
Abstract
The UN’s Sustainable Development Goal #5 (Gender Equity) includes violence against women and girls (VAWG), considering it as a violation of the rights of women and girls. The variety of risk factors for VAWG in Arab countries suggests the need to identify effective interventions to guide practitioners and policy makers. A systematic review of preventive interventions across the Arab League examined the outcomes of VAWG. Authors registered the study on the prospective register of systematic reviews database. Authors conducted the search for evidence up to 2023. Database searching identified 1,502 studies and after application of the eligibility criteria, 17 studies remained for inclusion. Quality appraisal used the Mixed Methods Appraisal Tool. Evidence emerged from eight Arab countries. Interventions occurred at the primary, secondary, and tertiary levels of prevention. However, only two studies employed interventions using more than one level of prevention, which considered systems strengthening and the development of community solidarity networks. The evidence revealed a lack of clear evaluation and evidence for the effectiveness of interventions and prevention alongside reactive approaches, with no evidence as to how systems may reduce or prevent VAWG. One main issue is patriarchal dominance in Arab countries creating the lack of a collective female voice in any of the evidence. However, Arab countries can change with support. Achieving the UN’s Sustainable Development Goal #5 by 2030 means interventions and programs need to include more than one prevention level, consider systems and include the collective female voice.
Introduction
Violence against women and girls (VAWG) is a significant public health issue, which exists globally (Johnson, 2008; Öhman et al., 2020; Román-Gálvez et al., 2021; Shen et al., 2022; Sri et al., 2021). The United Nations official definition of VAWG is any act of gender-based violence that results in, or is likely to result in, physical, sexual, or mental harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or in private life (United Nations, 1993).
The UN definition uses gender-based violence (GBV), which highlights that violence emerges from inequalities between men and women. Despite the interchangeable use of GBV and VAWG, both terms imply that VAWG arises because of gender inequality arising from discrimination against women in patriarchal societies. Therefore, inequality between the sexes is structural because constructions of femininity and masculinity are symbolic and reinforced by cultural norms. This article will use VAWG.
A key characteristic of public health is its focus on prevention and strategies occur at three points, primary, secondary, and tertiary, depending on when they occur and which population is selected to receive the intervention (Leavell & Clark, 1958). Interventions to reduce VAWG may focus on perpetrators of violence, women and girls most at risk, those who have already experienced violence or a combination of population groups. Interventions can act as deterrents, support women and girls to mitigate serious aftereffects and create legislation to increase equality and protect the rights of women and girls. A brief explanation of these three points follows:
Primary prevention: Focusing on preventing VAWG before it occurs and includes whole population strategies, examples include legislation, policy, and education.
Secondary prevention: Early intervention programs designed to detect potential VAWG and targeting population subgroups or individuals who may be either demonstrating early signs of VAWG, or who may be particularly at risk of developing violent behaviors, or who may be at risk of becoming a victim. Examples include screening individuals for risk, adjusting external physical environments to prevent the likelihood of VAWG occurring, working with groups to raise awareness and educate about VAWG.
Tertiary prevention:- Responses or interventions after violence has occurred, aiming to reduce the consequences and impacts of VAWG and prevent its recurrence. Examples include assisting women with coping with the long-term impacts of VAWG, setting up support groups for women to join in solidarity, setting up shelters for women experiencing violence.
The World Health Organization (WHO) offers a typology of violence, dividing it into three categories based on who commits the violent act. The three categories are (a) self-directed violence subdivided into suicide and self-harm; (b) interpersonal violence, subdivided into two further categories: family and intimate partner violence taking place within the home and community violence between individuals who are unrelated or who may not know one another and usually taking place outside the home; (c) collective violence, subdivided into social, economic, and political violence (Krug et al., 2002). Within these categories are four different acts of violence: physical, sexual, psychological, and deprivation or neglect. Although the WHO neatly categorizes violence, the subdivisions and types of action underline the complexity of VAWG.
The UN’s Sustainable Development Goal #5 (Gender Equity) includes VAWG as a violation of the rights of women and girls and a major challenge for the agency’s Agenda for Sustainable Development (UN Sustainable Development Goals, 2015). Overall estimates by the WHO suggest that almost one out of three women have experienced either physical or sexual violence from their partners (World Health Organization, 2013, 2018, 2022).
Policy level interventions addressing VAWG are those that promote gender equity and strengthen/enforce laws that address VAWG (UN Women., 2020). Some interventions target-specific population such as refugees or adolescent girls (Delkhosh et al., 2017; Noble et al., 2019), whereas others focused on VAWG interventions during the COVID pandemic, mobile apps to address the problem, and programs in low-middle income countries (Eisenhut et al., 2020; Kirk et al., 2017; Pearson et al., 2021). Each stressed the limitations of program evaluations because of changes in context such as emergencies (Robbers & Morgan, 2017).
Other reviews argue that when there are emergencies within countries, such as conflict or displacement, VAWG increases (Hossain et al., 2014). COVID-19 itself provided a unique situation where communities were isolated and locked-down, with early reports indicating that VAWG increased during this time because of social distancing measures and the separation of women and girls from social support networks (Bradbury-Jones & Isham, 2020; Chandan et al., 2020; Jarnecke & Flanagan, 2020; Marques et al., 2020). Research identifies the need for intersectional, intergenerational, and community approaches, which analyze the complexity of relationships in patriarchal societies and consider complexity, to reduce the occurrence of VAWG (Sánchez et al., 2020).
Women in Arab countries appear more at risk because of limited educational, economic, and social opportunities, coupled with traditional patriarchal values, making it difficult for women to leave their domestic roles and family responsibilities (Brookings Institution, 2013; Ty et al., 2015). Some research suggests that women not fulfilling their expected domestic roles apparently gives their husbands rights to beat them (Douki Dedieu et al., 2021; Douki et al., 2003). This is an explicit example of the subjugation of women and systematic infringement of their human rights. Moreover, it displays deeply ingrained cultural beliefs and attitudes about gender roles and the position of women in society.
Depictions of widely disparate prevalence rates across eleven Arab countries occur by type of violence: 6%–59% of women had experienced physical, 3%–40% sexual, and 5%–91% emotional violence (Elghossain et al., 2019; Hawcroft et al., 2019; Kisa et al., 2021; Mojahed et al., 2020). VAWG “undermines the mental and physical health of women and girls and violates their human rights” (Bell & Butcher, 2015, p. 4). For some women and girls, this leads to mental ill health, in particular depression and suicide (Afifi et al., 2011; Al-Modallal, 2012; Alzyoud et al., 2018; Eldoseri et al., 2014; Haj-Yahia, 1999, 2000; Hamdan-Mansour et al., 2011; Safadi et al., 2018; Shaikh et al., 2017). Women experiencing violence have more health problems and incur significantly higher healthcare costs than those who have not experienced violence (Klugman et al., 2014). The variety of risk factors for VAWG in Arab countries suggests the need for identification of interventions in this population to guide practitioners and policy-makers (Mojahed et al., 2020).
No reviews have considered interventions focusing on gender-based VAWG across Arab League countries. Therefore, the goal of this research is to conduct a systematic review on interventions for VAWG in the Arab League (a regional organization of 22 states in the Middle East and Africa), to ascertain which interventions are most effective.
Methods
The purpose of this review was to summarize the effectiveness of the intervention strategies used to address and prevent VAWG in Arabic-speaking countries. The research question for this review is “Which interventions are effective at reducing VAWG at individual and community level in the Arab League?”
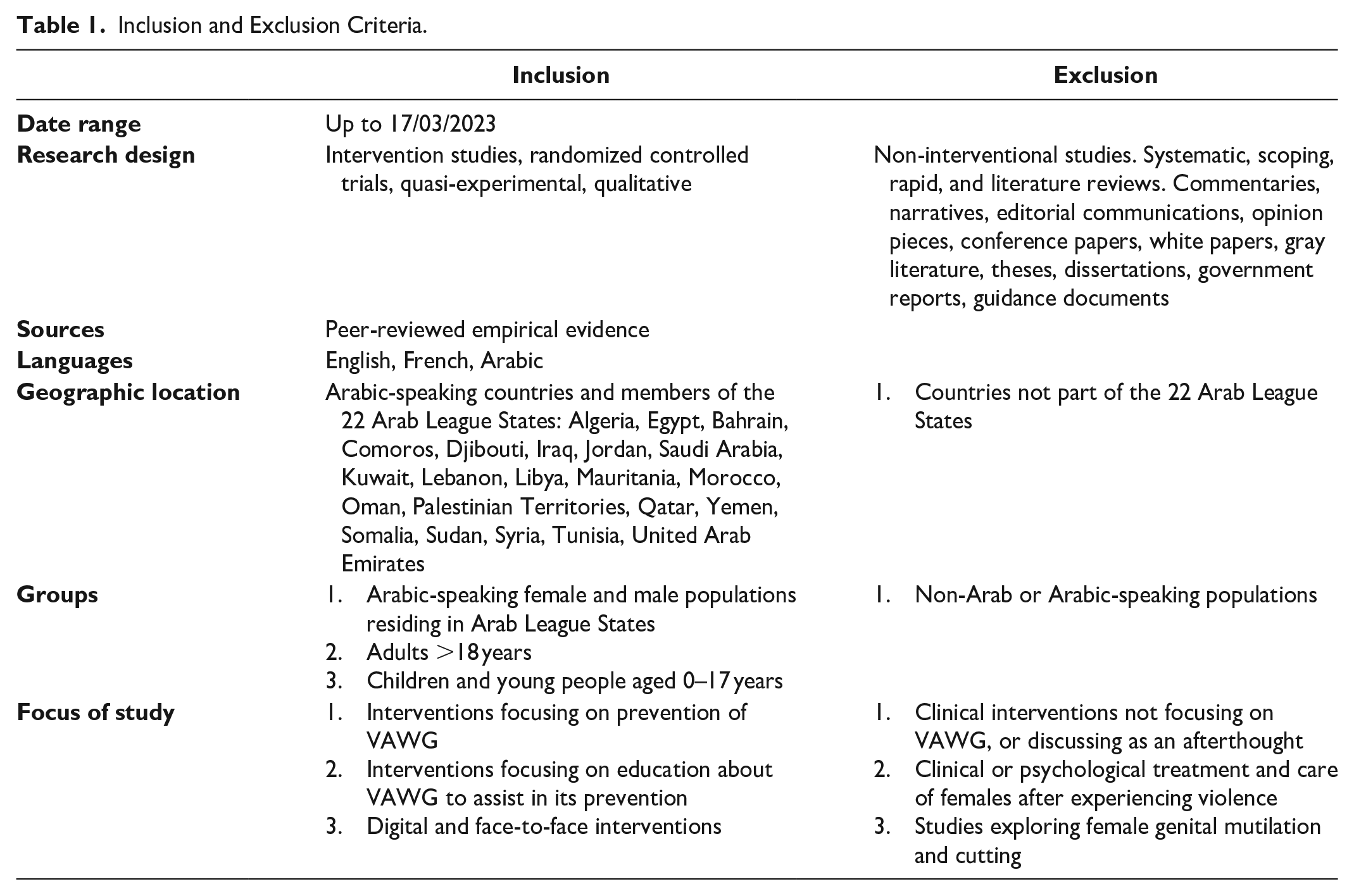
This study was a systematic review of the outcomes of preventive interventions involving VAWG across Arabic-speaking countries. The authors conducted the search for evidence up to March 17th, 2023. This review provides a best evidence synthesis and contributes toward improving the knowledge base of preventive interventions for girls and women at risk residing in a member state of the Arab League. For the purpose of this review, Arabic-speaking countries are defined as the 22 member countries of the Arab League States: Algeria, Egypt, Bahrain, Comoros, Djibouti, Iraq, Jordan, Saudi Arabia, Kuwait, Lebanon, Libya, Mauritania, Morocco, Oman, Occupied Palestinian Territories, Qatar, Yemen, Somalia, Sudan, Syria, Tunisia, and the United Arab Emirates (Blair et al., 2014; League of Arab States, 2022). Authors explored the elements of interventions, quality of evidence, target audiences, and program outcomes. The review employed the guidance for preferred reported items for systematic reviews and meta-analyses (PRISMA) (Page et al., 2021). The authors excluded female genital mutilation and cutting in this review in light of a recently published systematic review exploring prevention-based interventions (Abidogun et al., 2022). Table 1 provides more details of the eligibility criteria.
Inclusion and Exclusion Criteria.
The study registration number is CRD42022361852, accessed on the international prospective register of systematic reviews (PROSPERO) https://www.crd.york.ac.uk/PROSPERO.
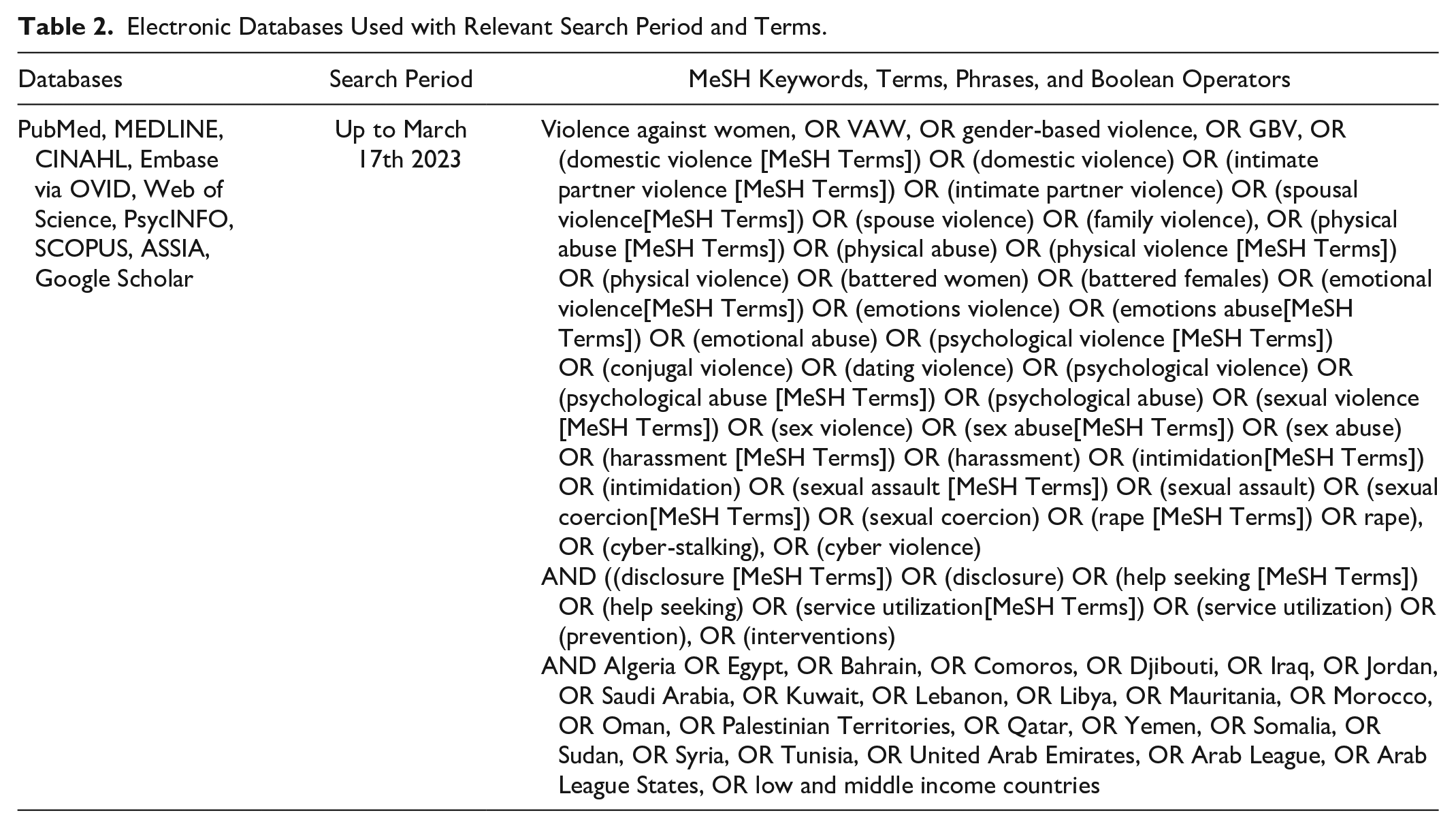
Databases used for searching were PubMed, Medline, Web of Science, PsycINFO, Embase, CINAHL, ASSIA, Scopus, and the first 100 citations on Google Scholar (Table 2). The search strategy was adapted in accordance with the indexing systems of each respective database used. Search terms involved used a combination of strategies, Medical Subject Headings (MeSH) keywords, phrases, and Boolean operators (Table 2).
Electronic Databases Used with Relevant Search Period and Terms.
Three of the authors (J.O., P.K., and B.A-E.) screened titles and abstracts for relevance. One author (B.A-E) used Rayyan QCRI software to assist in the screening process (Ouzzani et al., 2016). Forward and backward searching of retrieved records, identified through initial searches meeting eligibility criteria, producing any additional relevant literature for inclusion. Consultation with a third reviewer (either ED or EAC) resolved disagreements to reach consensus. J.O and B.A-E made the final decisions about inclusion and documented reasons for exclusion. This review employed the guidance for PRISMA (Page et al., 2021). Female genital mutilation was excluded in this review in light of a recently published systematic review exploring prevention-based interventions in Arab League countries (Abidogun et al., 2022).
Figure 1 provides the PRISMA flowchart leading to selected articles for this review.
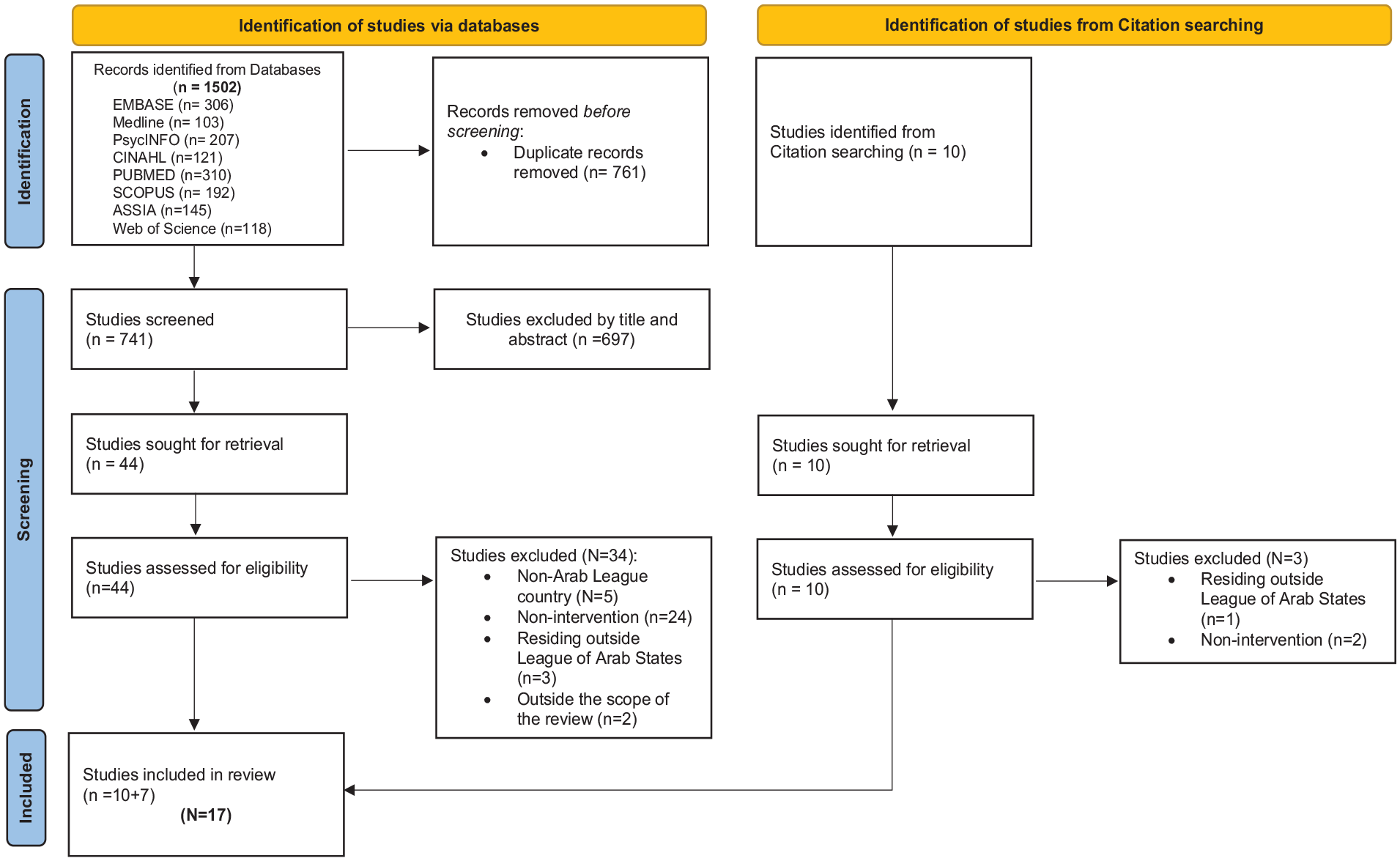
Preferred reported items for systematic reviews and meta-analyses flow diagram for violence against women and girls.
Results
Out of the 1,502 studies identified in databases and 10 from citation searching, removal of 761 duplicates left 751 studies for title and abstract screening. Using the eligibility criteria (see Table 1), researchers excluded 697 papers, leaving 54 papers for full text retrieval. Further application of the eligibility criteria left 17 studies for inclusion in the review. Tabulation of results included authors and date, country in which the study occurred, sample size, research design, length of intervention, outcomes, type of violence addressed, and public health level of prevention. Table 3 summarizes the characteristics of included studies.
Characteristics of the 17 Included Studies (n = 52,310).
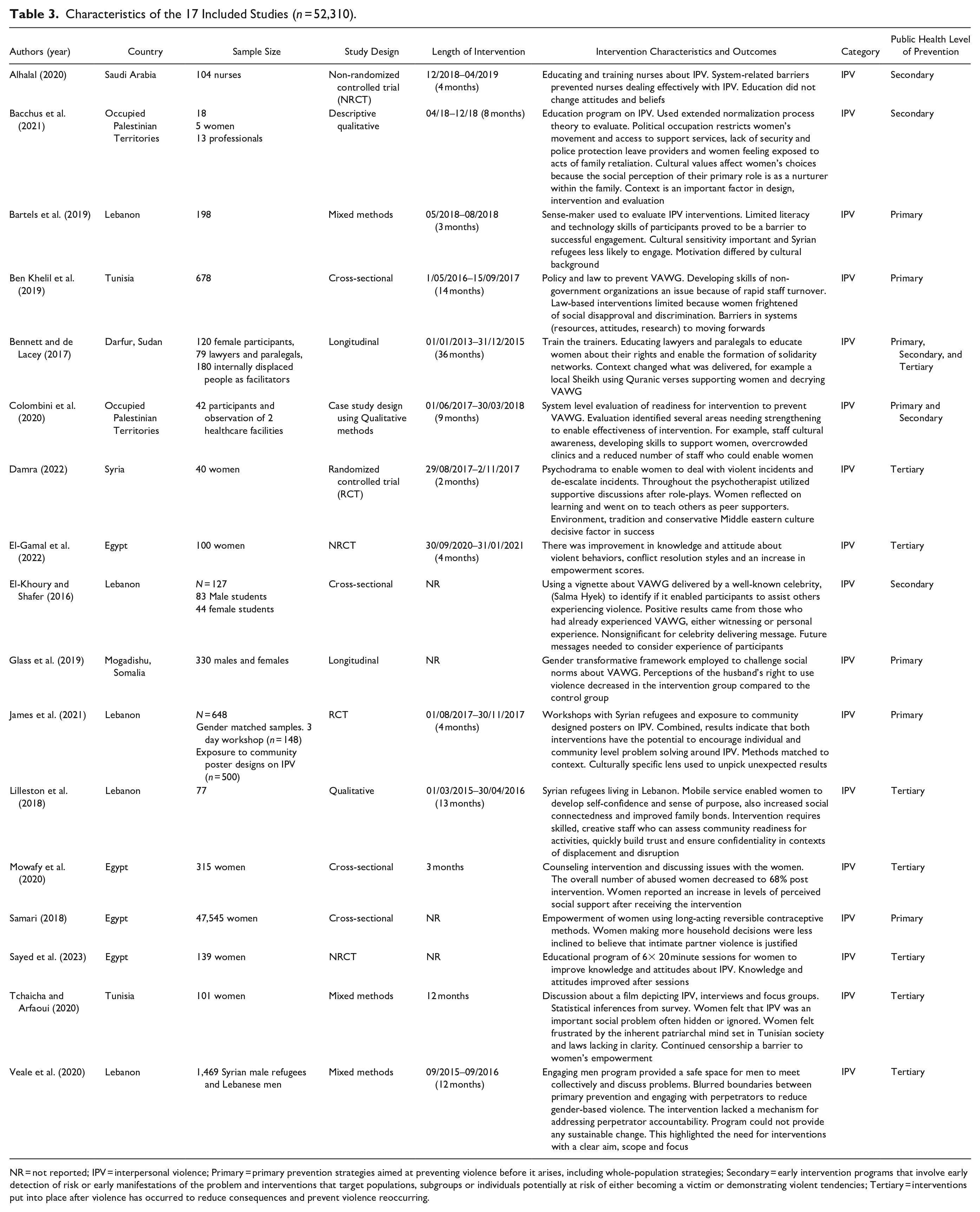
NR = not reported; IPV = interpersonal violence; Primary = primary prevention strategies aimed at preventing violence before it arises, including whole-population strategies; Secondary = early intervention programs that involve early detection of risk or early manifestations of the problem and interventions that target populations, subgroups or individuals potentially at risk of either becoming a victim or demonstrating violent tendencies; Tertiary = interventions put into place after violence has occurred to reduce consequences and prevent violence reoccurring.
Quality Assessment
Two reviewers (J.O., B.A-E) assessed the papers for quality using the Mixed Methods Appraisal Tool (MMAT), 2018 version (Hong et al., 2018, 2019). The MMAT includes two initial screening criteria, which assess for a clear research question/objective and for the appropriateness of the data collected to address the research question. For inclusion, studies must receive a “yes.” The tool contains a subset of questions to assess for quality for each study type—qualitative, quantitative, and mixed methods (see Table 4). Studies received 25% points for each “yes” response. Higher percentages reflected higher quality; 100% indicated the paper met all quality criteria. The first author (J.O.) checked 50% of included studies, then based on reaching 100% agreement, the primary reviewer (B.A-E) applied the tool independently to the remaining studies.
MMAT Quality Assessment.
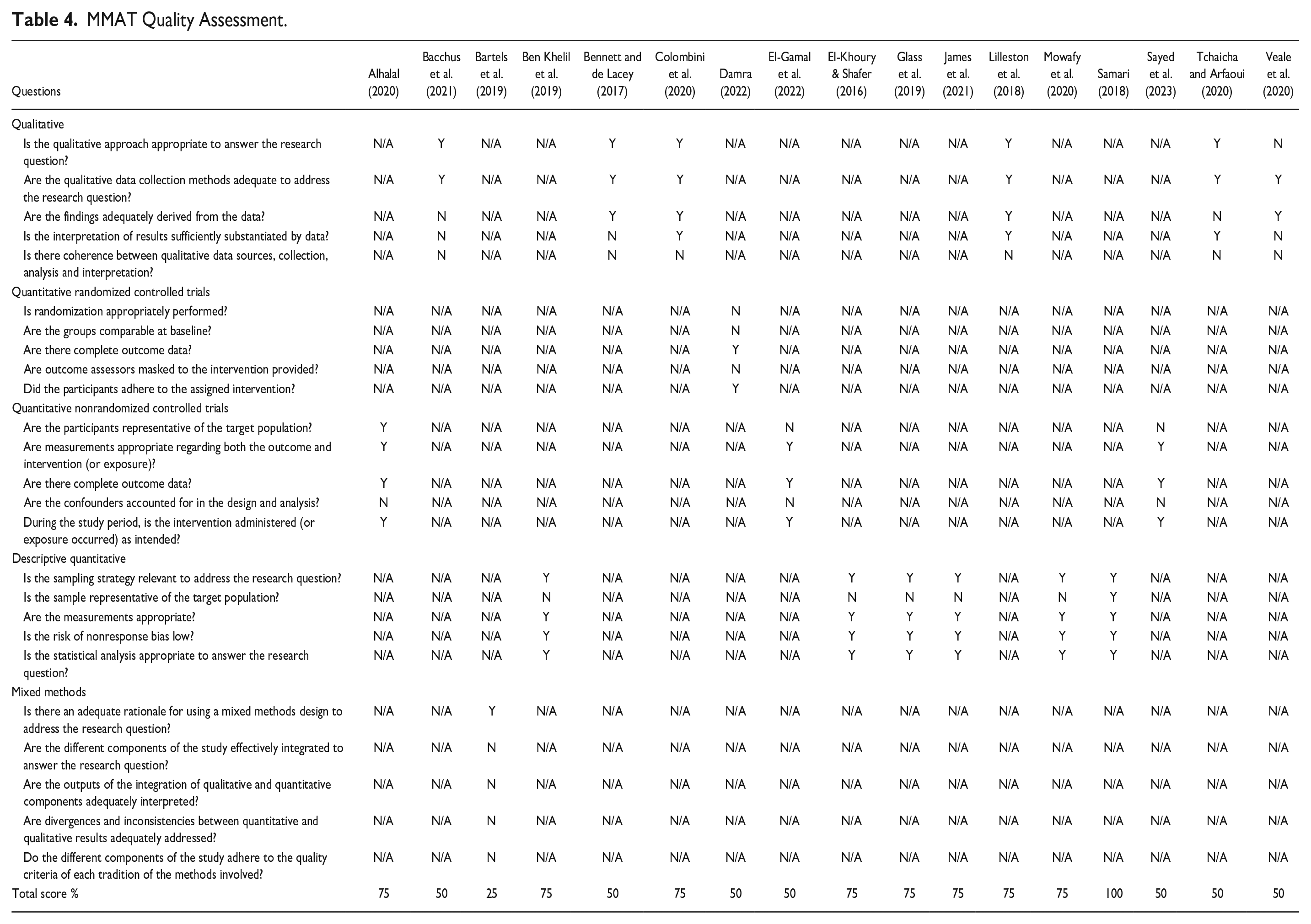
Scores for the 17 included studies ranged from 25% to 100%. One study (5.88%) received a 25% rating based on the MMAT criteria, seven studies (41.17%) received 50%, eight studies (47.05%) received 75%, and only one study (5.88%) scored 100%. The most frequent weaknesses were: (a) failure to acquire a large enough or justify sample size representing the population researched, (b) lack of discussion on researcher influence and analysis in qualitative studies, (c) lack of integration of qualitative and quantitative methodologies in mixed methods studies, (d) lack of clear description of randomization approach utilized in the randomized quantitative studies, (e) no identification of subthreshold rates for acceptable response or follow-up in non-randomized quantitative studies.
Countries
Evidence came from eight Arab countries. One from Saudi Arabia (Alhalal, 2020), one from Dafur in Sudan (Bennett & de Lacey, 2017), one from Mogadishu in Somalia (Glass et al., 2019), one from Syria (Damra, 2022), two from Occupied Palestinian Territories (Bacchus et al., 2021; Colombini et al., 2020), two from Tunisia (Ben Khelil et al., 2019; Tchaicha & Arfaoui, 2020), four from Egypt (El-Gamal et al., 2022; Mowafy et al., 2020; Samari, 2018; Sayed et al., 2023), and five from the Lebanon (Bartels et al., 2019; El-Khoury & Shafer, 2016; James et al., 2021; Lilleston et al., 2018; Veale et al., 2020). Although these are all Arab countries, they are diverse, each having a mixture of languages, differing cultural beliefs, social structures, laws, living arrangements, and attitudes toward women and range from low economic development to high. While the Arab League is a distinct political community, cultural background, identity, governance, and economics differ between the countries. For example, the percentage of full-time women employees in selected Arab League states is lower than that of men, except in Morocco (Ucal & Günay, 2019). In fact, the status of women in the Arab world has always been a sensitive, political issue, and challenging to address, with the Arab Human Development Report (United Nations Development Programme, 2002), designating women’s empowerment as one of the three major deficits impeding development in the Arab world.
Sample Size
The 17 studies yielded a total sample size of 52,310 participants. Variation between the studies meant sample sizes ranged from 18 to 47,545. This related to the variation in research designs from small qualitative descriptive studies (18 participants), randomized controlled trials (648 participants), to large cross-sectional studies (47,545).
Levels of Prevention
Tertiary prevention occurred in seven studies (Damra, 2022; El-Gamal et al., 2022; Lilleston et al., 2018; Mowafy et al., 2020; Sayed et al., 2023; Tchaicha & Arfaoui, 2020; Veale et al., 2020), where women had experienced interpersonal violence (IPV) and interventions educated women about rights, empowerment, and conflict management using a variety of methods. For example, one study used 12 weekly 90-min psychodrama sessions as a therapeutic practice and encouraged participants to use their body to express emotion, rather than verbalize events (Damra, 2022). This study, although small (20 participants), indicated that women participating in the psychodrama sessions displayed significant positive changes in Quality of Life and intimate partner violence, compared to the control group. Another study used six by-weekly face-to-face counseling sessions with a trained counselor for 98 women (Mowafy et al., 2020). Compared to controls, the study found that unconditional positive regard and listening assisted women psychologically, but that educational level and socioeconomic status also played a part in whether a woman remained in an abusive relationship or sought help to assist with the violence (Mowafy et al., 2020). This emphasizes the complexity of VAWG because of the numerous drivers involved. Another study used mobile outreach interventions such as development of support and craft groups, risk mitigation, and individual case management, which reached women in geographically isolated areas and women unable to leave the community (Lilleston et al., 2018). The study identified that in order to be effective, interventions required skilled, creative staff who could build trust and recognize community readiness for intervention. In one study, a female filmmaker asked Tunisian women to comment on the handling of a rape by police and the judiciary (Tchaicha & Arfaoui, 2020). It reported that barriers to women’s empowerment came from dominant patriarchal attitudes, laws lacking in clarity about women’s rights and continued censorship, but noted that progress on women’s rights alongside policy and laws on VAWG had been made in Tunisia since 2014 (Tchaicha & Arfaoui, 2020). One study focused on males, utilizing 12 sessions to work with Syrian and Lebanese refugee males, providing psychosocial support, teaching them how to recognize and emotionally regulate their feelings and reduce aggressive behavior (Veale et al., 2020). Lessons learnt from this study found that including and supporting men as well as women and families not only increased value, but also ensuring a study had a clear aim, scope, and focus; otherwise, its efficacy failed. The lack of effective evaluation emerged because researchers were unclear about what they intended to measure from the outset, it also identifies that evaluations needed to be competent and identify why and how and why they are successful, alongside identifying the minimum elements necessary for success.
Two interventions used leaflets and power-point as educational tools and to promote discussion, but failed to use behavior change theory and measure behavior before and after the intervention; therefore, the studies could not evidence whether the intervention changed behavior (El-Gamal et al., 2022; Sayed et al., 2023). Other evidence suggests that interventions focusing solely on educational or attitudinal components may not be effective in changing behavior (De La Rue et al., 2014; Heise, 2011).
Conservative Middle Eastern culture was a decisive factor in the reduced success of interventions (Damra, 2022). Here, the principle that girls and women are citizens with similar rights and privileges as boys and men is in tension with traditional understandings of women’s roles in Arab League countries. The enforcement of rigid gender roles, such as sister, daughter, wife, mother, and grandmother, emanates from traditional norms portraying women as subjects in need of control rather than individuals with rights. However, Arab women are not passive; Egyptian, Libyan, and Moroccan women have campaigned politically for recognition of their rights (Al Khazrouni, 2014; Johansson-Nogués, 2013). Other countries such as Tunisia and Lebanon do indicate a slow but positive shift toward supporting women and advocating against VAWG, while Saudi Arabia now allows women to drive with the agreement of their families, indicating that Arab countries can change perspectives on women’s rights and roles (Yassin & Hoppe, 2019).
Secondary prevention occurred in three studies, one educated staff about IPV and ways of detecting risk (Alhalal, 2020). However, system-related barriers prevented staff from detecting IPV and teaching women about violence and their rights failed to change attitudes and beliefs. However, this could be an issue with the way measurement of attitudes and beliefs occurred with an absence of standardized measurement instruments in the studies. One study raised awareness of domestic violence with women, used training and reinforcement to support primary healthcare providers in identifying and responding to domestic violence, documented domestic violence, and provided a care pathway for women who disclose domestic violence (Bacchus et al., 2021). It then used normalization process theory to evaluate the intervention. This study identified the importance of context when implementing an intervention because political occupation restricted women’s movements and access to support, coupled with the lack of security and police protection left providers and women feeling exposed to acts of family retaliation. The remaining study used a vignette or narrative exemplar acted by a well-known celebrity to educate women (El-Khoury & Shafer, 2016). Although, using a celebrity had little impact, results suggested that the most positive results came from women with direct and indirect experience of VAWG because their narrative schemas (internalized stories about violence), built from prior experiences, already contained direct or indirect experiences of domestic or interpersonal violence. These prior experiences meant that women were significantly more likely to display negative attitudes toward violence and engage with the messages about preventing violence, listen to the victim or encourage them to seek help and engage in bystander interventions by calling for help. Women with no experience of domestic or interpersonal violence were less likely to engage with prevention messages because their schemas had no foundational knowledge. Therefore, they found it more difficult to consider how helping or intervening to stop abuse would help the victim. This suggests that including women with direct experience of violence enables them to become active participants in intervening to help a victim, whereas women with no narrative schemas about violence became passive recipients of the anti-violence messages.
Primary prevention, for five studies used whole population strategies to prevent VAWG before its occurrence (Bartels et al., 2019; Ben Khelil et al., 2019; Glass et al., 2019; James et al., 2021; Samari, 2018). Barriers to success came from participants (a) possessing low literacy and technology skills, (b) coming from cultural backgrounds and geographic locations, which affected their motivation to attend interventions, (c) a high turnover of staff in non-government organizations affecting the establishment of trusting relationships, (d) fear of social disapproval and discrimination if disclosing violence, (e) a lack of trust in the law because women, or someone they knew had been previously failed by the legal system, and (f) system-related barriers, for example, availability of resources and readiness to support interventions. Low literacy and technology skills may be the result of gendered discrimination in education, particularly in low-income countries.
Two studies operated at more than one level (Bennett & de Lacey, 2017; Colombini et al., 2020). Bennett and de Lacey (2017) used primary and secondary levels of prevention to evaluate whether a system was ready for the intervention to support VAWG. This took 9 months. Evaluation identified several areas needing strengthening to enable effectiveness of intervention. Examples were developing skills of staff to support women, increasing levels of cultural awareness and staffing numbers. A final area in need of strengthening meant identifying ways of reducing overcrowding on clinics to offer women time and privacy to discuss violence. Colombini et al. (2020) used a design operating at primary, secondary, and tertiary levels of prevention when supporting women, training legal staff, and forming community solidarity networks. This particular study took 3 years to implement the interventions at the different prevention levels, indicating complexity, compared to some studies at tertiary and secondary levels of prevention, which ranged from 2 to 13 months.
Discussion
This systematic review produced evidence from 17 publications. Studies reviewed contained one of three levels of prevention, tertiary, secondary, and primary, or a mixture of levels, with length of time for interventions ranging from 2 to 36 months. Several publications were descriptive in nature with no anticipated behavioral or system change outcomes. Most of the publications included preventive programs or interventions designed to elicit positive change to individual behaviors, group behaviors, cultural perceptions, or community systems. However, the paucity of evaluation in many studies meant there was a lack of clarity about the factors necessary for the success of an intervention. The results or outcomes within these 17 publications failed to provide a clear relationship between programmatic or interventional effectiveness and levels of prevention.
Using more than one level of prevention provides the potential to alleviate specific barriers and a more effective outcome. For example, at the primary level of prevention, evidence revealed that issues related to fear and trust are significant and problematic. However, at the secondary and tertiary levels of prevention, barriers to programmatic outcomes including limitations to potential success were reported at interpersonal and community levels, such as perception of security and/or protection, community readiness, and availability of technology. Therefore, this provides the ability to amend interventions as they progress using this evaluative approach at the different levels of prevention. Just two pieces of evidence followed this approach (Bennett & de Lacey, 2017; Colombini et al., 2020), presenting a limitation for our discussion, but an opportunity for future programming and research.
Several studies involved refugees from prior sociopolitical conflict (e.g., war) not directly related to VAWG, yet none sought to intervene or prevent VAWG in direct connection with the conflict. There is a strong correlation between sociopolitical conflict with or without family or community displacement and VAWG (Hossain et al., 2014). There was a paucity of evidence as to how existing systems reduce or prevent VAWG prior to and during conflict because of a lack of evaluation. This presents a gap in the evidence base and an area for improvement. Current programmatic efforts used to address these circumstances appear reactive, and one suggestion may be to advocate for proactive approaches to intervention, prevention, and competent evaluation. For example, using a theoretical background for interventions from the outset such as Theory of Change (Taplin & Clark, 2012), not using single-level interventions and deciding on the specific goals of the program and tying those goals to specific interventions to enable evaluation to occur and identify whether the interventions are effective at producing outcomes. This is a primary suggestion for future VAWG research.
Women in the Arab League may experience the double burden of being a minority group (historically speaking) and a historically underrepresented group (culturally speaking), within a group that fosters and maintains uniformity. A lack of consideration of diversity at the legislative and judicial levels of governance and law enforcement systematically and institutionally harms women (UN Human Rights Office, 2014). At the tertiary level of prevention within this review, evidence indicates institutional barriers in the form of patriarchal dominance preventing new laws designed to protect women, existing laws that are ambiguous, and ongoing censorship of females (Tchaicha & Arfaoui, 2020). The dominant patriarchal mindset is perhaps most damaging because it acts as a barrier in challenging the idea that VAWG is tolerable, and women are to some extent of inferior status. This in turn affects the development of policies upholding women’s rights as equal citizens. Therefore, promotion of women’s rights in policy, more inclusion of women as equal citizens in some Arab societies, clarification of laws protecting women with harsher penalties for perpetrators of VAWG, alongside interventions challenging patriarchal mindsets to consider positive depictions of relationships with women, may assist with creating behaviors that are more acceptable. Arab societies are capable of change and some countries appear more progressive. Perhaps the Arab League can be encouraged to intervene and support the less progressive countries.
The WHO Geneva Convention advocates systems strengthening as one way of improving health outcomes (World Health Organization, 2007). The WHO-INTEGRATE framework considers complexity and identifies whether a system is ready for intervention and implementation (Rehfuess et al., 2019). This evidenced-based approach to population-level health interventions integrates (among other criteria) human rights, health equity, and equality to assessing health systems. Using the WHO guidance, incorporating equity and diversity in the planning/decision-making processes, as a lens through which to analyze the evidence, we can clearly identify that the collective female voice is missing in existing systems and new approaches to addressing VAWG. This indicates gender inequality and an imbalance of power.
Several limitations to the results and discussion within this review should be considered. Firstly, small sample size is an element common to many of the publications reviewed and included in this review, affecting generalizability of the information assessed and reported. Second, decisions made on how to organize and analyze the evidence reflects the multidisciplinary nature of the team. Although we attempted to be as transparent as possible with our methodological reasoning and decision-making, we recognize that this may be a limitation.
Lastly, search parameters for potential publications included a wide-ranging and diverse literature fitting the eligibility criteria. However, we may have unintentionally missed studies due to indexing or other reasons.
Conclusions
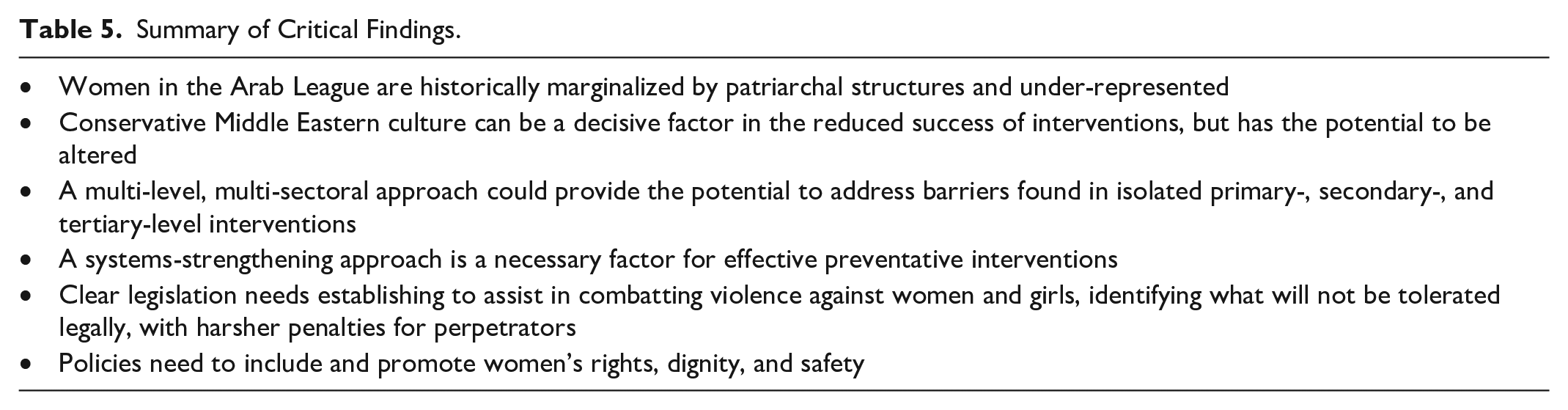
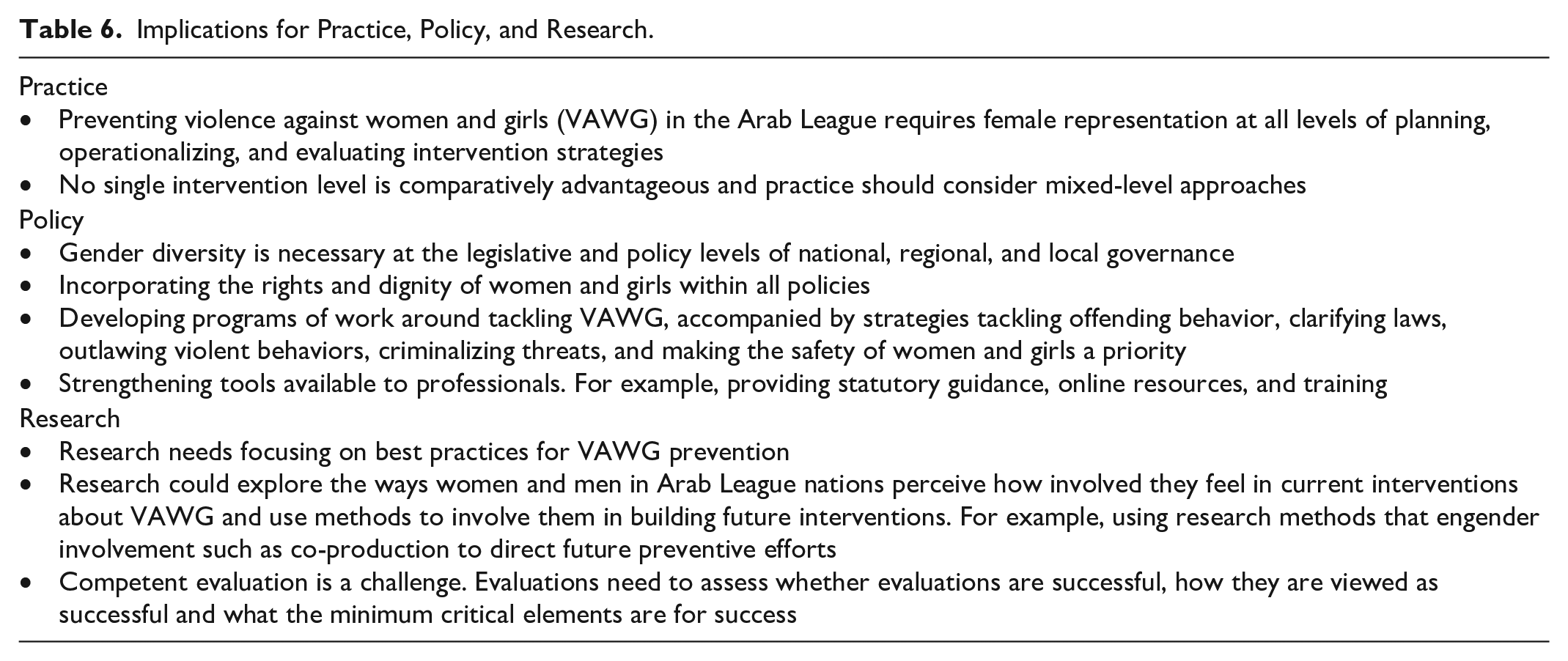
Conservative Middle Eastern culture historically subjects women in Arab League countries to forms of violence. Patriarchal dominance further marginalizes them from decision-making processes to prevent VAWG. All levels of prevention need to include the female voice to gain deeper insights as to ways of preventing the problem; diversity in representation is a key missing element in this systematic review. Another element is the lack of congruent or systematic effectiveness at any preventive intervention level or between levels. Evidence within this review suggests interventions containing multi-level approaches to prevention could alleviate specific barriers found within individual approaches to VAWG (Tables 5 and 6). This may enable further work toward achieving the UN’s Sustainable Development Goal #5 (Gender Equity) by 2030.
Summary of Critical Findings.
Implications for Practice, Policy, and Research.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.