
Abstract
Objective
The COVID-19 pandemic highlighted the role that local health departments (LHDs) have in cross sector can address alone, including the work of value alignment and the strategic use of organizational authorities. The practices by which LHDs used their authorities to conduct cross-sector work during the pandemic need exploration.
Method
We conducted semi-structured interviews with 19 public health leaders from metropolitan LHDs across the United States. Our interview guide assessed the values that LHD leadership prioritized in their cross-sector work as well as the range of organizational authorities they leveraged to influence external decision-making in other sectors.
Results
We found that LHDs approached cross-sector work by leaning on diverse values and authorities, each with unique implications for their work. The LHDs emphasized their approach to value alignment on a sector-by-sector basis, strategically using diverse organizational authorities—economic, political, moral, scientific, and logistical. While each authority and value we assessed was present across all interviewees, how each shaped action varied. Internally, LHDs emphasized certain authorities more than others to the degree that they more closely aligned with prioritized core values.
Conclusion
Our findings highlight the ongoing need for LHD leadership to improve their ability to effectively communicate public health values and the unique authorities by which health-supporting work can be facilitated, including how this message must be adapted, depending on the specific sectors with which the LHD needs to partner and the governance arrangement in which the LHD is situated.
Throughout the COVID-19 pandemic (hereafter, COVID-19), local health departments (LHDs) across the United States served an integral role in the public health response (Gostin & Wiley, 2020). The complexity of COVID-19 has also demanded cross-sector work—including a mix of collaboration, coordination, and cooperation—to achieve system-level changes that no sector can address alone (Castañer & Oliveira, 2020). In this context, many LHDs have worked with academia, health care, social services, education, and others to develop better informed and more impactful strategies to protect the health of their community (Burwell-Naney et al., 2021; Ravenhall et al., 2021).
Identifying common values is essential to cross-sector work (Landers et al., 2020). When making decisions with partners in the community, LHDs are often placed at a difficult juncture, balancing the needs and values of various sectors while upholding the core values of public health (DeBruin & Leider, 2020). Value alignment, defined as leveraging one or more shared values between organizations, is a critical tool for motivating cross-sector action that would not otherwise be realized. Whereas universal alignment (sharing all values across all partners) is rare, partial alignment among a few values is critical for driving collective action (de Montigny et al., 2019). Moreover, the challenge of value alignment likely varies across sectors, depending on the overlap in commonly held values in each sector. It has been demonstrated that traditional public sector values (e.g., altruism and justice) are more likely to align with commonly held values in community-based organizations (CBOs) than those in the private sector (e.g., entrepreneurship and individualism), implying that value alignment between government and CBOs may be more likely than alignment between government and the private sector (Miller-Stevens et al., 2014).
Cross-sector work also demands the use of various “authorities” that governmental organizations can leverage to influence behavior in other sectors. As outlined by public administration research on the various “policy tools” of government agencies, such influence can include but need not be limited to legal action (Acciai & Capano, 2021; Capano & Howlett, 2020). To affect behavior in their community, government agencies, such as LHDs, can lean on “soft” authorities that involve actions such as logistically coordinating action, communicating data and evidence, financially incentivizing desired outcomes, and appealing to morals (Blomqvist, 2016; Howlett & Fraser, 2009).
Cross-sector work has been especially challenging during COVID-19 as public health authority and values have received heightened scrutiny (Halverson et al., 2021; Juliano et al., 2021). To mitigate the spread of COVID-19 in their community, local governmental public health actions—stay-at-home orders, mask mandates, and travel restrictions—were often enacted (Gostin & Wiley, 2020). Pushback to these actions prompted the approval of new laws that limit public health’s legal authority (e.g., banning mask mandates; Weber & Barry-Jester, 2021) and lawsuits against public health agencies remain an ongoing challenge (Holt et al., 2021). These legislative actions have illuminated the complexities that emerge when conflicting values collide and organizational authorities are contested across sectors (Angeli et al., 2021).
Calls for improved cross-sector, health-related decision-making have reinvigorated the need to view local public health as a complex, multi-sector system (Brownson et al., 2020). Recognizing this call, we aimed to understand how LHDs leaned on organizational values and authorities to conduct cross-sector work during COVID-19, with the hope that our learnings will inform cross-sector work supporting health in this and other public health crises.
Method
During November and December 2021, we conducted semi-structured interviews with leadership from metropolitan LHDs across the United States to assess prioritized values and organizational authorities used to facilitate cross-sector work during COVID-19.
Interview Recruitment and Design
To ensure interviewees were aware of cross-sector concepts and skills, we recruited leaders from LHDs that participated in the Kresge Foundation’s Emerging Leaders in Public Health program (kresge.org/elph). Interviewees were not financially compensated for their participation. Two members of the study team (K.J. and K.H.L.) developed a semi-structured interview guide (Supplemental Appendix 1) and one researcher (K.J.) conducted the interviews. All interviews were conducted virtually and lasted between 45 and 90 minutes. The University of North Carolina at Chapel Hill (UNC) Institutional Review Board exempted this study (No. 20-2087).
The American Public Health Association’s (APHA) Public Health Code of Ethics, updated in 2019, identifies six core values for the field: professionalism and trust, health and safety, health justice and equity, interdependence and solidarity, human rights and civil liberties, and inclusivity and engagement (APHA, 2019). Using this code as a framework, our interview guide explored how these values were prioritized by LHD leadership in their cross-sector work. We also explored the range of organizational authorities they leveraged to influence external decision-making in other sectors. Organizational authorities were explored in relation to three different sectors, chosen to represent a spectrum of sector-specific values: business, CBOs, and local government.
Analytical Approach
We employed conventional content analysis to analyze transcripts (Hsieh & Shannon, 2005). After outlining a codebook based on our interview guide, additional codes were added while analyzing three randomly selected transcripts until all data fit an existing code (Supplemental Appendix 2). Using MAXQDA 2020 qualitative analysis software, two researchers (C.B. and K.J.) independently applied codes to all transcripts, initially resulting in a kappa coefficient of 0.58. Kappa coefficients above 0.60 are considered “substantial” (McHugh, 2012); C.B. and K.J. resolved coding disagreements until the percent agreement for all codes was above 0.60, establishing an overall kappa coefficient of 0.67.
Results
Seeking diversity among midsize, metropolitan LHDs, Emerging Leaders in Public Health Initiative (ELPH) staff connected us with leadership from 24 midsize, metropolitan LHD leaders across a range of perceived capability levels for cross-sector work, jurisdiction size, and political context. Of the 24 individuals approached, 19 (79%) agreed to participate. Our final sample of 19 participants represented LHD jurisdictions ranging from approximately 200,000 to 750,000 residents. Based on, in large part, the relationship between local and state public health employees, local–state governance models can be decentralized, centralized, mixed, or shared (Meit et al., 2012). The majority (n = 16/19) worked in states with decentralized or largely decentralized public health systems and within single-county jurisdictions (n = 11/19; Supplemental Appendix 3).
The Roles, Challenges, and Strategies to Uphold Public Health Values During COVID-19
Throughout COVID-19, the six APHA Core Values of Public Health were leveraged in different ways and contexts. Table 1 outlines each value’s unique role, as well as the associated challenges and strategies employed to adhere to each value during COVID-19.
Roles, Challenges, and Strategies of the APHA Code of Ethics Values During COVID-19
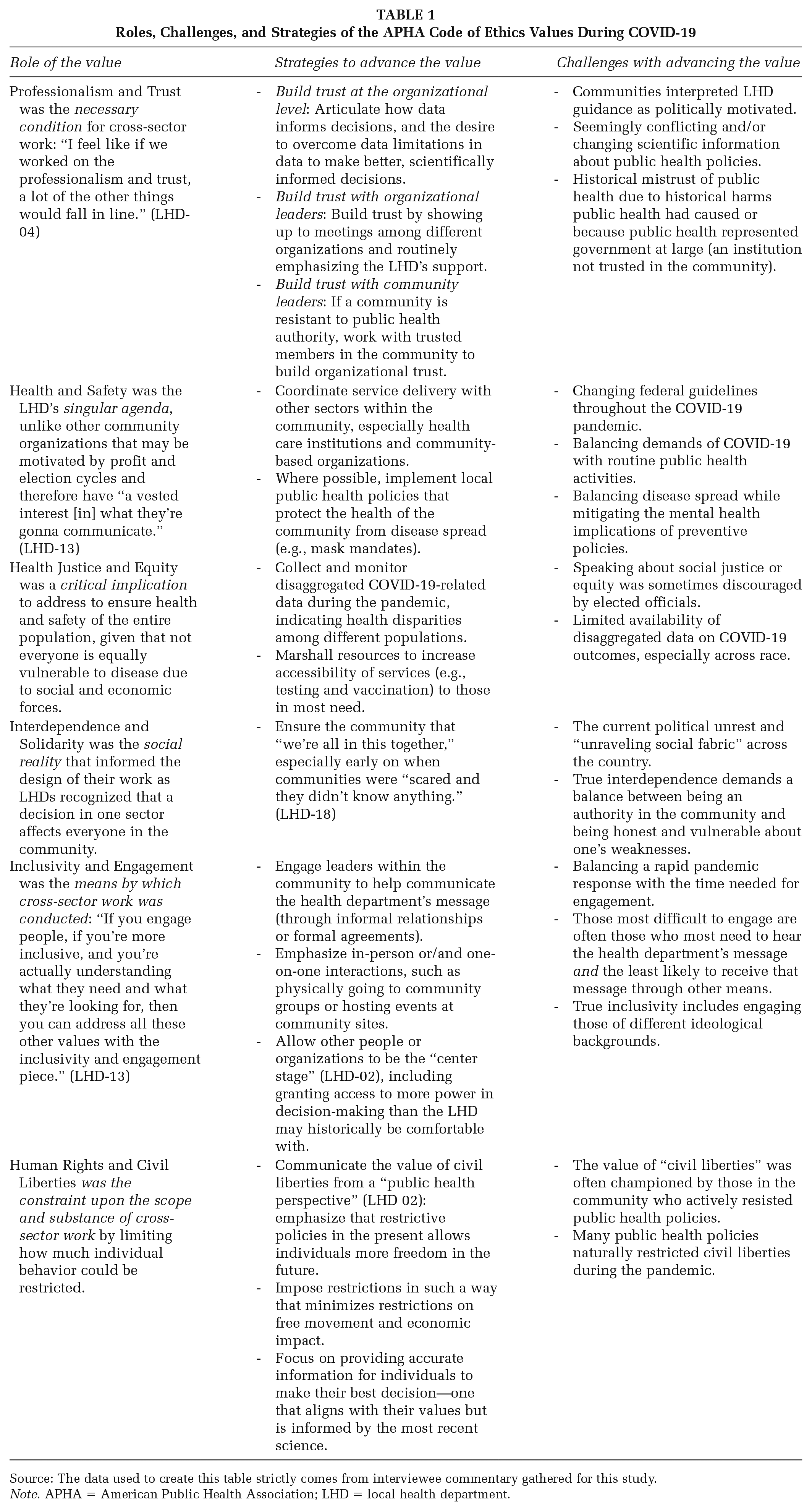
Source: The data used to create this table strictly comes from interviewee commentary gathered for this study.
Note. APHA = American Public Health Association; LHD = local health department.
Conflicts and Synergies for Each APHA Value
Interviewees discussed the strong overlap between the value of inclusivity and engagement with health justice and equity as pursuing equity demanded bringing historically marginalized communities “to the table and sharing power and listening to them and using their solutions” (LHD-09). Interviewees noted tension between promoting health and safety and the need to preserve the value of human rights and civil liberties through advancing “restrictive policies” that necessarily curtailed individual freedoms (e.g., mask mandates, social distancing). This tension was exacerbated by challenges with other values: The perceived lack of interdependence and solidarity in the country (“all of this has happened at a time when we ripped apart our society” [LHD-08]) made it difficult for LHDs to convince their communities to sacrifice for the common good. Threats to professionalism and trust also challenged the LHDs ability to convince “people that you’re wanting to do something . . . that’s going to benefit them” (LHD-13).
Importance and Challenge of Sector-Specific Value Alignment
Given the perceived “interconnectedness . . . of these decisions that get made” (LHD-12) across sectors, interviewees emphasized their role in seeking cross-sector value alignment. As opposed to persuading all sectors to seek alignment on values at the same time, LHDs spoke about value alignment as being “sector-specific,” both to avoid an overwhelming number of conflicting viewpoints “when you have everybody at the table” (LHD-02) and because “every sector had their own questions, they had their own concerns” (LHD-13). Six strategies for practicing sector-specific value alignment emerged from the interviews: practice humility, know your own values and how to articulate them, understand the values of the other sector, find points of connection between values, tailor your message to your audience, and work with trusted messengers (Figure 1).
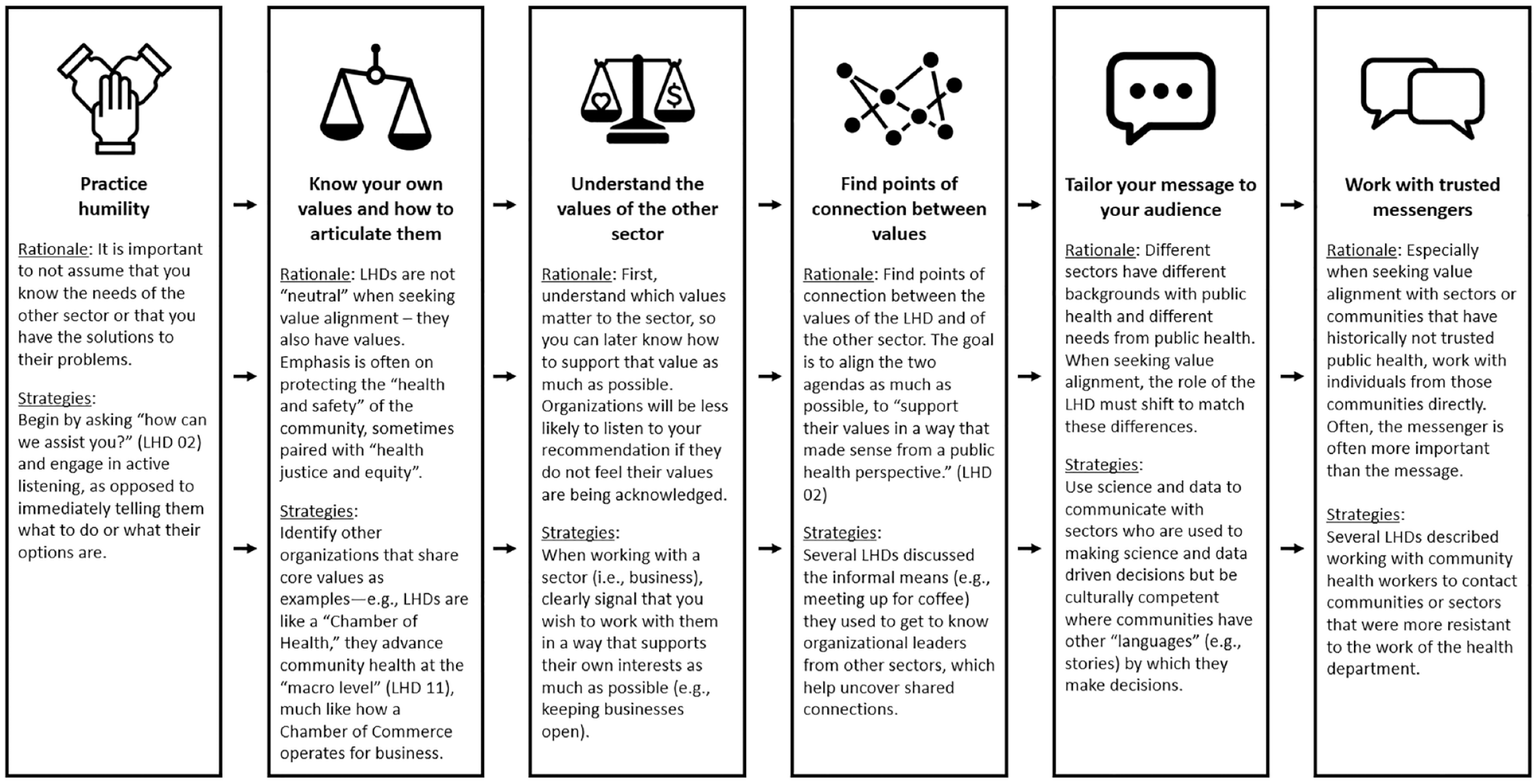
Reported Strategies for Cross-Sector Value Alignment Between LHDs and Other Sectors During the COVID-19 Pandemic
Challenges with value alignment were noted. Given that the crisis was public health focused, there was minimal room for compromise with sectors that did not share public health’s values. Challenges with value alignment were compounded in newer partnerships that lacked the baseline trust and familiarity with the other’s values common to long-lasting collaborations. LHDs also had to balance a rapid pandemic response with the substantial time needed for genuine value alignment.
The Use of Public Health’s Organizational Authorities During COVID-19
Effective Use of Diverse Organizational Authorities
Organizational authority exercised by LHDs in cross-sector work was categorized as being scientific, moral, economic, political, and logistical (Supplemental Appendix 2 outlines how authorities were defined within interviews). At least one instance of each authority was documented regarding the LHDs’ work with businesses, CBOs, and local government officials (Table 2).
Use of Local Health Department Organizational Authorities Across Sectors During COVID-19
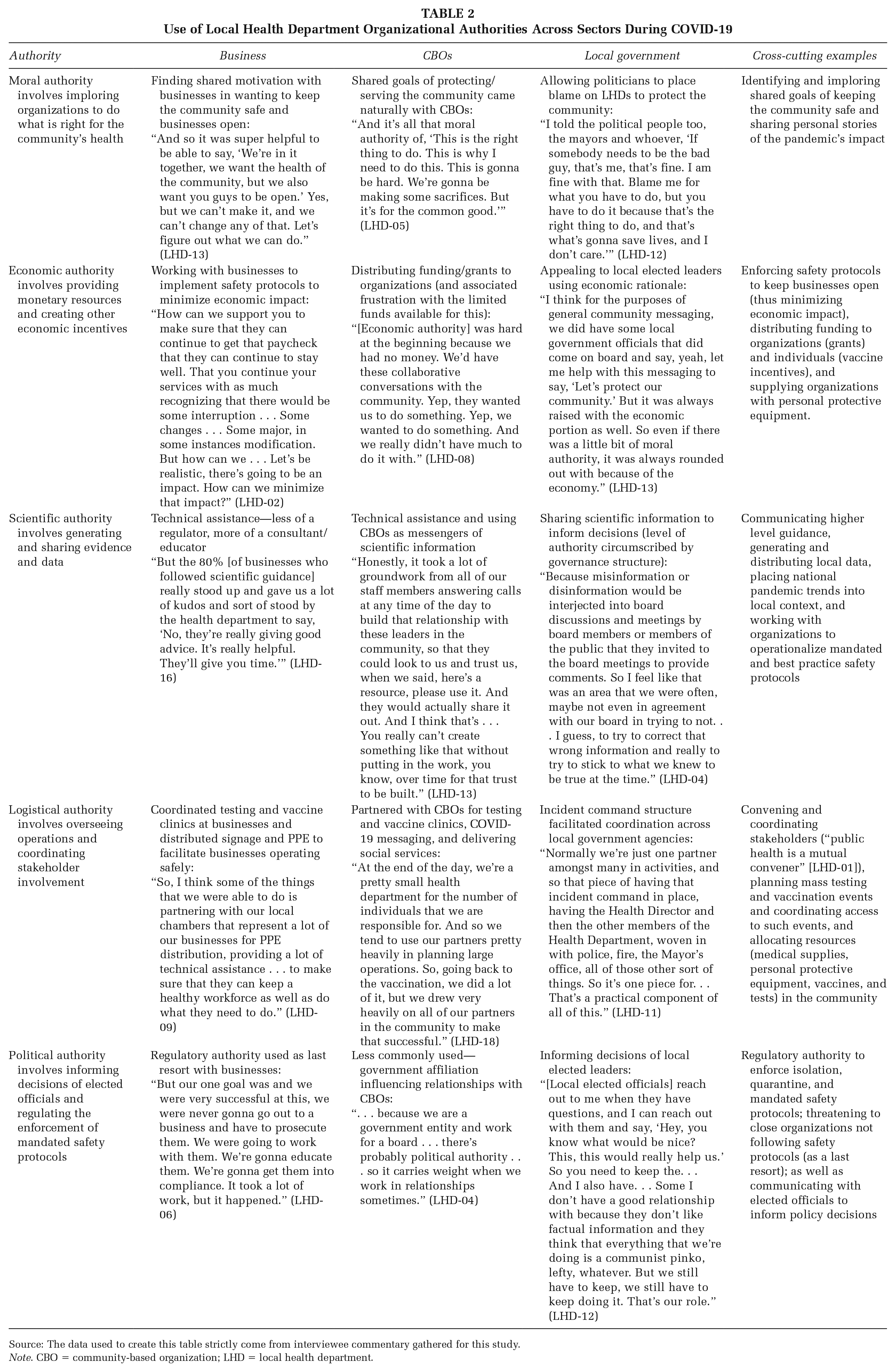
Source: The data used to create this table strictly come from interviewee commentary gathered for this study.
Note. CBO = community-based organization; LHD = local health department.
Across all sectors, scientific authority was referenced most commonly, followed closely by moral and logistical authority. In contrast, political and economic authorities were used less often, with some interviewees making a point to distance themselves from the use of political authority: “Well, one I can say that doesn’t work at all is political authority, so we try not to fall on that at all, unless it’s the last resort” (LHD-18).
Influence of Governance Structure on Organizational Authorities
The range of authority available to LHDs was notably influenced by the governance structure within and surrounding the LHD. Different structures had noted tradeoffs. Interviewees from centralized state public health systems discussed how leaders at the state level (i.e., surgeon general, governor) often took the “fall” for negative criticism of public health policies, providing LHDs “a ton of protection” (LHD-18) against criticism at the local level. However, when state leadership did not approve of public health restrictions, these interviewees could not implement desired policies at the local level. Communication to the public was also stifled in centralized systems as LHDs had to align their messaging to what were sometimes perceived as limited “talking points that we were provided” (LHD-10). This alignment frustrated local media and community members as it both slowed down LHD communications and made their messaging less transparent.
Tradeoffs were also noted in LHD health districts (as opposed to single county or city jurisdictions). As a semiautonomous unit of government separate from county-specific affairs, districts were able to be a “center of the wheel . . . more of a neutral place” (LHD-12) when convening agencies. However, their geographic reach also created confusion, as community members “lump[ed] us in with the county complex” (LHD-19) when expressing their frustrations (similar tensions occurred in overlapping jurisdictions between city and county health departments). In addition, it was harder for health districts to coordinate with single-county agencies.
Across all governance structures, interviewees expressed frustration over how elected officials and community members misunderstood LHD policy-making authorities. These groups would either wish the LHD could do something that it did not have the power to do, or they would wish the LHD did not have the power to do what they did: “I think our community wondered from time to time, why is the Health Officer not making this decision?” (LHD-01). This misunderstanding was especially pronounced with mask and vaccine mandates. In response, LHD leaders had to refer to state statutes to defend their authorities (e.g., their power to issue and enforce mask mandates).
Strategic Use of Organizational Authorities
Depending on the values of other sectors, LHDs tailored their organizational authority across sectors and for different audiences within sectors. Although scientific authority was used consistently, LHDs leaned on other types of authority, particularly moral, with those that were more skeptical of science: . . . science kind of became a bad word here too, so I really felt like [we] needed to pull at people’s emotions . . . I always saw myself as that little nagging angel or devil on the mayor’s shoulder, just constantly nagging him behind the scenes about what’s right, that these are lives that we’re talking about . . . just saying we need to do what’s right for the community. (LHD-15)
At times, several LHDs mentioned leveraging their partner’s authority (often CBOs) if it would be more effective to advance the LHD’s values: Our role was data and evidence, but we had to be very careful about how we shared that and with whom we shared it, so that others could really push the message and not us . . . because we didn’t have a lot of that gravitas. (LHD-19)
LHDs strategically related their use of authorities in the context of COVID-19 to their use of similar authorities prior to the pandemic, when their work was less public and, in some cases, less stigmatized. Logistical authority was more consistently respected by the community. “We’ve been . . . orchestrating events like this for years at a smaller level . . . we’re really trusted on the logistical part of pulling people together . . .” (LHD-06). LHDs related their regulatory (or political) authority to restaurant health and safety inspections. “You expect public health to make sure that the people in the restaurant cook the food appropriately, that places [have] proper hygiene and sanitation . . .” (LHD-02).
Influence of LHD Values on Their Use of Organizational Authorities
LHD values strongly guided cross-sector work through their exercise of each organizational authority. Shared values, particularly professionalism and trust, were foundational to the successful use of all authorities. Trust was relied upon for effective data and evidence sharing (scientific authority), partnerships with community organizations (logistical authority), and communication with elected officials (political authority): “I think what went well is that [local public officials] trust us” (LHD-14). Furthermore, trust was critical to exercising moral authority, in which LHDs implored a shared value system: “. . . where you build moral authority is when you have a history of collaborating. . .‘We’ve worked with them. We trust them . . . Okay. We’ll give that [moral authority] to them’” (LHD-08). Furthermore, in describing moral authority, interviewees conveyed a sense of moral obligation to protect the health and safety of the community, despite challenges to their scientific authority: I took a lot of risks based on what I believed was the public health moral authority . . . when we were starting to really absorb . . . how many people were dying . . . it really pushed us that much more to stay on track and not get distracted. (LHD-16)
Health justice and equity manifested as a moral obligation to protect all members of the community. To this end, LHDs exercised their logistical authority to ensure access to resources (e.g., testing, vaccination), particularly for community members with marginalized identities. “. . . we were really focusing on who had access to testing, who had access to vaccines . . . how we were building relationships where people could trust us . . . knowing that there’s historical distrust there” (LHD-11). Within funding constraints, LHDs also exercised economic authority by funneling funding and grants to CBOs that were more embedded in the community than LHDs could be: “We’re giving money to those [community-based] organizations . . . because we can’t do that [vaccine outreach] work. We need them to do that work” (LHD-03). Partnerships with a wide range of community members illustrated the value placed on inclusivity and engagement: “So, it was just an ongoing bringing the partners to the table, so we were the convener, we were the educator, we’d try to be a collaborative equal partner and not tell them what to do . . .” (LHD-17).
Whereas interdependence and solidarity were not emphasized as frequently when interviewees discussed their LHD’s values, it was foundational to their use of moral authority. Interviewees implored organizations and community members to follow recommended safety protocols for the collective good. “. . . our efforts will be successful together, or we will not be successful together . . . I think subconsciously part of it was to make people realize that, honestly, we are all interconnected” (LHD-02). In contrast to this notion of interdependence and solidarity, an underlying emphasis on human rights and civil liberties surfaced in interviewees’ discussion of their scientific authority. Rather than mandating behavior, interviewees largely viewed their scientific authority as providing clear scientific information to the public and organizations to inform their own decisions in accordance with their own value system: “We are here in a catalyst facilitator type of mode, we’re telling you what the facts are, we’re here to answer your questions, we’re here to be transparent, but ultimately [the] decision is up to you” (LHD-02).
Discussion
COVID-19 has highlighted the role of LHDs in working with organizations in other sectors to collectively improve community health. By interviewing leadership from metropolitan LHDs across the United States, this study highlights how public health values and authorities were operationalized for cross-sector work. Although each authority and value we explored was present across all interviewees, how each shaped action varied. Internally, LHDs emphasized certain authorities more than others to the degree that they more closely aligned with prioritized core values. Externally, values and the implementation of authorities were influenced by surrounding political and governance contexts.
Given how COVID-19 has demonstrated and exacerbated long-standing health inequities by race, ethnicity, income, disability, immigration status, “essential” worker status, and geography (Lopez et al., 2021), our interviewees expressed the heightened priority of “health justice and equity” as a core public health value guiding their pandemic response. To actualize this value, interviewees developed diverse partnerships and served in distinct roles in those partnerships. This finding aligns with Public Health 3.0’s (PH3.0) recommendation that “public health departments should engage with community stakeholders—from both the public and private sectors—to form vibrant, structured, cross-sector partnerships” (DeSalvo et al., 2017). Failing to work with sectors beyond health care will only exacerbate inequities driven by social and economic factors (Dalsania et al., 2022). PH3.0 clearly outlines the need for LHDs to work cross-sector to advance health equity, whereas our findings illustrate how LHDs have done this during the greatest public health crisis in the past century. Particular emphasis was given to the importance of value alignment—including the ability to articulate both the values of public health and those of other sectors, and creatively seek opportunities to find synergy between these value systems whenever possible. While health equity may be the prevailing goal, working cross-sector requires LHDs to become fluent in discussing the importance and operationalization of other values, too. LHD leaders also emphasized the nuance with which organizational authorities are leveraged in cross-sector work, demonstrated by an active consideration for which authority best fits the context and ultimately suggesting a “multiple hats” approach depending on the sector of interest. Further training should be developed to assist LHD leaders in both identifying the range of these roles and knowing which “hat” is most appropriate, given specific cross-sector objectives.
When discussing cross-sector partnerships to advance health equity, the authors of PH3.0 acknowledge that “the basic foundational structure of local governmental public health may itself be a barrier to efficient and cost-effective coordination at the local level.” Our findings confirm and clarify the tradeoffs between alternative governance structures on the ability for LHDs to effectively work cross-sector. To minimize both confusion (at best) and unwarranted threats (at worst), public health practitioners must communicate with the public and elected leaders on how governance shapes the authorities they have in the community. Another core dimension of governance, as documented by our interviewees, concerns the proximity of LHD decision-making to elected officials. Different arrangements provide degrees of structural separation between an LHD’s decision-making and political pressures. More research is needed to understand how alternative governance arrangements influence the ability for LHDs to navigate the dichotomy between political involvement and administrative neutrality; in turn, additional training should be developed to assist LHD leaders and their elected officials with this navigation. Similarly, policies should be considered to limit governance models in which there is a disproportionate influence of politics on public health decision-making.
This study has limitations. Our interviewees worked within midsize, metropolitan LHDs. It is unclear whether the strategies and challenges they expressed translate to the experiences of smaller LHDs, especially those in rural communities. In addition, the specific values and authorities we explored may have distracted from other relevant values and authorities not included in our interview guide. For instance, it is unknown whether values outlined in the APHA Code of Ethics have been formally adopted by LHDs across the country, including the LHDs in our sample. Similarly, organizational authorities outlined in our interview guide were assembled by members of the research team based on their own review of cross-sector activity within public health. Additional research should assess whether our list represents an exhaustive characterization of public health authorities, including whether the authorities utilized by LHDs align with public administration scholarship on policy tools available to government agencies. Finally, our interview guide did not explicitly define a list of organizations from the local government, business, and CBO sectors, leaving room for slightly different interpretations among interviewees as to what these sectors constituted.
Collectively, our findings highlight the need for LHD leadership to effectively communicate public health values and the unique authorities by which health-supporting work can be facilitated, including how this message must be adapted depending on the specific sectors with which the LHD needs to partner and the governance arrangement in which the LHD is situated.
Supplemental Material
sj-docx-1-hpp-10.1177_15248399231192989 – Supplemental material for Local Health Department Values and Organizational Authorities Guiding Cross-Sector Work During COVID-19
Supplemental material, sj-docx-1-hpp-10.1177_15248399231192989 for Local Health Department Values and Organizational Authorities Guiding Cross-Sector Work During COVID-19 by Karl Johnson, Caitlin B. Biddell, Katherine Gora Combs, John Wiesman, Monica Valdes Lupi and Kristen Hassmiller Lich in Health Promotion Practice
Footnotes
Authors’ Note:
This research was supported in part by the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through Grant Award No. UL1TR002489 and by Cooperative Agreement No. NU38OT000297 from the Council of State and Territorial Epidemiologists (CSTE), and the Centers for Disease Control and Prevention (CDC). C.B.B. was additionally supported by an NCI Cancer Care Quality Training Program grant, University of North Carolina at Chapel Hill (UNC-CH), Grant No. T32-CA-116339. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH, CSTE, CDC, or the universities employing the researchers. One of the authors in this study, M.V.L., currently works for the Kresge Foundation. However, her work with the Kresge Foundation did not have any bearing on the individuals we were referred to nor her assistance with data analysis. This analysis was NOT an evaluation of the Emerging Leaders in Public Health Initiative (ELPH), which is supported by the Kresge Foundation. Interviewees were NOT asked about their experience participating in ELPH. Our sample of interviewees consisted of local health departments (LHDs) that had participated in ELPH, but recruitment was done with assistance from members of the National Program Office for ELPH, which is not located within the Kresge Foundation and is not staffed by Kresge Foundation employees. M.V.L. was recruited to assist with this article strictly based on her experience serving previously as a local public health director prior to her joining the Kresge Foundation. For the remaining authors, no funding sources or potential conflicts of interest were declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.