
Abstract
This review aims to contribute to the understanding of violence against women and girls in conflict-affected and fragile settings through a systematic review and meta-analysis to document the available evidence on the prevalence of intimate partner violence and non-partner sexual violence during periods of armed conflict and in post-conflict periods. A total of 45 studies were included. Inclusion criteria were: population-based, observational studies that collected quantitative data with women (aged 15 years or older), included prevalence data on intimate partner violence or sexual violence, was collected in a conflict-affected context (active conflict or within 10 years after conflict) and was self-reported by women themselves. PubMed (Medline), PsycINFO, and Scopus were searched, and Demographic and Health Surveys were included for conflict-affected settings. The search covered literature published between January 1990 and August 2023. The results estimate that 39% of women and girls in conflict-affected settings have experienced physical or lifetime IPV, while 24% reported this violence in the past 12 months. For non-partner perpetrated violence, an estimated 21% of women and girls had experienced this violence in their lifetime and 11% reported having this experience during a period of conflict. When looking at sexual violence overall, an estimated 21% had experienced this violence, though there was considerable heterogeneity depending on the source of this data.
Gender-based violence (GBV) is a global problem affecting about one in three women during their lifetimes (World Health Organization [WHO], 2021). While common during peacetime, there is increasing awareness that situations of armed conflict can increase the risk factors that lead to GBV (Murphy et al., 2023). Feminist scholars have long documented these connections between war and gendered violence. For example, Brownmiller (1975) traced the history of rape in wartime back to the Crusades, while Brownmiller and Barry both explored the use of sexual violence by military men as a facet of warfare and a means to keep up troop morale through access to prostitutes (Barry, 1979; Brownmiller, 1975). Importantly, these feminist scholars conceptualized sexual violence during wartime as a means of power for the subjugation of women rather than fulfillment of sexual desire (Brownmiller, 1975).
While sexual violence has often increased during times of war, it was only in the late 1990s after the widespread media attention paid to violence in Rwanda and the former Yugoslavia that led to global action, such as the establishment of the Women, Peace and Security Agenda and Rome Statue of the International Criminal Court which classified sexual violence as a war crime (Coomaraswamy, 2015; Heineman, 2013; Preventing Sexual Violence in Conflict Initiative, 2019). While these international policy and judicial efforts highlighted GBV in humanitarian settings, they also often conceptualized GBV as only rape (Meger, 2012).
Despite the attention that non-partner sexual violence (NPSV) receives both in the media and from donors of humanitarian aid, existing research suggests that more women and girls experience violence within their own homes compared to violence perpetrated by strangers, even in conflict settings (Stark & Ager, 2011). Feminist scholars place violence against women during the conflict on a “continuum” where pre-existing gender inequalities help shape how women and girls experience violence during and after conflicts (Cockburn, 2004; Moser & Clare, 2001) and demonstrate how violence is experienced in both peace and conflict periods (Brownmiller, 1975).
Recent research has continued to build these connections between public and private violence with studies examining how simply residing in conflict-affected areas is associated with a higher prevalence of intimate partner violence (IPV), suggesting that conflict and humanitarian crises, directly and indirectly, affect the drivers of multiple forms of GBV (Ekhator-Mobayode et al., 2022; Kelly et al., 2018; Svallfors, 2023). In addition, research with women and girls who were directly affected by conflict (e.g., displacement, attacks on village) found that these experiences were associated with higher reported prevalence of both IPV and NPSV, further demonstrating the intersection of violence at the state/community level and experiences of interpersonal violence (Ellsberg et al., 2021).
To bring attention to the issue of GBV, both globally and during times of conflict, there have been sustained efforts to measure GBV prevalence over the past decades. In 2005, one of the first efforts to generate global data on GBV was published in the form of the WHO Multi-country Study on Domestic Violence (WHO, 2005). As part of this effort, a common, act-based measurement tool to collect prevalence data for IPV and NPSV was developed and implemented in 10 countries around the world. In 2013, an effort by WHO to summarize global violence against women and girls (VAWG) prevalence data found that 35% of women and girls had experienced physical or sexual violence in their lifetimes (WHO, 2013). In 2021, these estimates were updated by the WHO which found that 30% of women and girls globally had experienced physical or sexual violence in their lifetime (WHO, 2021). These estimates also showed that 26% of ever-partnered women have experienced physical and/or sexual violence at the hands of an intimate partner at some point in their lives, while an estimated 6% of women experienced NPSV since the age of 15 (WHO, 2021). While these most recent WHO global estimates are informative and based on detailed country-level data and modeling efforts, they reflect global averages which may mask significant differences between contexts. While the report does provide estimates by region (with rates of lifetime IPV ranging from 16% in Southern Europe to 51% in Melanesia) and country, these estimates don’t specifically look at contexts that are impacted by humanitarian crisis and may not include prevalence estimates from displaced populations (such as internally displaced or refugee populations) in their analysis.
The need for specific GBV prevalence estimates for humanitarian settings has been recognized and previous researchers have sought to create overall estimates to demonstrate how many women and girls living in humanitarian crisis experience GBV. For example, Stark and Ager (2011) attempted a meta-analysis of available GBV data from conflict settings but found that a lack of standardized, comparable data prevented a final synthesis. In Vu et al. (2014) conducted a meta-analysis specifically examining rates of sexual violence and estimated that 21% of women and girls in complex emergencies had experienced this violence (Vu et al., 2014). This figure has proved influential in providing a high-level estimate of the percentage of women and girls experiencing sexual violence during an emergency. However, since 2011 there has been no corresponding attempt to synthesize rates of IPV in these settings or create estimates that distinguish between non-partner sexual violence versus sexual IPV, which has impacted advocacy efforts to bring attention to this issue. Given the proliferation of evidence on IPV and NPSV that has been generated in the subsequent decade since these previous articles were published, a new attempt to bring together and synthesize the available evidence on GBV in humanitarian settings is required.
Methods
This article aims to contribute to the understanding of VAWG in conflict-affected and fragile settings through a systematic review and meta-analysis to document the available evidence on the prevalence of IPV and NPSV during periods of armed conflict and post-conflict. The protocol for the review was registered in PROSPERO (#CRD42023436917) on June 27, 2023. The review is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA) guidelines (see Supplemental Appendix 1 for the completed 2020 PRISMA Checklist).
The review included population-based, observational studies that collected quantitative data with women and/or girls (aged 15 years or older) to generate data similar to that presented in the WHO global prevalence estimates for VAWG which focus on populations 15 and older. The primary outcomes were the prevalence of IPV, NPSV, and sexual violence by any perpetrator. All outcomes rely on self-reported binary variables. Only physical or sexual IPV were included in this review to align our results with other international summarization efforts (e.g., WHO global prevalence estimates on VAWG). For violence perpetrated by non-partners, only sexual violence was included. A final measure of “any sexual violence” included any form of sexual violence (IPV, non-partner, perpetrator not specified). For articles where a summary figure for any sexual violence was not available, one measure of sexual violence (either sexual IPV or NSPV) was included in the final analysis.
For the systematic review, all prevalence estimates, no matter their recall period, were included. For the meta-analysis, individual estimates of violence were pooled by lifetime, past 12 months, and during a conflict period (as relevant based on the available data for each measure of violence). Where the recall period or perpetrator was unclear, classification was done based on the context of the study (e.g., rape in the context of a questionnaire about experiences of war-related incidents was assumed to be non-partner sexual violence during a period of conflict).
The population under investigation was conflict-affected women and girls (15 and older) living in an active conflict, or during a post-conflict period (10 years post-conflict). The settings were conflict-affected countries or refugee populations living in countries of immediate refuge (i.e., bordering the conflict-affected country). Conflict-affected settings were defined based on a review of available data from the Uppsala Conflict Data Program’s (UCDP/PRIO) Armed Conflict and Non-State Conflict Datasets (version 23.1) (Gleditsch et al., 2002; Pettersson, 2021; Sundberg & Melander, 2013), where countries that experienced large-scale conflict were classified as conflict-affected. In addition, if a peer-reviewed article self-identified as covering a conflict-affected population (including refugee populations in countries of immediate refuge) they were also included if the data was collected during a time of active conflict or within 10 years post-conflict.
The following databases were searched: PubMed (Medline); PsycINFO; and Scopus. The full search strategy can be found in Supplemental Appendix 2. Bibliographies of relevant articles uncovered by the search were also reviewed for further articles that meet the search criteria. The search covered literature published between January 1990 and August 2023 as this period coincided with a considerable increase in population-based quantitative surveys on violence utilizing similar measures. To complement the data collected through searches of peer-reviewed databases, we analyzed data from the DHS. For large-scale conflicts, countries with DHS surveys within 10 years of conflict either national (if the conflict generally affected most geographic areas) or sub-national (if the conflict was primary focused only on certain regions) estimates were utilized.
Studies were excluded from the review if they did not meet the conditions laid out above (e.g., correct setting, population, outcomes) and in the following circumstances: focusing on qualitative data only, relying on reports of male heads of households (as opposed to women themselves), focusing on assessing similarities/differences in reporting male perpetration and female victimization within couples, focusing on the experiences of active members of formal (state-based) armed forces or veterans of these forces and where the full paper was not able to be accessed.
COVIDENCE was utilized to manage study screening. Abstracts were independently screened for relevance by two reviewers and then, for selected studies deemed potentially eligible after abstract screening, a full-text review was completed by the same two reviewers. The two reviewers periodically met to review any emerging conflicts, and a third reviewer was available to adjudicate any conflicts that could not be solved by the primary reviewers. Data for meta-analysis was extracted to Microsoft Excel independently by each reviewer at the end of the screening process. Key study details (e.g., location, type of study) and prevalence data were extracted for each study.
Data analysis
To prepare the data for meta-analysis, DHS datasets were downloaded from the DHS program website. Violence prevalence estimates for each conflict-affected country or conflict-affected sub-region were calculated in Stata (StataCorp LLC- Version 16) (see Supplemental Appendix 5 for details). Logit-transformed weighted prevalence and variance data for each country (or conflict-affected sub-regions of the country) was calculated.
Prevalence estimates were summarized with pooled prevalence and 95% confidence intervals generated for lifetime, past 12 months, and during conflict (as relevant depending on what recall periods were used for each form of violence in the identified articles). Forrest plots for all estimates were generated. Meta-analysis was undertaken in R using the packages metafor (Viechtbauer, 2010) and meta (Schwarzer et al., 2015). Following the suggested approaches for pooling proportional data (Wang, 2023), random effects models using inverse variance weighting were employed to calculate the summary estimates and the DerSimonian–Laird estimator was utilized to calculate t2 (DerSimonian & Laird, 1986). The summary estimates were then transformed back into proportions for the final presentation, along with measures of heterogeneity (I2 and t2). Estimates were considered highly heterogeneous if they had an I2 of 80% or higher.
To further understand trends within the data, subgroup analysis was undertaken to generate estimates by type of published study (peer-reviewed article vs. DHS survey) as the conditions under which questions about violence are asked can affect disclosure (Ellsberg & Heise, 2005). Sensitivity analysis was undertaken by identifying and removing outliers (defined as studies with z-values of their residual estimates with absolute values exceeding two as suggested by Wang (2023) as well as re-running analysis excluding data collected from health clinic-based studies, which might have reported higher prevalence given the potential correlation of women seeking health services and experiences of violence.
Hoy et al.’s (2012) assessment tool for risk of bias in prevalence studies was used to assess the risk of bias assessment. Two additional criteria were added given the nature of the studies on GBV in conflict settings. For the first, a sample size of 500 or more was assessed as having less risk of bias based on similar assessments in previous reviews of violence in conflict settings (Rubenstein et al., 2020). The second was added to document if procedures related to ethical considerations specific to studies on violence—based on the recommendations from the WHO on researching VAWG—were documented by the study authors (WHO, 2007). The final tool also included domains related to representativeness, sampling strategies and size, case definition/data collection tools utilized, appropriateness of recall period, and how prevalence estimates were calculated (i.e., standard denominators used). This resulted in a score of 0 to 12 (with higher scores equating to less risk of bias). Summary results are presented in the results section and full details of the assessment procedure can be found in Supplemental Appendix 6.
Results
A total of 2,170 studies were reviewed after the initial search, including 2,158 studies identified from academic databases and 12 from other sources (Figure 1). A total of 45 studies were included in the final review, including 35 peer-reviewed articles and 10 DHS studies. Studies were excluded for a variety of reasons including lack of quantitative VAWG prevalence data, the study population under investing was children, the inclusion of other forms of violence in prevalence estimates, and data collected beyond 10 years after the conflict ended.
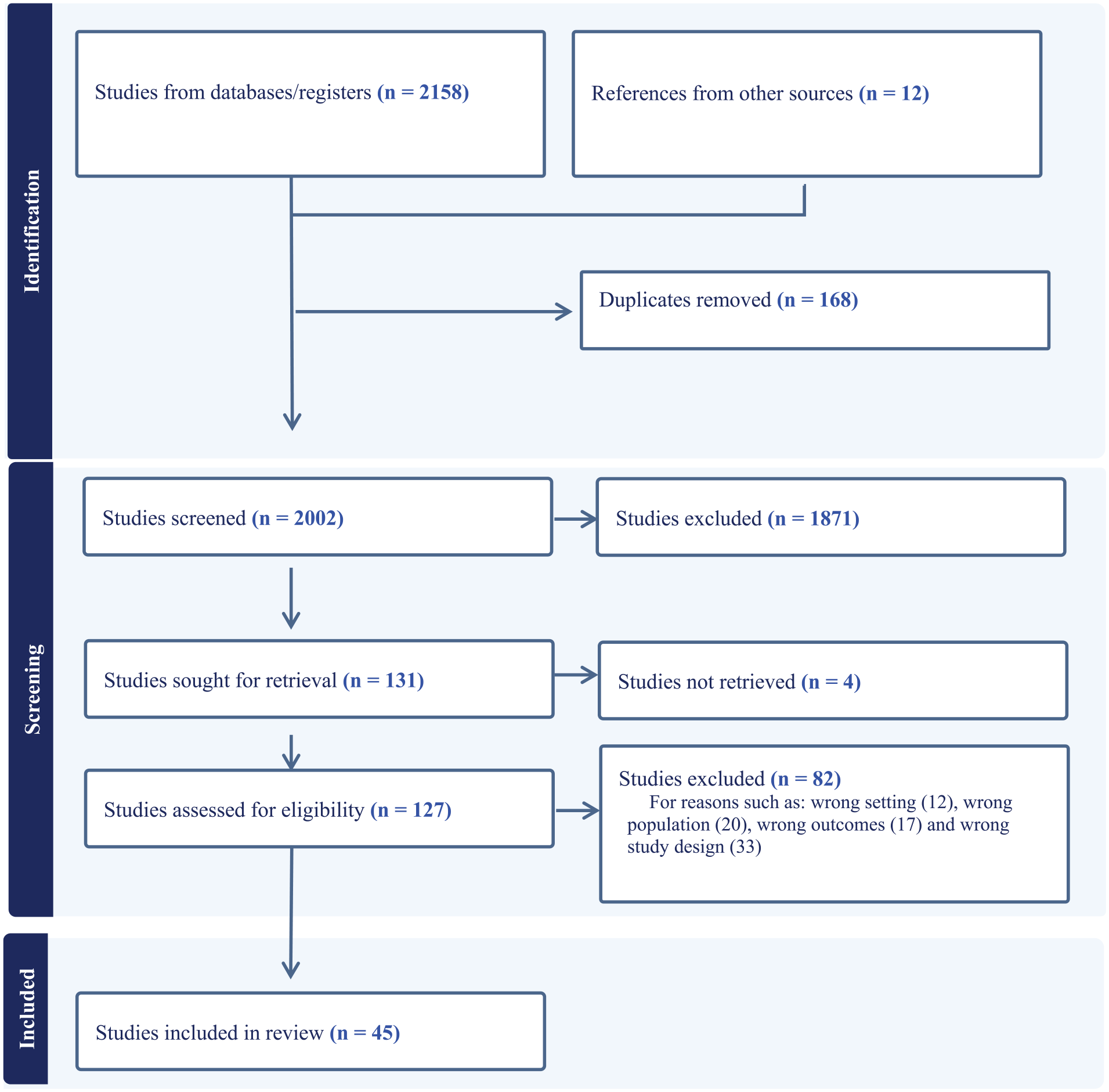
PRISMA flow diagram.
More studies explored the prevalence of IPV in conflict-affected contexts (21 studies reported lifetime physical IPV, 18 reported lifetime sexual IPV) compared to studies measuring non-partner sexual violence in general (eight studies reported lifetime non-partner sexual violence). A further 11 studies looked at experiences of NPSV during conflict periods specifically. An estimate of any form of sexual violence (NSPV, IPV-sexual violence, and sexual violence perpetrator specified) was also produced from the results of 21 studies. For time periods covered, IPV data was generally focused on lifetime or past 12 months’ experiences, while NPSV most often either covered lifetime experiences or specifically looked at a period of conflict. Geographically, the areas covered by the included articles were most often focused on countries within WHO’s African Region (28 studies). Eight studies included countries in the Eastern Mediterranean Region, five studies covered countries from Southeast Asia and four were from the Americas (2) and Europe (2). See Table 1 for a full list of included articles.
Included Articles.

Note. NR: Not reported; HH: Household; *Smallest sample size for violence variables reported when multiple violence indicators included. Countries where data collection took place are reported, though most are not nationally representative. For DHS surveys, if national estimates are used, the country is named. If sub-national estimates of conflict-affected regions are used. Full citations for each DHS report available in the reference list. See Supplemental Appendix 3 for details.
Overall, there was some variety in how IPV, NPSV, and sexual violence were measured across studies, though most studies used some kind of internationally accepted data collection tools (e.g., DHS domestic violence module questions [ICF, 2021], the WHO Multi-country Study tool [WHO, 2005], the Abuse Assessment Screening Tool (Soeken et al., 1998), the Harvard Trauma Questionnaire (Mollica et al, 1992), and the Reproductive Health Assessment Toolkit for Conflict-Affected Women (Hynes et al., 2007)). The vast majority of included studies (n = 36) utilized “act-based” measures of violence that asked if the respondent had experienced a specific act of violence (e.g., asking if the respondent has ever been “forced to have sex,” rather than if they had ever been “raped”) to ensure common understanding of each question. This included 21 studies that specifically used either the WHO or DHS question bank (with only very slight variations, if any) to assess experiences of violence. For questionnaires that did not utilize act-based questions, most studies were focused on wider assessments of war-time traumas experienced (e.g., the Harvard Trauma Questionnaire) and asked limited questions about experiences of GBV—mostly commonly if a respondent had ever been raped.
A 12-point risk of bias assessment was undertaken for each study to classify the risk of bias of including the study in the pooled estimates. Summary results are in Table 2, and details of how each study was scored are available in Supplemental Appendix 6. Overall, there was a wide range of scores, ranging from 3 to 10.5, with DHS studies generally scoring highest (less risk of bias) compared to smaller peer-reviewed studies. However, the score of most included articles was fair (an average score of 7.1 out of 12). Almost all studies used some kind of randomized sampling strategy (86%) and had some kind of sampling frame (village, block, or individual) (89%). Most studies (77%) used recall periods in line with international standards (past 12 months and/or lifetime). Lower scores were seen on indicators such as the sample size (which were generally small), lack of reporting of or large non-response rates, sample/denominator issues (e.g., only calculating IPV variables on those currently married, and samples focusing only on poor women), lack of documentation of the study team following the WHO’s ethical and safety principles and estimates that were not nationally representative.
Risk of Bias Summary (1–12 With Higher Scores Less Risk of Bias).

Note. DHS Afghanistan not assessed as only the dataset (rather than the full report) was available.
For the meta-analysis we generated estimates of IPV, NPSV, and sexual violence from any perpetrator. Results of each analysis are explored below.
Intimate Partner Violence
For IPV, we estimated pooled prevalence for lifetime experiences of physical, sexual, and physical or sexual violence (see Figure 2).
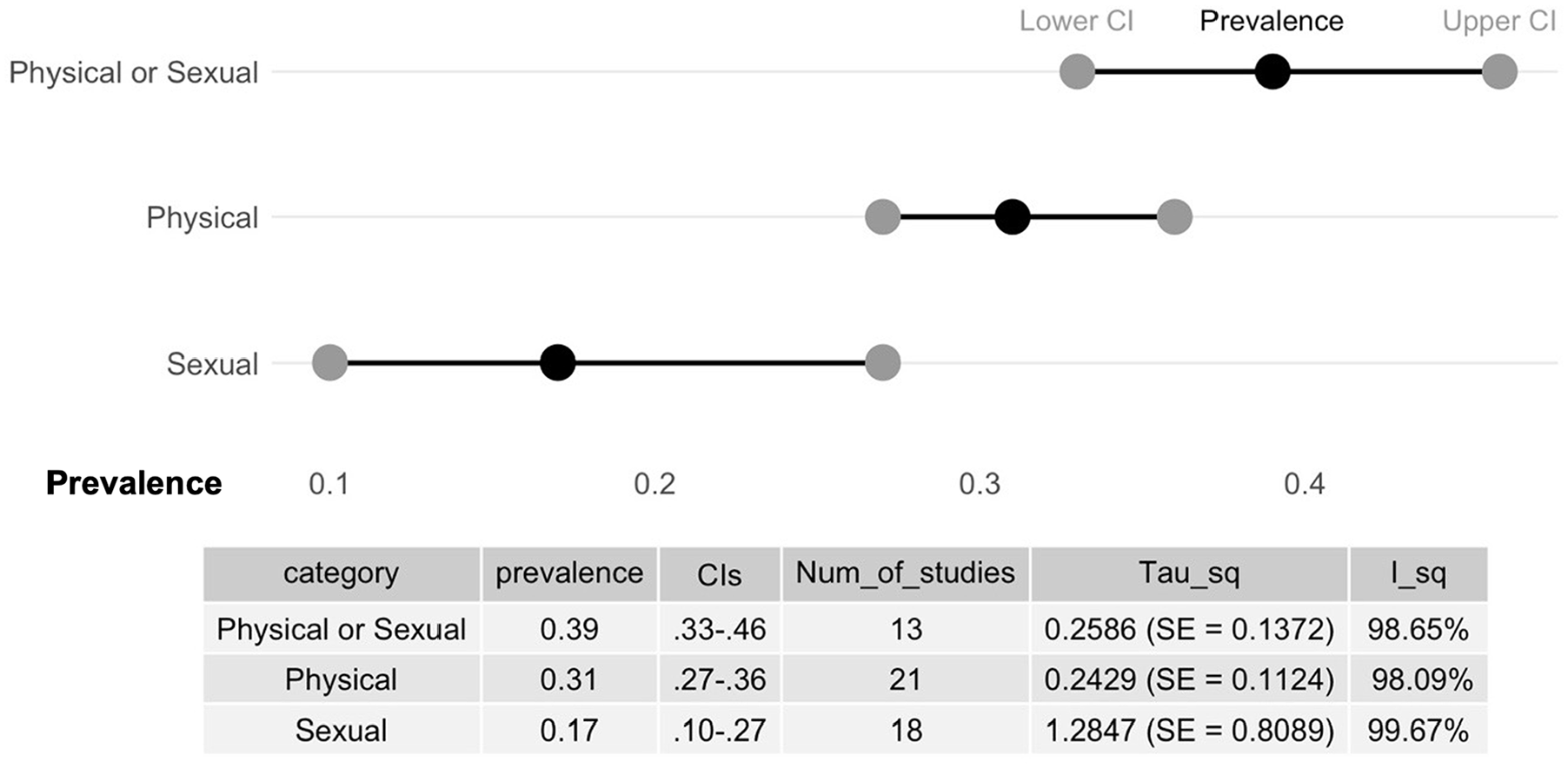
Pooled estimates of lifetime IPV.
We identified 13 studies that had estimates of lifetime physical and/or sexual IPV (Figure 3). The pooled prevalence of women and girls reporting experiences of lifetime physical or sexual violence was 39% (95% CI [33, 46]; I2 = 98.65%; t2 = 0.2586; 13 studies; 48,398 participants). Estimates derived from DHS studies only (PR: 39%; 95% CI [32, 46]; I2 = 97.98%; t2 = 0.1827; 9 studies) and peer-reviewed articles only (PR: 40%; 95% CI [26, 57]; I2 = 99.23%; t2 = .0.4648; 4 studies) were similar (p value for sub-group heterogeneity = .8381; see Appendix 7, Supplemental Figure 1). In sensitivity analysis, one study (Ellsberg et al., 2020) was identified as a potential outlier, however when removed the overall estimate stayed consistent (PR: 37%; 95% CI [32, 43]; I2 = 97.81%; t2 = 0.1675; Appendix 7, Supplemental Figure 2).
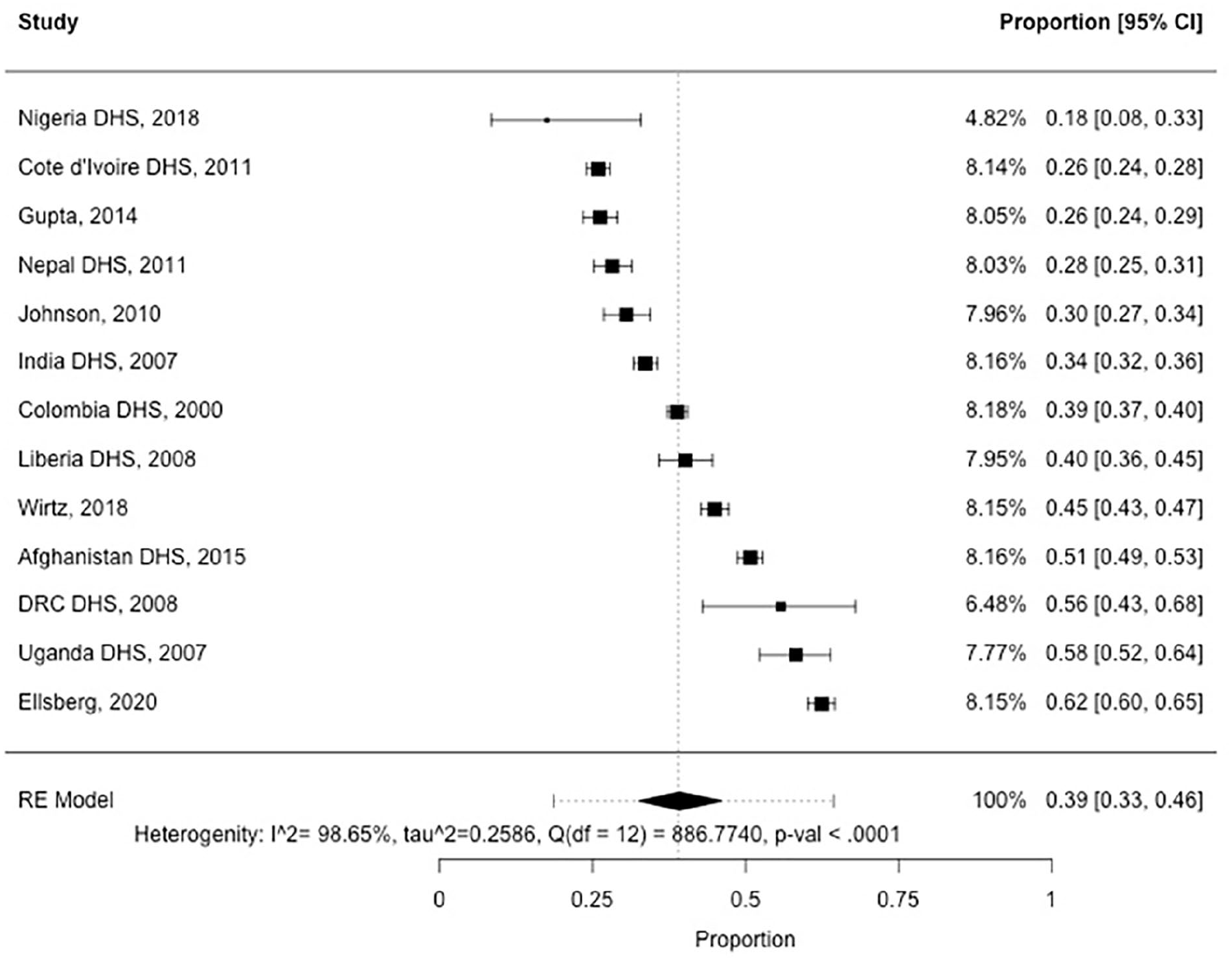
Pool estimates of lifetime physical or sexual IPV.
We included a total of 21 studies with estimates of lifetime physical IPV. The pooled prevalence was 31% (95% CI [27, 36]; I2 = 98.09%; t2 = 0.2429) of women and girls experiencing lifetime physical IPV (52,895 participants; Appendix 7, Supplemental Figure 3). Cross-sectional surveys were used as the data collection methodology in 21 of the 22 included studies and the overall estimated prevalence remained similar in a sensitivity analysis (PR: 30%; 95% CI [26, 35]; I2 = 98.05%; t2 = 0.2314) when excluding one study of health clinic attendees (Al-Modallal et al., 2015; Appendix 7, Supplemental Figure 4). In subgroup analysis, pooled estimates from DHS data (10 studies) were larger (PR: 37%; 95% CI [30, 44]; I2 = 98.28%; t2 = 0.2194) than estimates pooled from peer-reviewed articles (PR: 27%; 95% CI [20, 34]; I2 = 98.29%; t2 = 0.3626; 11 studies; p-value for sub-group heterogeneity = .0496). See Appendix 7, Supplemental Figure 5 for details.
Lifetime experiences of sexual IPV was pooled from the results of 18 studies, with an overall prevalence estimate of 17% (95% CI [10, 27]; I2 = 99.67%; t2 = 1.2847; 55,464 participants; Appendix 7, Supplemental Figure 7). In subgroup analysis, the estimate derived from peer-reviewed articles (nine studies) were much larger (24%; 95% CI [13, 40]; I2 = 99.66%; t2 = 1.3143) than those from DHS studies (12%; 95% CI [9, 16]; I2 = 95.16%; t2 = 0.2064; nine studies; p-value for sub-group heterogeneity = .0562). See Appendix 7, Supplemental Figure 8 for more details. In sensitivity analysis, the overall prevalence estimates remain quite similar (PR: 15%; 95% CI [10, 21]; I2 = 99.14%; t2 = 0.7476) to the main estimate when one potential outlier study was removed (Stark et al., 2013; Appendix 7, Supplemental Figure 9). All studies pooled to create the overall estimate of lifetime experiences of sexual IPV came from studies that utilized household surveys as their data collection methodology.
Studies that explored IPV in the past 12 months were generally separate from studies that examined lifetime rates of violence, with few studies examining both recall periods. Generated estimates of IPV in the past 12 months (Figure 4) based on the available studies were similar to lifetime estimates of IPV. Rates of past 12 months physical or sexual IPV were estimated to be 24% (95% CI [16, 35]; I2 = 99.08%; t2 = 0.5676; eight studies; 32,253 participants; Appendix 7, Supplemental Table 10). Fifteen studies were pooled to create a summary prevalence estimate of experiences of physical IPV in the 12 months prior to the survey, and an overall estimate of 27% (95% CI [20, 35]; I2 = 98.92%; t2 = 0.5573; 38,266 participants) was calculated (Appendix 7, Supplemental Table 11). Pooled estimates of sexual IPV in the past 12 months (17%; 95% CI [8, 28]; I2 = 99.21%; t2 = 1.5993; 13 studies; 34,061 participants) were also generated (Appendix 7, Supplemental Table 12).
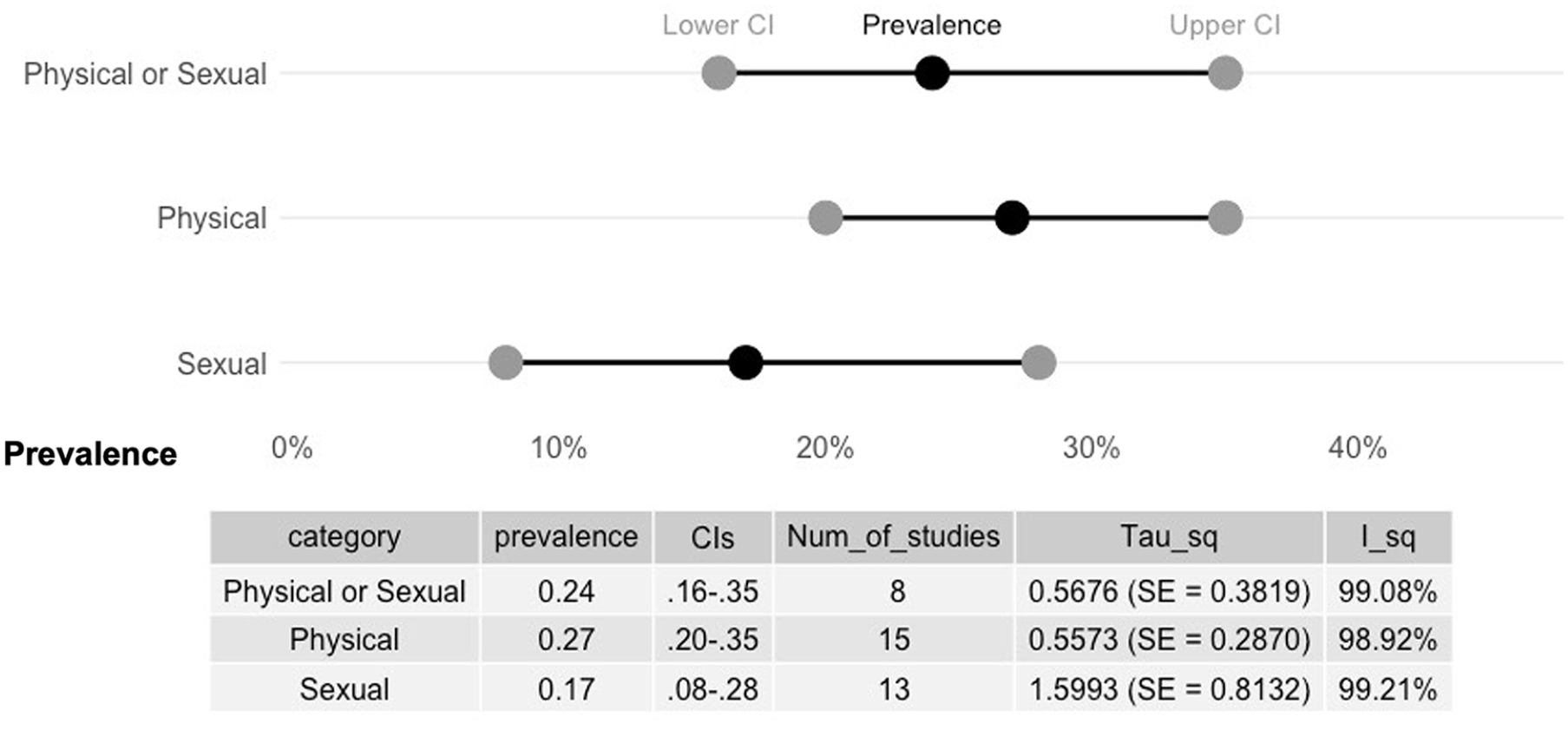
Pooled estimates of IPV in the past 12 months.
Non-Partner Sexual Violence
Turning to NPSV, pooled estimates were lower than estimates of experiences of IPV (Figure 5). Using data from eight studies, 21% (95% CI [13, 30]; I2 = 99.22%; t2 = 0.5416; 16,737 participants) of women and girls were estimated to have experienced NSPV in their lifetime (Appendix 7, Supplementary Figure 13). In sensitivity analysis, these estimates generally did not change (PR: 21%; 95% CI [15, 29]; I2 = 98.76%; t2 = 0.2668) when two potential outlier studies (Morof et al., 2014; Wirtz et al., 2018) were removed (Appendix 7, Supplemental Figure 14). For studies that specifically examined NSPV during a conflict period (often, though not exclusively, defined specifically conflict-related violence) was estimated to be 11% (95% CI [7, 18]; I2 = 97.74%; t2 = 0.7022; 11 studies; 7,948 participants; Appendix 7, Supplemental Figure 15). This estimate does not generally change when one potential outlier (Ainamani et al., 2020) was removed (PR: 11%; 95% CI [9, 14]; I2 = 90.94%; t2 = 0.1415; Appendix 7, Supplemental Figure 16).
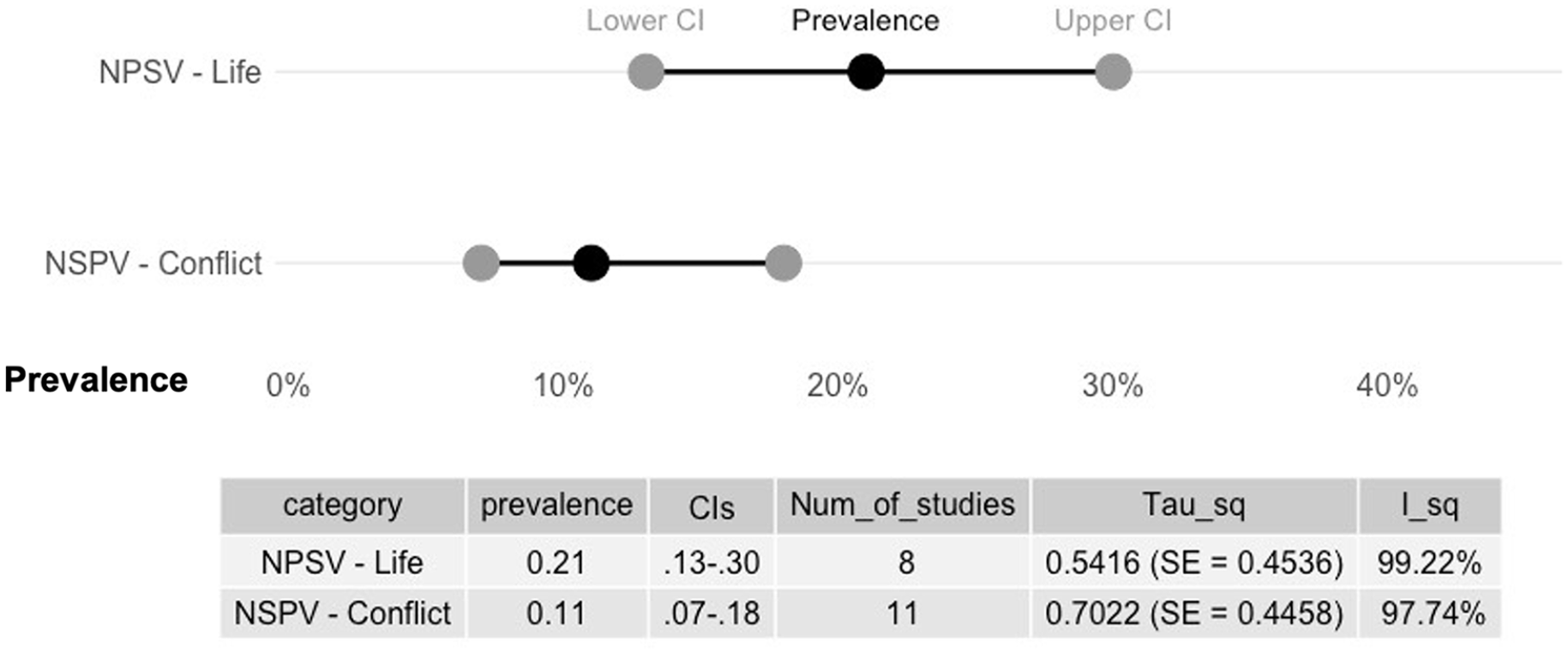
Pooled estimates of NPSV.
Sexual Violence—Overall
Lifetime sexual violence from any perpetrator (any sexual violence, non-partner sexual violence, or sexual IPV) was estimated to be 21% (95% CI [14, 30]; I2 = 99.63%; t2 = 1.0654; 21 studies; 67,586 participants; Supplemental Appendix 7, Figure 17). Estimates based on data from peer-reviewed articles (PR: 28%; 95% CI [20, 37]; I2 = 99.42%; t2 = 0.6246; 12 studies) were much higher than those based on DHS data (PR: 14%; 95% CI [9, 21]; I2 = 98.54%; t2 = 0.4759; nine studies; Figure 6).
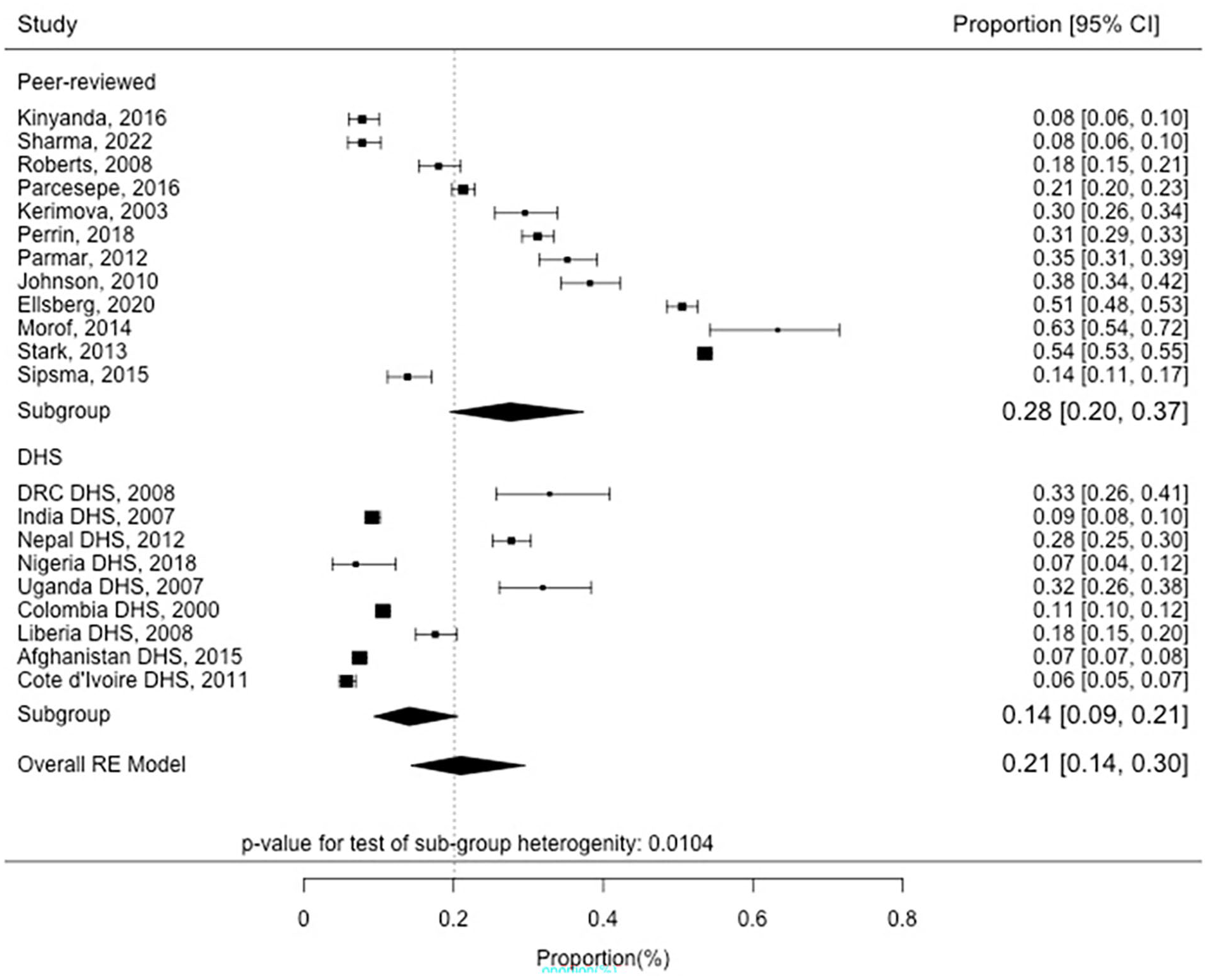
Estimates of sexual violence—Peer Reviewed versus DHS data.
Discussion
This review provides the first systematic effort to estimate the lifetime prevalence of both IPV and NPSV, as well as an aggregate estimate of the proportion of women who have experienced any type of sexual violence in conflict settings. The results estimate that 39% of women and girls in conflict-affected settings have experienced physical or lifetime IPV, while 24% reported this violence in the past 12 months (see Table 3 for the study’s critical findings). For non-partner perpetrated violence, an estimated 21% of women and girls had experienced this violence in their lifetime and 11% reported having this experience during a period of conflict. When looking at sexual violence overall, an estimated 21% had experienced this violence, though there was considerable heterogeneity depending on the source of this data.
Critical Findings.

Note. GBV = Gender-based violence; IPV = intimate partner violence.
Overall, compared to previous efforts to synthesize prevalence rates of GBV in conflict settings (e.g., Stark & Ager, 2011; Vu et al., 2014), this review was able to rely on data from relatively rigorous cross-sectional household surveys and generally excluded data from studies based on convenience samples, which were almost all that was available 10 years ago. The included studies in this review utilized relatively rigorous sampling methods (generally employing a sampling frame and some form of random sample), standardized recall periods, and adhered to international best practices in defining violence. For example, for measures of prevalence of IPV, the use of lifetime and/or past 12-month recall periods was almost uniformly employed across studies. In addition, most studies utilized standardized questions employed by the WHO Multi-Country Tool for Domestic Violence and/or the DHS Domestic Violence module. This represents a marked improvement in the availability of data on the issue of GBV in conflict-affected settings, though deficiencies (e.g., small sample sizes, study tools not validated in study settings, and differences in how violence variables are calculated) remain commonplace as these improvements were coming from a particularly low baseline in terms of study quality (Stark & Ager, 2011).
While there has been improvement in the standardization of measures of GBV overall, there are some differences that could affect the quality of our estimates including variations in underlying populations, recall periods, measurement tools, etc. For example, there was variation in age ranges (minimum ages 15 or 18; maximum ages 49, 64, or none), denominators (e.g., ever married, currently married, and ever partnered) utilized to calculate IPV, and sample populations (e.g., poor women, recently married women, and health clinic attendees) across articles. In addition, some studies that measured IPV were completely excluded from this review as they included other forms of IPV (primary psychological violence) in their overall estimates and did not provide disaggregated figures for only physical or sexual IPV.
In addition, differences in recall periods were common for studies examining NPSV and sexual violence in general—as many of the included studies were specifically interested in sexual violence that occurred during a conflict period. As each country’s conflict lasted a different length of time, this naturally leads to more variation in recall periods. However, some tools had unclear recall periods or, while stating they were exploring lifetime experiences of violence, were structured to be specifically exploring war-related incidents of violence. Similarly, the perpetrator of violence was not always clear in all data collection tools/studies and some of these tools focused on war time trauma exposure rather than GBV. These tools often only relied on a single question to assess experiences of sexual violence rather than utilizing a more complete definition that includes sexual assault or defining these topics (e.g., “have you ever been forced to have sex when you didn’t want to” rather than “have you ever been raped”) to ensure respondents have a common understanding of what is being asked.
Overall, the results of the meta-analysis produced estimates that are broadly in line with other efforts to generate global summary data for rates of GBV (e.g., WHO global estimates, and previous meta-analysis for conflict-affected populations). For IPV, our study suggests that more than one in three (39%) ever-partnered women and girls in conflict settings experience physical and/or sexual IPV, which is higher than the overall WHO global estimates of one in four women (26%). As the WHO estimates are based on country, regional, and global level modeling efforts, our study’s methods (meta-analysis of published prevalence data) do not necessarily allow for direct comparison with these figures. However, given the increased risk factors for experiencing IPV present in conflict-affected locations (e.g., increased poverty, breakdown of rule of law, increased presence of alcohol, drugs and guns, and normalization of violence), our findings are in line with theorized higher rates of GBV in conflict-affected areas (e.g., Murphy et al., 2023) and the results of other country-specific studies (e.g., Ellsberg et al., 2021; Kelly et al., 2018, etc.) that found that exposure to conflict is associated with higher rates of GBV. Rates of past 12 months physical and/or sexual IPV (24%) were also larger than the global WHO estimates during the same recall period (10%), potentially reflecting the increased risk factors contributing to experiences of violence during a conflict period as well as the lack of ability for women and girls to leave a violent relationship when their normal informal (e.g., proximity to family and access to employment) and formal (e.g., women’s centers and police) support structures have broken down.
Turning toward experiences of sexual violence in conflict-affected contexts, overall pooled estimates of lifetime NPSV (21%) and studies that specifically looked only at conflict-affected periods (11%) were much larger than global lifetime WHO estimates of NPSV (6%) (WHO, 2021). Estimates which sought to pool together all forms of sexual violence found similar results (21%). These estimates were very similar to Vu et al.’s (2014) previous meta-analysis results of sexual violence in complex emergencies (21%), further providing support for those results. These similarities are particularly interesting as they were generated despite some differences in the articles included in both reviews due to differences in inclusion/exclusion criteria and the proliferation of more rigorous studies in the past 10 years.
Importantly, there were some differences in our estimates depending on the type of study, with differences in the prevalence estimates generated when using only DHS studies compared to estimates from smaller academic, peer-reviewed studies. These differences were particularly evident in sexual violence variables where estimates collected through peer-reviewed studies resulted in larger pooled estimates compared to those from DHS datasets. For example, estimates of sexual IPV from peer-reviewed articles were double those from DHS studies (24% vs. 12%). Similarly, estimates of sexual violence overall were higher (28%) when examining data from peer-reviewed papers compared to those from DHS studies (14%). This suggests there are potential biases (e.g., recall, and social desirability) that might affect the DHS more strongly than smaller studies when examining very sensitive issues such as sexual violence—particularly in conflict-affected settings where sexual violence is highly stigmatized (Rose, 2023).
Generally, across the evidence base, we see that studies that focus specifically on the issue of GBV alone tend to generate larger prevalence estimates compared to studies that focus on a wider variety of topics. While many studies in this review (including the peer-reviewed literature) included GBV as one of many topics under investigation, some of the largest prevalence estimates were generated by studies with GBV as the single focus (e.g., Ellsberg et al., 2021; Parcesepe et al., 2016; Stark et al., 2013; Wirtz et al., 2018). Women’s willingness to disclose experiences of sexual violence is highly sensitive to methodological and safety issues, such as privacy and confidentiality, the number and phrasing of questions, whether the interview is face-to-face or uses methods that allow for anonymous reporting, the stigma attached to sexual violence, fear of retaliation by abusers, and the skill of interviewers (Ellsberg & Heise, 2005). Large-scale, multi-issue studies, such as the DHS, might be particularly likely to under-report experiences of sexual violence given the sensitive nature of this data, the difficulty in ensuring privacy during the interview, and the required trust needed to be built up between interviewer and respondent. For physical violence, particularly in locations where violence is widely accepted and tolerated, this same reluctance to disclose during a multi-topic survey might not be as common—reflected in more similarity in rates of physical IPV generated from DHS and peer-reviewed studies.
Overall, this article presents an attempt to synthesize the best available evidence on GBV in conflict-affected settings. However, several limitations have affected the efforts. For example, while there have been improvements in measurement consistency, the review team had to make decisions about how to pool data with different recall periods from the standard lifetime and past 12 months as well as measures that were unclear about who perpetrated the violence. Furthermore, there is still limited prevalence data on the issue of GBV in conflict-affected settings, and the fact that we were pooling data from different countries/contexts (i.e., studies estimating lifetime and past 12-month rates of violence were typically from different studies/contexts) contexts to generate each estimate could affect our results. In addition, the demonstrated heterogeneity of results depending on the study source (DHS vs. peer viewed, multi-issue vs. GBV-specific) affects our confidence in our overall estimates. Finally, there was an overall lack of diversity in the dataset, with most studies taking place in conflict-affected Africa, making this attempt at global estimates likely biased to the African context.
Despite these constraints, the results of this analysis are still important for the field. While rates of GBV likely vary considerably between conflict-affected contexts, when we look at rates of GBV in the WHO global estimates we also see considerable variation by country/region (WHO, 2021). Overall, GBV in both conflict and non-conflict contexts is caused by unequal power and patriarchy. These inequitable gender norms have been associated with higher rates of GBV in previous research (Heise & Kotsadam, 2015). We therefore expect experiences of conflict to interact with these pre-existing conditions and norms, both introducing new drivers of GBV and compounding existing ones (Murphy et al., 2023). As such, the prevalence of IPV and NPSV prior to conflict in any context would also affect violence rates after a conflict begins—reflecting considerable variation in rates of GBV both in peacetime and during conflict and affecting any effort to pool data across sites.
While these overall estimates of pooled prevalence may mask these variations of individual contexts, they do provide some utility. Importantly, they provide an initial estimate for programmers and policymakers to utilize in conflict-affected settings where data about prevalence rates of GBV is often limited. As noted in the Inter-Agency Standing Committee (2015) GBV Guidelines, collecting GBV prevalence data in acute emergencies “is not advisable due to methodological and contextual challenges related to undertaking population-based research on GBV in emergency settings (e.g., security concerns for survivors and researchers, lack of available or accessible response services, etc.)” (IASC, 2015). Therefore, these types of analysis efforts can provide programmers and policymakers with summary estimates to help inform their work, without putting survivors at additional risk by collecting additional primary data during a conflict.
They also draw attention to forms of violence—such as IPV during emergencies—that traditionally might not be prioritized in policy response during a conflict. The results of this review and meta-analysis provide further evidence that rates of IPV are higher in conflict-affected settings and that more women and girls experience IPV compared to NPSV. They point to the importance of considering IPV prevention and response as key programming in conflict-affected settings. While still limited, there have been more efforts in recent years to implement and evaluate programming in conflict-affected settings that focus on reducing both IPV and NPSV (Spangaro et al., 2021). Further investment in these types of programming—considering both IPV and NPSV—is needed. See Table 4 for further recommendations.
Key Recommendations for Practice, Policy, and Research.
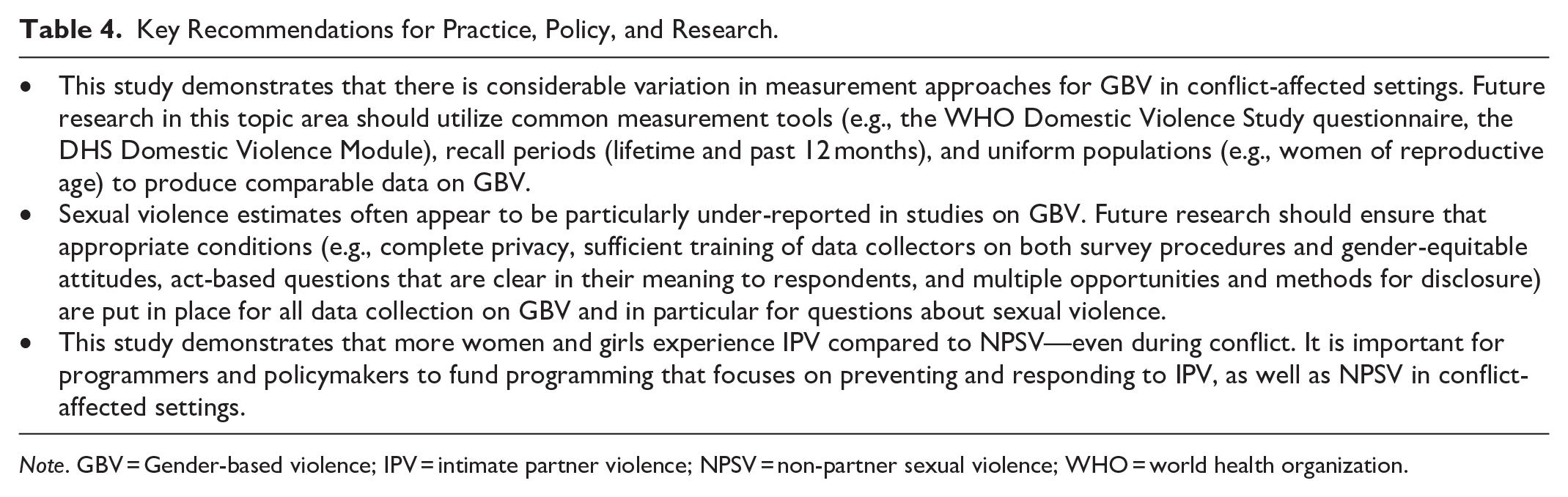
Note. GBV = Gender-based violence; IPV = intimate partner violence; NPSV = non-partner sexual violence; WHO = world health organization.
The results of this study demonstrate the high rates of violence that women and girls are experiencing in conflict-affected settings. They also point to the improving breadth and quality of data on GBV in conflict-affected settings. Researchers should continue to build this evidence in safe and ethical studies that draw upon the learning of GBV researchers globally and apply the WHO’s Ethical and Safety Recommendations for Researching, Documenting, and Monitoring Sexual Violence in Emergencies (WHO, 2007) to ensure the estimates produced are reliable and do not put participants at undue risk during or after data collection. High-quality data on GBV in conflict settings is possible, but the safety of women and girls should remain central to any research efforts. Policymakers and practitioners should continue to advocate for more evidence-based GBV programming but should work in partnership with academics to prioritize safety and ethics within these efforts.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241305355 – Supplemental material for Experience of Intimate Partner Violence and Non-Partner Sexual Violence in Conflict-Affected Settings: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-tva-10.1177_15248380241305355 for Experience of Intimate Partner Violence and Non-Partner Sexual Violence in Conflict-Affected Settings: A Systematic Review and Meta-Analysis by Maureen Murphy, Emily R. Smith, Shikha Chandarana and Mary Ellsberg in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
Thanks to Dr Vandana Sharma, Diana Arango and Dr Jennifer Seager for their reviews and comments on drafts of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Government of the United Kingdom’s Foreign, Commonwealth and Development Office (Contract #3680). The findings and opinions are those of the authors and not the Government of the United Kingdom.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.