
Abstract
The provision of effective mental health services to individuals attracted to children is rapidly expanding. However, these services have not yet been integrated into general mental healthcare systems and are mainly offered by organizations that predominantly provide services to child sexual abuse perpetrators. Little is known about the perspective, treatment goals, and approaches employed by prevention-specialist mental health professionals when working with clients attracted to children. To address this gap, we used purposive sampling to recruit 10 practitioners who had experience of working in prevention settings with clients attracted to children. After conducting semi-structured interviews and analyzing data through interpretative phenomenological analysis, we identified three main themes and four subthemes within the data. While most participants believed that attraction to minors is unmodifiable or doubted the possibility of modifiability, this belief did not necessarily manifest in their practice. Participants stressed the importance of finding safe alternatives for clients and highlighted the significance of accessing evidence-based information on alternative sexual outlets, such as sex dolls. One overarching theme that emerged across all themes and within participants' accounts was the concern of escalation, indicating a fear that pedophilic fantasies or alternative sexual outlets such as sex dolls could potentially lead to sexual offenses. The findings shed light on the approach of prevention-specialist mental health professionals in working with clients attracted to children and may be used to inform future intervention plans to facilitate service provision to this population.
Keywords
Introduction
Individuals attracted to pre-pubescent or pubescent children comprise 1–5% of males and less than 1% of females (Bártová et al., 2021; Dombert et al., 2016). Such individuals may seek psychotherapeutic services for various reasons, including stigma-related stressors such as social isolation (Jahnke, Schmidt, et al., 2015), mental health issues like depression and anxiety (Walker, 2017), suicidal thoughts (Cohen et al., 2020; Ingram et al., 2023), or concerns over their sexual preference (Stephens et al., 2021). Nonetheless, this population faces structural barriers in seeking help due to the widespread conflation between having a sexual attraction to children and engaging in sexually abusive behavior (Jahnke, Imhoff, & Hoyer, 2015), which leads to stigmatizing attitudes even among professionals (Jahnke et al., 2015; Levenson & Grady, 2019; Schmidt & Niehaus, 2022).
In recent years, growing scholarly attention to the stigma associated with a sexual attraction to children has prompted inquiries into how psychological services can most effectively improve such individuals' well-being and contribute to the prevention of child sexual abuse (CSA) (Beier, 2016; Cantor & McPhail, 2016; Lasher & Stinson, 2017; Lievesley et al., 2018). Notable differences exist in the approaches used to achieve these goals through mental health service provision.
One such difference is whether sexual attraction to children is viewed as a stable or modifiable state. This issue has been the subject of ongoing debate, resulting in at least two distinctive approaches to treatment. One approach relies on a theory that considers minor attraction as a form of sexual orientation that remains stable over time (Bailey et al., 2016; Beier et al., 2009; Berlin, 2014; Cantor & McPhail, 2016). For example, Seto’s conceptualization of chronophilia (2017) describes pedophilia as a sexual age orientation, suggesting that (based on the early age of onset, sexual and romantic components, and stability over time) pedophilia has a similar pattern to sexual gender orientation (Seto, 2012). Considering pedophilia as a sexual orientation implies that treatment might be more effective when it prioritizes developing self-regulation skills rather than attempting to alter sexual preference (Seto, 2012). Accordingly, accepting minor-attraction is a pivotal step in effectively managing its behavioral manifestation. This acceptance serves as a crucial foundation for clients, enabling them to process suppressed feelings, integrate their atypical sexuality into their sense of self, alleviate the internalized shame, and enhance their capacity to manage their desires responsibly (Beier et al., 2009; Cantor, 2018; Lievesley et al., 2018; Walton & Hocken, 2021).
Yet, other scholars have raised doubts about this perspective, suggesting that certain degrees of flexibility in sexual preference may exist, particularly when non-exclusive minor attraction emerges in later developmental stages (Fedoroff et al., 2014; Tozdan & Briken, 2015a, 2015b). Such scholars argue that acceptance could potentially diminish the motivation for change and reduce the individual’s self-efficacy to modify their sexual attraction (Lampalzer et al., 2021). In response to this claim, Cantor (2018) points out that if clients are informed that their pedophilic desire will cease, they may underestimate it and not attempt to develop skills for managing their sexual desire or avoid certain situations, hoping that it will disappear. Therefore, strong evidence is required to convince practitioners to promote the idea of modifiability. This is particularly important because mental health professionals are tasked to provide their clients with scientifically and clinically precise information, as outlined in the American Psychological Association’s Ethical Principles of Psychologists and Code of Conduct (2017, 2.04, 10.01b). Despite ongoing discussions, consensus on treatment objectives and approaches for clients attracted to children remains elusive.
The Present Study
Context
Recently, increased attention to preventive and proactive public health policies has led to increased levels of service provision for individuals in the community considered at higher risk for sexual offending (Piche et al., 2016), i.e., before offenses occur (Centers for Disease Control and Prevention, 2004). Those concerned about their sexual attraction to children may be a target population of such services (Beier, 2016). However, prevention-focused services are still less developed or limited compared to the treatment and rehabilitation of CSA perpetrators (Cantor & McPhail, 2016; Goodier & Lievesley, 2018), and often lack selective or specialized interventions (Christofferson, 2019; Piche et al., 2016). These services appear to adopt similar therapeutic approaches for clients who offended and those who did not, often administered by the same staff. This is unsurprising, as investigations into mental health professionals' readiness and perceived capabilities to serve clients attracted to children reveal negative or stigmatizing attitudes, knowledge inaccuracies and reluctance to offer services to this population among trainees (Gunnarsdottir, 2018; Hanson, 2018; Jahnke, Philipp, & Hoyer, 2015; Walker et al., 2022), accredited clinicians (Levenson & Grady, 2019; Schmidt & Niehaus, 2022), and primary, non-specialist healthcare providers (Lievesley et al., 2022). Given this context, there is a need to better understand the therapeutic goals and approaches of prevention-specialist mental health professionals who are engaged in providing care to clients attracted to children. This qualitative exploratory study aims to investigate this group of professionals' perspectives, treatment goals, and approaches in working with clients attracted to children.
Terminology
We used the terms “pedophilia” and “minor attraction” interchangeably in the research advertisement and during the interviews to describe a primary or predominant, exclusive, or non-exclusive sexual attraction to children across several minor-related chronophilic categories (Seto, 2017), spanning from infants to early pubescent children. Given the potential overlap of chronophilic categories (e.g., individuals may experience sexual attraction towards both prepubescent and pubescent children) and the lack of consensus within the scientific community regarding the age range of categories (e.g., hebephilia) (Blanchard et al., 2009; Stephens et al., 2019), pedophilia has been used loosely to refer to attraction to pre-pubescent and early pubescent children. This term seems to be more familiar to practitioners than terms such as “hebephilia” or “pedohebephilia.” Moreover, using “pedophilia” helped us to understand how participants conceptualize it (e.g., whether they conflate pedophilia and sexual offending against children).
The interview schedule was deliberately designed to allow participants to articulate their interpretation of pedophilia through initial questions and expand their answers by discussing their experiences with clients. Despite the flexible use of the term, adjustments were made during the interview as needed concerning the age of attraction or exclusivity (e.g., how do you assist a client exclusively attracted to pre-pubescent children in navigating sexual and intimacy needs?). In this report, to maintain consistency with the terminology used during the data collection, we continue to use the term 'pedophilia' as synonymous with minor attraction.
Methods
Research Design
We employed a qualitative method to explore participants' perspectives, therapeutic goals and approaches, collecting data through semi-structured interviews. The flexibility and exploratory nature of the qualitative interview (Braun & Clarke, 2013) allowed us to address our research questions.
After receiving approval from the Trinity College Dublin Ethics Review Board, we adopted a purposive sampling approach and included participants with relevant characteristics. The research advertisement was sent to several therapists’ email groups and several prevention-focused organizations that provide services to people who have offended or are concerned about their sexual thoughts, preferences, or behaviors. To obtain a more heterogeneous sample, we did not limit the geographical location of participants. To be eligible to participate in the study, individuals had to be, a) a mental health professional (e.g., psychologists, social workers), b) proficient in English, and, c) experienced in providing therapeutic services to clients with sexual attraction, fantasies, or behaviors involving children, irrespective of the clients' involvement in the criminal justice system. Out of sixteen professionals who initially expressed interest, ten individuals met the eligibility criteria and consented to participate in the study. Potential participants were informed that they would be specifically asked about “pedophilia” and “clients attracted to children.” Interviews were conducted using a hybrid format, with online interviews held and recorded via Microsoft Teams and face-to-face interviews recorded using a voice recorder.
Participants
Participants had various educational and professional backgrounds, including psychology (counseling, forensic), psychotherapy (integrative, psychodynamic, cognitive-behavioral, and sex therapy), and social work. Five participants held a doctoral degree in their field. Several participants held multiple qualifications, such as being a social worker or psychologist who had subsequently pursued training as a psychotherapist. The sample comprised six females and four males, with ages ranging from the 30s to the 70s and the duration of professional experience spanning 4–34 years (with an average of 15.5 years). Participants were based in Ireland, England, Scotland, and Canada. Some had experience working in social services (hospitals, prisons, probation service, mental health clinics), private practice, charities, or non-governmental organizations.
At the time of the interview, eight participants were working with one of three prevention-focused organizations. Organizations A and B offered therapeutic services to individuals accused of sexual offenses or non-offending clients concerned about offending behavior, including those concerned about minor attraction. Meanwhile, organization C exclusively served individuals involved in the criminal justice system for contact and non-contact CSA perpetration, including minor-attracted perpetrators. The therapeutic services provided by all organizations were voluntary, with two of them requiring clients to pay, while one received state funding. Two other participants provided treatment programs in prison for sex offense perpetrators, including minor-attracted CSA perpetrators. To maintain the anonymity of the participants involved in this study, we do not report the names of the organizations and have employed pseudonyms for participants throughout the article.
Data Collection
Semi-structured interviews were undertaken to collect data. Interviews lasted between 60 and 110 minutes, with a mean duration of 77 minutes. Participants were offered a €50 gift voucher as compensation, with the option to donate it to a relevant charity if they preferred.
The first author prepared the interview schedule, which the other authors subsequently reviewed. The schedule included open-ended questions and covered three broad areas: a) participants' definition and perspectives on pedophilia, b) participants' therapeutic focus, goals, and approaches when working with offending and non-offending clients attracted to children, and c) participants' views on intimacy and sexual needs of clients attracted to children, including their perspectives on sex dolls.
We asked participants to distinguish between their organization’s specific guidelines (if any) for treating clients attracted to children and the therapeutic approach they would adopt in private practice. Given that some participants worked in settings that only served offending clients, it was anticipated that they might not have prior experience working with non-offending individuals attracted to children. In this situation, the interviewees were asked to envision a hypothetical scenario involving a non-offending client who disclosed a sexual attraction to children in therapy. Employing hypothetical scenarios or vignettes during interviews is a common practice (Sampson & Johannessen, 2020; Törrönen, 2018) to understand participants' attitudes or decisions when they have not encountered the phenomena in question.
The interviewer allowed some flexibility in administering the schedule (Braun & Clarke, 2013) as participants' work settings and professional backgrounds varied, and subsequent discussions unfolded depending on how participants answered the core questions. All participants agreed to be contacted later for accuracy checking should any transcriptions be unclear or ambiguities arise in their accounts, necessitating follow-up questions. Four participants were subsequently contacted for this purpose, with one reviewing the interview transcription. Interviews were conducted by the first author, a clinical psychologist with some relevant professional training but no prior experience as a clinician in working with clients attracted to children or CSA perpetrators. For doing this research, the interviewer was engaged in prolonged parallel fieldwork in a prevention specialist organization with therapists and CSA perpetrators, also with a self-help organization for adults attracted to children. Throughout the research, she kept a reflexive journal to remain aware of potential biases or assumptions.
Data Analysis
Data were analyzed using interpretative phenomenological analysis (IPA). IPA’s inductive bottom-up approach to analysis is commonly used to understand health professionals' perspectives (Smith et al., 2009; Smith & Nizza, 2022). It is valuable in studies where individuals can provide insights or share their encounters with the phenomenon (Smith et al., 2009).
The data analysis process started with reviewing each transcription multiple times while simultaneously listening to the audio recording of the interview. For each chunk of the data, first, a short summary of the explicit content or “descriptive note”, and then a more conceptual, “interpretative note” was created. The linguistic aspects of the data, such as laughter, hesitation or metaphors were also noted. This process resulted in “experiential statements” (Smith & Nizza, 2022, p. 38), creating several concise summaries of each data portion. These experiential statements were clustered based on patterns, including convergence and divergence, commonalities, and differences. The most salient, recurrent, and central concept that organized several statements was considered as a main theme (e.g., Nature of pedophilia). Subthemes represented specific aspects of the central concept of the themes, nested in the main theme yet represent a notable aspect of it (e.g., Pedophilic fantasies “safe inside” or “stepping stone”?).
The analytical process was initially conducted for each interview and later across the dataset by the first author. Two strategies were adopted to ensure the rigor of the analysis. First, as recommended by O’Connor and Joffe (2020), 20% of the total data were re-analysed by co-authors independently. They generated initial notes and themes for one interview (each analyzing different interviews), and later, we reviewed and compared each other’s themes and analytical steps and discussed them to create the final themes. This helps ensure the trustworthiness, communicability, and transparency of the coding process within the research team and reach a consensual interpretation of the data. Second, negative case analysis (Morse, 2015) was employed when we actively scrutinized the data to identify potential instances that may not have aligned with our interpretations.
Findings
Themes and subthemes.
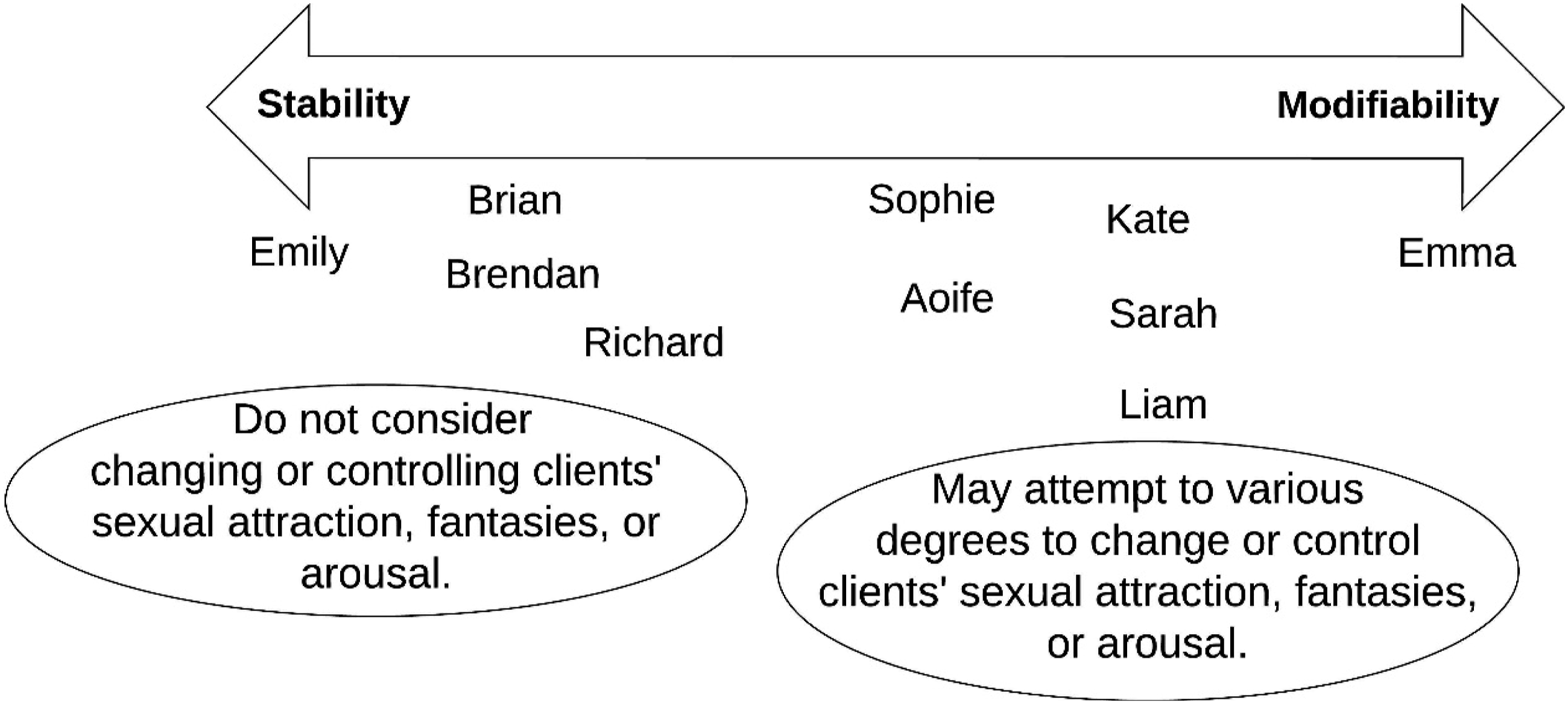
Schematic position of participants regarding modifiability of minor attraction.
Theme I: Nature of Pedophilia
This theme emerged as the most robust and predominant concept of this study, with discussions on other topics found to be interconnected with it. The theme reflects participants' views on the nature of pedophilic desire and the extent to which it is perceived as either stable or modifiable. This theme also includes participants' practical approach to whether pedophilic desire, including thoughts, feelings, or arousal, should or can be subject to psychotherapeutic interventions. Notably, we found that participants’ theoretical stance on the nature of pedophilia was not necessarily reflected in their practical approaches.
Subtheme I: Un/Modifiability
The majority of participants doubted the possibility of altering someone’s sexual attraction to children, which some participants described as an 'innate' and others as a 'fixated' condition. Emily firmly believed in the stability of pedophilia: “My view is that pedophilia is a sexual orientation, and just as you are not going to change someone who is gay into someone [who is] into the opposite sex, so you can’t turn a classic pedophile into someone who finds adult attractive. We aren’t going to do that.”
When asked about techniques, such as arousal reconditioning, Emily said: “See [by using such methods], you are getting dangerously close to conversion therapy. That is conversion therapy, and in my professional body, it is definitely not allowed. Ok? So, I think it would be unethical. I don’t use that because you are getting close to the thought police. We have certainly, in the [academic institution name], where I am involved, a sex-positive view. So long as someone’s sexual thoughts or fantasies and even behaviour don’t hurt or upset anybody else, as long as consensual, so long as they stay in the areas that are legal, they can do what they want.”
Brian and Brendan shared a similar view about the treatment of pedophilic sexual attraction. “I don’t know if these methods are effective. They might be helpful. We have never used such methods in our sex offender program. But… I think sexuality is who we are. too ingrained in us that I don't know if I believe it can be changed. Also, how effectively can it be measured?” (Brian).
Conversely, Emma, confidently stated that pedophilia is a modifiable 'interest': “Pedophilia is a sexual interest, but not a sexual orientation. Sexual orientation is who you fall in love with, whereas sexual interest is what you enjoy doing. So, a sexual interest is easier to change than a sexual orientation. Like saying, “I am gay,” it's hard to change. But to say, “I have a pedophilic interest”, it's easier to change my pedophilic interest than to change my orientation from being gay to being straight. So, it's kind of like comparing apples and oranges. I think it [pedophilia] is more conditioned than ingrained in the brain.”
Emma was involved in a program that attempted to change pedophilic sexual attraction as a main therapeutic goal. The program combined medication with individual and group therapy. Phallometry was used to measure clients' arousal responses. As Emma explained, clients were required to disclose their minor attraction to their families. Some submitted their computers to the clinic to avoid accessing Child Sexual Abuse Materials (CSAM). Emma was the only participant who claimed to have encountered clients whose erotic target had transitioned from children to adults. When questioned about the average duration of the treatment period that Emma asserted can bring about a change in clients attracted to children, she responded that individuals might undergo treatment for a period ranging from two to seven years. However, she acknowledged that for some clients, it might be years of effort and struggle, and “they are still going back to the pedophilic thoughts.”
When queried about the distinctions between individuals whose attraction to children has transformed and those who have not, Emma responded: “It's a matter of determination. I think it's a matter of mindset. It's almost like someone finally decides to quit smoking. You come to the determination that …you come to the decision that you are going to change, and then you change, and you take steps to change.”
Emma maintained that clients who have other conditions might have more difficulty changing: “People who have high psychopathy, for instance, adults with Asperger's …they have difficulty changing… so they need a little more attention.”
Richard viewed minor attraction as innate for some individuals and conditioned for others. “I still debate with myself what I think about this. But I suppose there are people for whom it's an innate desire. It's absolutely their desire. I think some people come at it more from desensitization through pornography. So, I think it is a continuum. For the former, [the therapeutic approach] is about accepting that terrible truth that they are dealing with pedophilia, and it is their innate sexuality, and I think you just have to accept it.”
Nonetheless, Richard dismissed using behavioural methods such as arousal reconditioning for individuals attracted to children. Believing that such methods are dangerous, he maintained that: “what people need are techniques or ways of managing their desire rather than trying to change them to something they're not.”
Five participants doubted the possibility of modifying core pedophilic sexual desire or sexual makeup. Yet they also indicated a willingness to entertain the possibility of changing pedophilic feelings, thoughts, or fantasies to varying extents in their clients. For example, Kate expressed that she would encourage clients to try and engage in relationships with adults in alignment with their (gender) sexual orientation. When asked about a client exclusively aroused by children, Kate suggested that it is worthwhile to explore the possibilities of relationships with adults. This is because, as she pointed out, many of her offending clients have not had any sexual experience other than solitary sexual activity or offending related to a child/ren. Kate acknowledged that she had never worked with non-offending clients attracted to children. Sophie, Kate and Aoife believed attraction to minors has psychological reasons and gaining insight can help individuals refrain from acting on it.
Subtheme II: Pedophilic Fantasies: “Safe inside” or “Stepping Stone”?
This subtheme represents participants' attitudes toward clients' sexual fantasies and whether those fantasies should be subject to change or suppression in therapy. This aspect of the theme deserves attention because, for some participants, sexual fantasies were seen as an inevitable aspect of sexual preference, while for others, it was viewed as a risky add-on or “symptom” that should be addressed. Emily mentioned: “I’ve actually come across people who are predominantly aroused by children and who have never gone anywhere near a child, so again, it’s a misperception that because of these kinds of tendencies, all children are at risk. Some choose to manage their sexual feelings and keep them all inside. Fortunately, we don’t have thought police yet” (laughter).
When asked whether she encouraged clients to suppress or stop their thoughts or fantasies, Emily responded by saying, “I don’t think that’s my role, and… again, they own their thoughts. My role is to stop people from offending.” However, Sarah vividly captured an opposite view: “They might have had an initial draw to minors, but then they're choosing to reinforce it as opposed to looking for an alternative. I would certainly challenge that and say, you're making yourself less safe for children, but also, you're putting yourself at a higher risk of reoffending if you're walking down that same path. I know some people would say what they do in their own head as long as they don't act on that … [it wouldn’t need intervention], but I think that if they're continuing to use that imagery and continuing to keep reinforcing their sexual template toward children, it's increasing their risk.”
In Sarah’s view, pedophilic sexual fantasies are inherently dangerous. Sarah’s reference to “reoffending” and “same path” hints at a possible influence stemming from her experience working exclusively with offending clients. Conversely, Emily regarded these thoughts as something that could be kept safely inside, considering attempts to control them as unnecessary surveillance. Emily and Sarah notably utilized the verb “choose,” emphasizing agency and control. However, Sarah extended the concept of agency to control sexual fantasies in mind, while Emily emphasized the choice to manage sexually harmful behaviors.
Other participants did not seem to consider altering clients' fantasies, and some, like Brian, held an uncertain view: “I wonder, by acknowledging those fantasies, are you allowing them to engage in that thinking that might go down the path of overcoming those internal barriers and ultimately may be engaging in online offending or contact offending?”
Participants were questioned about whether there is a guarantee that restricting masturbatory fantasies would not inadvertently intensify clients' desires to the extent of increasing the risk of sexual offending. Sophie considered such a possibility sensible: “Absolutely. It's like white bear syndrome, isn't it? Don't think about the white bear. I would agree with that”. Brendan said: “I agree. When you try to suppress something and push it down, it comes back stronger. I use the analogy of a big beach ball. if you're in the water and you're holding and then facing a beach ball, the harder you push down, the harder It resists. The pressure is pushing back up, and eventually, you can't hold it, and it shoots up the face, and it causes a mess for everybody. So that's how I think about trying to suppress or hide or push away whatever it is... an urge... You know? That's not to say just let it out, and everybody does what they want, but you just have to let them in a healthy way and manage it as best they can. It's what my instinct tells me.”
Kate and Liam acknowledged the significance of clients having a form of sexual outlet. However, they placed considerable emphasis on regulating the frequency and function of masturbation. Liam reported asking his clients to have a plan to control addictive or obsessive self-stimulating sexual behaviors. Kate highlighted the maladaptive use of sex as a coping mechanism in some individuals with a history of sex offenses when sex is utilized to relieve emotional pain or anger rather than sexual gratification. She maintained that all offending clients, irrespective of their sexual preference, are advised to limit masturbation to no more than 15 times per month.
Sarah expressed hesitation regarding the idea of not restricting pedophilic masturbatory fantasies: “I guess there probably isn't enough research on that if there are treatment protocols that “allow” (showing air quotes) those [pedophilic] fantasies. How do you allow someone's fantasy? People do what they want in their heads, but if one says that's fine for them to masturbate to fantasy, not images, but what's in their head, I actually don’t know if they go on actually to harm more or less than people who are discouraged. But I can understand your train of thought. It's like if we open and let the steam out a little bit, it’s less likely that somebody will blow and cause great harm by acting out with the contact offence. It's an interesting debate.”
Theme II. Alternatives without victims
This theme encapsulates professionals' discussions regarding potential alternatives in the intimate or sex lives of clients who are exclusively or predominantly attracted to minors. The first subtheme surfaced organically in conversations. The second subtheme represents practitioners' responses to a question about fictional sexual materials, including sex dolls.
Subtheme I: Safe Alternatives
Most practitioners referred to the idea of helping clients find “healthy” or “safe” alternatives. When asked to provide further details on a potential healthy alternative for clients' sex lives if they are exclusively attracted to children, five participants suggested celibacy and non-sexual intimacies: “It seems awful to think that you're going to say to somebody, you're just not going to have a sex life. That's part of you. It is over. But, in order to keep children safe and make sure that person doesn't go to prison, that's the reality that they find themselves in. I would encourage them to get some of their intimacy needs met through friendships” (Aoife). “Maybe the meaningful alternative for somebody isn't sexualized. You might find other aspects of their lives that are meaningful enough for them that they don't have to offend. Catholic priests have a sexual side because we're all sexual beings. It's like they kind of set it aside; they make a vow of chastity” (Sarah).
Emma mentioned that adult content could be a healthy alternative and explained a thought replacement technique: “We suggest people use legal pornography and masturbate to adult pornography. The whole idea is to work with the individual to try to get that individual to focus on their thoughts of adults rather than children, and whenever they have thought of a child or a sexual interest in a child, they immediately replace that with the thought of an adult, or they distract themselves with an activity that will get them not to think about that thought… Also, by virtue of focusing on other things, such as social skills, their sexual interests tend to change, which is interesting and what happens is by focusing and talking about adult sexual interests in the group and in therapy and by practising getting into romantic relationships of appropriate age and staying in appropriate age relationships, the individuals tend to, become more adult-focused and therefore, the interest in the child diminishes and goes into remission, but they have to continue focusing on adult interest for the rest of their life.”
Whereas Emily considered pedophilic fantasies as a source of sexual gratification: “They can use their fantasies in their head.” Liam suggested a similar notion of employing pedophilic fantasies for sexual relief. However, he did so with caution, viewing fantasies as a last resort in case all efforts to establish alternative fantasies failed: “In the case that a person might find it very difficult to generate an alternative sexual fantasy that didn’t involve an act that would be illegal, I guess …what I may do... I suppose ... one option would be a life of celibacy and abstinence and not trying to engage with any kind of sexual thought at all. How successful that would be, how wanted that would be… is open to debate. Assuming they want to have some sexual life on their own, then I think what I would be doing would be reinforcing the real harm that would be done, victim empathy, and all of those kinds of things. It may well be that I would help them work out a plan that was around active harm reduction, so there may be sexual fantasies that they could have as long as they will never commit to paper or share with anybody else or have images or materials that were illegal, would still provide some kind of sexual release for them. But again, one really needs to be careful that doesn't become a slippery slope.”
Encouraging clients to develop connections with adults and underscoring the potential negative consequences of acting on their pedophilic desires were mentioned by several participants. An outlier perspective was proposed by Sophie, even though she was hesitant about this controversial alternative: “I think... I don't know what I would do, but... I think what I might suggest to such an individual.... they might… I mean, you know, there are... adult sex dolls… they might use …not as a sex doll, I mean, they could use it as a sex doll but … but they would…I don't think there are any... [Hesitation, deep thinking, and a long stop].”
Subtheme II: Seeking Empirical Ground on Sex Dolls
The majority of participants took a cautious middle-ground stance regarding products such as sex dolls and stressed the need for empirical evidence. Some emphasized the potential for intensifying or reinforcing impacts, while others pointed to potential cathartic effects from a harm reduction perspective, indicating that they were not entirely convinced either way. Kate viewed the absence of an emotional attachment as a drawback of using sex dolls: “I think it's just so distasteful to the psyche to think of that, and the kind of knee-jerk response is to think no! because you're just feeling something that's really unhealthy. But… I don't know. I mean, we would always ask about fantasy, and if people are even fantasizing about a child, a child-based thing, I don't know if you can really change somebody, so finding a safe outlet is important. You'd have to do a lot of quantitative-based research to ensure that those things didn't condition people or discourage them from maybe more healthy attachments. I suppose what we would consider a healthy sexual attachment is one that has some level of emotional attachment, even if it's only brief, but there is a kind of respect, and no one goes away feeling horrible. That's why we're trying to encourage that act should feel good, and it shouldn’t be a wave afterwards of shaming.”
Brian expressed concern about the potential escalating effects of sex dolls: “I don't know if I'm fully comfortable with that. I think if we are looking at harm reduction piece, it will make sense because there is no victim per se. But I think again, does that lead to the risk? I think it needs to be looked at. Do you have to look at person's use of it? Also, you know, is there an addictive piece in it? Is there an escalation of behaviour?”
Similarly, Aoife emphasized the significance of monitoring clients who use such products to ensure controlling the perceived escalating effect: “I'm not opposed to that, to be honest with you, and anything that keeps children safe, I think, is positive. So, if they're going to use that doll rather than looking for an actual child, I would see that as being a really good safety feature. The only caveat I would talk with that is if the person is being monitored by a probation officer or a therapist because my fear would be that… I know from working with other clients that it's like, you use that for a while, and that's another rises you. and then, you're able to climax easier… and then, after a while, you're looking for something different, So, it's like, that's not enough anymore. Then you go looking online on, then you go … possibly you find yourself then on playgrounds and things like that.”
Brendan referred to the shortage of research evidence regarding the impact of using sex dolls: “It's controversial. I wouldn’t like to come down hard on one side or the other at the moment because I just don't know. I've thought of that all the time. It's hard to know what effect that would have. I'm probably a little bit more on the “Let them do it” as it might satisfy that urge and allow them to have a relatively healthy sex life. I don't know. I'd love to see some research on it.”
Richard, Emily, and Emma expressed opposition to the use of sex dolls. Emily flagged the potential reinforcing impact. Richard raised safety concerns for users and the lack of evidence for its effectiveness, while Emma argued against its necessity, claiming that pedophilia is modifiable.
Theme III. Slippery slope
Regardless of participants' beliefs about the modifiability of pedophilia and their attempts to change it, an overarching theme of the Slippery slope was encapsulated across all themes. This underlying concept represented the concern over the development, progress, or reinforcement of pedophilic desire. Interviewees were worried that if clients’ pedophilic desires (or, for some, sexual fantasies) were not subject to intervention or found an alternative outlet for release in the absence of any child victim (e.g., through private journaling or sex dolls), the desire might still escalate, reinforce, or potentially progress to more advanced stages, such as online or contact sexual offending.
In discussions about the nature of pedophilia, several participants, with reference to their clients who consume CSAM, noted that the majority of them are not pedophilic. Instead, they had developed a proclivity for children through habituation. It was commonly referred to as “desensitizationd” by participants. The idea was that CSAM consumers might be pornography users who found the same type of content boring and sought out more extreme types. For example, Emily maintained that: “Pornography often confuses people and gives them a wrong message and intercourse with their sexual template.” Kate asserted that “The internet [i.e., CSAM] can act as a catalyst to crystallize and magnify previously unconscious pedophilic interests.” Similarly, in the discussion of pedophilic fantasies and alternatives like sex dolls, the Slippery slope theme emerged across the data recurrently.
Other Commonalities
All participants in the study considered exploring clients' past experiences, such as childhood trauma. They also commonly referred to gaining insight into the reasons for minor attraction and addressing maladaptive coping strategies in therapy. Another common treatment objective was improving interpersonal relationships. A few participants mentioned the Good Lives Model (Ward, 2002) as their preferred approach. Although addressing the stigma of sexual attraction to children was not considered a therapeutic goal, three participants acknowledged the difficulty of disclosing pedophilic feelings in therapy. The focus was predominantly on risk paradigm, prevention, and harm reduction. Participants also emphasized the inadequacy of academic programs and/or continuing professional development for clinicians and advocated for more accessible mental health services for non-offending individuals attracted to children.
Discussion
This study aimed to explore perspectives, treatment goals, and approaches of prevention-specialist mental health professionals toward clients attracted to children. Participants expressed diverse opinions regarding whether pedophilia constitutes a stable form of sexuality. While some participants rejected the idea or possibility of altering one’s sexual makeup or expressed skepticism, others entertained the prospect of change to various degrees.
The idea that pedophilia is a lifelong form of sexuality has gained increasing recognition within the scientific community (Berlin, 2014; Moser, 2019; Seto, 2012). The few scholars who support the idea of change mainly focus on the potential implications of accepting stability (Tozdan et al., 2018) and why they believe such a change is feasible (Briken et al., 2014). Other claims are frequently accompanied by anecdotes or clinical observations (Fedoroff, 2018 & 2019) rather than concrete quantitative data with replicable methodologies or follow-ups. The only available data about the change (Müller et al., 2014) appeared to result from chance (Cantor, 2018) and has been criticized for lack of rigor in methodology and statistical analysis (Bailey, 2014; Cantor, 2015; Lalumière, 2015; Mokros & Habermeyer, 2016).
In the DSM-5 and its revision (DSM-5-TR), no remission criteria have been mentioned for pedophilic disorder (American Psychiatric Association, 2013, 2022). Currently, there is no robust empirical evidence supporting the notion that individuals with sexual preference to children undergo spontaneous or intervention-induced changes in their sexuality, leading them to become teleiophiles (predominantly sexually attracted to adults). Neither such data nor subsequent follow-up or reporting on the long-term effects of the treatment exist. As Cantor (2018) points out, there is always room for progress in science. However, the assertion of change thus far appears unsupported.
Some of the participants in our study evidenced an inconsistency between their attitudes about the nature of pedophilia and their therapeutic strategies. For instance, while questioning the modifiability of minor attraction, these participants reported that they would encourage clients to change their fantasies, thoughts, or emotions. These clinicians, while seemingly considering sexual attraction to children as stable, still leaned toward attempting to eliminate, control, or stop it. Such attempts included encouraging clients to focus on dating adults, redirect or replace their fantasies, and recondition their arousal. In one case, a participant who believed in the modifiability of pedophilia recommended that clients use legal pornography for sexual self-stimulation and adopt techniques such as thought replacement.
A study on general health professionals (Lievesley et al., 2022) indicates that they highly prioritize controlling or changing sexual attraction as a treatment goal when working with minor-attracted clients. The use of such approaches was attributed to practitioners' belief in the possibility of choice over sexual attraction to children, which aligns with our findings. Similarly, we observed examples implying the idea of choice in a few participants' accounts. For instance, Emma pointed out that such clients can decide to quit pedophilia in the same way people quit smoking. While the idea of choosing pedophilic attraction is a common misconception among the public (Jahnke, Imhoff, & Hoyer, 2015), dequately powered quantitative studies are required to explore the prevalence of such underlying assumptions among specialist professionals.
While motivating individuals with non-exclusive attraction to children to develop intimacy with adults might sound reasonable (Fedoroff, 2019), the impact of such therapeutic suggestions on clients with exclusive minor attraction is unclear. One possibility is that such recommendations can increase sexual frustration or shame and negatively affect self-esteem. Additionally, watching pornography might increase sexual preoccupation, potentially leading to more frequent or intense child-related sexual fantasies. It remains uncertain whether advising clients to suppress and discontinue sexual fantasies involving minors intensifies, diminishes, or has no effect on such fantasies in the long term among individuals attracted to children.
Some authors suggest that deliberate control of thoughts may have a rebound effect (Hooper & Mchugh, 2013; Wegner, 1994). An experiment conducted by Johnston et al. (1997) revealed that in individuals who committed CSA, the accessibility of child-related thoughts increased after an instructed suppression period. Suppression and avoidance are generally considered maladaptive emotion regulation strategies and risk factors for depression, anxiety, and maladaptive behaviors such as substance misuse (Aldao et al., 2010). A study on individuals attracted to children found that thought suppression is associated with higher levels of guilt and shame about sexual attraction, lower levels of hope about the future, and lower levels of subjective psychological well-being (Lievesley et al., 2020). Individuals attracted to children reported that thought suppression had been detrimental and conflicted with their therapeutic progress (Dymond & Duff, 2020). They also reported attempts to change pedophilia as unhelpful (Schaefer et al., 2023) and described their sexual attraction as enduring (Walton & Duff, 2017).
Considering uncertainties about the effectiveness of such strategies on clients attracted to children, applying them can pose an ethical dilemma. The Hippocratic ethical principle of beneficence and nonmaleficence guides practitioners to help or, at least, do not harm. This principle does not imply that a method should be employed unless proven ineffective or unsafe. Rather, it cautions against using a method unless it has been proven to be effective and safe (Ghaemi, 2008). Furthermore, strategies such as confiscating a client’s device or mandating disclosure to the family (which can lead to severe consequences) appear to be similar to surveillance and supervision rather than therapy, in which the client’s autonomy and self-determination must be at the heart of the practice (Cottone & Tarvydas, 2016).
Participants expressed a need for supporting evidence when considering alternative sexual outlets like sex dolls, which aim to manage existing desire rather than change it. While still limited, available empirical evidence does not support the idea that sex dolls have escalating effects. Instead, doll ownership is linked to reduced levels of sexual preoccupation and self-reported arousal in hypothetical abuse scenarios (Harper & Lievesley, 2022). Moreover, doll owners show a lower tendency toward sexual aggression (Harper & Lievesley, 2023). In a mixed-method study, minor-attracted doll owners report less sexual preoccupation compared to teleiophilic doll owners. The qualitative accounts of doll owners indicate they channeled their sexual fantasies toward their dolls while reporting a decline in interest in real children through doll use (Desbuleux & Fuss, 2023).
The idea that dolls and other fictional sexual outlets could become a slippery slope has long been a theoretical concern which has not been empirically tested until recently (see Harper & Lievesley, 2020 for a detailed review). Of specific interest in this study was that participants sought empirical evidence for utilizing sex dolls but not equivalent evidence for some of their suggested methods, such as encouraging non-offending clients to discontinue their sexual fantasies. We hypothesized that it might be due to a bias toward changing minor attraction. When a strategy is perceived as morally justifiable or “right” and does not evoke discomfort, there is a reduced tendency to subject it to critical scrutiny and investigate empirical evidence for its effectiveness.
As expected, most prevention-specialist professionals in our sample displayed comfort and sympathy, with relatively low levels of explicit stigmatizing attitudes toward non-offending clients attracted to children, likely due to their familiarity with the subject. However, some underlying assumptions, such as the uncontrollability of such clients and the inevitability of offending (Lawrence & Willis, 2021), dangerousness, and choice, were revealed during the conversation, mainly at a more implicit or linguistic level. For example, using terms such as 'potential offenders,' 'those who consider offending,' or 'those who still have not offended' to describe non-offending clients implies that some participants believed clients attracted to children are more inclined to offend rather than resist their sexual attraction. Moreover, the participants' overall approach was centered mainly around the risk paradigm when discussing non-offending clients attracted to children. While the prevention of child sexual abuse is undoubtedly a legitimate goal, the risk-management approach has been criticized for perpetuating social and self-stigma around minor attraction, which implies that individuals attracted to children are inevitably destined to offend unless preventive measures are taken (Jahnke, 2018; Lievesley & Harper, 2021). Some clients may perceive such efforts as incongruent with their needs and expectations, leading them to avoid seeking support to distance themselves from suspicions of being treated as potential offenders 1 (Cacciatori, 2017; Grady et al., 2019; Lievesley & Harper, 2021).
Additionally, a recent study found no significant difference among clients in a well-known prevention project (Dunkelfeld) compared to a control group on a waiting list in dynamic sexual offense risk factors such as sexual dysregulation, offense-supportive attitudes, recent behaviors related to CSA and CSAM consumption (Mokros & Banse, 2019). Considering the insufficient effectiveness of such risk paradigm approaches, it has been suggested that greater attention should be paid to other factors, including the psychological effects of living with minor attraction and stigma-related stressors (e.g., loneliness, low self-esteem, self-stigma, and shame) (Jahnke, 2018; Lievesley et al., 2020) and clients' overall well-being (Grady et al., 2019). This consideration also encompasses preventive elements since enhanced psychological well-being is associated with a reduced risk of sexual offending (Ward & Stewart, 2003; Yates, 2016).
It is well established that clients' treatment needs and priorities should be the focal point of practice (Tjeltveit, 2003). As the American Counseling Association (ACA, 2014) Code of Ethics recommends, counselors are advised to set aside personal values that do not align with the legitimate counseling goals of the client. Of particular relevance here is a study on the priorities and needs of individuals attracted to children (Levenson & Grady, 2019b). This study found that while managing sexual feelings was a treatment priority for some clients, nearly as prominent was the need to deal with shame and stigma and to learn adaptive coping strategies to live a fulfilling life despite minor attraction.
Limitations
The findings of this study need to be considered within the context of its limitations. First, the sampling was impacted by self-selection bias. Even though we selected participants based on certain inclusion criteria from volunteers who contacted us, those who came forward to participate in the interview might possess distinct characteristics compared to those who did not. For example, they might be more comfortable and confident discussing the topic. Despite our study having a relatively small sample, the number of participants is appropriate for the chosen analysis method. Most IPA studies are conducted with small samples ranging between three and six individuals. Typically, samples larger than 10 are not recommended for IPA (Smith et al., 2009).
Second, we had to rely on participants' subjective understanding of their clients or situations. Therefore, all biases and limitations of self-reports should be taken into consideration. Half of the interviewees were asked to envision a hypothetical scenario involving a non-offending client attracted to children. While this reflects the participants' different experiences and is not a limitation per se, hypothetical scenarios tend to minimize self-serving bias compared to recounting real events. Therefore, such participants possibly expressed their attitudes more freely.
Third, prevention specialist professionals, depending on their roles and work settings, may vary in their level of information about their clients. For instance, professionals working in prison settings usually have access to assessments from other resources. Those working with convicted clients in the community often can request police reports or conduct collateral interviews. In one organization, a phallometric test was required before treatment began, while in another, clients were the sole source of information and could seek support with a pseudonym. Another significant issue is the variation in mandatory reporting laws across jurisdictions that can affect the extent of clients' self-disclosure in therapy. For instance, in Ireland, professionals are mandated to report clients' access to CSAM, whereas this is not within the realm of mandatory reporting obligations of therapists in certain provinces in Canada. This range of contexts and availability of information undoubtedly influence our participants' case formulation and interpretation of each client and, consequently, the findings of this study.
Conclusion
In this study, we explored the perspectives, treatment goals, and approaches of prevention-specialist mental healthcare professionals working with clients attracted to children. Unsurprisingly, the risk paradigm was predominantly favored among clinicians in our sample. Five clinicians considered the possibility of changing clients' sexual preferences despite having reservations about its feasibility. This suggests a potential bias towards such a change as a socially desirable outcome. The practicality and safety of these attempts in therapeutic settings must undergo rigorous empirical evaluation.
Furthermore, the concerns raised by many participants under the Slippery slope theme underscore the necessity of obtaining more empirical evidence on the effects of fictional outlets, such as sex dolls, on sexually offending behaviors among individuals attracted to children. The findings can offer insights for improving future service provision for individuals attracted to children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funding from the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie Grant Agreement No. 861047.