
Abstract
Sexual violence (SV) is a widespread public health and human rights problem, with countries in East Africa having higher rates than the global average. Prosecutions of SV in East Africa are rare, and survivors face many challenges accessing medico-legal justice and services. Developing initiatives that support survivors in navigating the criminal justice system is vital, yet there is limited research on efforts to improve the criminal justice system’s management and treatment of survivors. We conducted a scoping review of research on initiatives to strengthen responses toward investigating and prosecuting cases. We identified 25 academic articles and reports through a search of electronic databases and gray literature that address these initiatives in East Africa. The results reveal that seven types of initiatives have been studied: one-stop centers (OSCs), multisectoral referral networks, gender desks, community interventions, mobile applications, and specialized police and prosecution units. Upon review, we found that barriers to success include a lack of resources and facilities, a lack of trained health care, police, and judicial personnel to perform services, weak medico-legal partnerships, and stigma and impunity restricting the uptake and fair distribution of services. Overall, limited systematic evidence on the effectiveness and adaptability of initiatives exists, showing that SV interventions in East Africa remain an under-researched and under-resourced area, and need greater scientific rigor to inform practice and coordinated advocacy. This review is a call to action for policy makers and service providers working in East Africa—and for international bodies working toward achieving Sustainable Development Goals 5—to improve criminal justice initiatives.
Keywords
Introduction
The United Nations (UN) defines sexual and gender-based violence (SGBV) as an act that is based on societal gender norms between males and females where consent is not obtained or freely given (UNHCR, 2011). These acts can cause physical, mental, or sexual harm, and include rape, forced or early marriage, and other forms of violence committed by intimate partners and non-partners (Beyene et al., 2019; World Health Organization (WHO), 2007). Sexual violence (SV) falls under the SGBV umbrella, occurs in times of peace and conflict, and is one of the world’s most traumatic and widespread human rights abuses (Garcia-Moreno et al., 2005; Tulchinsky & Varavikova, 2014). The WHO defines SV as “any sexual act, attempt to obtain a sexual act, unwanted sexual comments or advances, or acts to traffic, or otherwise directed against a person’s sexuality using coercion, by any person regardless of their relationship to the victim, in any setting including but not limited to home and work” (World Health Organization/London School of Hygiene and Tropical Medicine, 2010). SV is considered to be both a human rights violation and a public health issue that impacts every community and is associated with a range of adverse effects on the wellbeing of survivors and their families (Garcia-Moreno et al., 2005).
Data on SV is critically important for developing, financing, and coordinating initiatives that support survivors, yet SV is notoriously difficult to investigate, and there is a scarcity of reliable, easily accessible information (Akpoghome et al., 2021). The WHO estimates that one in three women globally will experience some form of physical and/or SV in their lifetime (WHO, 2021). The prevalence of SV in East Africa is higher, especially in regions with low gender equality scores, where social norms that stigmatize survivors prevail and limit effective prevention and response strategies (WHO, 2021). Despite evidence of how pervasive SV is—and growing efforts of policymakers to eliminate it—SV in East Africa remains an under-researched and under-resourced area, especially considering the high population areas and poverty rates that put a strain on services for survivors (Aust et al., 2019; UNGA, 2006; WHO, 2013).
Comparing data on SV within East Africa is difficult due to variations in legislation, definitions, and concepts that limit policy transfer and coordinated advocacy between countries (Kilonzo et al., 2009). Statistical estimates of SV are often aggregated with other types of violence, which makes it difficult to ascertain the rate of SV alone. Further, intimate partner SV rates are measured more often than non-intimate partner SV rates. Nevertheless, the prevalence of SV in East Africa appears to be higher than the WHO estimated global average. For instance, the lifetime prevalence of physical, sexual, or emotional violence committed by a partner against women is 47% in Kenya (Institute of Medicine & National Research Council, 2015), the lifetime prevalence of SV committed by an intimate partner against women is 59% in Ethiopia province (Garcia-Moreno et al., 2005), the lifetime prevalence of physical and/or SV against women is 43.6% in Tanzania province (Garcia-Moreno et al., 2005), and the prevalence of physical violence and/or SV is 63% among women in Uganda (Sensasi, 2014).
SV prosecutions are rare around the world, including in East Africa (Bohner et al., 2009; Brown et al., 2007). Victims often do not report to the authorities, and perpetrators are seldom arrested and held accountable (Akpoghome et al., 2021). In many countries, survivors do not know the law and their rights, or have trust in the judicial process. They may be silenced by financial barriers, a culture of stigma and impunity, or overly bureaucratic and poorly resourced systems (Owiti et al., 2018). They might encounter corruption, non-empathetic responses (hostility, blame etc.), or discrimination from police and law enforcement, and risk reprisal from perpetrators and backlash from their communities if they do report (Akpoghome et al., 2021; Seelinger, 2014). Thus, there are many barriers to disclosing SV, with the perceived costs of reporting an incident (e.g., re-traumatization, stigmatization, etc.) often outweighing its anticipated rewards (Ji et al., 2022). Consequently, SV survivors often instead rely on their community’s resources and informal accountability methods (McGlynn et al., 2016; Wagner et al., 2022).
Among those who choose to report to the authorities, survivors face further challenges in accessing vital services (e.g., emergency medical care, safe shelters) along the medico-legal system. “Forensic” or “medico-legal” evidence is essential in the investigation and prosecution of rape in many countries around the world, including those in East Africa (Kilonzo et al., 2009). For instance, in Kenya, if the survivor chooses to disclose the assault to the police, they must have had a forensic medical exam by an approved government provider (Gaitho et al., 2020). The provider will document the crime, the injuries, and forensic evidence on an official government form (i.e., the Post Rape Care form) (Olson et al., 2022). Moreover, survivors of SV must disclose to medical providers that they have been violated to receive free medical services (S. R. Rockowitz et al., 2021). Without a forensic medical exam, the case will not be pursued by the police. High-quality, timely documentation of forensic evidence has been shown to increase trial prosecution, conviction rates, and survivor agency (Gray-Eurom et al., 2002; Kjærulff et al., 2019). Consequently, a functional chain of obtaining, preserving, and conveying evidence from the community and health facility to the police is vital for survivors who seek justice.
Developing effective strategies that help survivors access services at the intersection of medical and justice processes is complex and requires coordination between a range of actors (WHO, 2015). Resource constraints and a lack of trained health care workers or police impede survivors’ access to care and justice (Gaitho et al., 2020). Examples of this are: health centers being poorly equipped and lacking adequate facilities for specimen testing and/or the examination and legal documentation of injuries (Holmes & Bhuvanendra, 2014); clinics being difficult to access due to distance and lack of transportation; survivors having to recount their experiences to varied providers who are not skilled in trauma-sensitive interviewing, post-rape care, or forensic medicine (Morel-Seytoux et al., 2010); survivor and witness testimonies being recorded after long delays that decrease their ability to recall the attack precisely; and survivors being discouraged from accessing support due to having to report crimes to the police as a condition of receiving health care (Stevens et al., 2022).
Implementing initiatives that create positive change for the way in which survivors are managed and treated by the criminal justice system is essential to improve their experience of disclosing SV to authorities and their ability to access vital services and justice. In this paper, we present a scoping review of research on initiatives that have been implemented to strengthen the criminal justice system response toward SV in East Africa, including coordinated response centers, 1 medico-legal practitioner training, programs that provide information to the public about SV laws and survivors’ rights, gender desks, 2 specialized police forces, 3 and mobile applications for documenting forensic evidence.
Our goals are to identify the types of initiatives that have been tested to address shortcomings in medico-legal responses, evaluate the scientific rigor of past research, and summarize the conclusions reached by the authors regarding their effectiveness, as well as barriers and opportunities for implementing them. Understanding the strength and weaknesses of medico-legal systems, as reported in the literature, will demonstrate why survivors’ cases often fail to progress through the criminal justice system. It will further help identify opportunities to strengthen medico-legal partnerships in responding to SV and support more effective case prosecutions. We focus on East Africa to consolidate lessons learned on criminal justice and service delivery in this region, demonstrate where resources are needed to better support survivors, identify best practice initiatives, and facilitate cross-country advocacy, up-scaling, and adaptability of survivor-centered care.
Method
The search strategy involved keyword searches of academic databases and targeted searches of gray literature. Web of Science, PubMed, Science Direct, Embase, and Cochrane were searched using keyword search strings. These included: “sexual violence” + “Africa” + “criminal justice”; “sexual violence” + “Africa” + “criminal justice interventions”; “sexual violence” + “Africa” + “police”; “sexual violence” + “Africa” + “legal”; “sexual violence” + “Africa” + “court”; and “sexual violence” + “Africa” + “memory”. Due to the hypothesized paucity of literature related specifically to East Africa, keywords were kept quite general, and articles were tagged geographically during first screening. Targeted searches of gray literature databases included Save the Children’s Resource Centre and UN Women’s Virtual Centre to End Violence Against Women and Girls. In addition, systematic reviews on similar topics were searched for relevant interventions.
Following the UN geoscheme designation, we expanded “East Africa” when possible in the database search to include “Burundi,” “Comoros,” “Djibouti,” “Democratic Republic of Congo (DRC),” “Eritrea,” “Ethiopia,” “Kenya,” “Madagascar,” “Malawi,” “Mauritius,” “Mayotte,” “Mozambique,” “Reunion,” “Rwanda,” “Seychelles,” “Somalia,” “South Sudan,” “Tanzania,” “Uganda,” “Zambia,” and “Zimbabwe.” The geoscheme lists all the above countries, except the DRC, as being in the East African region (Mendelson et al., 2014). As the DRC is a member of the East African Community and is often included in broader conceptualizations and policy work in the region, it has also been included in our analysis (EAC Partner States, 2022).
Studies were screened by two reviewers, with a first screening based on article title, abstract, and keywords, and a second screening of relevant studies based on assessing the full article against the inclusion/exclusion criteria. These criteria were: published between 2005 and 2019; type of initiative (specifically focused on SV as opposed to generally improving criminal justice); working with health professionals, the police, criminal justice prosecutors, the judiciary, governance, policy or regulatory bodies; conducted by NGOs, donors or national/local/municipal governments; type of study (academic, peer-reviewed involving either qualitative or quantitative methods, program reviews, and impact evaluations from practitioners); and language (either English or French due to the language constraints of the authors).
Studies that passed second screening were analyzed against the following questions: Who did the initiative work with? What activities did the initiative undertake? What was the target population? What were the outcomes/impact of the initiative? What are some of the barriers or challenges to initiatives to strengthen criminal investigation and prosecution of SV? The quality of the studies was also evaluated (when applicable) using the Joanna Briggs Institute’s critical appraisal tools (JBI, 2020). Based on these questions, the main categories identified were type of initiative, outcomes/impact, and barriers or challenges. Drawing on these categories, the authors classified initiatives into groups, which are discussed below.
Results
A total of 24 individual studies that examined 33 separate interventions are included in this review. Of these, 14 are academic studies derived from academic database searches, and 10 are practitioner or gray literature studies identified during targeted gray literature searches. An overview of the selection process can be found in Figure 1. In terms of geographic spread, most studies (n = 9) solely focused either on Kenya or included interventions in Kenya in addition to other relevant countries. Countries included in the studies were Zambia (n = 7), Rwanda (n = 3), Malawi (n = 3), Uganda (n = 1), Sudan (n = 1), and Zimbabwe (n = 1). This finding is similar to that of other reviews conducted in East Africa, which also found that the most studied country in the region regarding SV is Kenya (S. Rockowitz et al., 2021).
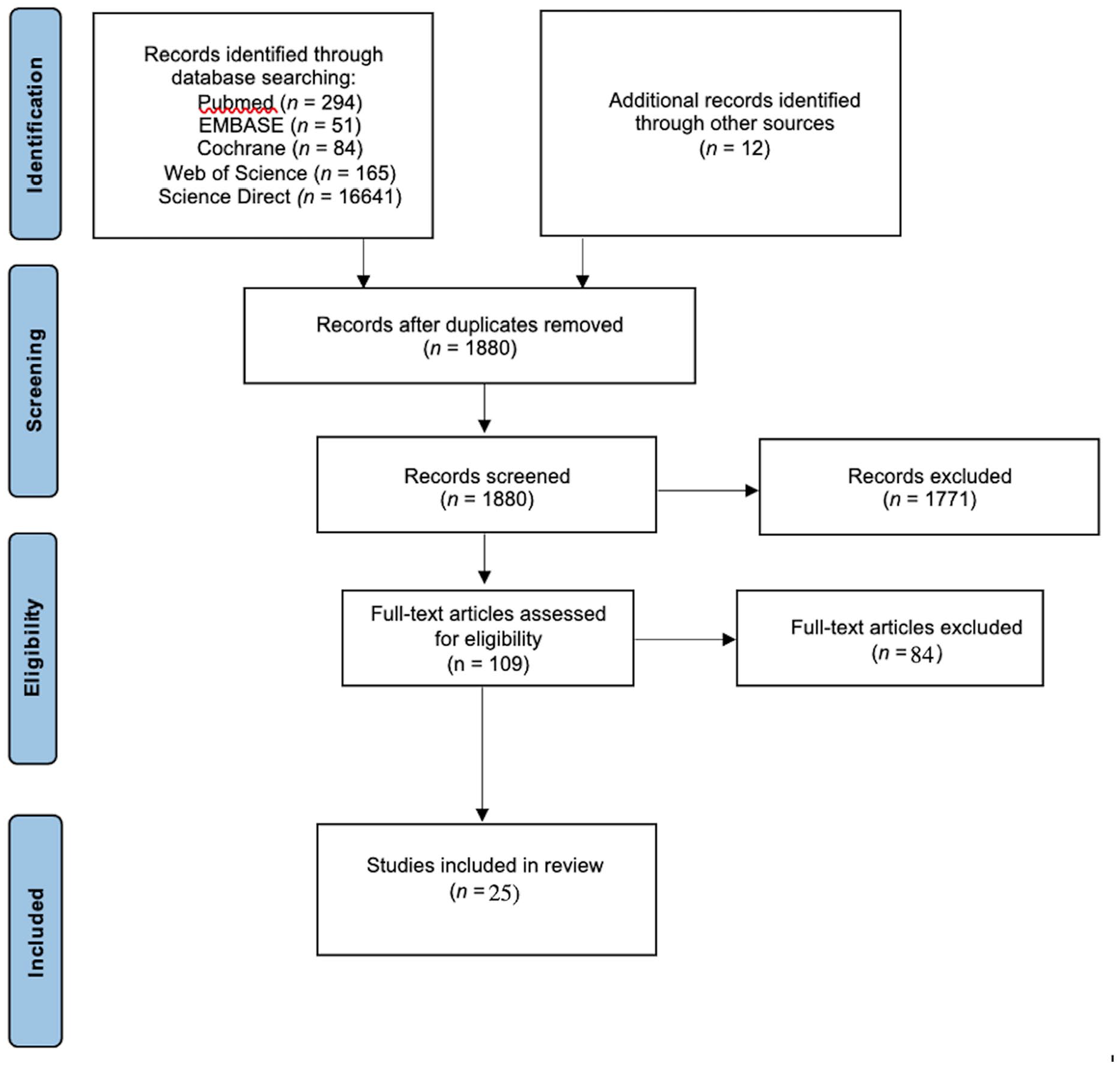
PRISMA diagram of study selection process.
Whilst searches were conducted from 2005 onwards, the earliest study included is from 2009. Nearly half of the studies (n = 12) were published between 2017 and 2019. One reason for this is that many of the studies are related to the same or different phases of the same intervention. For example, there are three studies related to MediCapt, a mobile app designed to support forensic-medical evidence collection and chain of custody that were published between 2017 and 2019 (Anastario, 2019; Mishori et al., 2017; Naimer et al., 2017). Further, three studies were related to the same or different phases of an intervention to improve the collection and documentation of post-rape evidence in Kenya spread across the time period (Ajema et al., 2015; Population Council, 2018).
Across the 24 studies, case studies were the most common research approach (n = 9), followed by mixed methods research (n = 5), feasibility assessments (n = 2), descriptive studies (n = 2), evidence reviews (n = 2), clinical records reviews (n = 1), operations research (n = 1), qualitative interviews (n = 1), and finding assessments (n = 1). Sample sizes varied depending on the approach. For example, Buard et al. reviewed 866 patient records, while Musiwa surveyed 25 professionals and conducted 15 key informant interviews (Buard et al., 2013; Musiwa, 2018). A subset of all studies (n = 7) was concerned with developing or testing project models that could be scaled up.
The interventions were specifically designed to strengthen the criminal investigation and prosecution of cases and those where criminal justice links are part of the overall intervention package (e.g., police training designed to strengthen referral networks). Examples include MediCapt, multisectoral interventions in Kenya to strengthen the documentation of medico-legal evidence, and the establishment of specialized police units and courts. The interventions were primarily assessed during peacetime and in non-humanitarian contexts, while two included conflict-related SV, and four focused on humanitarian contexts. Of the studies that provided participant information, 10 interventions focused on all survivors (women, men, and children), whilst eight focused on women and girls, five on children, and one on girls. The remaining studies referred simply to survivors, or did not provide specific information.
Initiatives
We identified six types of interventions for SV in peacetime and non-humanitarian contexts (see Table 1). The one-stop centre (OSC) model (n = 9), which brings together a range of services for survivors, was the dominant intervention type. Other intervention types (in order of frequency) include: multisectoral network strengthening (n = 6), specialized police units (n = 3), gender desks and police training (n = 2), community interventions (n = 2), and finally mobile applications (n = 2). Based on their foci and target audience, these types of interventions were combined into three broader categories: (a) legal sector interventions; (b) collaborative interventions; and (c) technological interventions. In a final section, we review (d) initiatives that have been developed for conflict situations and humanitarian contexts, because East Africa, as a region, has a history of civil conflict leading to large populations of refugees and internally displaced persons for whom interventions differ by necessity of resource limitations and involvement of international non-governmental organizations.
Number and Type of Intervention by Country of Study.
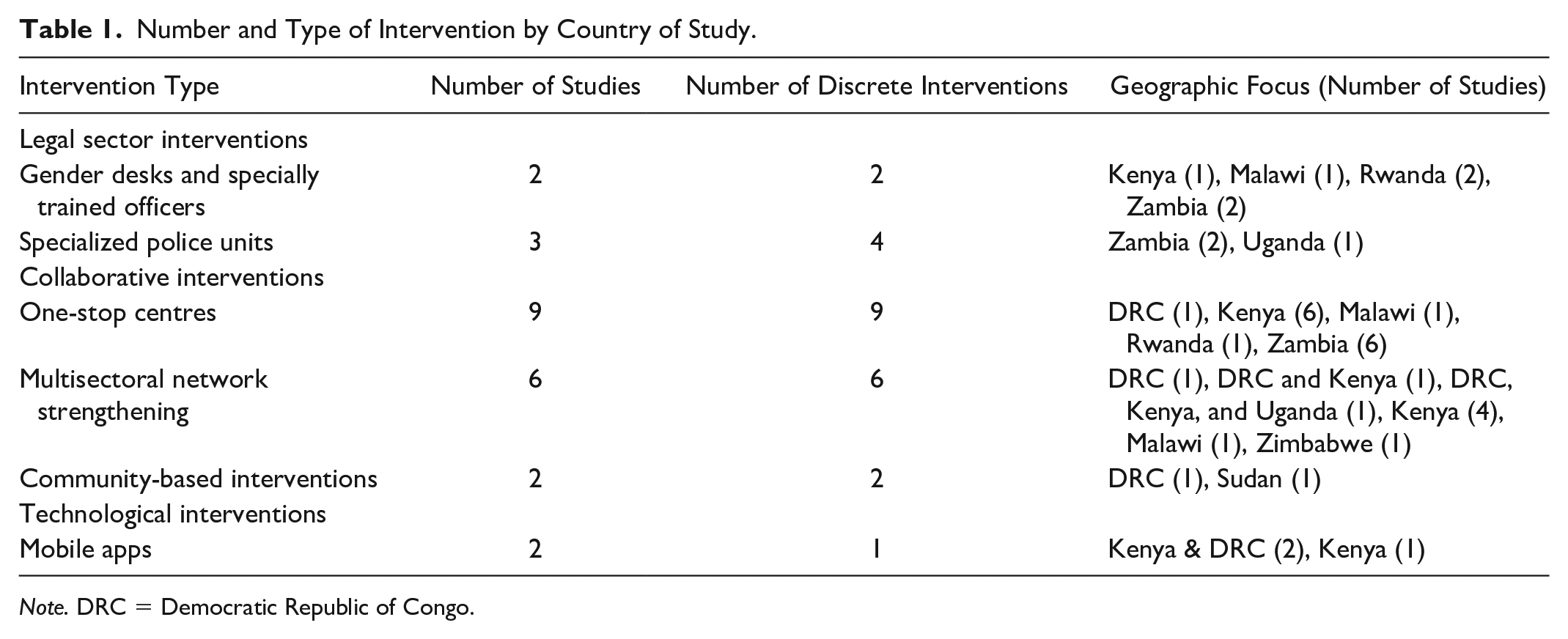
Note. DRC = Democratic Republic of Congo.
Legal Sector Interventions
Interventions in this category are those that target the legal sector, primarily through work conducted with police officials or at police stations.
Gender Desks
Gender desks aim to enhance police responses to SV by increasing logistics and police capacity to investigate cases and counsel survivors, assist survivors in accessing health, legal, and psychosocial support, develop strategies and guidelines for dealing with incidents, and raise public awareness of related risks and the role of the police (United Nations Development Fund for Women (UNIFEM)). For instance, officers of the Rwanda National Police who were specially trained on SV cases have been placed in each of the country’s 69 police stations to ensure survivors have decentralized access to specialized support (Moser, 2009). Funded by UNIFEM and other donors, some of these officers have been provided with equipment including desks, computers, and vehicles. Related activities include training police station commanders on standard operating procedures for SGBV and the development of SGBV curricula and training manuals for the two police training schools (Moser, 2009). Between 2005 and 2009, key activities supported by UNIFEM focused on training and capacity development including Standard Operating Procedures for responding to SGBV, investigating cases, psycho-social counseling, establishing coordination structures with stakeholders from other key sectors including legal service providers, and community sensitization (UNIFEM).
It is unclear, however, whether these initiatives increase rates of reporting, the number of cases brought to court, or the number of prosecutions, although an assistant inspector at one of the police stations with a gender desk in Rwanda did feel that the presence of SGBV officers helped survivors feel more willing to come forward (Moser, 2009). Between 2006 to 2007, the number of reported cases in Kigali increased but then decreased in 2008 (Moser, 2009). UNIFEM argued that potential reasons for the low reporting of cases was a lack of community trust in the police, the persistent backlog of rape cases in the prosecutor’s office, challenges in infrastructure, normative perceptions of SV, and misinformation about procedures that may have discouraged survivors from reporting and prevented cases from being processed in court (Moser, 2009). The authors concluded that activities such as the establishment of community policing committees may help to ensure that information on SV is exchanged between communities and the police. However, better data management and monitoring systems, including better documentation and data systems for case management, were recommended (Moser, 2009).
The Rwanda Defence Force has established a gender desk that works with the country’s leading mobile company to provide a free hotline to report SV cases that potentially implicate the military (UNIFEM). Reports of SV to the Rwanda Defence Force have increased since the gender desk was established in 2008. Possible reasons for the success of this initiative may be the local military deployment and 24-hour patrol due to which the military is well placed to locate and respond to issues, as well as that military staff are sometimes present when the police are not (Moser, 2009).
Specialized Police Units
The model of specialized police units adopted varies by country and there are different types with different mandates and relations to the larger police force (Seelinger, 2014). An intervention in Zambia that was conducted with two police stations and one hospital in Lusaka Province sensitized the police and health providers to the national guidelines of responding to child sexual abuse and introduced transportation services for child survivors from police stations to and from the hospital for post-rape care services (Population Council, 2018). To ensure child survivors have access to comprehensive care and justice, victim support unit officers are trained to take child samples to the lab and take statements from attending health professionals, yet these requirements have often been inconsistently implemented due to lack of awareness and training (Chelwa et al., 2017; Population Council, 2018).
Evaluation of the intervention found that specialized police units facilitated access to post-rape care in Zambia; 90% of caregivers of child survivors who presented at the police station were willing to accept police transportation and accompaniment to the health facility site which simplified access to services for child survivors and caregivers (Population Council, 2018). Of those accompanied to the health facility by police, 95% received same-day SGBV care. However, for the overall intervention package to be effective, the study concluded that post-rape care in health facilities needed to be strengthened, understaffing addressed, and that it should be ensured that administrative costs, such as for photocopying, were not borne by survivors (Chelwa et al., 2017).
Across Uganda, specialized units have increased reporting of rape; however, their existence has not necessarily led to increased convictions due to barriers in the legal system (Bacon, 2015). Shortcomings of the legal process resulted in a backlog of 100 cases for similar reasons as discussed in previous interventions, such as coordination problems, resource constraints, and insufficient evidence to support a case in court. Common challenges across countries include undefined relationships between specialized units and the wider police force and limited mobility such as limited access to transportation needed to collect crime scene evidence (Seelinger, 2014). Victim support unit officers further often lack basic equipment and resources to conduct investigations (e.g., vehicles and communication equipment or the ability to analyze and use forensic evidence; Morel-Seytoux et al., 2010).
In addition to specialized police units, some countries in East Africa also have proposed “specialized prosecution units” (Seelinger, 2014). Although these are similar to police units, they differ in that they are more wide-reaching and include prosecutors, support staff, and welfare staff, and are therefore seen as a more intensive approach (Seelinger, 2014). In Uganda, the Sexual Offences Section in Kampala (established by the Directorate of Public Prosecutions), and in Kenya the Office of the Director of Public Prosecutions’ SGBV unit were established to assist with SV cases (Seelinger, 2014) by acting as point persons that can advise police prosecutors at the magistrate and appellate levels (Seelinger, 2014). However, at the time the research was conducted, these units were not yet operationalized; thus, evidence on their effectiveness is lacking.
Collaborative Multi-sectoral Interventions
The next group of interventions involves collaboration between multiple sectors, either through the establishment of multisectoral service provision establishments, referral strengthening mechanisms, or the inclusion of communities.
One-Stop Centers
OSCs were the most common intervention type studied across the papers reviewed, with examples from the DRC, Malawi, Rwanda, Kenya, and Zambia (Bernath & Gahongayire, 2013; Buard et al., 2013; CARE, 2013; Keesbury et al., 2012; Morel-Seytoux et al., 2010; Mukwege & Berg, 2016; Mulambia et al., 2018; Ranney et al., 2011; Temmerman et al., 2019). OSCs are typically located in or attached to a hospital or a government referral facility and provide medical, legal, and psychosocial services for SV survivors. For example, the SGBV Recovery Centre at the Coast Provincial General Hospital in Mombasa, Kenya, provides emergency health care, free mental health support, paralegal services, and integrated cooperation with the police, judiciary, local leaders, and the wider community (Temmerman et al., 2019). Similarly, Panzi Hospital and Foundation in DRC supports social reintegration through programs addressing social exclusion and financial wellbeing (Amisi et al., 2018).
OSCs have several features that may increase the number of survivors seeking post-SV care and the number of cases that progress through the criminal justice and legal systems compared to other, less collaborative approaches to service provision. First, medical and forensic capacity at OSCs can often exceed what is available elsewhere (Bernath & Gahongayire, 2013) and may include specialized medical kits for the proper collection, documentation, and preservation of evidence, or outreach activities with communities (CARE, 2013). Second, having a center nested in a facility that is used to provide resources other than just for SV, such as a general health center, has the potential to reduce stigma, including for males, who may find it particularly difficult to seek treatment (Temmerman et al., 2019). Third, coordinated paperwork between medical and legal service providers (i.e., the use of standardized post-rape care forms) can support cases progressing through the criminal justice system (Temmerman et al., 2019).
There are a mix of funding modalities for OSCs including donor support, NGOs, and government ministries. Keesbury et al. (2012) compared services provided by NGO-owned OSCs, NGOs partnered with health facility-owned OSCs, and health facility-owned OSCs. They found that facilities attached to and run in connection with a hospital provided better health services to survivors. This shows that funding and operations management of OSCs impact service provision.
At Rwanda’s Isange OSC in Kigali, every survivor is seen by a judicial police officer who has close links with the police gender desk and immediately starts an investigation (Bernath & Gahongayire, 2013). Nonetheless, there is limited evidence that OSCs increase the number of cases reported to the police or improve the rate of legal resolution. For example, in the case of the Isange OSCs in Rwanda, whilst the number of cases were recorded, no data were collected on the number of forensic interviews conducted, the number of medical reports supplied to prosecutors, or the number of successful prosecutions (Bernath & Gahongayire, 2013). Consequently, it is not possible to determine whether the OSC met its stated objective of “a greater percentage of admissible forensic interviews thus leading to increased percentage of convictions” (Bernath & Gahongayire, 2013).
The SGBV Recovery Centre in Kenya has a users’ committee comprised of health staff, police, and the public prosecutor’s department who meet every 3 months to review cases presented to court and discuss challenges with specimen collection, police preparation of cases, and prosecution to improve outcomes (Temmerman et al., 2019). Between 2015 and 2018, 2,719 survivors who received care at the recovery center in Kenya were referred for legal services, but only 13% of cases progressed to court (Temmerman et al., 2019). The authors suggest that reasons for the low number progressing to court include survivors and families choosing to resolve the case out of court or there being inadequate evidence for prosecuting the case, as the survivors may have changed clothes, had a bath, or reported several days after the incident. In contrast, Mulambia et al. (2018) found that of 107 families of a child who had received services at the Blantyre OSC in Malawi, 95% had an initial police report taken and 27% of cases ended in a criminal conviction for child sexual abuse. However, 25% of families surveyed were not satisfied with the law enforcement response (Mulambia et al., 2018).
These examples illustrate several barriers and challenges to effectiveness in terms of OSCs strengthening the criminal investigation and prosecution of SV cases. There are barriers to implementation (e.g., staff time constraints and lack of basic medical supplies resulting in long wait times) and barriers to achieving multi-sectoral coordination, such as corruption and mistreatment of survivors by the police (Mulambia et al., 2018; Temmerman et al., 2019). In Kenya and Zambia, the research suggests weak linkages between OSCs and the legal system, as well as challenges faced by victims in reporting cases to police stations, and in accessing legal services and representation in court (Keesbury et al., 2012). Given the intent of the OSC to facilitate easier reporting between victims and the legal system, the fact that survivors accessing OSCs are having similar problems as those who seek care independently raise concerns about the effectiveness of the OSC model. CARE argues that a lack of permanently assigned police and other government officers negatively impacted case follow-up, and similar concerns have been raised about paralegal services provided by volunteers (CARE, 2013). Efforts to tackle these challenges have thus far included SV training for the police and the establishment of gender desks in police stations (Keesbury et al., 2012). Other enablers to effectiveness were identified as supportive laws and policies, as well as regular interagency meetings to coordinate services and support, address challenges, and to delegate tasks (Olson et al., 2020).
Multisectoral Network Strengthening
The multisectoral interventions identified by this systematic review vary in terms of approach, but commonly work with health, law enforcement, and legal professionals and agencies to increase the number of cases being reported, and/or those progressing through the criminal justice system. While some initiatives attempt to address SV from various angles, such as the Victim Friendly Court system in Zimbabwe which aims to provide preventive/protective treatment and support services for victims of child sexual abuse, others take a more targeted approach, for instance via the use of a locally assembled rape kit in Kenya to facilitate the collection, documentation, and utilization of medico-legal evidence (Ajema et al., 2015; Musiwa, 2018; Population Council, 2014). Both initiatives were found to improve access to services for victims, indicating that there is not a one-size-fits-all approach to improving survivors’ access to justice.
Multisectoral interventions have also been implemented to improve referral patterns between the police and service providers. In many countries in East Africa, survivors must report their case to the police to receive medical services. Bernath and Gahongayire (2013) argue that forcing survivors to interact with the police violates the principles of “victim’s choice” and could deter some survivors from seeking post-SGBV care. At the SGBV Recovery Centre in Kenya, for example, 75% of survivors who received care between 2013 and 2018 were referred to the center by a police station (Temmerman et al., 2019). Survivors who self-referred to the hospital and who have received medical and psychological care are subsequently referred to the nearest police station (Temmerman et al., 2019). From the literature we reviewed, it is evident that police are often the first point of contact for survivors seeking care, even though the medical consequences of their assault may often be more time-sensitive and pressing than their need to engage with the police. In mandating police engagement before service access, medico-legal systems are forcing survivors to prioritize legal questions over their physical and mental wellbeing.
Strong communication channels between the police and health facilities are needed, particularly in situations where their roles intersect. A key aspect of case progression in the criminal justice system is the quality of forensic evidence available, which can vary wildly depending on factors such as provider knowledge of evidence collection, protocols for conducting rape examinations, and a lack of comprehensive guidelines indicating the roles of different actors in handling forensic evidence (Ajema et al., 2011; Wangamati et al., 2016). Additionally, a lack of clarity about who can sign a medical exam form and testify in court serves as a bureaucratic roadblock even once a survivor has presented for evidence collection and samples have been gathered (Morel-Seytoux et al., 2010). This uncertainty surrounding seemingly straightforward procedures, such as who signs which forms and who transfers the evidence from one institution to another, seriously hampers case progression for SV survivors.
Multisectoral training was a key part of interventions in Zambia and Malawi covering both the health and criminal aspects of police response (Keesbury & Askew, 2010). According to post-intervention evaluation data, the initiatives—intended to strengthen linkages between police stations and health facilities—resulted in over 90% of survivors being referred to health facilities by the police (Keesbury & Askew, 2010). In Zambia, an intervention that trained the police to deliver emergency contraception to eligible survivors and to refer survivors to health facilities for further clinical management and forensic evidence collection increased victim reporting rates by 48% in participating police stations from 2006 to 2007 (Keesbury & Askew, 2010). Enablers of this intervention are thought to be the presence of a high-ranking police officer in the training in Zambia, which demonstrates police commitment, and the presence of experienced health professionals (Keesbury & Askew, 2010).
Community Interventions
Community-based approaches to interventions can tackle some of the root causes for a lack of justice for SV survivors. Often someone would be willing to speak to professionals if they only knew where to start. Creating opportunities for improved awareness of SV management is a key priority for community education around SV, including knowledge of the steps that survivors should take following an incident to increase the chance of a successful prosecution (e.g., not taking a bath to preserve forensic evidence; Temmerman et al., 2019). Examples of such interventions are The Women’s Rights in Darfur Training of Trainers Programme in Sudan, a 3-year program which prepared lawyers and paralegals to deliver community outreach projects to build local capacity to prevent and respond to SV, sensitize communities, and empower internally displaced women and girls to claim their rights (Bennett & de Lacey, 2018) as well as the USAID-funded Ushindi project in eastern DRC, which ran from 2010 to 2018 and delivered a package of services to survivors of community-level SV partly through faith-based community resources and leveraging local networks (Bennett et al., 2017).
In terms of effectiveness, Bennett et al. (2017) measured the number of people treated and supported through the different services offered as part of the intervention in the DRC. Legal counseling was provided by lawyers in legal clinics established in safe houses; however, no outcome data were available at the time the review was conducted. Nevertheless, Bennett et al. argue that the reach of the project shows that community leaders have significant potential to fill a critical gap in service provisions for survivors in unstable settings, and that, with adequate training, supervision, support, and incentives, informal providers can effectively extend the reach of the health system to marginalized and highly stigmatized people (Bennett et al., 2017). Flexible implementation and intervention approaches, such as working with faith-based organizations and other community actors, are needed to meet the varied needs of survivors and ensure the sustainability of service delivery (Bennett et al., 2017). Similarly, research in Darfur working with lawyers and paralegals to expand their knowledge about human rights law and women’s rights found that interventions must be tailored toward the implementation context, making large-scale roll-out of programs challenging (Bennett & de Lacey, 2018).
Technological Interventions
Technological interventions are the most recent category of interventions and summarize efforts designed to improve medico-legal initiatives to SV responses via the use of technology.
Mobile Applications
With the increase of mobile phone and broadband access in low- and middle-income countries, mobile applications that intend to standardize the documentation of SV evidence for forensic purposes and preserve it for use in legal proceedings have started to emerge (Mishori et al., 2017; Stevens et al., 2022). Two of the studies in this review related to the MediCapt mobile phone application which is a digital platform developed by Physicians for Human Rights to facilitate the comprehensive collection of evidence by clinicians, accessed via a mobile application for clinicians and a web-based app for law enforcement and the judicial system (Naimer et al., 2017). MediCapt combines a standardized medical intake form for forensic documentation and a secure mobile camera, allowing data to be securely transmitted to the police and courts (Mishori et al., 2017). Physicians for Human Rights researchers can also use the web app to look at de-identified, aggregated data for early detection of mass crimes to trigger a rapid response. The standardized form considers limited resources and varying technical skills and has a writable pictogram feature so clinicians can add marks to show where an injury is located (Naimer et al., 2017).
Following the development phase, 4 the app was piloted in Kenya with patients in late 2018 with plans to scale-up to new facilities in the DRC and Kenya in 2020 (Anastario, 2019). It is not clear how these plans have been impacted by COVID-19. During the field-testing phases several perceived and actual barriers to implementation were identified, including both personal (individual levels of comfort with technology) and systemic such as cultural preferences for paper forms and limited internet connectivity (Mishori et al., 2017). Key findings from the program’s evaluation include improved internal coordination due to the use of a formal chain of custody document, standardized medical documentation, as well as more successful prosecutions and convictions due to law enforcement training. It is particularly notable that perceptions of and quantitative evidence of adjudication outcomes favoring the survivor increased in the period immediately following the intervention, and that the relative amount of medical evidence in the Post-Rape Care form appearing in the legal record (a key focus of Physicians for Human Right’s programming) was associated with an increased likelihood of an adjudication outcome favoring the survivor (Anastario, 2019).
Refugee Contexts
Medico-legal responses to survivors of SV in refugee populations are complex. Whilst this paper is not specifically focused on refugee populations, a small number of interventions that aim to improve responses to SV in refugee contexts and contexts of displacement were identified. However, peer-reviewed studies or evaluations of interventions were rare, and evidence of impact was limited. This supports Block et al. and Spangaro et al.’s findings that there is a paucity of evidence for the effectiveness of responses to SV experienced by refugees and that there is a limited number of studies examining their impact (Block et al., 2019; Spangaro et al., 2013). Additionally, interventions in these contexts often did not match the categories used earlier in this paper, which is why they are being described separately.
Initiatives that have been tried as part of UNHCR operations include mobile courts (although failure to appear by survivors and withdrawal of cases are key challenges), efforts to improve linkages between traditional and formal courts in Kenya, and support for SV committees in Burundi and Djibouti, which refer cases to court (Mirghani et al., 2017). Oxfam’s Protection Programme in eastern DRC included establishing Protection Committees to improve referrals to legal services within 72 hrs, among other aims (Holmes & Bhuvanendra, 2014). Other examples of initiatives to improve medico-legal responses in refugee contexts in East Africa are the Population Council’s 2018 to 2020 VOICE project which harnesses the Africa Regional SGBV Network (comprised of service providers) to provide technical support to UNHCR and NGOs in implementing a range of evidence-based models addressing SV in refugee programs in eight countries (Djibouti, Ethiopia, Rwanda, South Sudan, Sudan, Tanzania, Uganda, and Zambia). However, no evidence of impact was found for these initiatives. Instead, several challenges in legal responses to SV in humanitarian situations and refugee populations were identified, including remotely located refugee camps with limited access to resources, socio-cultural norms around gender inequality and SV, a lack of data to inform appropriate program responses, capacity and resource constraints and lack of coordination, lengthy legal procedures, and plural legal systems that might result in the non-application of international human rights standards at the expense of survivors (Holmes & Bhuvanendra, 2014; Mirghani et al., 2017).
Multisectoral interventions to support refugee populations can include components related to criminal justice. For example, the CARE International Refugee Assistance Project in Dadaab, Kenya, included legal and litigation support as well as education and behavioral change components, amongst others (Holmes & Bhuvanendra, 2014). This program has helped to strengthen SV reporting structures and 8 out of 10 reported incidents are brought to the attention of the police. This suggests that awareness campaigns on the importance of accessing legal protection and clinical services have been effective, although traditional approaches and stigma can still inhibit the reporting of incidents and the number of perpetrators arrested was very low (Holmes & Bhuvanendra, 2014).
Discussion
Our review examined the body of research produced on medico-legal initiatives in East Africa between 2005 and 2019, assessing the types of initiatives that have been researched, their geographic and substantive focus, and methods used. The review incorporated a synopsis of 25 eligible studies that examined seven types of interventions. Overall, the volume of research was low and restricted to certain regions, with many countries in East Africa (Burundi, Comoros, Djibouti, Ethiopia, Eritrea, Madagascar, Mauritius, Mayotte, Mozambique, Réunion, Seychelles, Somalia, and Tanzania) being the subject of no papers at all. Information on the effectiveness of medico-legal initiatives as they pertain to survivors’ access to justice and service provisions is scarce. We found that this may be the case for several reasons, including social stigma and a lack of funding for initiative development and implementation. The review shows a peak in studies on interventions between 2017 and 2019 which might reflect the increasing focus and push for progress toward Millennium Development Goal 5 at international and regional fora.
Throughout the iterative process of finding papers for this review, it became clear that there are few studies that used formal evaluation methods. Thus, the majority of papers included did not have pre- and post-intervention data. As a result, the majority of studies describe how interventions are being used and what the demographics and journeys are of those who interact with the intervention. The findings reflect that survivors’ interactions with the criminal justice system have not yet been comprehensively assessed and that service provisions require more in-depth theorizing, conceptualizing, and monitoring.
The review shows that intervention types are heterogeneous and differ depending on their target audience and the resource availability in the respective region. This has implications for the kinds of conclusions that can be drawn from this review, particularly with regards to a cross-regional comparison of the benefits and challenges of interventions, as well as their potential to be scaled up. Based on the studies included in this review, three broad types of initiatives have been investigated: initiatives that target reforms of the legal sector such as the implementation of specialized units for supporting, investigating, and/or prosecuting SV cases, initiatives that aim to improve referral and support networks via multisectoral collaboration and community interventions, as well as technological interventions that are designed to support health professionals and legal proceedings by collecting forensic documentation.
While the aims of these types of initiatives have partially been met, the review identified shortcomings across them that limit their effectiveness and prevent survivors from accessing the health and justice system via the case referral pathway. Barriers to initiatives succeeding to improve medico-legal responses to SV in East Africa include: (a) a lack of resources and facilities to sustain the initiative; (b) a lack of trained health care, police, and judicial personnel to carry out services; (c) stigma, discrimination, and corruption limiting the uptake and fair distribution of services; (d) weak medico-legal partnerships restricting pathways of accessing services; and (e) weak synthesis of initiatives for SV during peace time and conflict.
The first stumbling block for many of the initiatives was a lack of resources to sustain the initiative, such as a lack of human resources and equipment. According to our review, insufficient facilities for specimen testing, proper examination, and legal documentation of offenses are common in the region. This hinders both medical and police investigations, and thus presents a significant barrier to criminal justice and effective prosecutions. Additionally, there was a clear rural–urban divide in accessing treatment opportunities. The interventions were largely located in and served urban areas. Evidently, it can be difficult for rural residents to reach services, especially in areas with poor transportation and limited financial resources (Njuki et al., 2012). This means that the strength of a country’s infrastructure has lasting effects on survivors’ wellbeing and recovery. Even for survivors who live in the city where services are provided, or in refugee camps with services on-site, transportation issues, fear of reprisal, clan differences, and childcare commitments may prohibit timely access, which in turn impedes the collection of evidence for investigations and prosecutions (Kimani et al., 2020; Muuo et al., 2020).
Second, staff across the different sectors often lack adequate competencies with respect to documenting evidence and implementing medical or criminal justice interventions; yet attempts to provide guidance and formulate additional protocols are rare, with no acknowledgment of why these protocols do not exist in the first place, such as insufficient training, time, or resource constraints (Seelinger, 2014; Wangamati et al., 2016). A lack of training in assessing and documenting reported incidents can result in delays in delivering post-rape services (Population Council, 2014; Stevens et al., 2022). Insufficient training also impedes opportunities for collecting forensic evidence, resulting in missing or incorrect collection and handling of evidence (Ajema et al., 2011; Wangamati et al., 2016). Consequences of this also include increasing the risk of re-traumatizing survivors.
Third, social norms and the stigma around SV contribute to low reporting rates, as well as how cases are treated by police practitioners. Service providers may hold negative attitudes toward survivors (Wangamati et al., 2016) and this affects the efficacy of interventions. Customary systems, such as those in East Africa, can be sexist and may produce unfavorable outcomes for women and girls (Cone, 2019). A perception of corruption or negligence by police can discourage the use of other types of services (Mulambia et al., 2018). Our review further shows that lack of trust in authorities, misinformation about legal proceedings, and past failures of prosecuting perpetrators may discourage survivors from reporting and prevent cases being adjudicated. Interventions appear to have more reach if they are collaborative or community-based, for instance, by engaging religious leaders and community elders.
Fourth, policy frameworks and implementation systems and structures do not clearly articulate links between the medical and legal sector and functioning medico-legal partnerships have not been established consistently throughout the region. Weak linkages between the medico-legal sectors can hamper interventions designed to facilitate the prosecution of SV cases and violate the rights of survivors a second time (UN Women, 2021); hence, the strengthening of multisectoral collaborations to improve efficiency in the delivery of justice is key to successful interventions (Njuki et al., 2012). The sustainability of interventions is also important, particularly in the case of donor-funded, international-NGO implemented projects, which need to be integrated into national SV responses (Morel-Seytoux et al., 2010).
Fifth, types of SV, justice systems, and the impact they have upon convictions appear to be understudied according to our review. Research commonly focuses on conflict-based SV separately from SV that occurs in peacetime (Mishori et al., 2017; The Global Women’s Institute & International Rescue Committee, 2016). Conflict-based SV is a critical issue; however, there needs to be a heightened connectedness between interventions aimed at peacetime SV and conflict-based SV. Whilst there are added complexities to conflict-based crimes, such as the possibility of authority figures perpetrating the crimes (Human Rights Watch, 2017), there are overlaps regarding barriers that prevent survivors from accessing justice both in times of peace as well as in times of conflict.
Strengths and Limitations
Research about barriers to justice and service provisions in East Africa is growing, yet limited and little work has been undertaken that evaluates the efficacy of interventions. In describing and comparing interventions implemented in East Africa, the review contributes to a better understanding of survivors’ interactions with the justice system and barriers that should be removed to allow survivors to access comprehensive care and support. The review highlights that there is a lack of evidence and that there are particularly thin evidence bases related to lower-income areas and survivors in conflict settings and humanitarian contexts.
Given the scale of the problem of SV and the challenges in adjudicating cases in low-resource settings, this review has identified a relatively small number of studies and interventions. It may have failed to capture some relevant articles due to the authors’ choice of databases and journals, as well as the search remaining limited to publications written in English and French. Moreover, few studies with East African authors, as well as international collaborations where East African researchers are first authors, were found, which illustrates persisting power imbalances in knowledge production and the distribution of research funds. Due to the selected studies being country-specific, with many derived from Kenya, the results cannot be generalized to SV survivors in other regions without a proper evidence base to support doing so. The review covers interventions in cases with female as well as male survivors from all age groups. The lack of a gender-expansive population in this paper is not due to inclusion criteria but rather a lack of literature about those who identify as other than strictly male and female.
Due to the varying research methods employed and information published across studies, the quality of the papers could not be assessed consistently, and the effectiveness and ubiquity of some of the interventions could not be determined. We have therefore chosen a narrative approach to reporting our findings which may in part limit the systematicity of our review yet allowed for the inclusion of a larger number of studies and enabled a multidisciplinary team to participate in the review process.
Opportunities
Findings from the review highlight that rights realization for survivors requires strengthening enabling environments, including strengthening the coordination of efforts across the law enforcement and court sectors, as well as policy and legal frameworks for investigations and prosecutions alongside public health programming. Alignment between national and local frameworks is also important. For example, given the role forensic evidence plays in judicial proceedings, it is important that local protocols for collecting evidence align with national protocols (Wangamati et al., 2016). Several interventions in this study referred to the importance of having laws, policies, national guidelines, and standard operating procedures in place.
Knowledge of the effectiveness of interventions is limited and unevenly distributed yet learning about the gaps in existing programs is crucial for service development and research planning phases. More research is needed to identify effective interventions during peacetime, as this could contribute toward creating a sustainable infrastructure that can assist in responding and protecting survivors in times of conflict.
There is a gap between research on SGBV and technology that needs to be reduced in order to explore how tech-based interventions and digital innovation can provide new ways of supporting survivors. Research on technological tools for gathering testimony (Stevens et al., 2022) and evidence, such as MediCapt, is in its infancy, and research and development of initiatives that prevent and respond to technology-facilitated SV is lacking. To harness the positives of technology and engage meaningfully with a range of non-traditional stakeholders such as the business and technology sector, developing international standards and codes of conduct that ensure the safety and survivor-centeredness of solutions is crucial (Murad Code Project, 2022; UNFPA, 2022). Thus, there is considerable opportunity for research on technology use and misuse, and how to share knowledge and coordinate efforts across the medico-legal pathway. Given the ever-increasing role of technology in GBV interventions, including data collection and response activities (Institute for International Criminal Investigations, 2021; Stevens et al., 2022), there is a pressing need to comprehend how widespread access to technology in low- and middle-income countries can help combat SV in East Africa. Apps, like MediCapt, that can transform the documentation and prosecution of SV by connecting police, medical, and legal professionals while ensuring an ethical and contextually appropriate design demonstrate the major role technology can play in systematically addressing the gaps in medico-legal processes in the region.
To enhance efforts of preventing and prosecuting cases of SV, interventions need to be co-developed and assessed by survivors. Since women and children are disproportionately impacted by SV (WHO, 2022) it is positive that we found instances where research is being conducted on interventions that aim to aid women and children’s access to justice. However, it is also important to ensure that other groups, such as men, are not excluded.
Conclusion
Given the known lasting psychosocial and physical effects of SV on survivors, there is a clear need for further research on how to strengthen the criminal justice system and incorporate criminal justice interventions into existing referral pathways to ensure a smooth justice-seeking process for survivors. Researchers should also account for the disproportionate focus on some countries over others, being sure to allocate resources to under-resourced and under-researched locations that may need significant criminal justice system strengthening.
Supplemental Material
sj-docx-1-tva-10.1177_15248380231165694 – Supplemental material for A Systematic Review of Criminal Justice Initiatives to Strengthen the Criminal Investigation and Prosecution of Sexual Violence in East Africa
Supplemental material, sj-docx-1-tva-10.1177_15248380231165694 for A Systematic Review of Criminal Justice Initiatives to Strengthen the Criminal Investigation and Prosecution of Sexual Violence in East Africa by Sarah Rockowitz, Kirstin Wagner, Rachel Cooper, Laura Stevens, Kari Davies, Jessica Woodhams, Wangu Kanja and Heather D. Flowe in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380231165694 – Supplemental material for A Systematic Review of Criminal Justice Initiatives to Strengthen the Criminal Investigation and Prosecution of Sexual Violence in East Africa
Supplemental material, sj-docx-2-tva-10.1177_15248380231165694 for A Systematic Review of Criminal Justice Initiatives to Strengthen the Criminal Investigation and Prosecution of Sexual Violence in East Africa by Sarah Rockowitz, Kirstin Wagner, Rachel Cooper, Laura Stevens, Kari Davies, Jessica Woodhams, Wangu Kanja and Heather D. Flowe in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.