
Abstract
Introduction:
Sexual dysfunction (SD) is a common problem in chronic kidney disease (CKD) and endures in 50% of patients after kidney transplantation (KTx), diminishing patients’ expectations of life after KTx. Unfortunately, SD is often ignored by renal care providers. Research questions as part of a research project among all renal care providers, transplant surgeons’ perspectives were obtained on sexual health care for KTx recipients, including their opinion on who should be accountable for this care. In addition, surgeons’ practice and knowledge regarding SD were evaluated.
Design:
A 39-item questionnaire was sent to all Dutch surgeons and residents specialized in KTx (n = 47).
Results:
Response was 63.8%. None of the respondents discussed SD with their patients, before or after surgery. Most important barrier was that surgeons do not feel accountable for it (73.9%); 91.7% thought this accountability should lie with the nephrologist. Another barrier was insufficient knowledge (39.1%). In 75% of the respondents, (almost) no knowledge regarding SD was present and 87.5% noticed education on SD was insufficient during residence training.
Discussion:
Dutch renal transplant surgeons rarely discuss SD with their patients with CKD, as they do not feel accountable for it; this accountability was appointed to the nephrologist. Knowledge and education regarding SD were found insufficient in enabling surgeons and for some it reflects in barriers toward discussing SD. Results emphasize that accountability for providing sexual health care to patients with CKD should lie elsewhere; however, surgeons could briefly provide information on sexual health after KTx, so unfulfilled expectations may be prevented.
Introduction
Sexual dysfunction (SD) is a common and underestimated problem in both men and women with chronic kidney disease (CKD). 1 Disturbances in sexual function are first noticed in the early phase of kidney failure and deteriorate further as renal function declines. 1,2 Sexual dysfunction has a strong negative impact on patients’ quality of life (QoL), and deterioration of QoL due to SD has been reported in both male and female patients with CKD. 3 –5 Adding to patients’ personal burden, SD affects social and married life. 6 Decreased partner satisfaction is a common problem; 50% of both male and female partners had decreased libido. 7 In male patients, 70% had erectile dysfunction (ED). Other sexual problems reported by men are reduced libido, difficulty in achieving orgasm, and anejaculation. 1,8 In female patients, sexual issues are twice as frequent compared to the general population; during dialysis, the prevalence of SD increases to 70%. 9,10 Sexual issues reported by women are reduced libido and lubrication, difficulty in getting aroused, pain during intercourse, and difficulty in achieving orgasm. 1,10 The etiology of SD is often multifactorial. Besides the uremic milieu, factors such as comorbid illness, anemia, hormone disturbances, autonomic neuropathy, vascular diseases, hyperparathyroidism, hyperprolactinemia, side effects due to medication, and psychosocial factors all contribute to the existence of SD. 1,2
Kidney transplantation (KTx) prolongs the life of patients with CKD and will enhance survival rates as well as QoL. 11,12 Due to normalization of the hormonal disturbances, transplantation improved sexual health (eg, libido), energy, and fertility. 13,14 However, after transplantation, the prevalence of SD still remains 46% in both men and women. 15 For instance, literature reports that kidney transplant recipients experience unusual hair growth (69.7%), decreased interest or ability to perform or respond sexually (60.9%), and changes in body shape (54.8%). 16 Immunosuppressive medication prescribed after transplantation also contribute to impotence in men and loss of sexual interest in both men and women. 17 The persistence of SD after receiving a kidney transplant negatively influence patients’ well-being, as research has shown sexual side effects after renal transplantation have the most negative impact on life satisfaction after transplantation. 16,18,19 Due to a shortage of organ donors, patients are more likely to receive a living donor kidney transplant from a relative or partner. 20 As a result, the relationship between recipient and donor may deteriorate as recipients may feel they owe the donor or are afraid to disappoint if they lose the graft. 21
Despite the evidence SD is a clinically relevant problem in patients with CKD before and after transplantation, this issue is often neglected in research as well as daily practice. 22 Sexual health is often ignored by health professionals during consultation, particularly after transplantation. 23,24 Motives for undervaluation of SD by renal care providers remain uncertain. This information is essential in order to be able to enhance current situation for patients with CKD.
Specific Aim
This cross-sectional study focused on current practice, opinions, and barriers of Dutch transplant surgeons regarding the discussion of SD with patients with CKD waiting for or after receiving a kidney transplant. In addition, this survey addressed surgeons’ level of knowledge and received education on SD in patients with kidney disease.
Design and Methods
Design, Setting, and Population
Data for this cross-sectional survey were collected using a questionnaire sent to all Dutch practicing surgeons and transplant fellows (n = 47). In the Netherlands, kidney transplantations are generally performed by transplant surgeons with a small minority by vascular surgeons. The study sample was obtained by contacting all Dutch transplantation centers (n = 9) to enquire information on their practicing surgeons and fellows. To ensure all Dutch transplant surgeons were reached, members of the Dutch Transplantation Association who specialized in KTx were included. Pediatric surgeons were excluded, as this study focused on patients over 15 years old. The Medical Ethics Committee of the LUMC Leiden reviewed the study and declared that for this analysis, without any interventions or patients, no formal ethical approval was needed.
Instrument Design and Development
The questionnaire used for this survey was developed by the authors, including an urologist-sexologist (H.W.E.) and a transplant surgeon (J.R.). The structure and design of the questionnaire were derived from questionnaires used in previous studies regarding sexuality and health-care providers, with items based on issues described in literature and additional themes identified by the authors. 25 –27 The survey was pilot tested by 5 transplant surgeons from the Leiden University Medical Centre. No adjustments were needed according to their comments. The pilot questionnaires were included for analysis because the definitive questionnaire remained unchanged.
The 39-item questionnaire contained multiple choice and open-end questions (available in the Online Supplementary material). Answers to the questions will be interpreted with the use of quantities and percentages. The first page consisted of demographic questions as well as an opt-out possibility. The reason for withdrawal could be noted. The second part of the questionnaire focused on current practice, potential barriers, and opinions of transplant surgeons with regard to discussing SD during consultation.
Data Collection and Procedure
All surgeons received the questionnaire at their work address; nonrespondents received a reminder letter 2 and/or 3 months after the initial mailing. All data were processed anonymously.
Data Analysis
Data analysis was performed by using IBM SPSS statistics v20 (IBM Corp, Armonk, New York). Gender and hospital location of respondents as well as nonrespondents were known . To make a comparison between nonrespondents and respondents, hospitals were classified by population density of the area. Class I included areas with a population density of 907 or less citizens per km2, class II had a population density of more than 907 citizens per km2. Age of nonrespondents remained unknown. Descriptive statistics and the Pearson χ2 test were used to compare demographic information of nonrespondents with demographics of the respondents. Demographic information of respondents and results of the survey were analyzed using descriptive statistics. Bivariate associations between demographic information and categorical data were calculated by using the Pearson χ2 test. The independent sample t test was used to calculated bivariate associations in case of numerical data. Outcomes were considered statistically significant if the 2-sided P values were <.05.
Results
Survey Responses
Thirty of the 47 questionnaires, including the 5 pilot questionnaires, were sent back resulting in a response rate of 63.8%. Three respondents were not willing to participate, reasons for not participating were “not enough experience” (n = 2) and “I don’t follow-up on patients” (n = 1). One participant was excluded due to an incomplete questionnaire. Additionally, 1 surgeon specialized in recovering deceased donor kidneys for transplantation and 1 pediatric surgeon were excluded (n = 2). Twenty-four (51.1%) of the 47 surveys sent were analyzed.
Demographics
Demographic comparison between respondents and nonrespondents is listed in Table 1. There was no significant difference in the distribution of gender or hospital location between respondents and nonrespondents (χ2 test, P = .47 and P = .07).
Demographic Comparison Between Nonrespondents and Respondents.
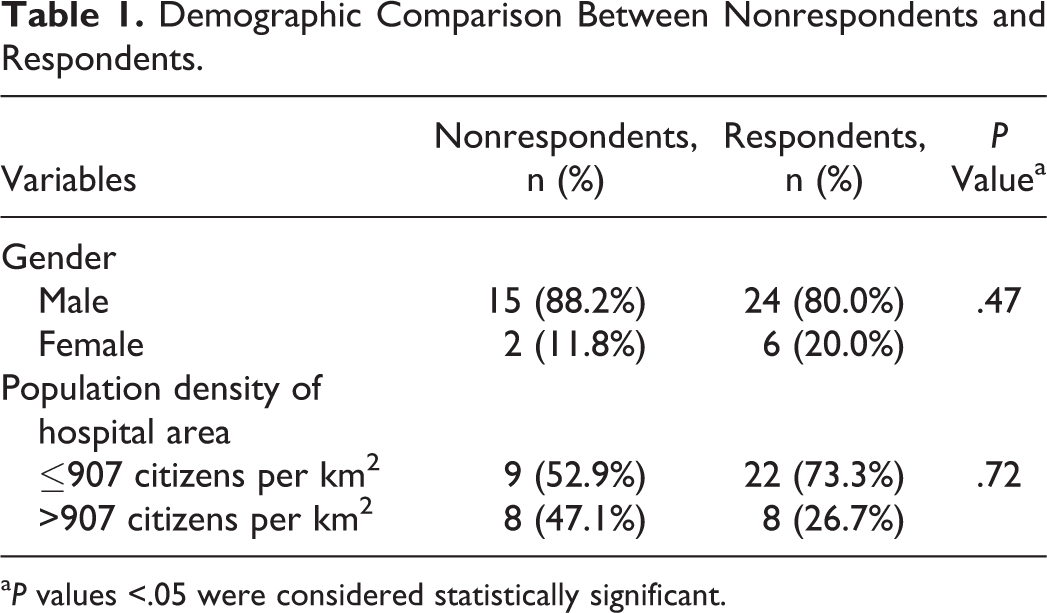
a P values <.05 were considered statistically significant.
Table 2 illustrates the demographic and practice characteristics of the analyzed respondents. The majority of the respondents was male (n = 17, 70.8%).
Respondent Characteristics (n = 24).
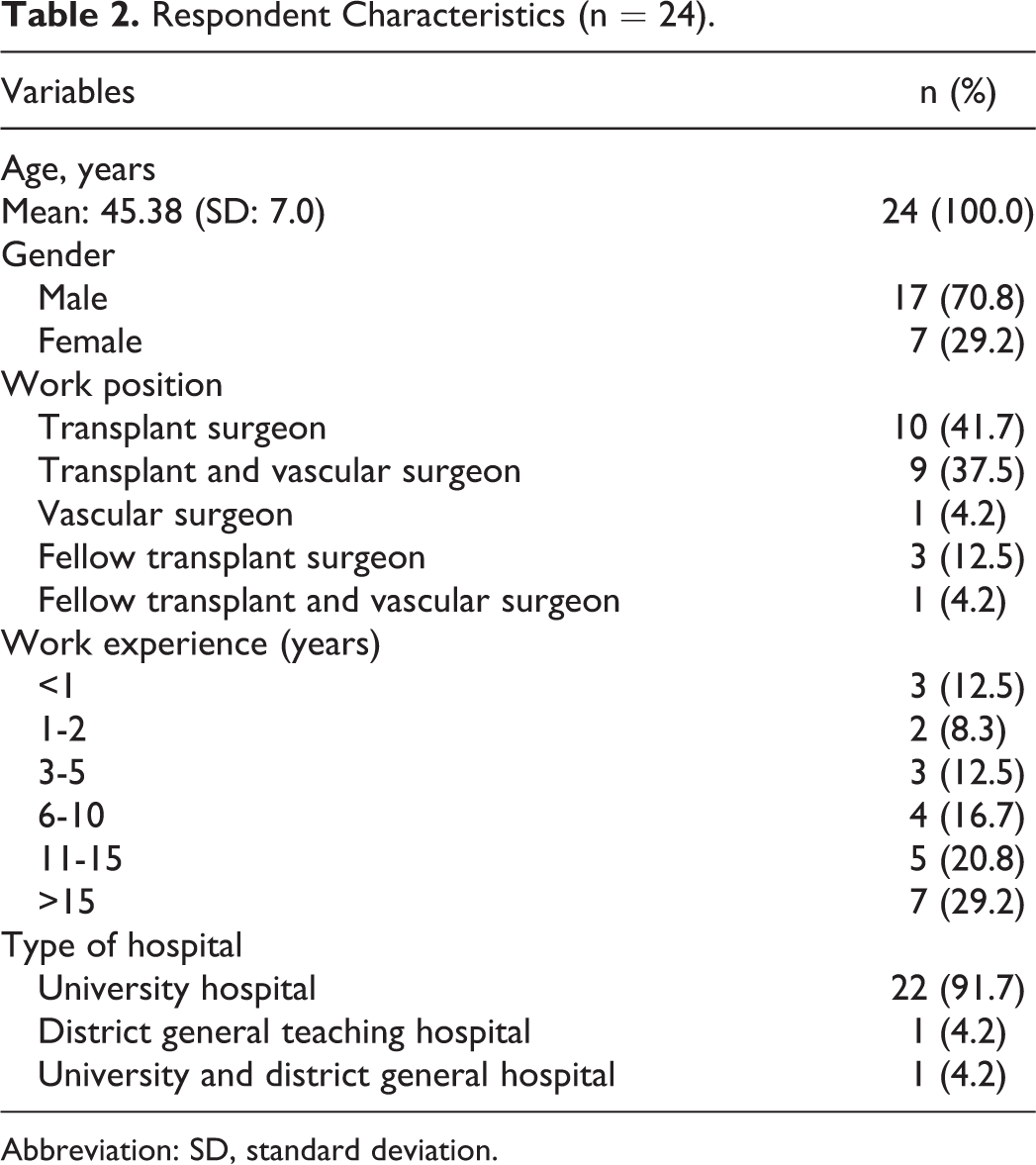
Abbreviation: SD, standard deviation.
Current Practice
When asked to describe current practice, all respondents answered (n = 24, 100%) that they (almost) never discussed SD with their patients before or after surgery. The large majority of the surgeons (n = 23, 95.8%) noticed that patients (almost) never express their sexual concerns spontaneously. Only 1 respondent experienced that patients express their concerns spontaneously in less than half of the cases.
Respondents were asked if the partner was present when SD was discussed. Almost 60% of the respondents (n = 10) answered that the partner was (almost) never present when SD was discussed and 11.8% (n = 2) said in less than 50% of the cases. Other answers given were in 50% of the cases (n = 1, 5.9%), in more than 50% of the cases (n = 2, 11.8%) and (almost) always (n = 2, 11.8%). On the question “How often do you tell your patients about the effect of immunosuppressant’s on sexual function?” 81.8% (n = 18) answered to never do so. The answers seldom and sometimes were both given by 2 (9.1%) respondents.
The majority of the respondents (n = 22, 90%) never inquired if their male patients use phosphodiesterase type 5 inhibitors. None of the respondents prescribed this type of medication to their patients with CKD.
Knowledge and Training
Surgeons were asked to rate their current knowledge level of SD. Seven (29.2%) respondents thought that they had some knowledge necessary to discuss SD, 60% (n = 14) stated to have not much, and 12.5% (n = 3) had no knowledge at all. None of the surgeons thought they had a lot of knowledge. Thirty percent (n = 7) considered themselves in need for additional training in order to properly discuss SD with patients. In answer to the question “Do you think sufficient attention is paid to SD as well as treatment options during residence training?” 87.5% (n = 21) replied negatively.
Barriers
The questionnaire contained a list of possible barriers to discuss SD during consultation, and the transplant surgeons were asked to which extent they agreed with those barriers. The list including surgeons’ answers is listed in Table 3. The main barrier to discuss SD during consultation is that surgeons do not feel accountable to do so (n = 17, 73.9%). Almost 40% (n = 9) of the respondents agreed that insufficient knowledge is an important barrier as well. However, 8 (34.8%) respondents disagreed and 6 (26.1%) were indecisive on this. In addition, insufficient training was a barrier for 5 respondents (21.7%), while 14 (60.9%) respondents did not consider this aspect as a barrier.
Barriers not to Discuss Sexual Dysfunction.a
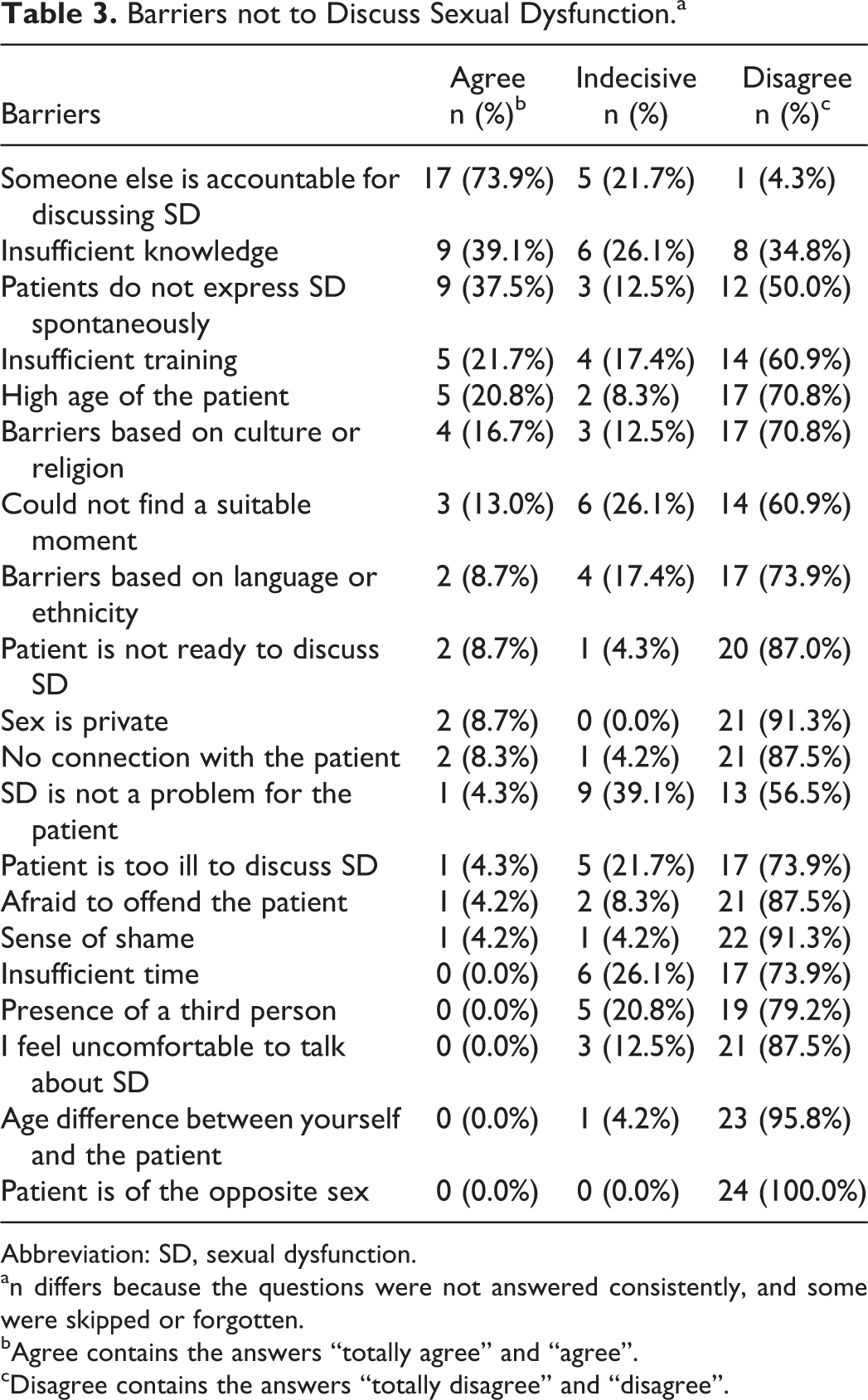
Abbreviation: SD, sexual dysfunction.
an differs because the questions were not answered consistently, and some were skipped or forgotten.
bAgree contains the answers “totally agree” and “agree”.
cDisagree contains the answers “totally disagree” and “disagree”.
Accountability and Local Agreements
The survey addressed whether clear agreements have been made within their department with regard to which care provider is accountable for discussing SD with patients CKD. Fifty percent (n = 12) had no clear agreements within their department, a third (n = 8, 33.3%) was unaware of such agreements. Four (16.7%) surgeons responded that clear agreements were present.
When asked which renal care providers should be accountable for discussing SD, the majority (n = 22, 91.7%) of the surgeons answered the nephrologist. Only 1 respondent agreed with the statement that this accountability should lie within their own group of professionals.
Focusing on the referral of patients with sexual issues to professionals specialized in SD, 19 (82.6%) respondents were aware of this possibility at their workplace. Four (17.4%) respondents were unaware of this possibility. The estimated percentage of patients referred to a sexual health-care provider was less than 1%.
Discussion and Conclusion
The present study revealed Dutch renal transplant surgeons rarely discuss sexual health concerns with their patients with CKD. Multiple factors may contribute to this finding. First of all, transplant surgeons skip the discussion of SD due to their perception that other renal care providers are accountable. The majority of the surgeons stated that the accountability should lie with the nephrologist. Previous research among nephrologists showed that this opinion is shared by this group of professionals since they pointed out themselves to be accountable for discussing SD with patients with CKD. 25 However, the same study also revealed that more than 90% of nephrologists often skip SD discussion as well. Seen in this light, there might be a role for other renal care providers (eg, dialysis nurse, and social worker) in discussing and detecting SD. At least, clear agreements should be made within medical departments regarding which care provider should be accountable for sexual health care since only a small percentage of the respondents in this survey were aware of the presence of such agreements. By formulating clear agreements within all nephrology departments, the incorporation of sexual health care for patients with CKD into current health-care system might be facilitated.
Second, an important factor that may contribute to the current undervaluation of SD is the lack of knowledge among surgeons on SD in CKD. The majority of Dutch surgeons had insufficient knowledge on SD, and some also noted insufficient knowledge as a barrier to discuss SD with their patients. These outcomes might be a result of inadequate education on SD in CKD since the vast majority of the surgeons stated that this subject is not addressed sufficiently in current educational system. In order to fully understand the impact of SD on patients with CKD, improvement of surgeons’ current level of knowledge on SD might be helpful. By incorporating adequate education into residence training, the level of knowledge on sexual health of this group of renal care providers will be improved, and awareness might be raised on the importance of this part of renal health care. For surgeons currently practicing, supplementary training could be provided.
This study evaluated clinical practice of transplant surgeons regarding SD in patients with CKD. Unfortunately, the omissions in sexual health care by physicians are present in many, if not all medical departments for illnesses that highly affects sexual function, for example, cardiology and surgical oncology. 26,27 The same applies for the department of nephrology, accountable for substantial part of renal health care. 25 Undervaluation of SD by care providers is recognized by patients with CKD, as several studies on patient-centered perspective reported little attention is paid to psychosocial support, including sexual health. 13,23,24 Besides, patients avoid addressing SD during consultation with their physician; in their perception, physicians may react reluctant and disinterested. 28 Awareness of patients’ concerns and burdens should be raised among transplant surgeons, and other renal care providers, to enhance the current situation.
Recommendations for Practice
Providing information on sexual health to patients with CKD awaiting KTx is extremely important, as they hold high expectations on life after transplantation and tend to overestimate the improvements of QoL. 11,12,15 If information is provided in the preoperative setting on sexual health after transplantation, these unfulfilled expectations might be prevented and it might encourage patients to discuss SD after transplantation if necessary. Considering surgeons’ daily practice, the accountability for providing extensive sexual health care to patients with CKD should not lie within this group of professionals. However, managing patients’ expectations of surgery is part of the preoperative care provided by surgeons. Therefore, it could be important for transplant surgeons to mention that, although transplantation tends to improve sexual health, the persistence of SD after transplantation is not uncommon.
Strength and Limitations
The perspective of renal transplant surgeons on sexual health was explored in this descriptive study. Unfortunately, formal comparison with literature was limited. In addition, due to the low response rate, nonresponse bias may have occurred and might have decreased the statistical power of the study. The study was performed using a nonvalidated questionnaire due to the nonexistence of validated questionnaires exploring all study aims. As a consequence, the answers given by the respondents may have been biased due to subjective questioning. The questionnaire was not tested for validity, as this instrument will not be reused. Also, the self-reported character of the questionnaire may have caused respondents to provide socially desirable answers. Finally, this study was performed in a single country, so findings may not represent the current situation worldwide.
Conclusion
Dutch surgeons performing KTx omit discussions of SD with their patients with CKD. They do not feel accountable to do so and think this accountability should lie with the nephrologist. Moreover, insufficient knowledge and inadequate education regarding SD are issues present in this group of professionals and for some surgeons they even reflect in present barriers toward the discussion of SD. By providing adequate sexual education to (future) transplant surgeons, level of knowledge could be enhanced and awareness could be raised on the importance of sexual health. The results emphasize that accountability for providing extensive sexual health care to patients with CKD should lie with another renal care provider. However, surgeons could briefly provide information during preoperative consultation on sexual health after transplantation so unfulfilled expectations in transplant recipients might be prevented. Finally, the development of multidisciplinary medical protocols on which renal care providers has the accountability to discuss SD may lead to improvement, as it could serve as the foundation for sexual health care for patients with CKD.
Footnotes
Acknowledgments
The authors thank all Dutch transplant surgeons who took the time to fill out the questionnaire. Linguistic supervision was performed by Emma Horton, MD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.