
Abstract
Mental Health Professionals (MHP) often harbor strong negative attitudes toward people with a sexual attraction to children, hindering the provision of essential treatment. This reluctance stems from pervasive stigmatization, contributing to mental health issues among people with pedophilia and exacerbating risk factors associated with child sexual abuse. Limited research and small sample sizes in prior studies underscore the need to conduct a meta-analysis, examining the effectiveness of educational interventions as a tool for reducing stigmatization toward people with pedophilia in MHP. Eight studies meeting specific inclusion criteria were identified through a literature search. These criteria included (a) peer-reviewed empirical, (b) quantitative data, (c) a focus on attitudes toward people with pedophilia, (d) a sample of MHP that might come in contact with people with pedophilia (or the general public), (e) the intervention is educational, (f) the educational intervention is based on people with pedophilia, (g) pre- and post-test data, and (h) be written in English. Comparable variables within these studies encompassed dangerousness, social distance, intentionality, deviance, punitiveness, anger, sympathy, and motivation to treat. The intervention significantly improved perceptions of dangerousness (d = 0.65), social distance (d = 0.33), intentionality (d = 0.38), and punitiveness (d = 0.77). However, it showed non-significant effects on deviance (d = 0.22), anger (d = −0.22), sympathy (d = −0.12), and motivation to treat (d = −0.04). These findings indicate that educational interventions can reduce MHP stigmatization toward people with pedophilia, especially with contact-based and sufficiently prolonged interventions.
Introduction
People with pedophilia are marked by a pervasive and profound level of stigmatization, evident not only within the general public (Combridge & Lastella, 2023; Elchuk et al., 2022; Imhoff, 2015; Jahnke et al., 2015a; Jahnke et al., 2015c; Jahnke, 2018b; Jimenez-Arista & Caldera, 2023; Lawrence & Willis, 2021; Stelzmann et al., 2022) but also among Mental Health Professionals (MHP; Harper et al., 2018; Jahnke, 2018b; Lasher & Stinson, 2017). This stigmatization persists irrespective of the presence or absence of a documented sexual offense against a child (Levenson et al., 2020; Maroño & Bartels, 2020; Maroño et al., 2023). For the purpose of this study, individuals who self-identify as pedophiles will be collectively referred to as people with pedophilia.
In the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association [APA], 2013), a clear distinction is drawn between pedophilic disorder and pedophilic sexual interest. Both conditions entail a primary or exclusive sexual attraction to prepubescent children, with the individual being at least 16 years old and at least 5 years older than the child. Additionally, they must have experienced “recurrent, intense sexually arousing fantasies, sexual urges, or behaviors involving sexual activity with a prepubescent child, for a minimum of six months” (APA, 2013, p. 697). The key differentiation between pedophilic disorder and pedophilic sexual interest is seen in the presence of severe distress or significant interpersonal difficulties which are essential for the diagnosis of pedophilic disorder. Despite this distinction, both terms share the commonality that an individual can be identified as a pedophile without the occurrence of any associated offense. However, emerging research suggests a correlation between pedophilia and an increased risk of sexually offending children (Beier et al., 2015; Blagden et al., 2018; Hanson & Bussière, 1998; Houtepen et al., 2016; Ischebeck et al., 2021; Jahnke et al., 2015c; Jahnke, 2018b; Levenson et al., 2020), underscoring the imperative for essential treatment. Moreover, the high level of stigmatization experienced by people with pedophilia contributes to exacerbated mental health issues (Blagden et al., 2018; Elchuk et al., 2022; Houtepen et al., 2016; Jahnke et al., 2015c; Lawrence & Willis, 2021; Stevens & Wood, 2019), further emphasizing the critical need for treatment. However, the reluctance of MHP to engage in the treatment of people with pedophilia due to prevailing stigmatization poses a significant challenge (Harper et al., 2018; Jahnke, 2018b; Lasher & Stinson, 2017; Levenson et al., 2020). This highlights the critical need to explore avenues for reducing MHPs’ stigmatization toward people with pedophilia and enhancing their willingness to provide treatment. Such efforts are essential not only for minimizing mental health challenges within the people with pedophilia community but also for mitigating the potential occurrence of future sexual offenses. The aim of the present study is, therefore, to investigate the effectiveness of educational interventions as a tool for reducing stigmatization toward people with pedophilia in MHP, using a meta-analysis.
Stigmatization of People with Pedophilia
The term “pedophile” is often used interchangeably with the term “child sexual offender” (Feelgood & Hoyer, 2008; Harper & Hogue, 2015; Jahnke et al., 2022; Stelzmann et al., 2022), despite empirical evidence revealing that over three quarters of individuals who sexually offend against children do not possess pedophilic tendencies (Blanchard et al., 2001; Kesicky et al., 2014; Schmidt et al., 2013; Seto, 2018; Seto & Lalumière, 2001). Instead, such offenses are often committed due to factors such as fear of sexual relationships with adults and limited social skills in heterosocial interactions (Sigre-Leirós et al., 2015). For instance, Seto and Lalumière (2001) and Kesicky et al. (2014) found that only 27% and 16.2% of offenders, respectively, demonstrated a sexual interest in prepubescent children. On the other hand, Braveheart (2024), reported that only 5% of Australian men who have committed sexual offenses against children acknowledge having sexual feelings toward them. Consequently, people with pedophilia constitute a minority among those who sexually offend against children. It is also important to note that the actual prevalence of pedophilia may be underreported and remains largely unknown due to factors such as undiagnosed cases and a lack of self-reporting. Recognizing this distinction could potentially contribute to stigma reduction (Grady et al. 2019; Houtepen et al. 2016; Imhoff, 2015; Jahnke et al. 2022; Jahnke et al. 2015a) and warrant further investigations to yield more generalizable conclusions.
Previous research has systematically examined the dimensions of stigmatization directed toward people with pedophilia. These dimensions encompass perceptions of dangerousness, social distance, intentionality, deviance, punitiveness, anger, and sympathy (Harper et al., 2018, 2022; Imhoff, 2015; Lawrence & Willis, 2022; Snethen & Warman, 2018). Dangerousness involves individuals’ assessments of the potential threat posed by people with pedophilia, through the fear of them engaging in child sexual offending. Social distance measures the willingness of individuals to socially engage with and accept people with pedophilia. Intentionality explores beliefs regarding the control people with pedophilia have over their sexual urges and the perceived choice associated with their attraction to children. Deviance evaluates the extent to which individuals perceive people with pedophilia as different from the general population. Punitiveness gauges individuals’ inclinations to advocate for punitive measures against people with pedophilia, regardless of any indication of criminal behavior. The dimensions of anger and sympathy assess individuals’ emotional responses when contemplating people with pedophilia.
By dissecting stigmatization toward people with pedophilia into multifaceted dimensions, a more nuanced understanding of the various factors contributing to stigmatization emerges. This approach has the potential to offer insights crucial for tailoring effective educational interventions.
Consequences of Stigmatization
Stigmatization has been identified as a significant factor contributing to various mental health issues among people with pedophilia (Blagden et al., 2018; Elchuk et al., 2022; Houtepen et al., 2016; Jahnke et al., 2015c; Lawrence & Willis, 2021; Stevens & Wood, 2019). For instance, Jahnke et al. (2015c) conducted an online survey involving German males (N = 104) who self-identified as pedophiles. In this study, 64% of participants assumed that the German general public held a negative view of them. This assumption led to social distancing behaviors, as people with pedophilia feared public discovery of their sexual interest in children, resulting in higher reported levels of loneliness (Jahnke et al., 2015c). Another study, examining mental health issues related to having a sexual interest in children, found elevated rates of addiction (13%), anxiety (18%), depression (16%), self-harm/self-hatred/suicide (30%), and various other mental disorders (23%) among people with pedophilia (Stevens & Wood, 2019). These mental health challenges were attributed to the fear of discovery of their sexual interest, apprehension of violence toward them, concerns about finding an age-appropriate partner, guilt associated with morally conflicting thoughts, and subsequent suicidal ideation and attempts (Stevens & Wood, 2019). Furthermore, stigmatization also contributes to people with pedophilia being reluctant to seek professional help, partly due to stigmatizing perceptions from MHP, noting a fear of being stigmatized, judged, and/or reported (Grady et al., 2019; Houtepen et al., 2016; Levenson & Grady, 2018; Levenson et al., 2017).
The pervasive mental health issues experienced by people with pedophilia underscore the critical need to reduce stigmatization and provide effective, high-quality treatment. Therefore, it is pertinent to examine MHPs’ attitudes toward people with pedophilia and their willingness to engage in the treatment of this population. Understanding and addressing MHPs’ perspectives can be pivotal in developing interventions that facilitate a more supportive and therapeutic environment for individuals grappling with pedophilic tendencies. Such efforts are essential not only for enhancing the mental well-being of people with pedophilia but also for mitigating the potential risks of sexual crimes associated with their condition, ultimately fostering a safer and more inclusive society.
Attitudes from MHPs
Research indicates that a significant number of MHPs exhibit reluctance in treating people with pedophilia, often stemming from a lack of knowledge about this population and the specific treatment they require (Levenson et al., 2020; Lievesley et al., 2022; Martinec Nováková et al., 2023; Parr & Pearson, 2019; Schmidt & Niehaus, 2022). For instance, a Swiss study revealed that 97.6% of the MHPs without previous experience in treating people with pedophilia, reported to lack of specific treatment skills (Schmidt & Niehaus, 2022). Similarly, another study identified a lack of adequate formal education and/or training as the second most significant reason behind MHPs’ reluctance to treat people with pedophilia (Martinec Nováková et al., 2023). This is particularly noteworthy considering that offense-specific, group-based psychotherapeutic treatment conducted by qualified psychologists has been established as an effective preventive measure for reducing the occurrence of future child sexual abuse (Beier et al., 2015; Gannon et al., 2019; Garcia et al., 2013; Kear-Colwell & Boer, 2000; Mokros & Banse, 2019).
The evidence highlights the crucial need for MHPs to receive comprehensive education and/or training about people with pedophilia. Such initiatives are vital not only for addressing the knowledge gaps among MHPs but also for fostering a more informed and empathetic approach to the treatment of people with pedophilia. By providing MHPs with the necessary tools and insights, the broader objective is to reduce stigmatization and enhance their willingness to engage in the treatment of people with pedophilia.
Educational Interventions as Stigma Reduction
Previous studies have suggested that educational interventions can be effective in diminishing stigmatization toward individuals with mental disorders (Dalky, 2012) and people with pedophilia (Harper et al., 2018, 2022; Lawrence & Willis, 2022). A systematic review by Dalky (2012) revealed that contact-based interventions, involving direct or indirect interactions with stigmatized individuals through methods like videos, were notably more effective than web-based and computer-assisted educational programs. Specifically, the work of Harper et al. (2018) and Harper et al. (2022) indicated that both narrative and informative interventions proved effective in reducing individuals’ punitive attitudes and stigmatization toward people with pedophilia (with the exception of the variable deviance). This underscores the significance of interventions, particularly for MHPs who may regularly encounter stigmatized individuals such as people with pedophilia.
The findings suggest that interventions involving narratives and informational content can contribute significantly to altering attitudes and reducing stigmatization. Tailoring such interventions for MHPs is particularly relevant, given their potential to come into direct contact with individuals facing stigma, including people with pedophilia.
The Present Study
The existing body of research underscores that people with pedophilia often contend with various mental health issues (Blagden et al., 2018; Elchuk et al., 2022; Houtepen et al., 2016; Jahnke et al., 2015c; Lawrence & Willis, 2021; Stevens & Wood, 2019). Left untreated, these mental health challenges may potentially escalate to child sexual abuse (Beier et al., 2015; Blagden et al., 2018; Hanson & Bussière, 1998; Houtepen et al., 2016; Ischebeck et al., 2021; Jahnke et al., 2015a, 2015c; Jahnke, 2018b; Levenson et al., 2020). Recognizing therapy as a preventive measure against offending, it becomes imperative to prioritize therapeutic interventions for people with pedophilia. However, MHPs often harbor negative attitudes toward people with pedophilia and may lack the necessary treatment skills, resulting in reluctance to provide efficient therapy (Levenson et al., 2020; Lievesley et al., 2022; Martinec Nováková et al., 2023; Parr & Pearson, 2019; Schmidt & Niehaus, 2022). This underscores the critical need to explore effective strategies to reduce stigmatization and enhance MHPs’ willingness to treat people with pedophilia.
The present study aims to provide insights into the efficacy of interventions in reducing stigmatization toward people with pedophilia among MHPs. Two separate meta-analyses were conducted—one focusing solely on MHPs and another including both MHPs and the general public to increase generalizability and achieve a more precise estimate of the effectiveness of the interventions (Wolf, 2015). The study hypothesizes that:
H1: Educational interventions about people with pedophilia will significantly reduce MHPs’ stigmatization (dangerousness, social distance, intentionality, deviance, punitiveness, anger, sympathy), and this effect will increase when data on the general public is added.
H2: Educational interventions will enhance MHPs’ motivation to treat people with pedophilia.
Methodology
Literature Search
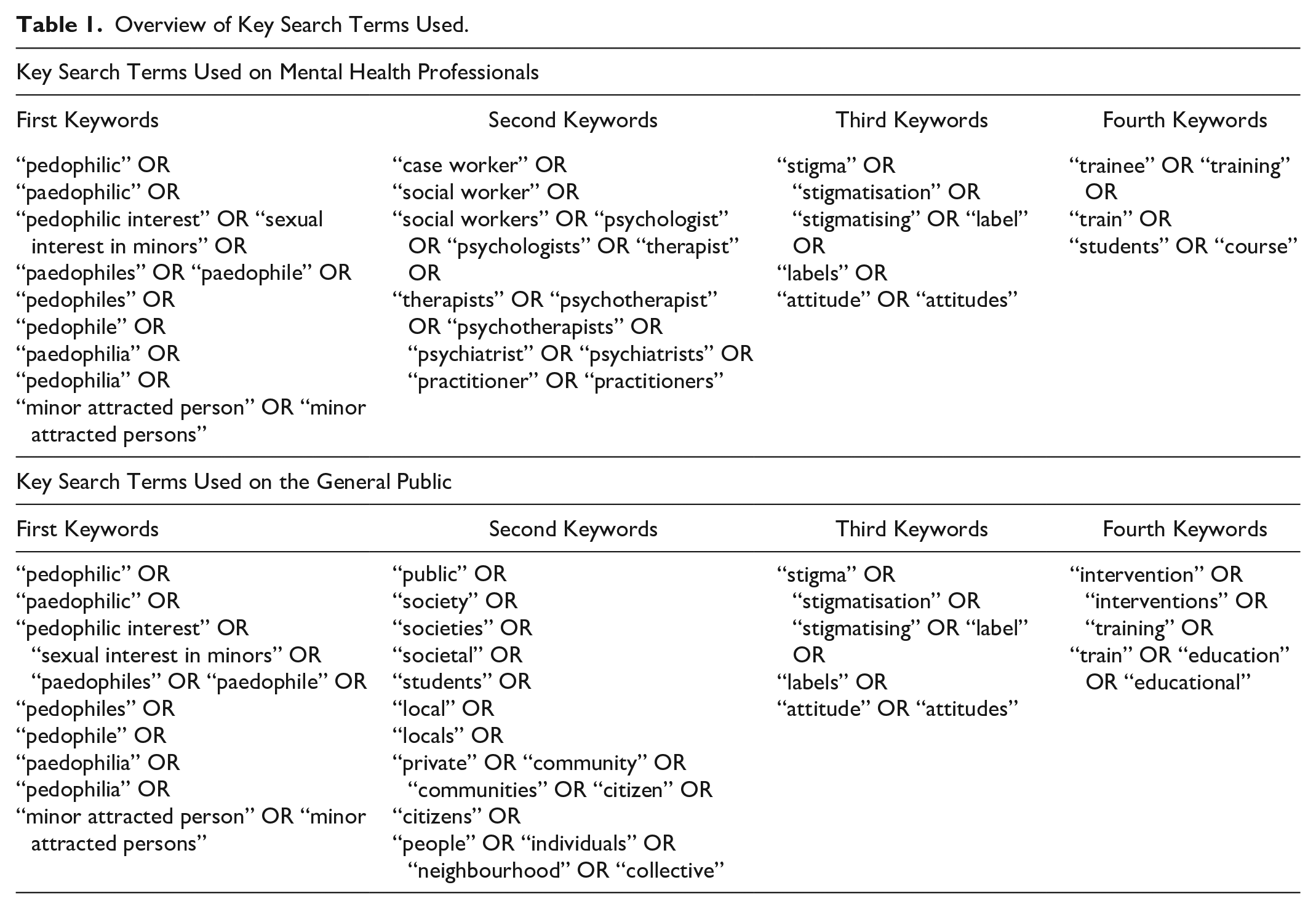
A literature search was conducted in August 2023, utilizing the University Library, PubMed, and ProQuest. Data were limited to primary original research and case studies published in peer-reviewed journals to ensure reliability and quality. No limit was imposed on publication dates for any of the databases. The key search terms used to explore these databases are displayed in Table 1.
Overview of Key Search Terms Used.
Separately, the two authors assessed the studies, which had been selected for potential eligibility, in full text and screened for the selected inclusion criteria. Four studies for MHPs and four for the general public were deemed eligible, respectively. Two PRISMA diagrams were produced to provide a visual of the search and review of studies (see Figure 1).
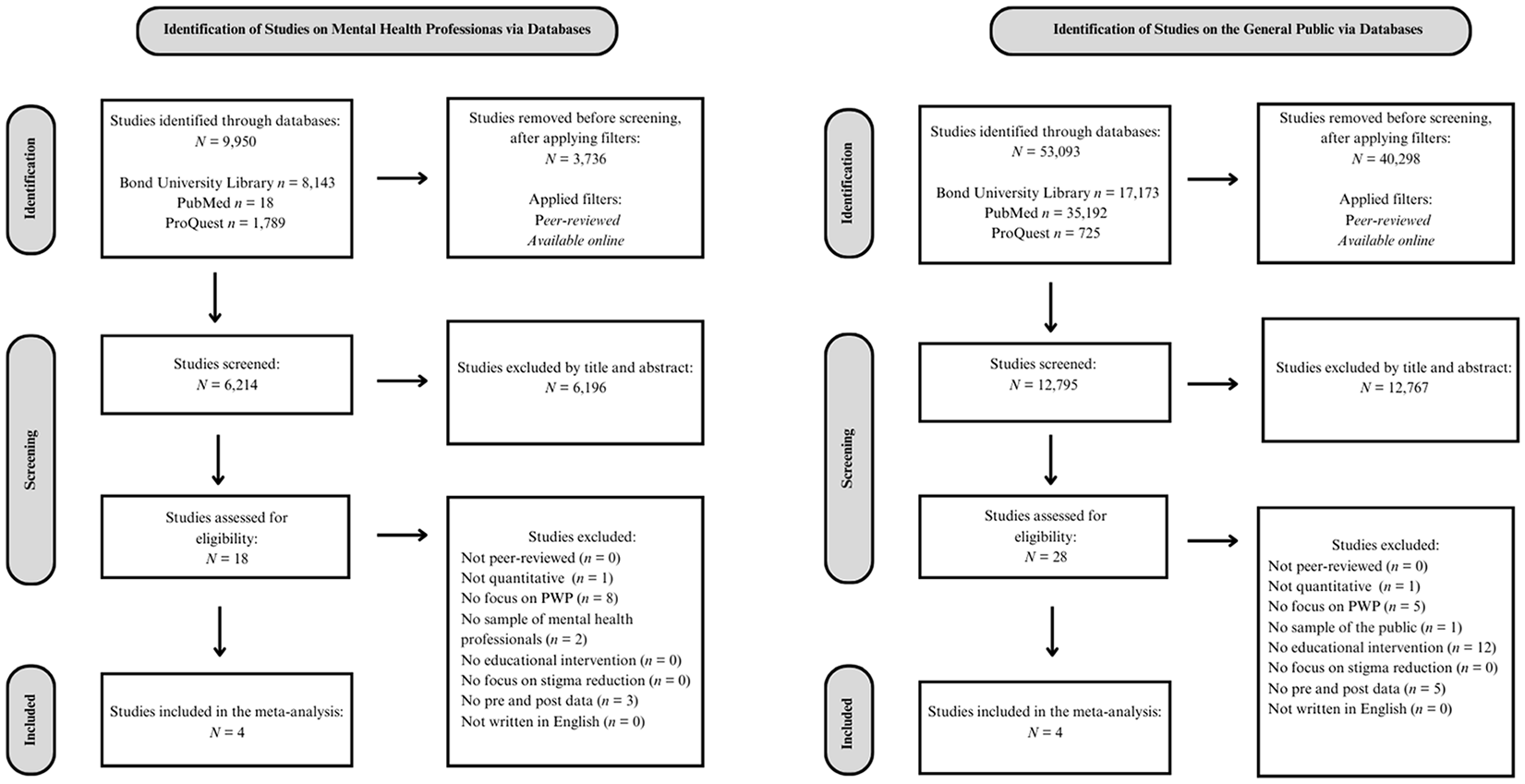
PRISMA diagram of the procedure for selecting the included studies in the meta-analysis.
Inclusion Criteria
Studies eligible for the current meta-analysis were required to contain the following criteria: (a) peer-reviewed empirical, (b) quantitative data, (c) a focus on attitudes toward pedophiles, (d) a sample of MHPs that might come in contact with pedophiles (or the general public), (e) the intervention is educational, (f) the educational intervention is based on pedophiles, (g) pre- and post-test data, and (h) be written in English.
Data Collection
A data collection table was made to create a better overview of each included study for both MHPs and the general public. The data collection table included information on (a) the study IDs, (b) the country in which the study was conducted, (c) the age of the participants, (d) the sample sizes, (e) the occupations of the participants, (f) the type of educational intervention, and (g) the variables measured (see Table 2).
Overview of Included Studies in Both Meta-Analyses.
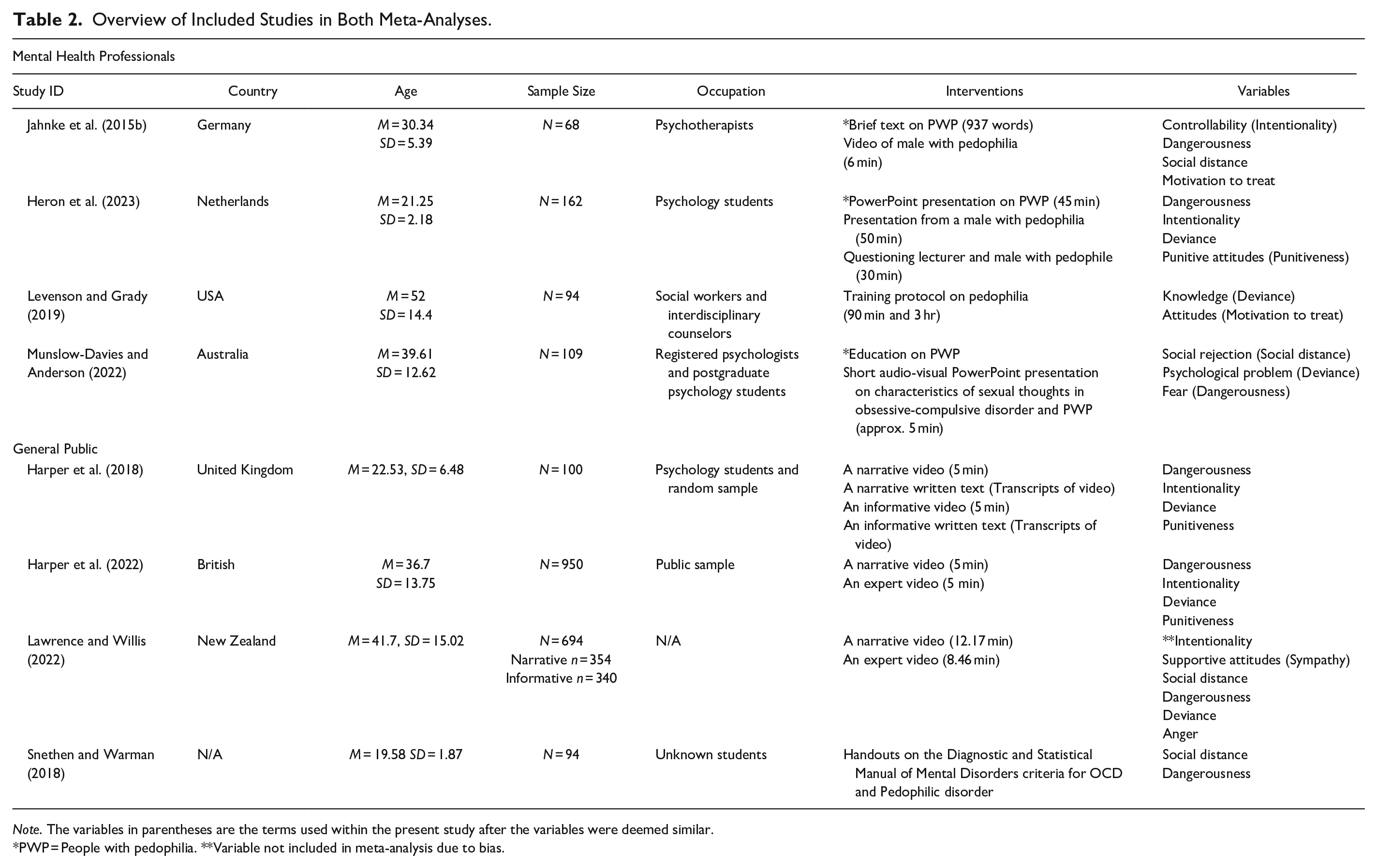
Note. The variables in parentheses are the terms used within the present study after the variables were deemed similar.
PWP = People with pedophilia. **Variable not included in meta-analysis due to bias.
Initially, the sample sizes, means, and standard deviations for each comparable variable in the included studies were identified, extracted, and added to an Excel sheet. Then JASP Version 0.18.0, Amsterdam, Netherlands was harnessed to conduct the meta-analyses where it, for each variable, computed the p-value, 95% Confidence Interval (CI), forest plots, funnel plots, and a regression test for funnel plot asymmetry (Egger’s test). The funnel plot displays whether the included studies are symmetrically scattered around the overall effect size—asymmetry and deviations from the overall effect size suggest publication bias, which is commonly seen in smaller studies (Kossmeier et al., 2019). Because there was only very limited number of studies for the MHP it was decided to also include the general public to increase power.
Heterogeneity Testing and Risk of Bias Assessment
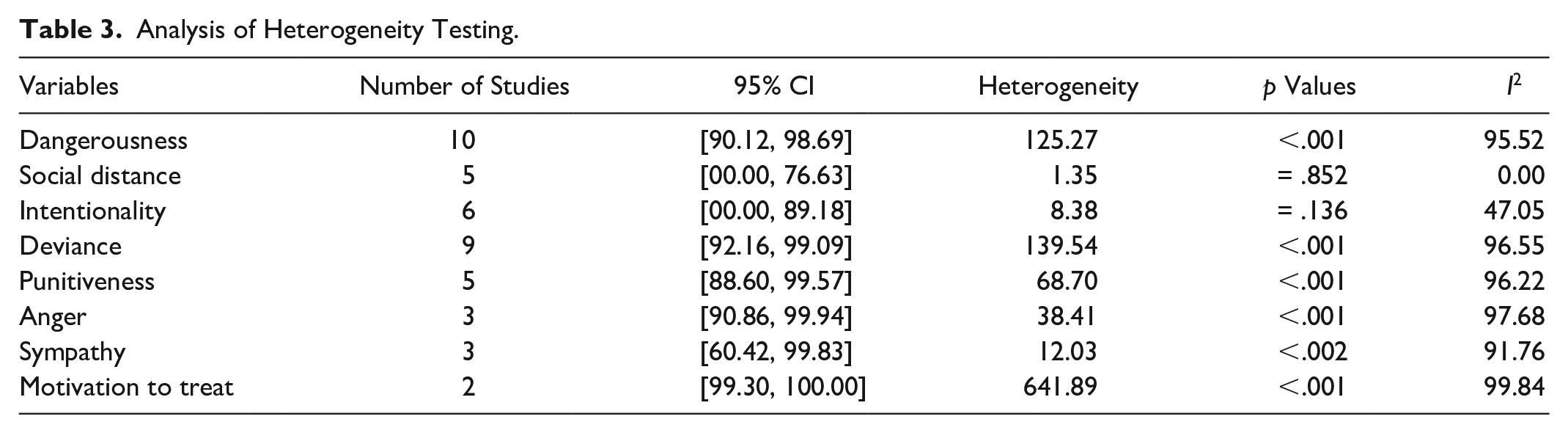
Residual heterogeneity was tested using Cochrane’s Q statistic to examine if the included studies were measuring the same effect (see Table 3). The level of heterogeneity can also partly determine the difficulty in drawing overall conclusions (Higgins & Thompson, 2002). The online software JASP was used to calculate the percentage of I2. A categorization of the value of I2, being as follows: 0% no heterogeneity, 25% low heterogeneity, 50% moderate heterogeneity, and 75% high heterogeneity was used (Higgins et al., 2003).
Analysis of Heterogeneity Testing.
It is important to assess the risk of bias, as biases can lead to under- or over-estimations of the actual effect of the measured educational interventions (Boutron et al., 2019). To assess the potential risk of bias in the included studies, 12 items that could indicate bias were identified. The 12 items were consistent with previous meta-analyses. If an item was present in a study, it was given a value of 1. If the item was absent, it was given a 0. Therefore, cumulative scores were ranging from 0 to 12, where 12 indicated the lowest risk of bias. The Risk of Bias Assessment was conducted independently by the two authors to ensure the minimization of errors in the assessment (Higgins et al., 2019) and increase inter-rater reliability. The individual assessments were then discussed in unison to find consensus on any disagreements. The total score for each included study on MHPs ranged between 6 and 8 (M = 7.0), making the overall risk of bias below average. For the included studies on the general public, scores ranged between 8 and 12 (M = 10.0), indicating low risk of bias (see Table 4).
Risk of Bias Assessment of Included Studies on Mental Health Professionals and the General Public.
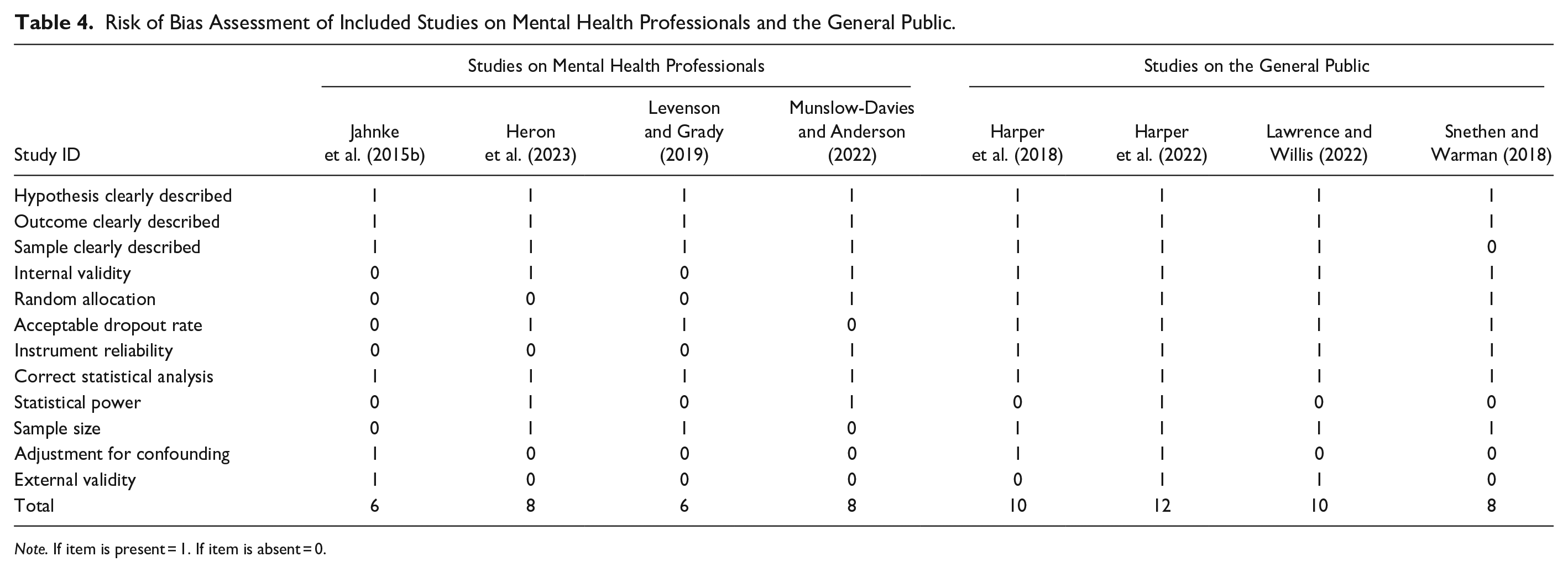
Note. If item is present = 1. If item is absent = 0.
Results
Meta-Analyses
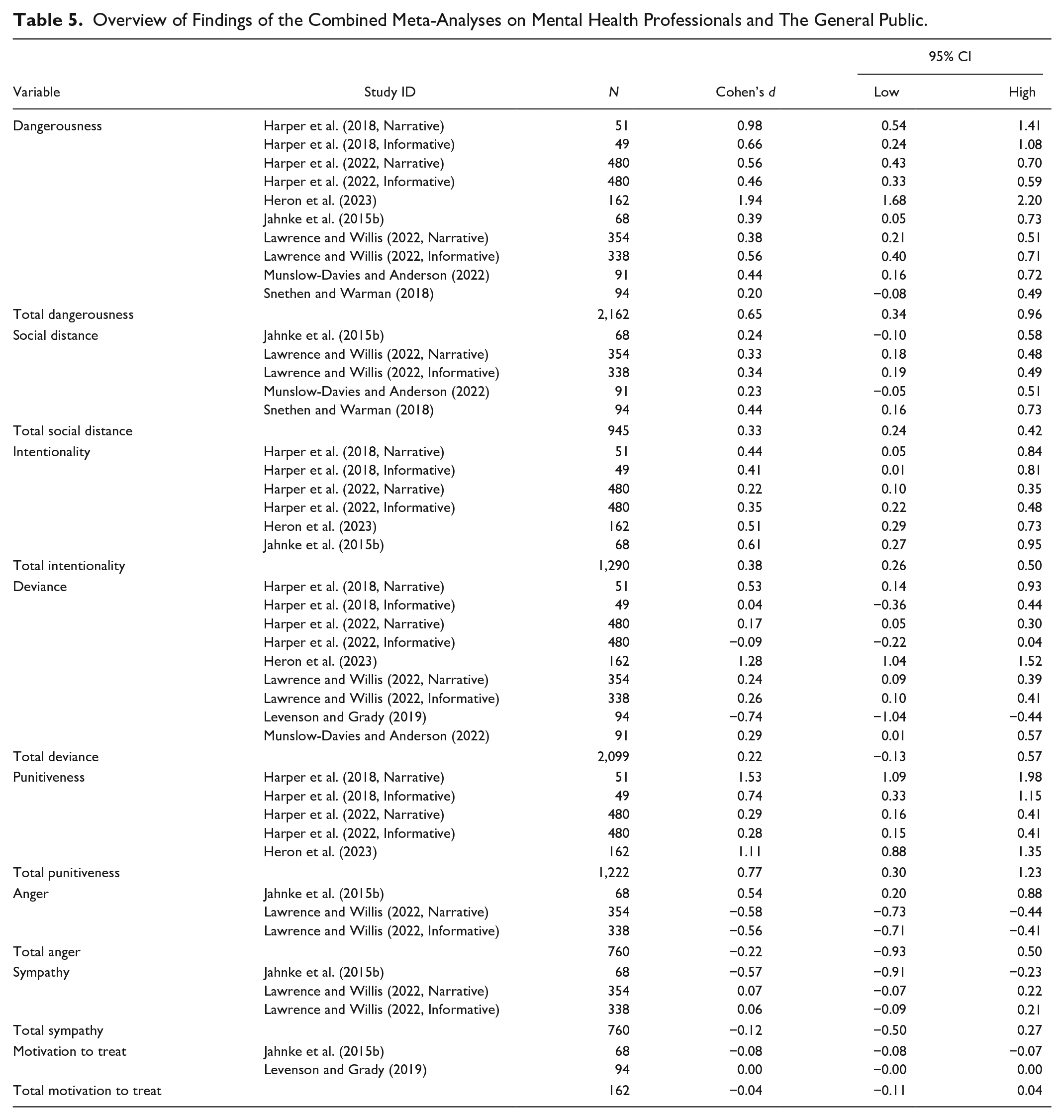
The results will be presented in the order of each variable (dangerousness, social distance, intentionality, deviance, punitiveness, anger, sympathy, and motivation to treat). Within each variable, the results for the MHP will be presented first, followed by the results for the MHP and public combined with a corresponding forest plot. A summary table of all results is presented at the end (see Table 5).
Overview of Findings of the Combined Meta-Analyses on Mental Health Professionals and The General Public.
Dangerousness
The meta-analysis for dangerousness depicted a significant effect of the combined studies on MHPs z = 3.34, p < .001, with a medium effect size, (d = 0.60) 95% CI [0.25, 0.95] (Cohen, 1988), implying a significant difference between pre- and post-test intervention scores. When adding the studies on the general public, it showed a significant result z = 4.13, p < .001 (See Figure 2). The corresponding forest plot produced a medium effect size, (d = 0.65) 95% CI [0.34, 0.96] (Cohen, 1988).
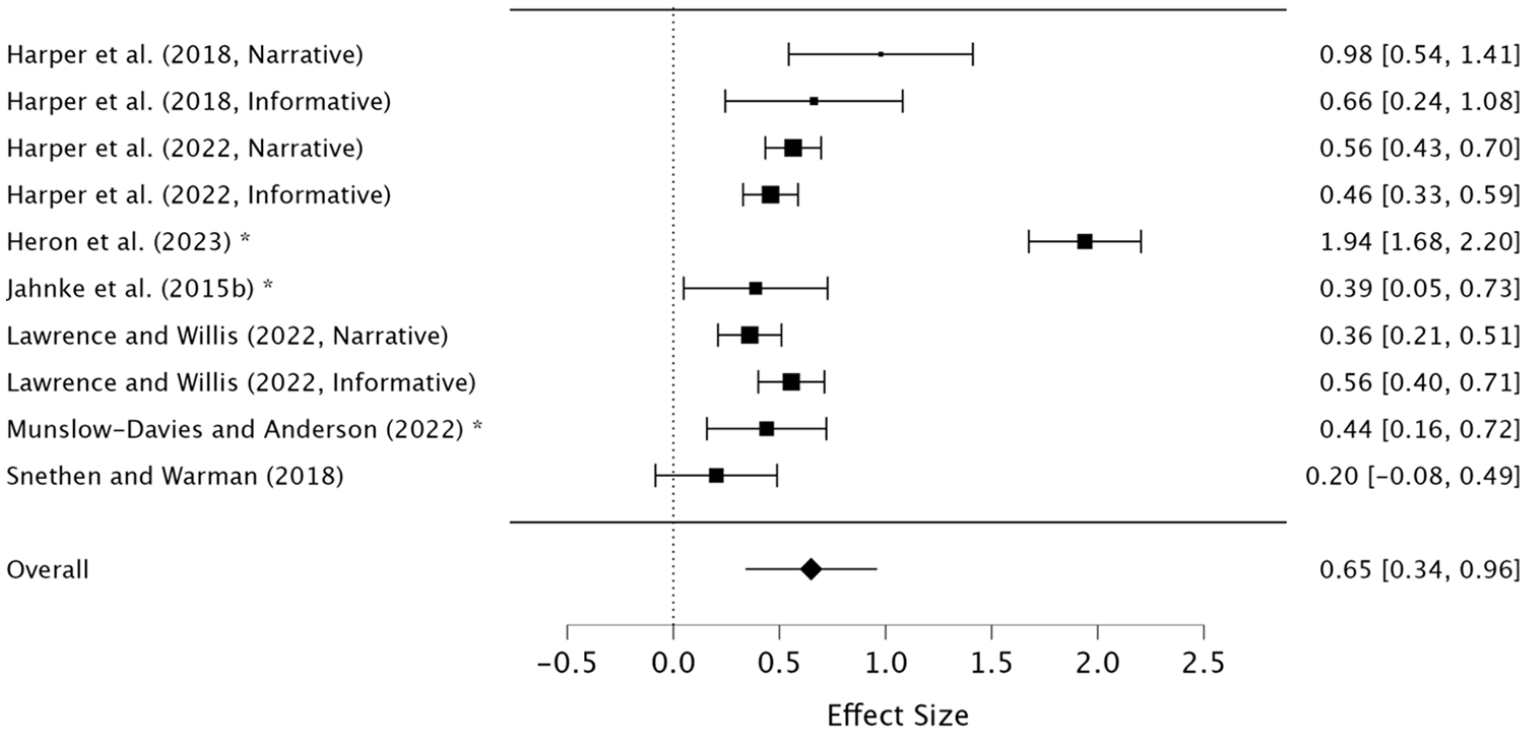
Forest plot: meta-analysis of dangerousness.
Social Distance
The meta-analysis on MHPs showed a significant effect on social distance z = 2.79, p = .005, with a small effect size (d = 0.31) 95% CI [0.09, 0.52] (Cohen, 1988). When adding the public, the meta-analysis produced a significant effect z = 7.09, p = .001, with a small effect size (d = 0.33) 95% CI [0.24, 0.42] (Cohen, 1988), indicating higher significance when increasing the number of studies (See Figure 3).
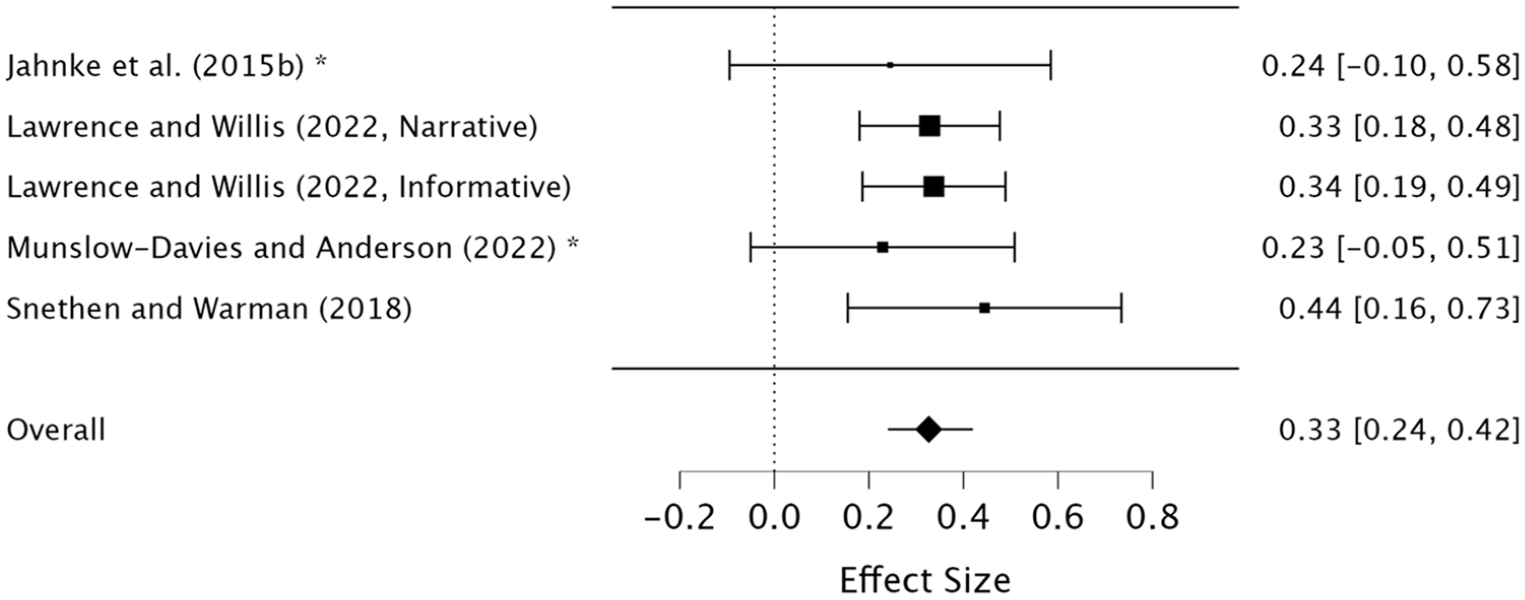
Forest plot: meta-analysis of social distance.
Intentionality
The meta-analysis on MHPs showed a significant effect z = 5.70, p < .001, with a medium effect size, (d = 0.54) 95% CI [0.35, 0.73] (Cohen, 1988). When adding the studies on the general public to the meta-analysis on intentionality, it continued to show a significant effect z = 6.00, p < .001; however, now with a small effect size, (d = 0.38) 95% CI [0.26, 0.50] (Cohen, 1988) (See Figure 4).
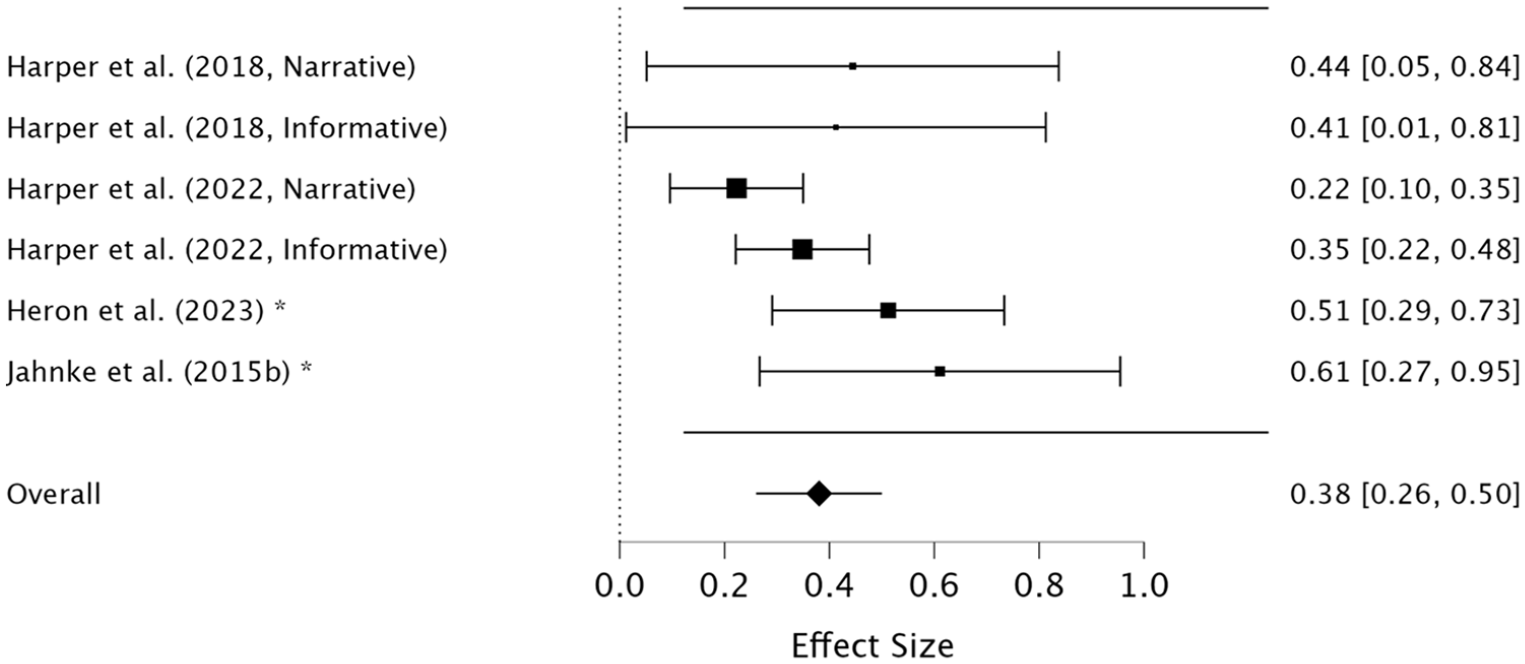
Forest plot: meta-analysis of intentionality.
Deviance
This meta-analysis presented a non-significant result on MHPs z = 0.48, p = 0.631, with a small effect size, (d = 0.28) 95% CI [−0.86, 1.42] (Cohen, 1988), implying no significant difference between pre- and post-test intervention scores. Despite adding the general public, the meta-analysis still produced a non-significant result z = 1.25, p = 0.21, with a small effect size, (d = 0.22) 95% CI [−0.13, 0.57] (Cohen, 1988; See Figure 5).
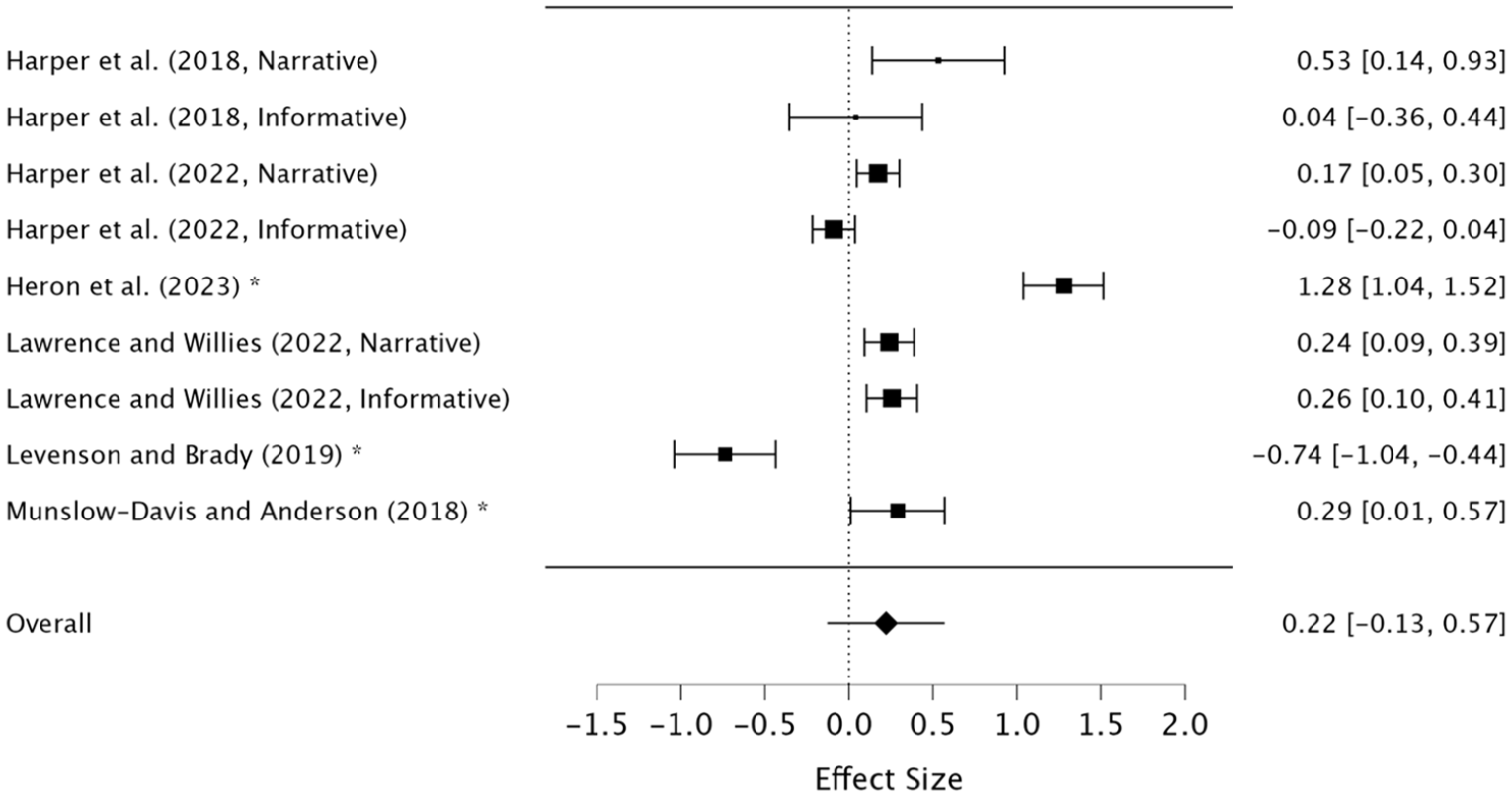
Forest plot: meta-analysis of deviance.
Punitiveness
As there was only one study on MHPs that had measured punitiveness, it was not possible to conduct two separate meta-analyses. However, when adding the studies on the general public to the meta-analysis on punitiveness, it presented a significant result z = 3.20, p < .001, with a medium effect size, (d = 0.77) 95% CI [0.30, 1.23] (Cohen, 1988), indicating educational interventions might have a significant effect in changing MHPs’ punitive attitudes toward PWP (See Figure 6).
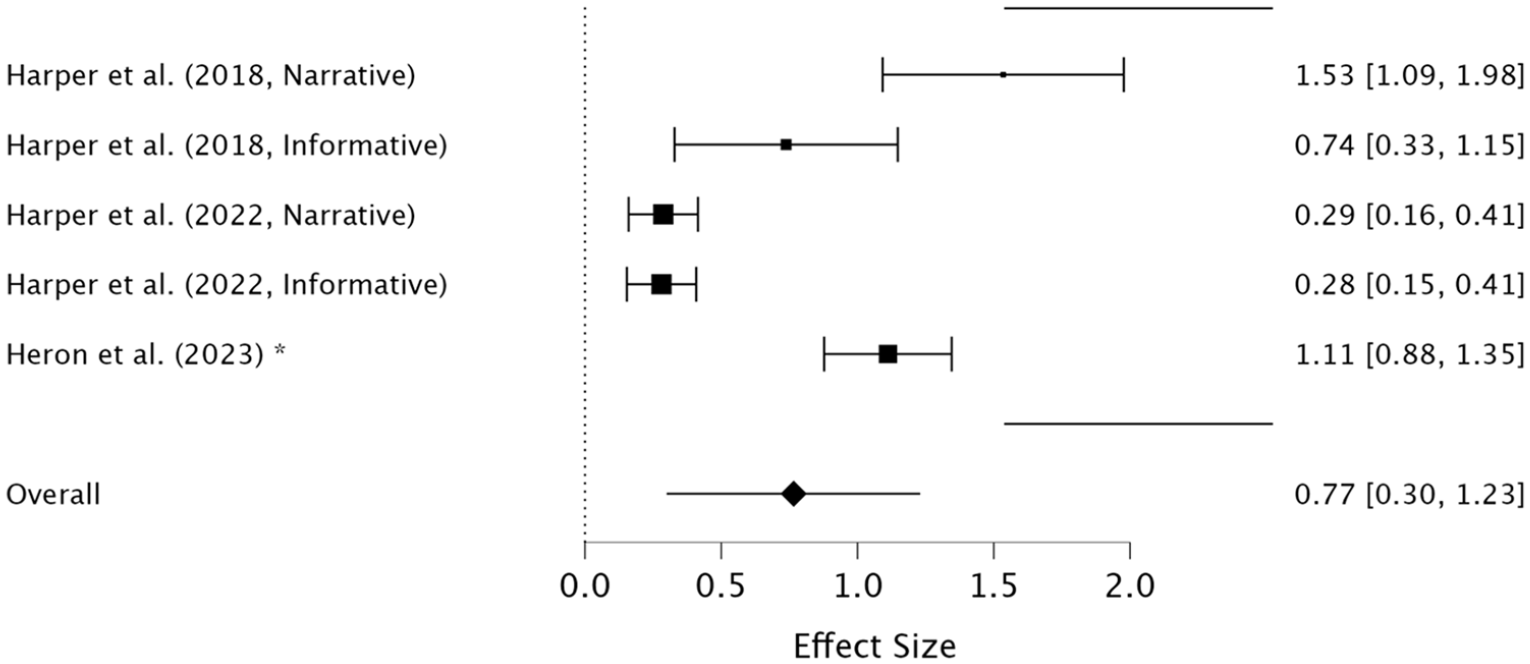
Forest plot: meta-analysis of punitiveness.
Anger
It was not possible to conduct two separate meta-analyses, as only one study measured anger on MHPs. When adding the studies on the general public it showed a non-significant result z = −0.60, p = .552, with a negligible effect size, (d = −0.22) 95% CI [−0.93, 0.50] (Cohen, 1988; See Figure 7).
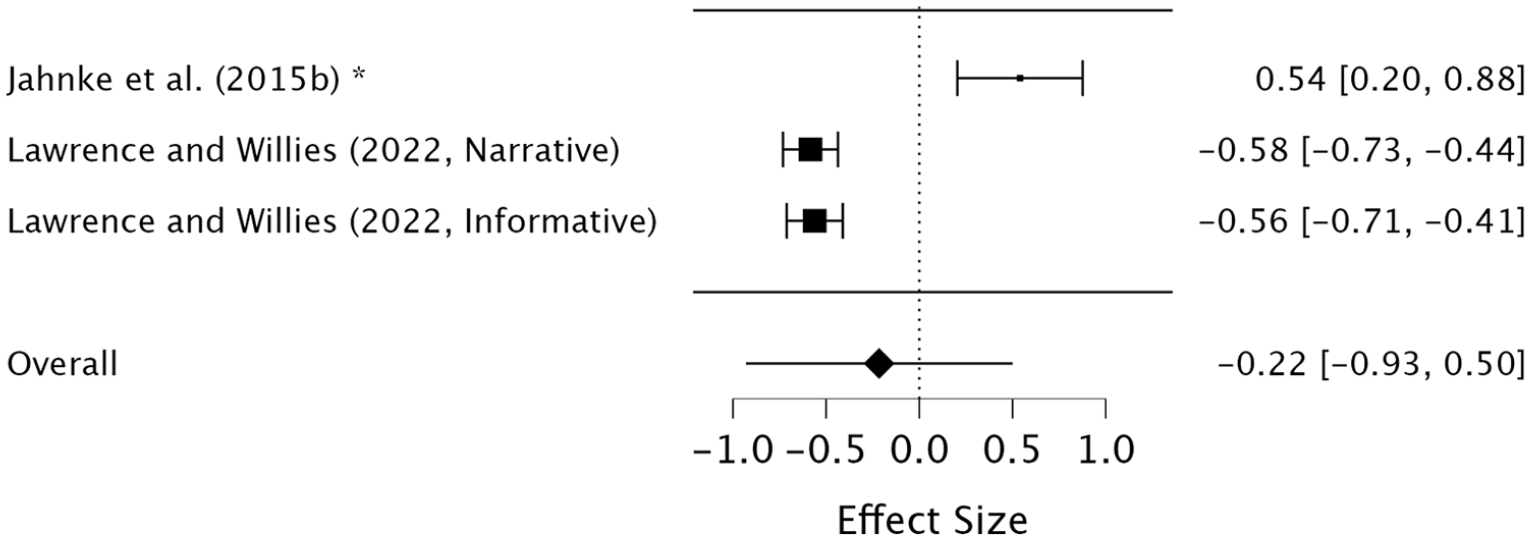
Forest plot: meta-analysis of anger.
Sympathy
It was not possible to conduct two separate meta-analyses, as only one study measured sympathy on MHPs. When adding the studies on the general public to the meta-analysis, it displayed a non-significant result z = −0.60, p = .548, and a negligible effect size, (d = −0.12) 95% CI [−0.50, 0.27] (Cohen, 1988; See Figure 8).
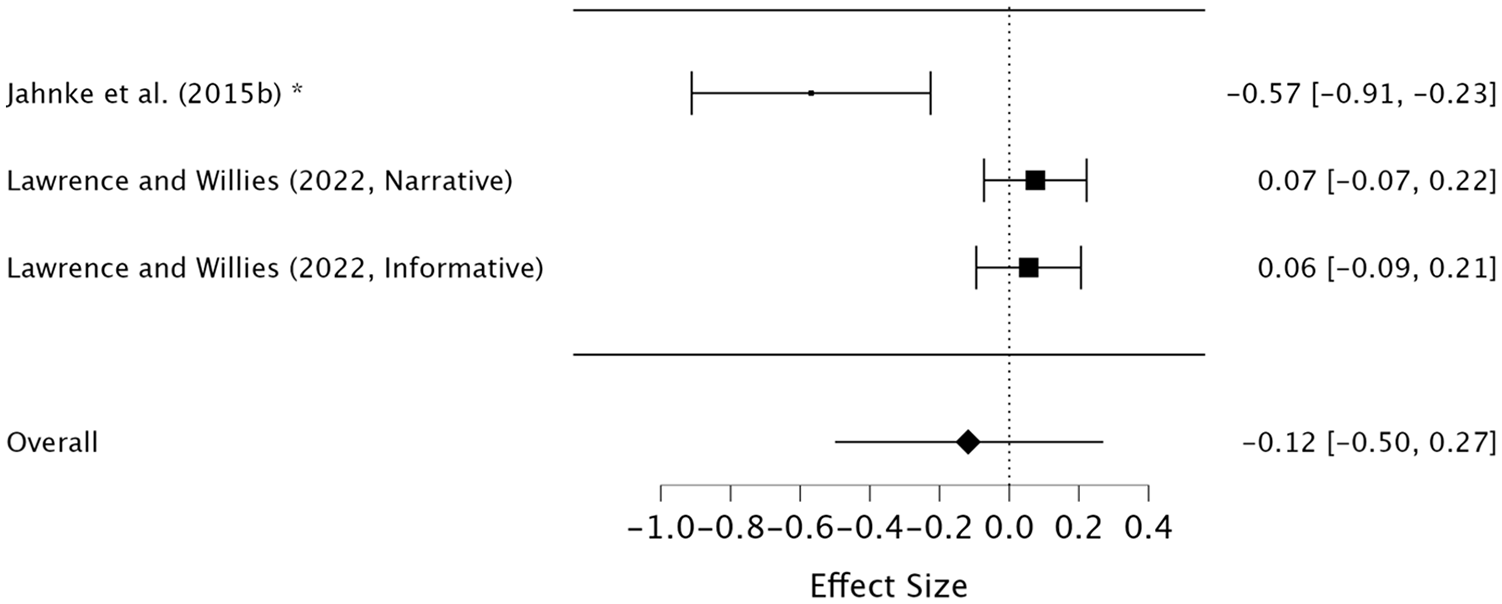
Forest plot: meta-analysis of sympathy.
Motivation to Treat
The meta-analysis showed a non-significant effect on motivation to treat z = −0.99, p = .318. With a negligible effect size, (d = −0.04) 95% CI [−0.11, 0.04] (Cohen, 1988; See Figure 9).
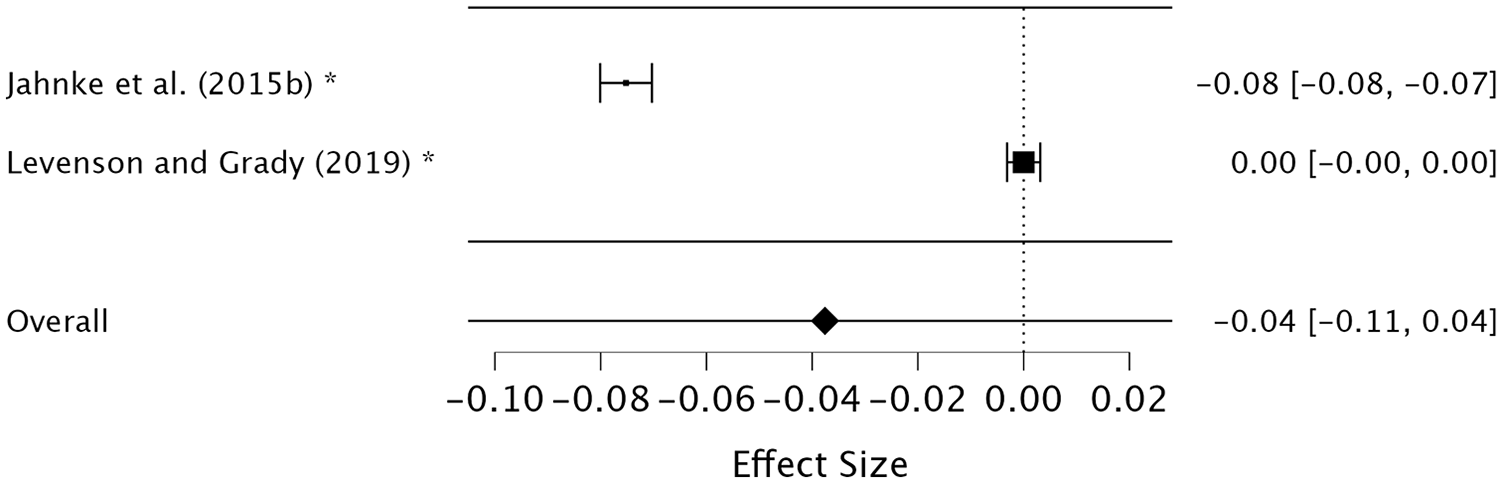
Forest plot: meta-analysis of motivation to treat.
Discussion
The purpose of the present study was to examine whether educational interventions on people with pedophilia would be effective in reducing stigmatization toward these individuals among MHPs and consequently make MHPs more willing to treat them. It was therefore hypothesized that (H1) educational interventions about people with pedophilia would significantly reduce MHPs’ stigmatizations of them, and this effect would increase when data on the general public was added, and (H2) educational interventions would enhance MHPs’ willingness to treat people with pedophilia. The results of the present study found that the first hypothesis was partially supported, as the intervention significantly improved perceptions related to dangerousness, social distance, intentionality, and punitiveness, with effect sizes ranging from small to medium. However, it showed non-significant effects on deviance, anger, and sympathy. The second hypothesis was not supported, as the scores on MHPs’ motivation to treat people with pedophilia did not increase post-interventions.
Significant results were found across several key areas, indicating that educational intervention can help improve MHPs’ stigmatizing perceptions, highlighting the importance of awareness and education. Dangerousness assesses MHPs’ perception of the potential threat posed by individuals with pedophilia, specifically the fear of them committing child sexual abuse. Punitiveness assesses whether MHPs hold punitive attitudes toward people with pedophilia. Research indicates that people with pedophilia often hesitate to seek professional help due to the fear of being rejected and stigmatized (Grady et al., 2019; Houtepen et al., 2016; Jackson, 2022; Levenson & Grady, 2018; Levenson et al., 2017). Therefore, significant results in these areas are crucial, as individuals with pedophilia might be more inclined to seek help if MHPs do not equate pedophilia with child sexual abuse or believe they should be punished. Regarding pedophilia, a study by Jahnke (2018a) shows that the public has a desire to socially distance themselves despite having the knowledge of the individual being non-offending. Increased social distance is associated with heightened discrimination and prejudice against those with mental disorders (Baumann, 2007; Toner et al., 2018). Social distance is viewed as an indicator of negative attitudes toward individuals with mental disorders, reflecting the varying degrees of willingness to engage in relationships with them (Jorm & Oh, 2009; Salunkhe et al., 2022; Toner et al., 2018). Therefore, a significant result for this variable is highly relevant as professional relationships are important for effective therapy (Ardito & Rabellino, 2011; Kornhaber, 2016; Mottram, 2009). Intentionality measures beliefs about whether people with pedophilia can control their sexual urges and refrain from offending. The significant results for intentionality are important because if MHPs recognize that some individuals with pedophilia can control themselves, it suggests that these individuals can be helped in remaining offense-free. On the other hand, the educational interventions did not have significant outcomes on some variables, which might be due to the limited number of studies included, the type of interventions, and the duration which were between 6 and 12 min.
Upon completing the meta-analysis, the authors recognized the critical importance of the results, not only in measuring the pre- and post-intervention effects on various variables but also in identifying the most effective components within the interventions aimed at changing MHPs perceptions of individuals with pedophilia. Consequently, it is imperative to examine certain included studies individually to draw more robust conclusions regarding the most effective aspects of educational interventions.
The primary objective of this paper was to assess whether educational interventions are an effective means of reducing MHPs’ stigmatization of individuals with pedophilic tendencies, thereby increasing their motivation to provide treatment. Only two studies, Jahnke et al. (2015b) and Levenson and Grady (2019), created interventions with the purpose of increasing MHPs’ motivation to treat people with pedophilia. As it has been ascertained that two studies are acceptable when conducting a meta-analysis if the results are pooled meaningfully (Ahn & Kang, 2018), it is worthwhile to look at these two studies individually and examine their type of intervention. The interventions’ impact on motivation to treat was non-significant, with Jahnke et al. (2015b) even demonstrating a negative effect. However, it is noteworthy that Jahnke et al. (2015b) was quite successful in altering MHPs’ attitudes on other variables between pre- and post-intervention. A closer examination of the components used in Jahnke et al.’s (2015b) intervention could potentially explain the negative effect on motivation to treat, as the intervention lacked a focus on specific therapeutic training related to pedophilia, which MHP have deemed essential to enhance their skills and confidence necessary to increase their motivation to treat people with pedophilia (Martinec Nováková et al., 2023; Schmidt & Niehaus, 2022). Interestingly, Levenson and Grady (2019), who emphasized treatment skills and training in their intervention, did not observe any effect from pre- to post-intervention. A plausible explanation for this could be the composition of their participant group, which consisted of therapists with prior experience working with individuals who had sexually offended children. This prior experience likely indicates existing comfort, competence, and motivation to treat such individuals. Furthermore, all participants voluntarily enrolled in the training, suggesting an inherent open-mindedness toward individuals with pedophilia, which may have biased their pre-intervention scores. In contrast, Jahnke et al. (2015b) utilized a randomly selected group of psychotherapists. Therefore, the findings related to motivation to treat should be interpreted with caution, highlighting the urgent need for future research to explore effective training interventions that can increase and improve MHPs skills and competencies in treating individuals with pedophilic tendencies.
Another component within each intervention that appears effective is the use of narrative educational material as opposed to purely informative content. Harper et al. (2018) tested two different interventions: one using a narrative video and text, and the other using an informative video and text. They assessed four variables in total, finding that their narrative intervention had a significant effect across all variables and showed slightly better results compared to the informative intervention. However, it is noteworthy that Harper et al. (2022) replicated the procedure used by Harper et al. (2018) but found the informative intervention to have a greater effect on intentionality compared to the narrative intervention. The primary difference between the two studies was that Harper et al. (2022) used a larger public sample with an equal gender split, suggesting that gender may be an important factor to consider in future research. Moreover, despite the apparent effectiveness of narrative interventions in Harper et al. (2018) and Harper et al. (2022), the study by Lawrence and Willis (2022) also tested both narrative and informative interventions, with results on five variables showing considerable variation between significant and non-significant effects. Interestingly, Lawrence and Willis (2022) found that informative interventions were either more effective or equally as effective as narrative interventions. Given that there is less than an 8 min difference in the duration of the interventions across these three studies, duration does not seem to account for the differences in results. Examining the participant samples may provide some insight. Harper et al. (2018) reported the best results, and their study was the only one to have psychology students included in their sample. In contrast, Harper et al. (2022) and Lawrence and Willis (2022) sampled the general public. Since psychology students may be more open-minded and possess greater knowledge about sexual deviance than the general public, this could be a plausible explanation for the differing outcomes. Therefore, future research is recommended to test narrative and informative educational interventions on both MHPs and the general public, to better understand their relative effectiveness across different populations.
The study that stands out most prominently across all the meta-analyses is the study by Heron et al. (2023), which found significant results for their specific intervention across all tested variables and showed a remarkably higher effect size compared to other studies. This is likely attributable to their unique approach, involving an in-person presentation by a self-identified pedophile. This method aligns with prior research suggesting that contact-based interventions, such as in-person presentations, yield more significant results compared to interventions primarily consisting of narrative videos (Dalky, 2012). When examining the variable of deviance, which was non-significant overall, Heron et al. (2023) again demonstrated a significant and remarkably larger effect size compared to the other studies. This suggests that, despite deviance being non-significant in this meta-analysis, educational interventions may significantly influence outcomes related to deviance, and potentially other variables, if they include in-person presentations. This indicates the need for future research to confirm whether this unique approach is what specifically contributes to their large effect size.
Another important aspect of educational interventions worth considering is the duration. Lawrence and Willis’ (2022) intervention lasted 3 hr, making it the longest, while Heron et al. (2023) was 2 hr and 5 min and the other studies varied between 5 and 13 min. Interestingly, despite Lawrence and Willis (2022) achieving some significant results, the intervention by Heron et al. (2023) appears remarkably more effective. This is noteworthy, as research suggests that varying durations of interventions have different effects on reducing stigmatizing attitudes toward individuals with mental disorders (Clay et al., 2020). As such, this highlights the importance of examining the duration of interventions in future studies, as excessively long or short interventions might have a negative effect. Overall, these aforementioned findings suggest future research should focus on interventions that incorporate in-person presentations, narrative interventions, and examine the optimal duration to maximize effectiveness.
Implications
The present study adds to a growing field of research on the reduction of stigmatization toward people with pedophilia, with a specific focus on MHPs and the effectiveness of educational interventions as a tool for stigma reduction. It also contributes to MHPs’ understanding of people with pedophilia and the mental health issues that can arise without proper therapy, potentially leading to child sexual abuse (Beier et al., 2015; Blagden et al., 2018; Hanson & Bussière, 1998; Houtepen et al., 2016; Ischebeck et al., 2021; Jahnke et al., 2015c; Jahnke, 2018b; Levenson et al., 2020). It highlights the importance of destigmatizing people with pedophilia among MHPs in order for people with pedophilia to be able to receive effective treatment, as well as build professional relations between the MHPs and their patients who self-identify as pedophiles.
The present study, also demonstrates that educational interventions can, to some extent, help reduce the stigmatization toward people with pedophilia among MHPs. It is therefore highly recommended to implement some form of educational interventions to all MHPs. For example, educational interventions can be implemented as part of the curriculum for mental health education such as psychology, social work, and psychotherapy. Furthermore, educational interventions about people with pedophilia should be made available for MHPs who might come in to contact with people with pedophilia. Professionals working directly with people with pedophilia in correctional services, should be given mandatory courses on people with pedophilia in order to better support and treat them. By educating current and future MHPs about people with pedophilia, it might be possible to improve the lives of people with pedophilia, while potentially reducing risk for child sexual abuse to occur.
Limitations and Suggestions for Future Research
There are several limitations to the present study. First, of the included studies regarding MHPs, Jahnke et al. (2015b) was the only one that had a control group and conducted a follow-up test. The present study therefore excluded the measurements for both the control group and the follow-up test, which can be considered a limitation, as follow-up tests can provide a better representation of the effects of the interventions, as a certain time period allows for learning or attitude decay and on-going external stimulation to be measured (Stratton, 2019). Furthermore, none of the included studies measured behavioral change after the educational interventions. Future research should measure both follow-up tests and behavioral change among MHPs in their work settings to better determine the actual effects of educational interventions.
Another limitation is that the educational interventions implemented in each study have very different structures, durations, and foci. For example, the study by Levenson and Grady (2019) had the longest educational intervention of 3 hr, with the shortest intervention being only 5 min. Heron et al (2023) was the only study that included an in-person presentation, with Munslow-Davies and Anderson (2022) presenting a 5 min video with only informative information on people with pedophilia. This impacted the heterogeneity and could potentially impact the overall results of the effectiveness of educational interventions, as long narrative or in-person interventions might be more effective. Therefore, it is recommended to conduct future research on different types and durations of educational interventions to assess the effectiveness of specific interventions.
Moreover, the present study highlights a significant limitation in that MHPs were not provided with the specific training they identified as essential, contributing to their apprehension about treating PWP. This situation underscores the broader issue of practicing outside one’s area of expertise due to inadequate training, which could inadvertently perpetuate stigma or lead to suboptimal care outcomes. This cautionary note not only points to a critical gap in the professional preparation of MHPs but also emphasizes the urgent need for future research to explore effective education interventions that can equip these professionals with the necessary skills and competencies to expand their practice areas confidently and competently.
Finally, the current meta-analysis relied on a relatively small number of studies. While incorporating additional studies from the general public did enhance the statistical power of the analyses, it still presents challenges in reliably generalizing the findings to the specific population of MHPs. This issue, however, stems from the scarcity of available research rather than methodological oversight. Consequently, it is recommended that future meta-analyses be conducted as more specialized studies become available, which will help in providing more definitive insights.
Conclusion
The present study underscores the efficacy of educational interventions in reducing MHPs’ stigmatization toward people with pedophilia. The meta-analyses reveal a significant impact of these interventions on altering MHPs’ perceptions of people with pedophilia, particularly in dispelling notions of dangerousness and intentionality, diminishing the need to socially distance themselves from people with pedophilia, and fostering less punitive attitudes. However, the study did not find any significant changes in MHPs’ motivation to treat people with pedophilia, meaning that the second hypothesis was not supported. Of prime importance, it is concluded that the efficacy and outcome of the educational interventions highly depends on the type, duration, and focus of the intervention.
Despite its limitations and some non-significant results, the present study adds to a growing field of research on reducing MHPs’ stigmatization toward people with pedophilia. Consequently, educational interventions on the topic of people with pedophilia is recommended to be implemented as part of the curriculum of mental health educations such as psychology, social work, and psychotherapy. Furthermore, educational interventions on people with pedophilia should be made available for MHPs who might encounter them during their work. By educating current and future MHPs about people with pedophilia, it might be possible to improve the lives of people with pedophilia, potentially reducing risk factors for child sexual abuse to occur.
Summary of Critical Findings
● Educational interventions can reduce stigmatization in MHPs toward people with pedophilia, to some extent.
● Highlight the importance of stigma reduction of people with pedophilia.
● First meta-analysis to examine the topic.
● The efficacy of educational interventions depends on the type, duration, and focus.
Summary of Implications for Practice, Policy, and Research
● Educational interventions for people with pedophilia should be part of the curriculum for MHPs.
● Educational interventions should be available for mental health professionals.
● Mandatory educational interventions should be provided to MHPs working directly with people with pedophilia.
● Adds to the growing body of literature examining stigma reduction toward people with pedophilia.
● More research that focuses on the enhancement of MHPs’ motivation to treat.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.