
Abstract
Purpose:
The purpose of this study is to describe a new bailout maneuver for use during fenestrated thoracic endovascular aneurysm repair (fTEVAR) in the event of wire wrap or wire entanglement with the proximal graft fabric.
Technique:
A 68-year-old-man with hypertension and chronic atrial fibrillation underwent elective thoracic endovascular aneurysm repair (TEVAR) with a left subclavian fenestration to treat a residual arch and thoracic aortic aneurysm after previous type A dissection repair. The procedure was challenging due to malrotation of the main body graft, as well as wire entanglement of the precannulated through-and-through wire on the leading edge of the main body fabric. A novel bailout maneuver is described. Through-and-through access was maintained, and a long 8F sheath was delivered through the fenestration from femoral access, and an 8.5F steerable sheath was delivered through upper extremity access. This allowed coaxial snaring of a new through-and-through wire via the gutter between the stent-graft and native aorta in the seal zone, which both reoriented the fenestration, and permitted placement of a bridging stent to the left subclavian artery.
Conclusion:
The retrograde-access gutter snare (RAGS) technique described above provides a streamlined approach to achieve technical success in challenging fenestrated thoracic endovascular aneurysm repair (fTEVAR) cases.
Clinical Impact
This technical note describes the retrograde-access gutter snare (RAGS) technique that can provide a successful bailout maneuver for fenestrated TEVAR (fTEVAR) devices. The RAGS technique offers an approach to be used with precannulated custom-made or physician-modified fTEVAR devices in which wire wrap or wire entanglement precludes access through the fenestration after deployment of the main body device. Instead of traditional attempts at de novo cannulation of the fenestration from upper extremity or femoral access, the maneuver offers an approach to maintaining through-and-through access to facilitate snaring a new wire proximal to the leading edge of the main body fabric, which can then be used to deliver a covered stent into the fenestration from either the upper extremity or femoral access. This technique offers an added benefit of potentially realigning malrotated fenestrations via tensioning of the new through-and-through wire.
Keywords
Introduction
Traditional endovascular approaches to treating aortic aneurysms with proximal landing zones in Ishimaru zones 0 to 2 have required some form of surgical debranching of the aortic arch vessels to facilitate an appropriate landing zone. 1 Total endovascular approaches have included physician-modified endografts (PMEGs)2–4 and in situ fenestration techniques5–7 to restore patency to the aortic arch branches with stented or unstented fenestrations. Custom and off-the-shelf devices are also available to complete a total endovascular approach to zone 0 to 2 interventions using either branches or fenestrations.8–10 These devices can face technical challenges secondary to stent-graft rotation, malalignment, and wire entanglement that can be potentially challenging to navigate. This report describes a novel bailout technique that can potentially be used with multiple custom, off-the-shelf, or physician-modified graft designs when tackling the problem of wire wrap and fenestration malalignment.
Technique
A 69-year-old male with a past medical history of hypertension, atrial fibrillation, benign prostatic hypertrophy, and a previous left inguinal hernia repair presented with a 6 cm thoracic aortic aneurysm secondary to aortic dissection. He had presented 1 year prior with acute type A aortic dissection extending from above the sinotubular junction to the left common femoral and right external iliac arteries. This was repaired with aortic arch replacement to Ishimaru zone 2 with a 30 mm Dacron graft and debranching of the innominate and left common carotid arteries with a 16× 8 mm bifurcated Dacron graft. A postoperative computed tomography (CT) scan demonstrated maximum transverse diameter of the remaining aortic dissection to be 4.5 cm in diameter. During regular surveillance, this rapidly enlarged to 6 cm in 1 year. A large fenestration was visible at the origin of the left subclavian artery just distal to the surgical graft anastomosis (Figure 1). We designed a single-fenestrated thoracic endograft to land in the surgical graft proximally, extended by a Zenith Alpha ZTA-P-30-201 stent-graft (Cook Medical, Bloomington, Indiana) in the true lumen into the supraceliac aorta, and a custom 40 mm false lumen-occluding endograft deployed in the false lumen at the same level as the distal seal of the endograft in the true lumen (Figure 2). The procedure was performed in our hybrid operating room (Artis Zeego; Siemens, Munich, Germany) under fusion imaging guidance. The patient was in the supine position under general anesthesia with the left arm on an adjustable arm board. Ultrasound-guided percutaneous bilateral femoral access and left axillary access were obtained with 2 Perclose Prostyle closure devices (Abbott Vascular, Abbott Park, Illinois) placed in all 3 access sites. Percutaneous left common femoral vein access was also obtained using ultrasound guidance to facilitate balloon occlusion of the IVC for controlled hypotension during endograft deployment. A glidewire (Terumo, Somerset, New Jersey) was first placed into the ascending aorta in the surgical graft, and Visions PV .035 IVUS catheter (Philips Volcano Corporation, San Diego, California) was used to confirm true lumen access throughout the aorta. A vertebral catheter was advanced across the aortic valve, and through this a double-curved Lunderquist wire (Cook Medical, Bloomington, Indiana) was placed into the LV apex. Over this wire, the main body was advanced to the descending thoracic aorta, and the precannulated catheter was used to advance a 450 cm glidewire (Terumo, Somerset, New Jersey), which was snared through the left axillary access using a 35 mm Amplatz Gooseneck Snare (Medtronic, Santa Rosa, California) to establish through-and-through access.
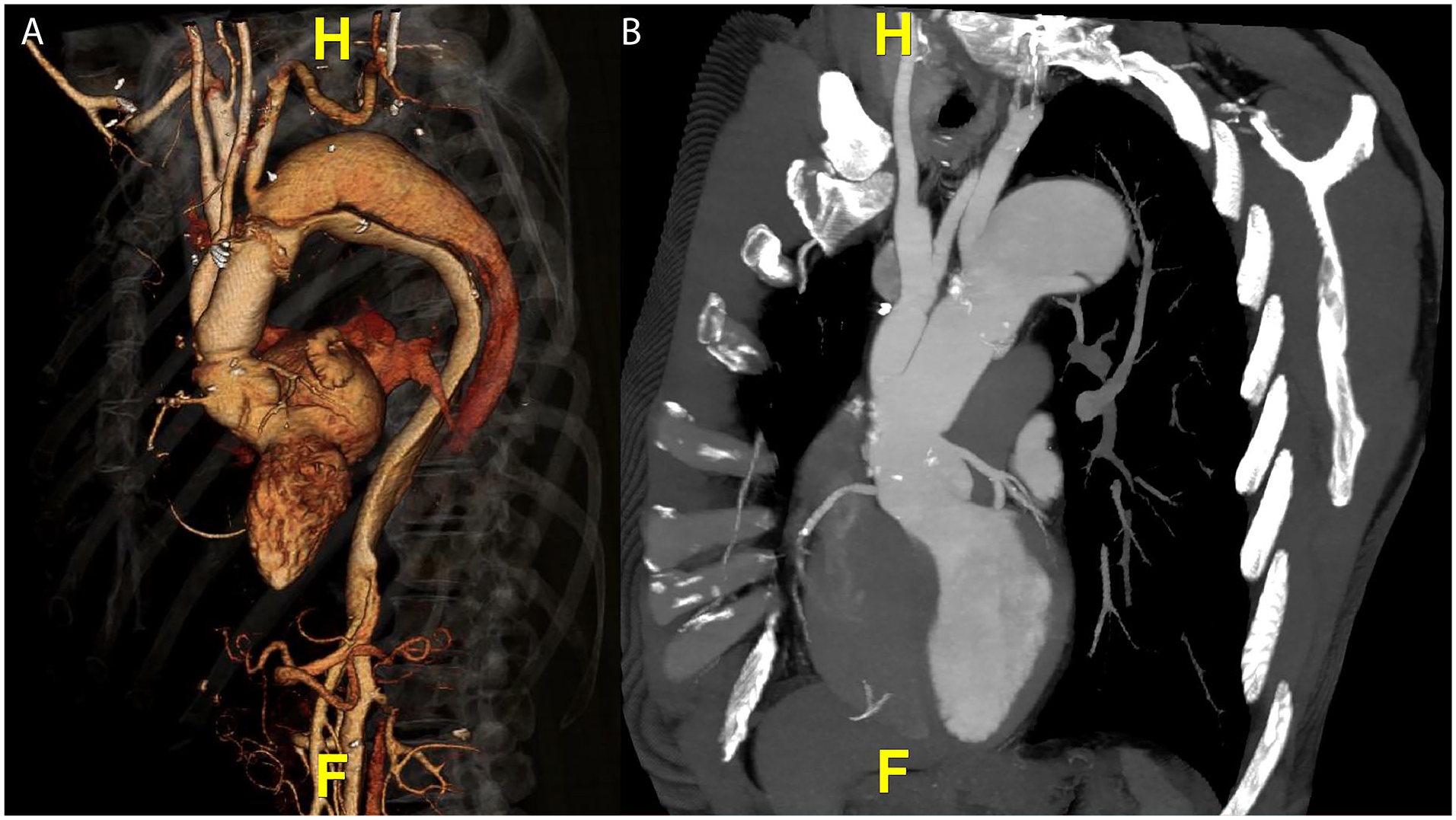
(A) 3D volume rendering of preoperative CT scan demonstrating residual dissection distal to the ascending aortic surgical graft, with the left subclavian artery arising off the false lumen and aneurysmal dilatation of the proximal descending thoracic aorta causing true lumen compression. (B) Large dissection septum fenestration visible at the base of the left subclavian.
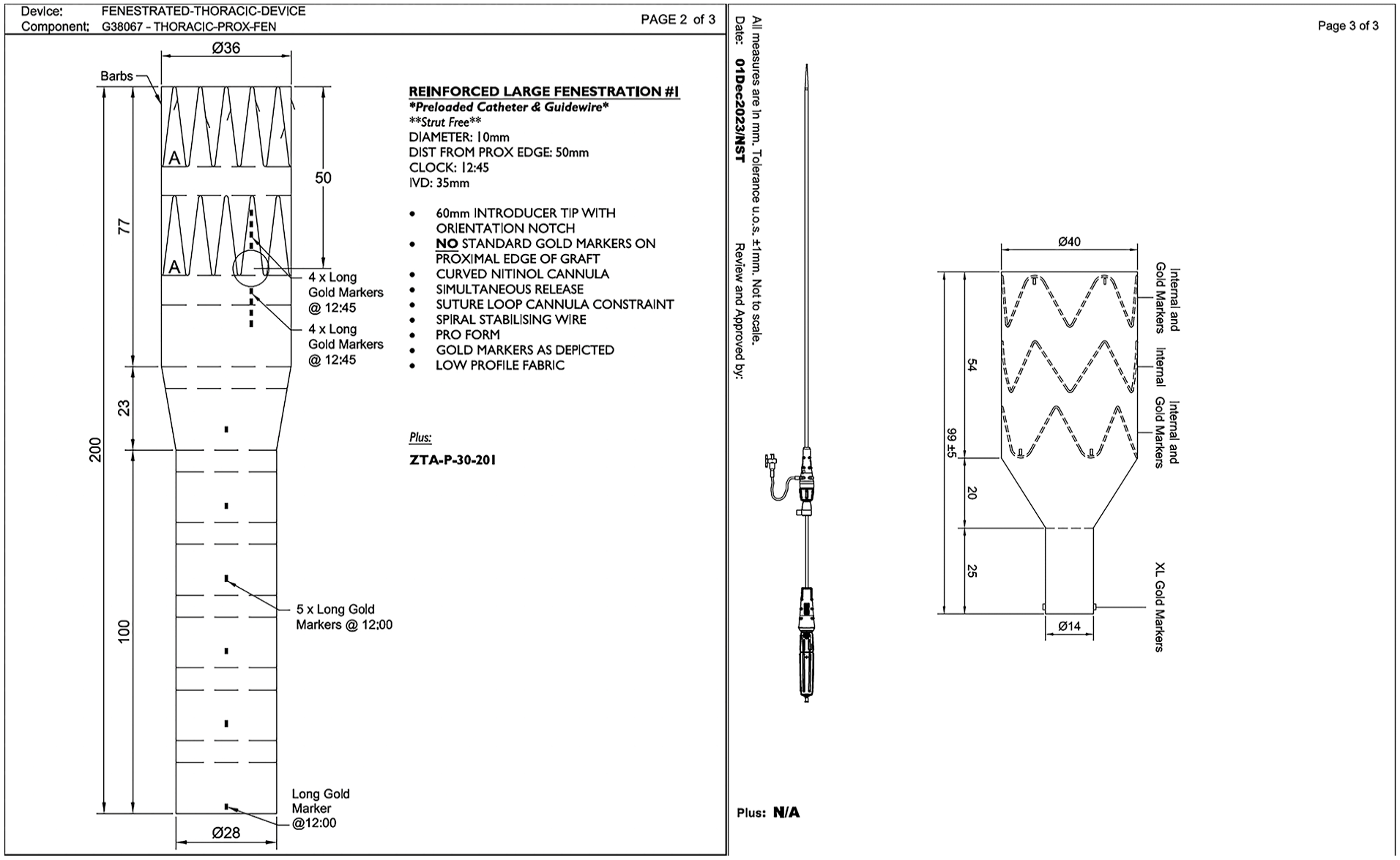
Designs for custom left subclavian fenestrated device and false lumen-occluding endograft.
The procedure was complicated by wire wrap between the main body stiff wire and precannulated hydrophilic wire, which necessitated withdrawing the main body device and resnaring the precannulated glidewire to resolve. The steep angulation of the aortic arch created by the surgical graft induced significant stent-graft rotation upon advancing the device into the location of the proximal seal. After successfully achieving a suitable orientation, the device was unsheathed under controlled hypotension with IVC balloon occlusion. The device was observed to migrate distally and rotate anterior away from the subclavian artery origin during deployment. Despite tensioning of the through-and-through wire, the precannulated wire became entangled on the leading edge of the stent-graft.
Attempts were made to advanced 5F angled catheters from the axillary and femoral access over the through-and-through wire to disentangle the wire from the leading edge of the fabric, but these proved unhelpful. It was felt that attempts to recannulate the fenestration from above or below would be significantly challenging given the rotation of the main body as the fenestration appeared to be sealed against the aortic wall. In order to navigate this challenge, we planned to attempt snaring a new through-and-through wire in the aneurysmal portion of the thoracic aorta using coaxial access from the axillary and femoral sheaths. This would allow placement of sheaths into the gutter between the proximal sealing stent and surgical graft to manipulate wires and catheters retrograde into the aneurysm to facilitate snaring a new through-and-through wire, which we have named the retrograde-access gutter snare (RAGS) technique.
An 8F × 90 cm Pinnacle Destination guide sheath (Terumo, Somerset, New Jersey) was advanced from femoral access to just outside of the fenestration, and the valve was punctured coaxially to advance a buddy wire out the fenestration into the ascending aorta. Over this coaxial wire, we placed a 100 cm C2 catheter and were able to successfully reform the reverse curve in the space between the proximal sealing stent and the surgical graft, which then allowed us to direct a glidewire retrograde into the thoracic aneurysm. Subsequently, an 8.5F × 65 cm Destino Twist (Oscor Medical, Palm Harbor, Florida) steerable sheath was advanced to the subclavian ostium from axillary access, and this was coaxially punctured to place a buddy wire outside of the custom device at the left subclavian ostium. A 125 cm VanSchie 3 catheter was then used to advance the buddy wire retrograde into the thoracic aneurysm parallel to the femoral buddy wire. By advancing a 6F snare catheter over the axillary wire followed by a 35 mm Amplatz Gooseneck snare, we then successfully snared the femoral wire and re-established through-and-through access without entanglement at the leading edge of the fabric (Figure 3 and Supplemental Video 1). The original through-and-through wire entangled with the leading edge of the stent-graft was then removed. Tensioning the new through-and-through wire allowed us to advance the femoral 8F × 90 cm sheath into the Oscor sheath using the sheath-rendezvous technique, which reoriented the fenestration to the correct orientation guided by wire tension (Supplemental Video 2). The 8F femoral sheath was then exchanged for a 10F × 80 cm Cook Flexor Sheath (Cook) to facilitate placement of a Bentley BeGraft Aortic (Bentley Innomed, Hechingen, Germany) 12 mm × 59 mm bridging stent into the left subclavian artery below the takeoff of the vertebral artery. The BeGraft was reflared on both sides using a 12 mm × 20 mm Mustang (Boston Scientific) balloon. Subsequent deployment of the distal thoracic stent-graft and false lumen-occluding endograft was performed uneventfully. Completion angiography showed no evidence of endoleak and no evidence of false lumen filling proximal to the false lumen-occluding endograft. Prostyle sutures successfully achieved hemostasis at all 3 access sites.
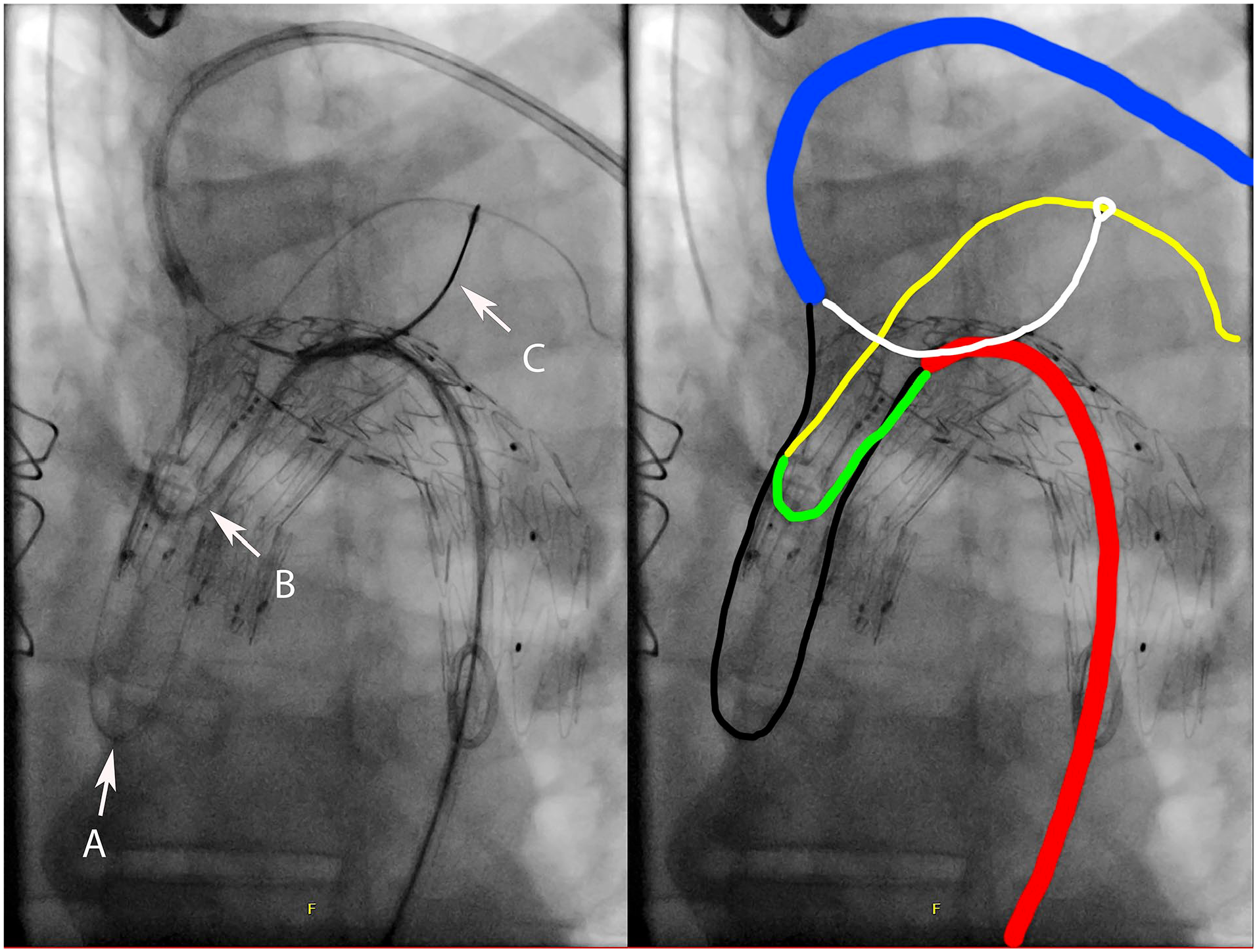
Successful execution of the RAGS technique. (A) Through-and-through wire entangled with the leading edge of the stent-graft. (B) C2 catheter reformed in the gutter of the proximal endograft seal zone. (C) Snare exiting coaxial from the upper extremity steerable sheath. Black—original precannulated wire entangled with the proximal edge of the fTEVAR. Blue—8.5F steerable sheath from left arm access. Red—8F sheath from transfemoral access. Green—5F C2 catheter introduced coaxially through femoral access sheath and reformed in the proximal seal gutter. Yellow—new hydrophilic wire aimed retrograde in the descending thoracic aorta. White—6F Gooseneck snare coaxial through left arm access sheath successfully engaged with the new transfemoral wire in yellow.
The patient was transferred to a monitored step-down setting for 24 hours and received a postoperative CT scan prior to discharge, which confirmed the absence of false lumen filling with no endoleak and patency of the left subclavian artery. This also confirmed successful reorientation of the fenestration, with only mild angulation of 19° in the anteroposterior orientation (Figure 4). The patient was successfully discharged on postoperative day 2.
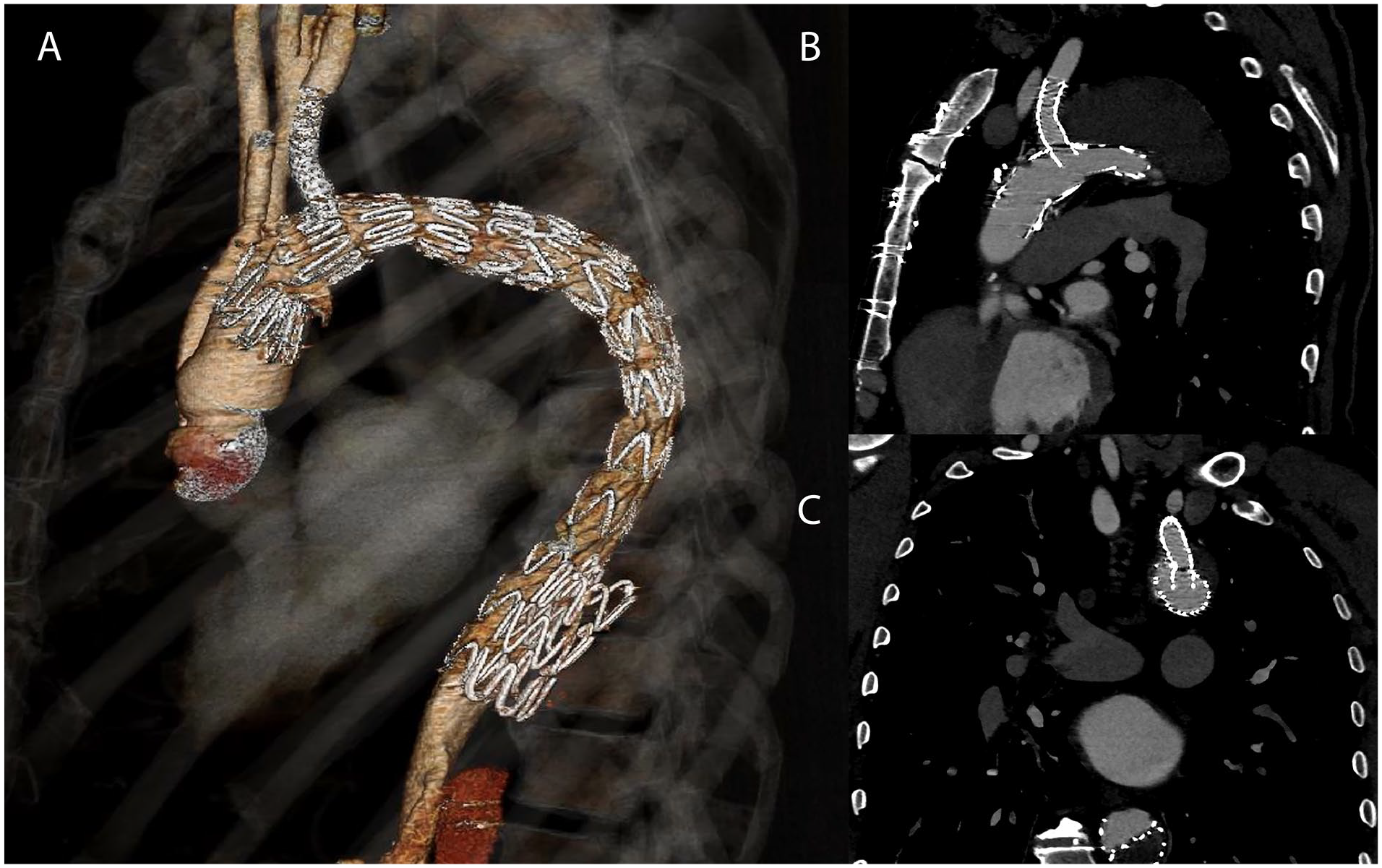
(A) 3D volume rendering of postoperative CT scan demonstrating successful exclusion of the false lumen and thoracic aneurysm, with cessation of retrograde false lumen filling below the level of the false lumen-occluding graft. (B and C) Long-axis and short-axis views demonstrating appropriate reorientation of the fenestration with minimal angulation of the left subclavian stent-graft.
Discussion
Although technical success rates of endovascular repair for custom branched and fenestrated grafts are high, 11 the volume of experience with branched and fenestrated arch grafts is not as robust. 12 Although several bailout maneuvers for thoracoabdominal grafts are well described such as the snare ride technique, 13 the balloon anchoring technique, 14 and the elevator technique, 15 troubleshooting techniques to overcome challenges with branched and fenestrated thoracic grafts are not as robust.
Technical approaches to the deployment of the Cook fTEVAR platform have been described previously, 16 which address troubleshooting approaches in navigating wire entanglement and malrotation. These previously described troubleshooting techniques included buddy puncture of upper access to cannulate the fenestration retrograde, antegrade catheterization and snaring after abandoning through-and-through access, liberation of the entangled wire with catheter or balloon manipulation, or abandonment of the fenestration with chimney graft rescue or extra-anatomic bypass.
Our technique takes advantage of the entangled precannulated wire to place sheaths outside of the fenestration from both upper and lower extremity access to avoid the need for de novo cannulation of the fenestration. This allows for an attempt at snaring a new through-and-through wire in any location proximal to the proximal edge of the fabric of the fTEVAR device. Although in this case the large proximal thoracic aneurysm provided a suitable space for snaring retrograde to the fenestration, this could conceivably be done anywhere between the graft fabric and aortic wall, similar to a subintimal recanalization using the subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) technique. 17 The establishment of a new through-and-through wire also offers the potential added benefit of realigning the fenestration in the event of imperfect deployment of the main body graft. We believe this adds a valuable troubleshooting technique that can be explored prior to resorting to chimney grafts or extra-anatomic bypass to preserve the fenestration.
Conclusion
Technical challenges caused by wire wrap and device malrotation can compromise the success of fTEVAR. The RAGS technique represents an option to attempt to preserve the fenestration with the added benefit of potentially correcting malrotation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.P. is a co-founder and chief medical oQicer of Frontline Medical Technologies Inc and is a consultant for Gore Medical. J.L. is a consultant for Terumo Medical. All authors received no support from any organization for the preparation or submission of this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Informed Consent
The patient involved in this technical note gave verbal consent for participation and publication of the images in this case.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.