
Abstract
Ethical climate is one of the important factors in the working climate of the hospital. Considering the difference in the Ethical climate in different departments of the hospital and the importance of the ethical climate in the delivery ward, this study aimed to assess the characteristics of hospital ethical climate in delivery ward of educational hospitals in southeast Iran. This descriptive and multi-center study was conducted from 2020 to 2021 in educational hospitals in southeast Iran. Two hundred forty midwives working in delivery wards, midwifery instructors, and midwifery students were included in the study by census method. Data collection tools included a demographic information form, Olson's Hospital Ethical Climate Survey, completed using the self-report method. The mean ethical climate in the midwifery group (3.82 ± 0.63 out of 5) was higher than in the instructors’ and students’ groups. The lowest mean score obtained from the ethical climate questionnaire of participants was associated with the inability to use their experiences in the delivery ward. The lowest mean of ethical climate from the midwives’ point of view is the Physicians’ dimension and the patient's dimension from the instructors’ point of view. The highest mean score belonged to the ethical climate of the supervisors. According to the results of the present study, it is suggested to implement protective laws to support the higher independence of midwives to improve the ethical climates by using their experiences in the delivery department.
Introduction
Ethical climate can be defined as a set of behaviors, emotions and impressions characteristic for a given organization (Victor & Cullen, 1988). In other words, an ethical climate refers to shared perceptions between members of an organization or part of an organization as to “what constitutes right behavior” and arises when “members believe that certain forms of ethical reasoning or behavior are expected standards or norms for decision-making within the firm” (Martin & Cullen, 2006). The ethical climate of the work environment is the result of organizational policies, procedures, and practices concerning ethical issues. It reflects the regulations and instructions of the organization and their relationship with the ethical principles that affect employee attitudes and determine employee behavior (Olson, 1995).
Ethical climate is defined by (Olson, 1998) as “an organizational variable that can be managed and changed in order to improve the workplace environment. It consists of perceptions of organizational practices and conditions that facilitate the discussion and resolution of difficult patient care issues, and provides the context for ethical decision-making in the clinical setting” (Olson, 1998, p. 345). The ethical climate of a hospital can impact midwives’ and nurses’ approach regarding ethical decision-making or ethical dilemmas in the workplace (Jiang et al., 2021) A negative ethical climate can lead to reduced motivation, job performance, and job satisfaction (Lemmenes et al., 2018; Özden et al., 2019; Saygili et al., 2020). It is related to the provision of health services and patient safety (Aly et al., 2020) An improved ethical climate helps to reduce medical errors (Hwang & Park, 2014; Ghasemi et al., 2022) and it has been found to influence job satisfaction, perceived workplace support and commitment (Abou Hashish, 2017) and intent to leave a position. (Barr, 2021) Also, a researcher shows that the perception of ethical work climate directly influences people's decision-making when faced with difficult issues (Shacklock et al., 2013) and it has also been found to be related to moral distress (Abdeen & Atia, 2020). In addition to significant impacts on health care workers and health service delivery, ethical climate itself is influenced by a complex range of factors, including organizational culture, leadership, policies, procedures, and team structure (Koskenvuori et al., 2019). On the other hand midwives experienced various ethical dilemmas while working in the delivery ward (Türken & Çalım, 2022) For these reasons, the ethical climate of the delivery ward is very important for midwives to provide quality care.
The level of ethical climate is largely determined by the relationships between nurses and colleagues, patients, physicians, managers, and the hospital (Olson, 1998). The Hospital Ethical Climate Survey (HECS) is a questionnaire consisting of five subscales including relationship with peers, patients, managers, hospital, and physicians. The subscales of colleagues and physicians had the highest and lowest scores, respectively (Olson, 1998). On the other hand, in the study of Pauly et al., hospital subscales had the highest and lowest ratings, respectively (Pauly et al., 2009). In contrast, in the study of Shafipour et al., the highest score of ethical climate belonged to managers/ factor, while the minimum score was related to physicians (Shafipour et al., 2016). Studies have reported different results regarding ethical climate scales. These contradictions may indicate the influence of environmental characteristics, such as the nature of the hospital (private or public), employment status, and type of unit, which are the foundations of ethical climate (Ghorbani et al., 2014).
Despite numerous studies on the ethical climate of different occupations, according to our research, few studies have been conducted on the midwifery profession, especially in the delivery ward, or in other words, the midwifery emergency department. Turkan et al. and Dziurka et al. conducted a study to investigate the ethical climate of midwives, which was related to other departments (Turkan Karaca et al., 2018; Dziurka et al., 2022). The present study aimed to assess the characteristics of hospital ethical climate in the delivery ward of educational hospitals in southeast Iran. It is possible to improve midwifery care by improving the ethical climate in the delivery ward of educational hospitals in southeast Iran using the results of the present study.
Research Method
This descriptive and multi-center study was conducted from 2020 to 2021. The sampling method was census method. The sample of this study included 129 midwives working in the delivery department, eight midwifery instructors, and 103 midwifery students from selected educational hospitals of Kerman medical universities. Kerman province is located in southeast Iran. The province has four universities of medical sciences, each with a delivery ward. The four delivery wards of the medical universities of Kerman, Rafsanjan, Bam, and Jiroft were evaluated. Midwifery staff and instructors with at least an associate's degree and at least 1 year of work experience in the maternity ward were included. Bachelor's students in their sixth semester were also eligible to enter the study. Exclusion criteria were unwillingness to participate in the study.
Olson's HECS and demographic information form were used to collect the data. The demographic information form included age, marital status, education level, work experience, hours of work per week, employment status, work shift, local status, and dormitory or non-dormitory (for students).
This study is approved by the Medical Ethics Committee of Shahrood University of Medical Sciences with code IR.SHMU.REC.1397.209. Data were provided by the participants in a self-reported manner in the treatment centers of the research setting. After oral and written information about the study was provided and informed written consent was obtained, the participants were provided with a questionnaire to fill out. SPSS software version 25 was used to evaluate the data. Descriptive statistical methods (frequency, percentage, mean, standard deviation), and ANOVA was used.
Findings
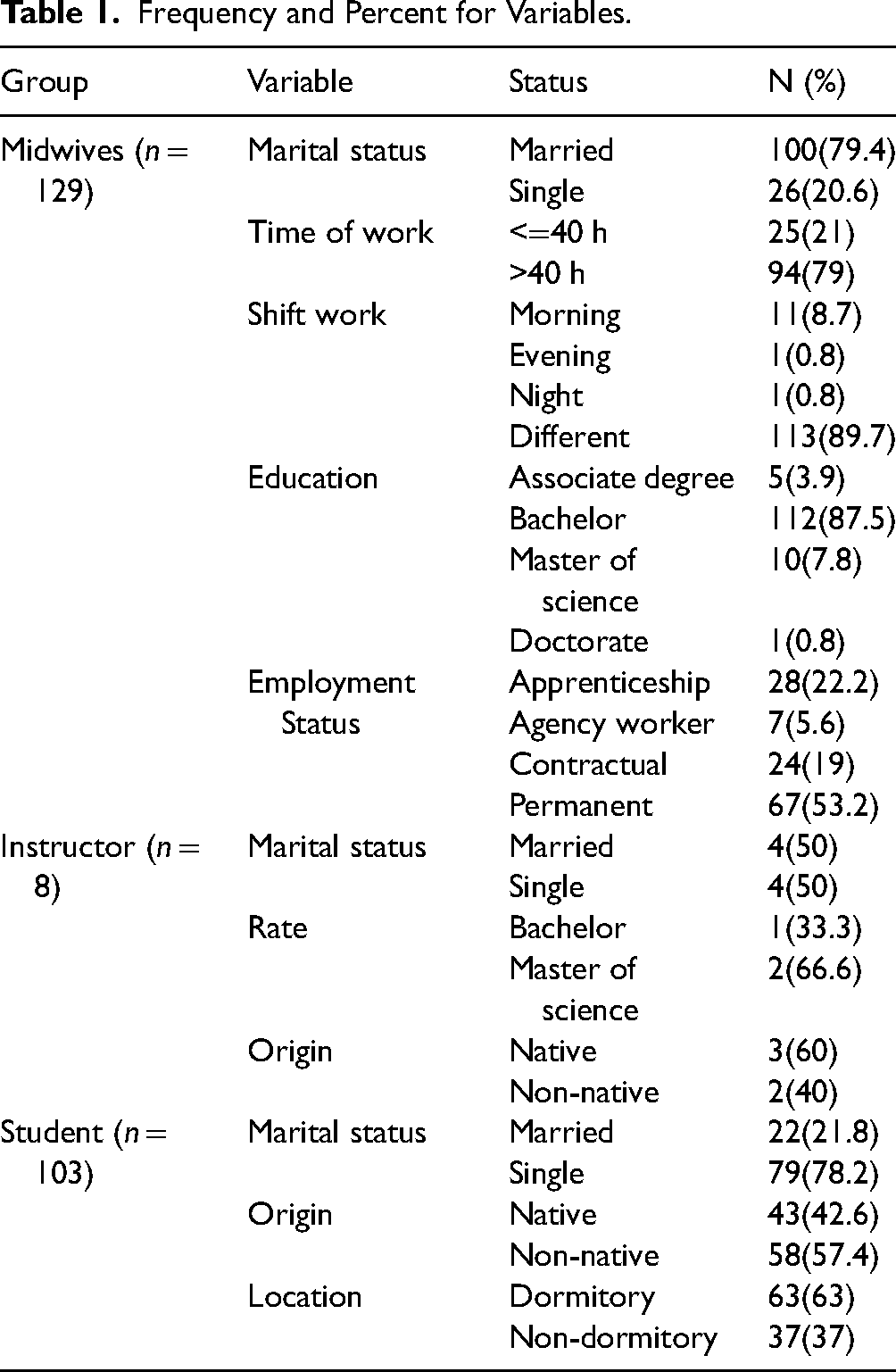
The mean age of participants, including midwives, instructors, and students, was 34.04 ± 8.01, 28.85 ± 5.17, and 22.38 ± 2.37, respectively (Table 1). The mean score of the ethical climate in midwives out of 5 was higher (3.82 ± 0.63) than instructors (3.28 ± 0.37) and students (3.53 ± 0.57). There is a significant difference in the dimensions of ethical climate between the three groups, except for the ethical climate of physicians. (Table 2)
Frequency and Percent for Variables.
The Central Tendency and Dispersion of Variables.
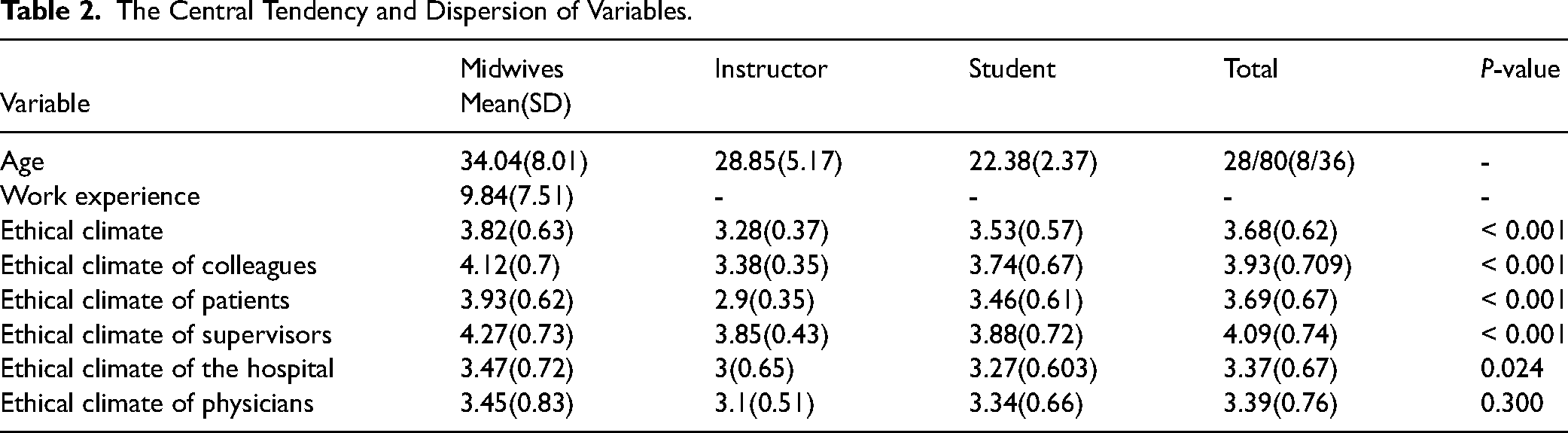
From the point of view of midwives, relationship with physicians, from the point of view of educators, patient–midwife relationship has the lowest average ethical climate. (Table 2) Based on the results, supervisor's support for midwives in clinical decisions and respectability of supervisors are more than other items in view of all three groups.
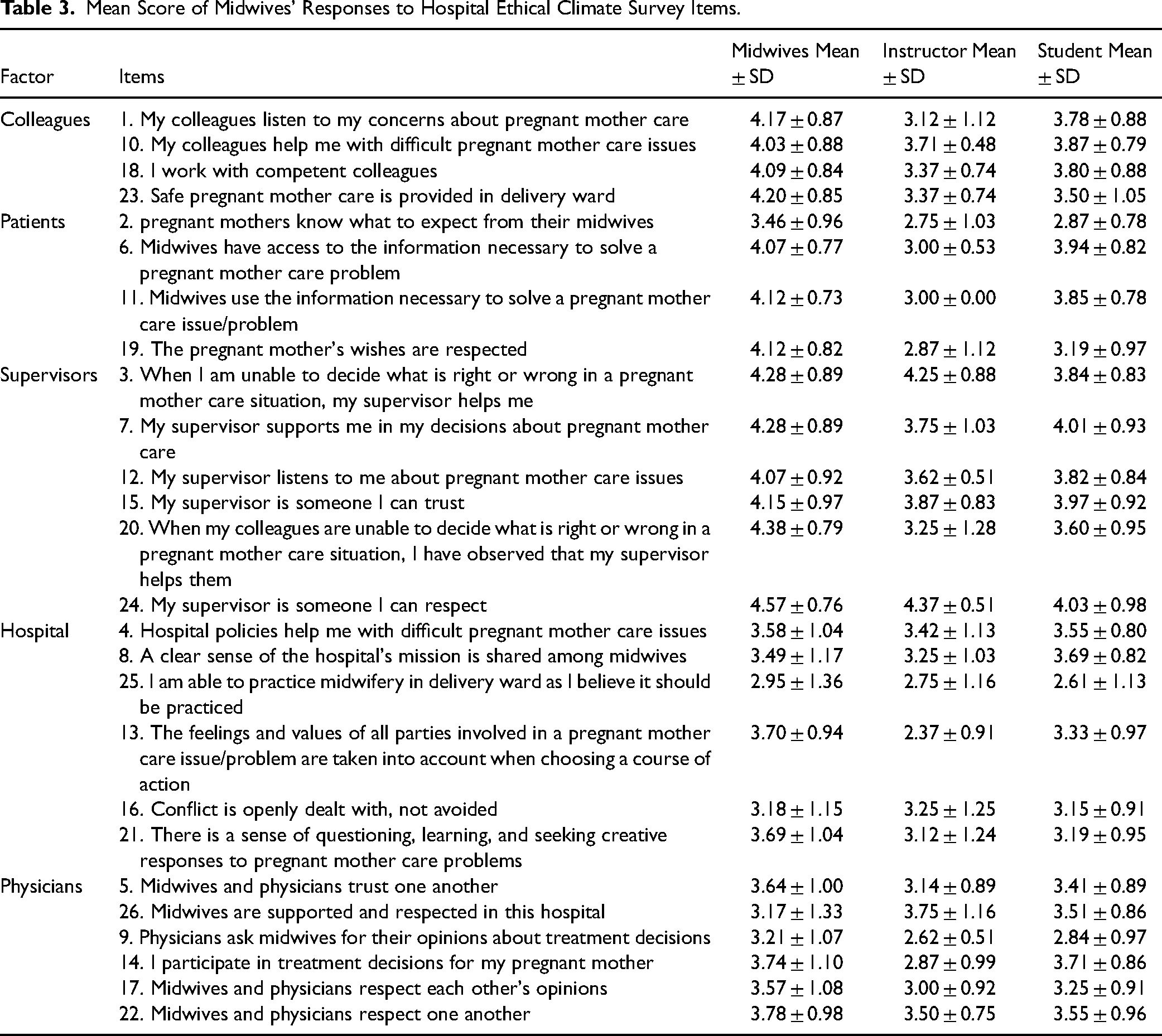
Considering that the lowest mean score obtained from the ethical climate questionnaire in the group of instructors out of 5, related to the cases of mothers’ awareness of expectations from midwives (2.75 ± 1.03), access to information needed to solve problems related to maternal care pregnant (3 ± 0.53), midwives use of necessary information to solve problems related to the care of pregnant mothers (3 ± 0.00), and respect the wishes of pregnant mothers (2.87 ± 1.12). It can be concluded that the patient–midwife relationship in the delivery ward is weak.
The lowest mean score obtained from the ethical climate questionnaire in three groups of participants was related to item 25, “I cannot use my midwifery experience as I should in the delivery department” and also items 9, 13, 14. In other words, according to all three groups, consultation with midwives in treatment matters is less than expected (Table 3)
Mean Score of Midwives’ Responses to Hospital Ethical Climate Survey Items.
Discussion
The present study aimed to assess the characteristics of hospital ethical climate in delivery ward of educational hospitals in southeast Iran. The midwives reported a more positive ethical climate than the instructors and students, which seems to be due to the greater compliance with and higher awareness of governing rules and regulations among the midwives. However, the ethical climate dimension of supervisors was the most positive among the studied participants, with all midwives reporting that they received respect and support from supervisors.
Studies by (Ozdoba et al., 2022; Turkan Karaca et al., 2018; Shafipour et al., 2016) and Dziurka et al. are consistent with the results of the present study. Like the present study, these studies reported a same level of organizational and managerial ethical climate from the perspective of midwives and nurses. Studies have indicated that supervisors’ appreciation of their employees and their respect and support for them can affect the ethical climate and job satisfaction of people in the workplace (Özden et al., 2019; Jang & Oh, 2019; Faramarzpour et al., 2021). Supervisors help to create an ethical climate in the workplace by prioritizing ethical values in their relationships with patients and staff and following ethical principles (Ozdoba et al., 2022).
According to the results of the study by (Fazljoo et al., 2014; Khazani et al., 2013) and (Shafipour et al., 2016) and (Faramarzpour et al., 2021), (Dziurka et al., 2022) like this study the ethical climate of physicians received the lowest score. The study by Khosravi et al., 2022 also confirms that from the point of view of midwives cooperation with gynecologists and with interdisciplinary working groups is a concern for midwives. This result can indicate that the atmosphere of cooperation and mutual relations between midwives and gynecologists in Iran is at a low level, and among the reasons for this, one can mention the doctor-centeredness and their superior prestige. Joolai et al. (Joolaee et al., 2013) also mentioned such issues as the doctor-centered systems in hospitals, lack of adequate staff awareness of ethical issues. It should be noted that considering the importance of the midwifery profession and the effective role of midwives in making physiologic childbirth pleasant and as a result increasing fertility, creating a positive atmosphere of cooperation and mutual relations between midwives and gynecologists seems necessary and requires careful consideration.
Patient ethical climate includes the pregnant mothers’ awareness of care, service providers’ access to information needed to solve problems related to mother care, the use of essential information to solve problems related to care, and respect for mothers’ demands. Respect for mothers’ demands had the lowest mean compared to the means of other ethical climates from the viewpoint of midwifery instructors, which is in line with the results of the study by Jahan Tigh et al. (Jahantigh et al., 2015). This result can be attributed to the difference between holistic and biomedical perspectives in the treatment process of instructors and staff, with instructors showing a more client-centered perspective in the treatment process due to the nature of their academic role in the clinical environment. It also seems that involving more faculty members and students in different stages of dealing with clients to provide services can increase adherence to codes of ethics.
On the other hand, all studied participants gave the lowest score to the hospital climate, so in their opinion, not being able to properly implement the midwives’ experience led to a relatively negative organizational climate. This means that midwives not able to practice in delivery ward as they believe.
According to midwifery instructors and students, consultation with midwives in medical care is low, which indicates that midwives are not consulted in delivery wards. This is while considering the role and responsibility of midwives in childbirth, the consultation with midwives in the delivery ward should be much more. Researchers also state that there are many obstacles against the implementation of midwives’ decisions in the delivery ward like intrapersonal, contextual, and institutional/organizational factors (Jefford et al., 2010). Other studies have shown that the cooperation of gynecologists and midwives and the participation of midwives in clinical decisions according to scientific protocol and research-based studies can increase the quality of services and reduce the rate of cesarean sections (Lotfi et al., 2014; Downe et al., 2010).
Differences between the dimensions of the tools used to investigate the organizational ethical climate and inaccurate reporting of details on dimensions and statements by studies have led to limitations in comparing the results of similar studies with the present study.
The present study investigated the ethical climate of midwives in the delivery ward of educational hospitals. The results can be used in implementing intervention strategies to promote and improve the organizational climate, especially in the delivery ward.
Conclusion
According to the results of this study and the importance of organizational ethical climate in midwives, it can be suggested that authorities prepare and implement programs to improve the ethical climate of organizations. This can be done by conducting more studies on improving the ethical climate of hospitals. Also, it seems that in order to improve the ethical climate of the organization in the delivery ward of educational hospitals, it is necessary to have laws to protect independence of midwives in order to take advantage of the existing potentials, and involving faculty members and students in different stages of dealing with clients.
Limitations
This study used a self-report questionnaire to collect data, so some people may not have provided accurate answers. The large number of questions in the questionnaire lengthened its implementation time, which may have affected the accuracy of the participants’ answers. Although questionnaires were valid and reliable, the researchers cannot investigate all aspects of these. The small number of samples in each hospital and university led to the use of the census method for sampling.
Footnotes
Acknowledgement
We hereby express our gratitude to midwives working in delivery wards of the medical universities of Kerman, Rafsanjan, Bam and Jiroft. This article is the result of the approved research project number 97196 of Shahroud University of Medical Sciences.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Medical Ethics Committee of Shahrood University of Medical Sciences with the ethics code IR.SHMU.REC.1397.209.