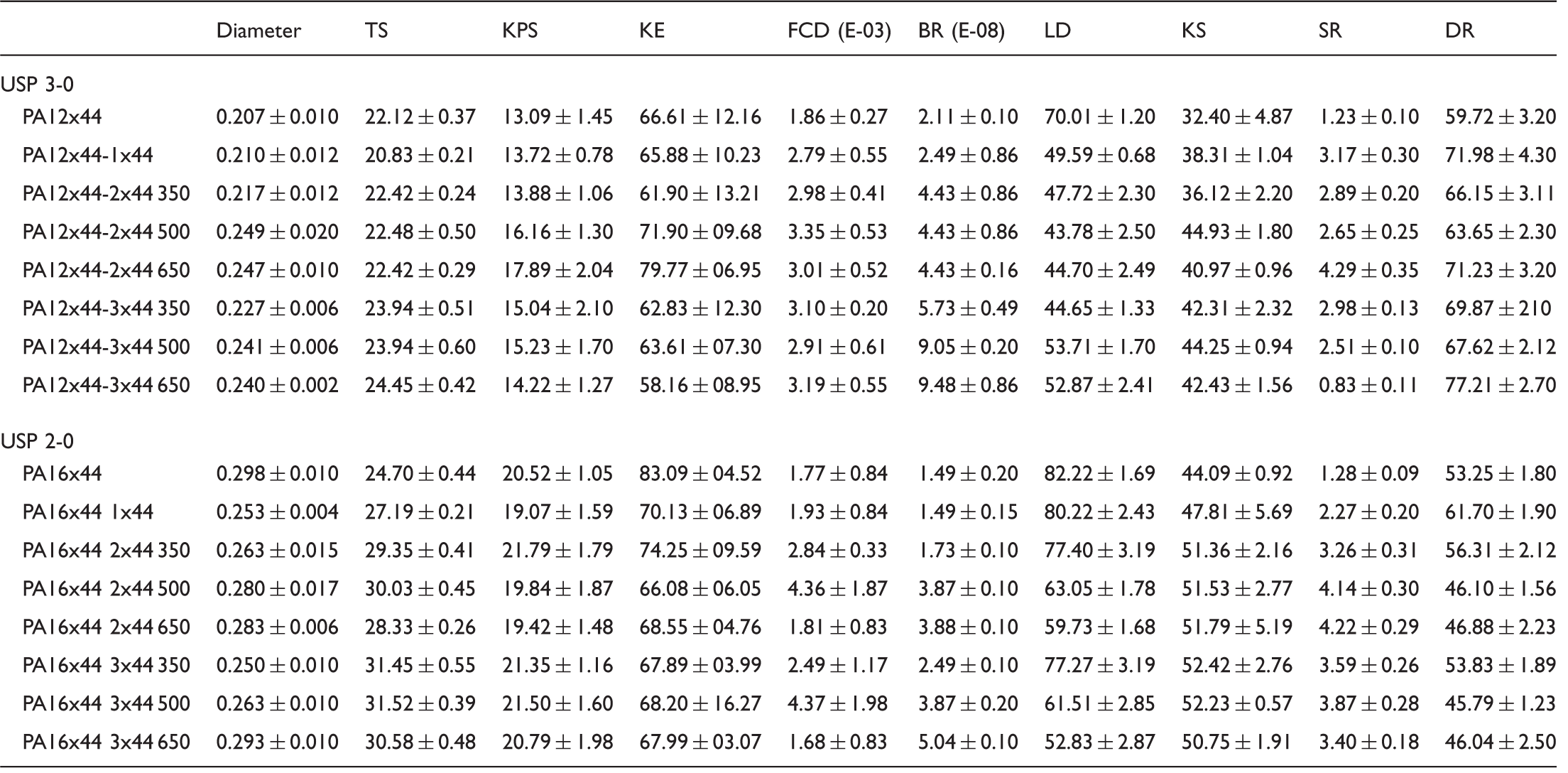
Note: FCD: friction coefficient difference; USP: United States Pharmacopeia; TS: tensile strength; KPS: knot pull strength; KE: knot efficiency; BR: bending rigidity; LD: lateral deformation; KS: knot security; SR: slippage ratio; DR: deformation recovery.
GQI allows an easy appreciation of suture quality and guides suture choice. GQI of braided polyamide sutures having USP 2-0 and USP 3-0 were determined. Results are presented respectively in Figures 10 and 11. Figure 10 shows an increase of GQI when adding one yarn as braid core yarn in the braided suture composed of 16 sheath yarns (USP 2-0). However, adding braid core to suture braided with 12 sheath yarns (Figure 11) or further adding of yarns to braid core in the braided suture of 16 sheath yarns has reduced GQI. Although, adding of braid core ameliorates suture resistance from both doctor's and patient's side and percentage of DR, but involves production of suture having high diameter, rigid structure, rough surface, and exhibit low KE and high SR (Table 5). This can be explained by crushing of braid core yarns in compacted braided structure.
Global quality index of braided suture having USP 2-0 fabricated in different conditions. Global quality index of braided suture having USP 3-0 fabricated in different conditions.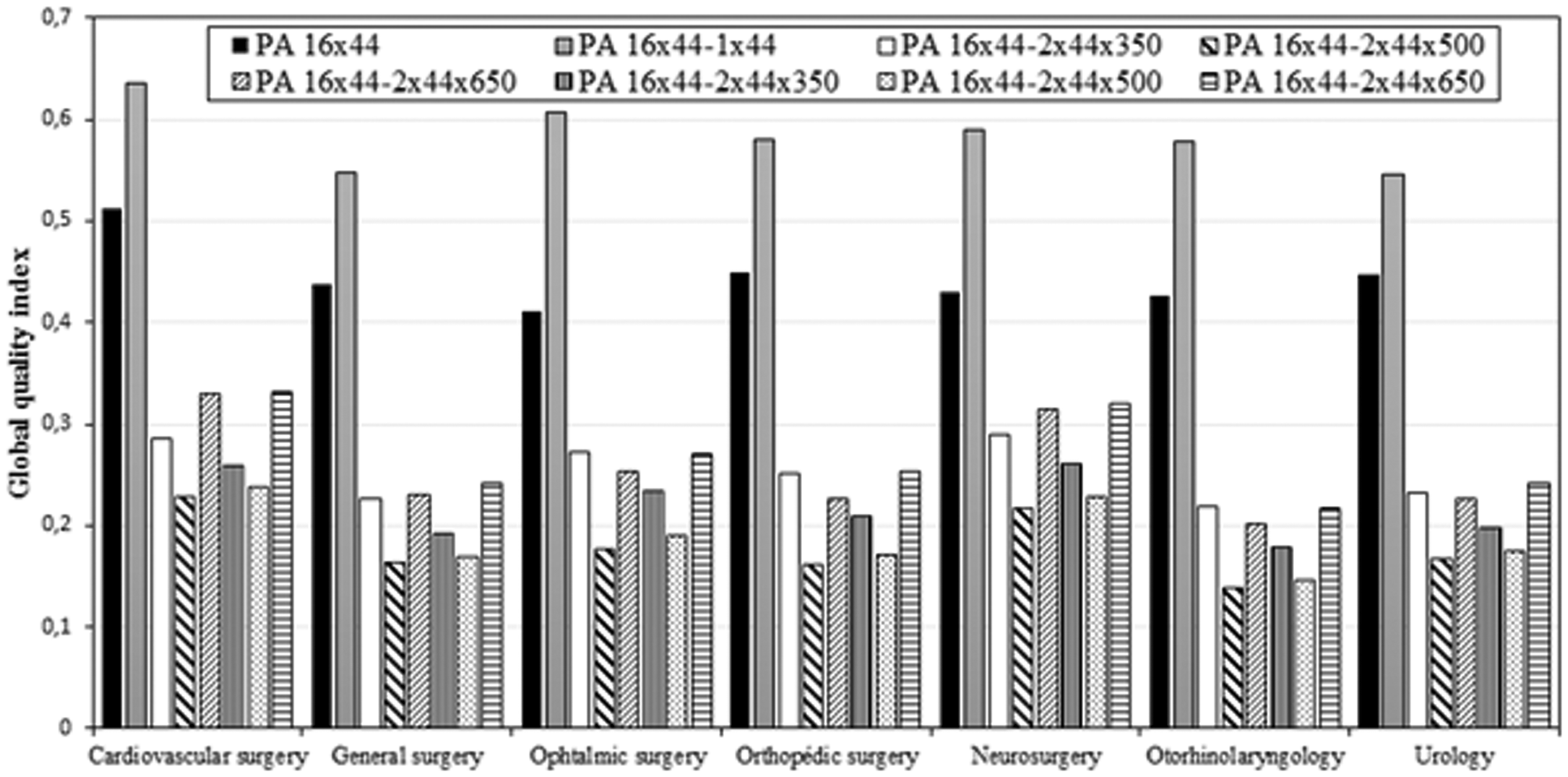

Increase of twist value of cabled core leads to decrease of GQI especially in the case of braided suture having USP 3-0. An improvement of GQI is obtained in the case of braided suture (USP 2-0) with cabled core twisted at 650 twist/m. This result is due to the improvement of filament mechanical properties associated to twisting.
Conclusion
Suture key properties include many mechanical properties affecting suture success. Suture success is a multi-criteria phenomenon that requires simultaneous satisfaction of different qualities needed during wound healing and suture tying. A compromise permitting to best satisfy different desires related to different surgery interventions based on GQI obtained by desirability functions was defined in this study.
Evaluation of suture qualities by Tunisian surgeons has been performed in order to determine surgeon's requirement degree, weight, and objectives of individual desirability functions for each suture property. Measured properties have been transformed to individual satisfaction degree and global desirability index was determined for the appreciation of surgeon's satisfaction.
This index is useful to regroup the different properties affecting suture quality in only one index representing the global quality of suture varying between 0 and 1. It helps surgeon to choose the best suture for each surgical intervention. In order to be useful by suture manufacturers, GQI should be presented in graphical curves as a function of suture manufacturing conditions. The presented methodology in this paper is limited to the development of GQI. The development of mathematical model permitting the prediction of surgeon's satisfaction using fuzzy logic or neural network will be investigated in other future study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.