
Abstract
Sexual and gender-based violence (SGBV) leads to severe sequelae for individuals and communities. Lack of cross-sector coordination inhibits effective medical–legal support and justice for survivors. Multisectoral trainings for health, legal, and law enforcement professionals on survivor-centered SGBV care were conducted in Kenya during 2012–2018. Evaluation utilized objective structured clinical examinations, standardized patients, knowledge assessments, and interviews. A total of 446 professionals participated in 18 trainings. Mean knowledge scores increased from 75.6% to 84.7% (p < .001). Thirty interviews revealed improved survivor confidentiality, increased specialized hospital care, more comprehensive forensic care, and greater cross-sector collaboration. Participants reported survivors feeling more comfortable pursuing legal action and increased perpetrator convictions.
Sexual and gender-based violence (SGBV) has been identified as a critical public health issue and a violation of human rights (World Health Organization, 2013). The World Health Organization reports up to 70% of women have suffered physical or sexual violence from an intimate partner in their lifetime (Garcia-Moreno et al., 2005). Sexual and other forms of gender-based violence increase in prevalence in times of conflict and are known risk factors for mental health conditions and reduced psychosocial well-being (Tol et al., 2013). Consequences of SGBV range from the physical and psychosocial to the spiritual and socioeconomic. They include unwanted pregnancy, fistulae, sexual dysfunction, sexually transmitted infections, posttraumatic stress disorder, anxiety, and depression (Ba & Bhopal, 2017). Social impacts commonly include rejection by family, community, and spouse as well as an increased risk of drug and alcohol abuse (Ba & Bhopal, 2017). SGBV has also been known to have negative costs to countries (Ellsberg & Heise, 2005; Fulu & Miedema, 2015) as the violence hinders peacebuilding efforts, postconflict rehabilitation, and generational reconstruction (Blay-Tofey & Lee, 2015). In fact, SGBV against women costs some governments up to 3.7% of their Gross Domestic Product—twice as much as most governments spend on education (Soliman & Kalle, 2020).
Women in sub-Saharan Africa face some of the highest rates of SGBV in the world, with prevalence rates up to 65% in some countries (Arnold et al., 2008; García-Moreno et al., 2013; Gebreyohannes, 2007; Iliyasu et al., 2011; Letta et al., 2014; Mullu et al., 2015; Umana et al., 2014; Wandera et al., 2017). Women in some African countries are also at the greatest risk of being killed by their intimate partners or family members (United Nations Office on Drugs and Crime, 2018). In Kenya, sexual violence was extensively used as a tool of intimidation during and after the 2017 General Election, according to a report by the Kenya National Commission on Human Rights (Kenya National Commission on Human Rights, 2018). A majority (54.5%) of these sexual assaults were perpetrated by security agencies. Another study approximated an increase of 22% in SGBV incidents without an identifiable aggressor, 20% in incidents involving multiple aggressors, and 18% in situations where survivors waited more than one month to consult a medical support agency, all in correlation with the postelection violence period following the highly contested presidential election of 2007 in Kenya (Anastario et al., 2014).
Healthcare, law enforcement, and legal professionals’ attitudes toward SGBV and survivors of SGBV factor immensely into ensuring adequate survivor care (Ferdowsian et al., 2016). Oftentimes, SGBV goes unreported due to stigma and inadequate medical and legal support (Ba & Bhopal, 2017; Smith et al., 2019; Verelst et al., 2014). The United Nations reports that more than 60% of female survivors do not seek assistance, with <10% of women who seek help appealing to the police (United Nations Economic and Social Affairs, 2015). Social norms often prevent survivors’ empowerment by placing the blame on survivors and furthering the perception of SGBV as customary (Glass et al., 2018; Read-Hamilton & Marsh, 2016). Law enforcement views generally follow along similar lines, dismissing SGBV as insignificant or driving the focus of policing efforts nearly exclusively on a stigmatized subset of offenders such as male youth gangs (Walby et al., 2014). In Kenya, a review of sexual assault survivors attending an assault recovery center found that 43% of assaults were reported to the police and only 44% of survivors received counseling (Ranney et al., 2010).
To effectively address SGBV in times of conflict, efforts must be made to strengthen forensic capacity and establish a multisectoral model for combatting sexual violence (Lokuge et al., 2016; Shako & Kalsi, 2019). We hypothesized that improved forensic training and establishing multisectoral networks of physicians, nurses, psychologists, police officers, prosecutors, and judges could significantly increase collaboration among professionals across sectors and improve care and justice processes for survivors of SGBV.
Methods
In collaboration with clinicians, police officers, lawyers, judges, and grassroots civil society organizations, Physicians for Human Rights (PHR) developed in-person trainings to strengthen the way duty-bearers respond to the needs and care of survivors of SGBV using trauma-informed, survivor-centered approaches and to enhance the way they collect, document, and preserve forensic evidence of sexual violence to support local prosecutions. Local partners, through a series of roundtable discussions, helped to identify the content priorities of these trainings. The trainings included multisectoral introductory forensic training, advanced crime scene investigation for law enforcement, advanced forensic documentation training for clinicians, institutional capacity training, advanced pediatric evaluation for clinicians, and training of trainers (Table 1). Training participants were medical, legal, and law enforcement professionals who regularly worked with SGBV survivors in and around the diverse communities of Eldoret, Kisumu, Nairobi, and the Rift Valley.
Description of Trainings Conducted by PHR's Program on Sexual Violence in Conflict Zones for Medical, Legal, and Law Enforcement Professionals.
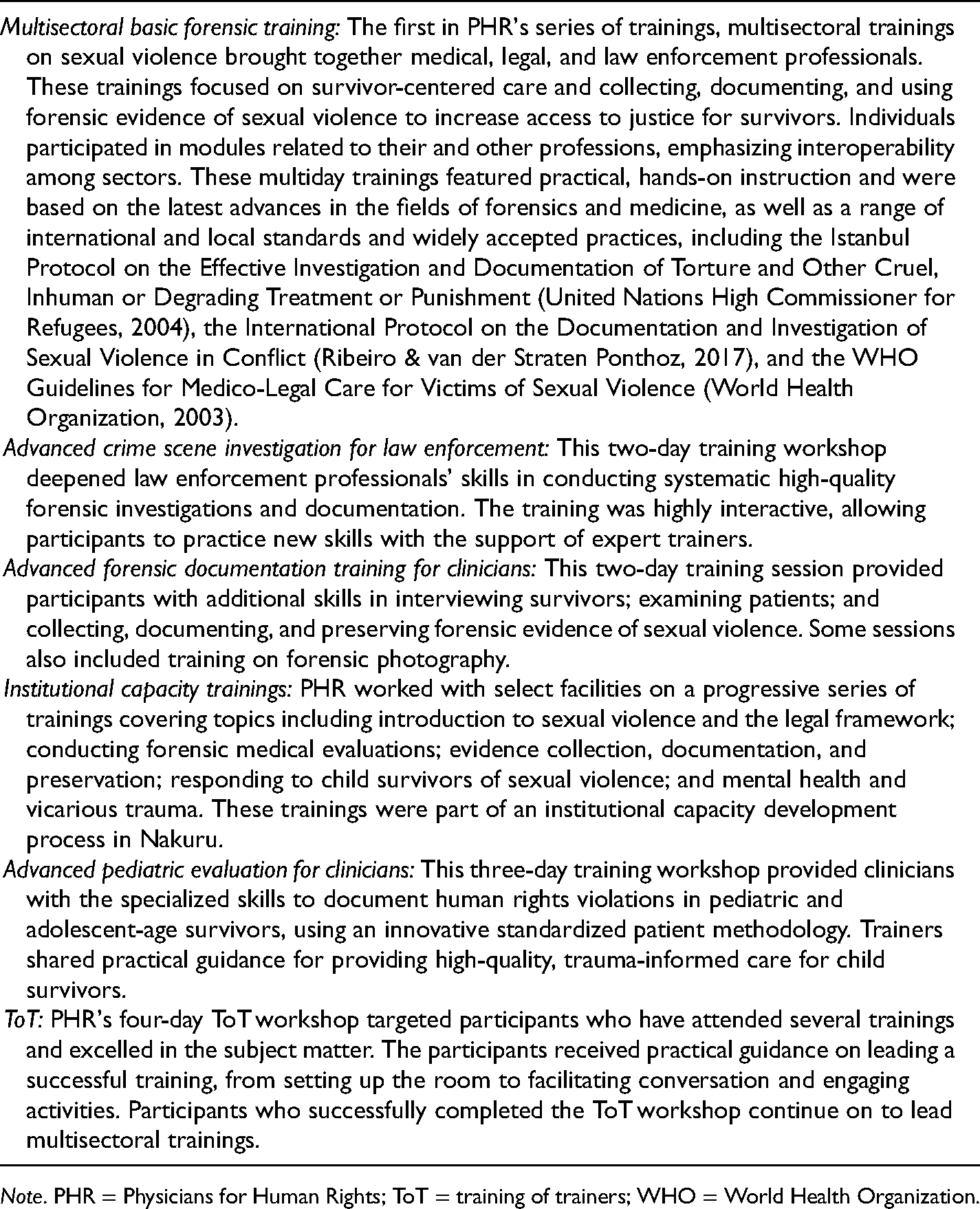
Note. PHR = Physicians for Human Rights; ToT = training of trainers; WHO = World Health Organization.
Trainings were typically two to four days in duration and utilized best practices in adult learning, such as clinical roleplays and objective structured clinical examinations (OSCE) using trained standardized patients (SPs). During the trainings, expert PHR medical trainers, forensic professionals, and the SPs completed structured checklists to evaluate trainees and provide feedback to improve the quality of clinical care and forensic documentation. Trainees also completed a closed-response knowledge and attitudes questionnaire before and after the trainings (Appendix A: Knowledge Assessment).
To extend multisectoral communication beyond the training periods, trainees were given a suite of PHR-developed learning materials, including a lexicon booklet that translates unfamiliar medical terms into language understandable by legal and law enforcement officials and a curriculum companion that trainees can use as a reference tool for best practices for interviewing survivors, examining patients, documenting findings, and packaging evidence. Trainees were also encouraged after their training to distribute the information to peers through formal training sessions as well as on-the-job mentoring. PHR collaborated with multisectoral training participants to establish networks of medical, legal, and law enforcement professionals in each county. At the close of each training, participants were invited to join a WhatsApp group to reinforce coordination and collaboration across medical, law enforcement, and legal sectors. With WhatsApp groups and regularly scheduled network meetings, each county's medical–legal network of professionals collaborated on specific cases and shared best practices.
Several months after training, trainees were contacted by phone by PHR and asked to participate in semistructured interviews. To understand the new program areas, purposive sampling was by training topic rather than chiefly by the professional sector. The interviews were conducted by two independent external evaluators, with each interview lasting approximately 30–60 min. Following full transcription, interviews were analyzed using a qualitative and inductive coding procedure inspired by a grounded theoretical approach (Charmaz, 2016; Service, 2008). To conduct this type of analysis, the study team first subjected all interview data to open coding (present progressive summations of text) within each programmatic area (k = 5). Second, the study team conducted axial coding within a single programmatic area that was used to structure the subsequent presentation of results for each programmatic area.
Trainee responses to the pre- and posttraining closed-response questionnaires were analyzed by using SPSS 25.0 (Armonk, NY) and a two-tailed paired samples t-test with an alpha value of .05. This study was reviewed and received ethical approval from the Georgetown University institutional review board (Protocols 2016-0661 and 2016-1404).
Results
Trainings
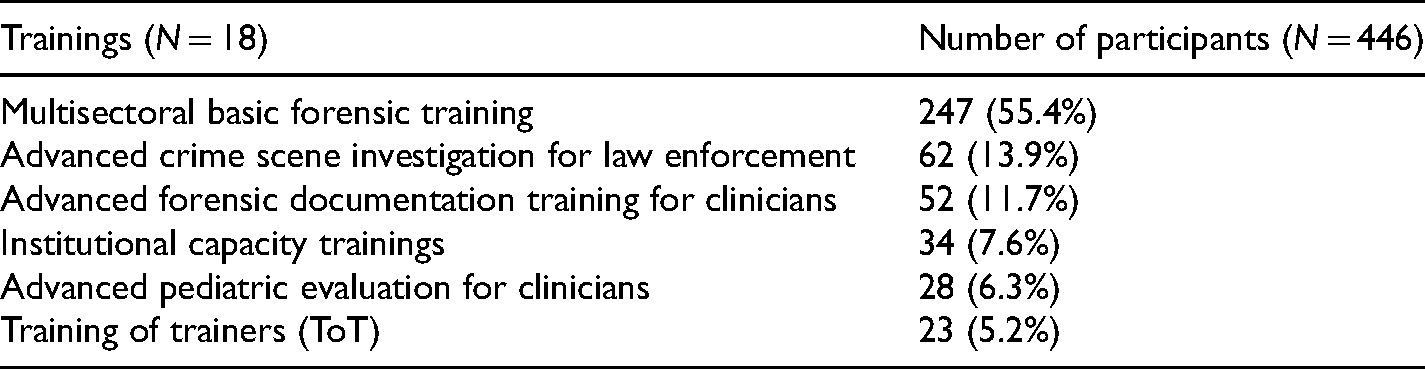
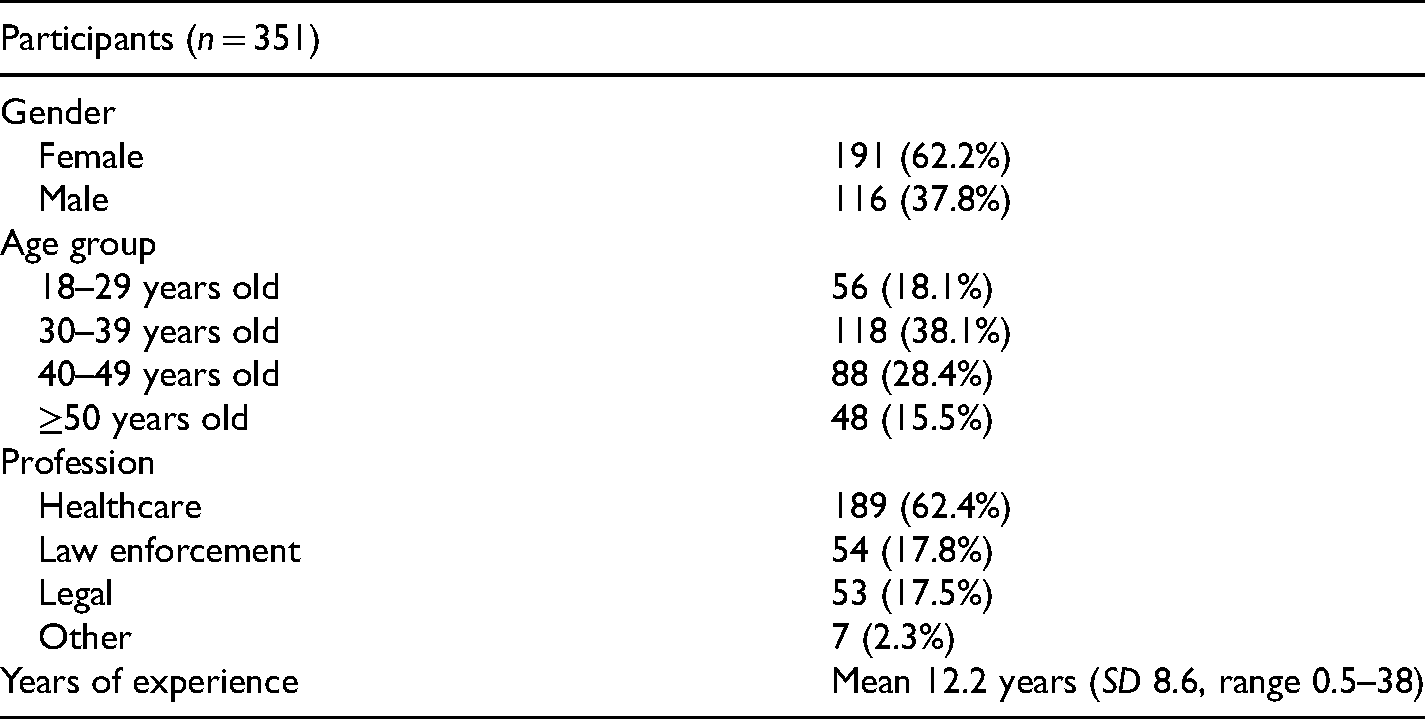
Eighteen training workshops were conducted from June 2012 to May 2018 involving 446 participants (Table 2). The mean number of participants per training was 24.8 (range 9–37). Age and sex-disaggregated data for 11 trainings incorporating pre- and posttraining knowledge assessment tests were collected. Training participants included health (51.1%), law enforcement (57.9%), legal (9.9%), and other (9.4%) professionals. Of trainees completing the pre- and posttest assessments, the majority (62.2%) were female, a plurality (38.1%) were 30–39 years old, a majority (62.4%) were healthcare professionals, and their mean years of professional experience was 12.2 (SD 8.6, range 0.5–38) (Table 3).
Training Workshops Conducted Between 2012 and 2018 in Various Locations in Kenya.
Characteristics of Training Participants Completing the Pre- and Posttraining Knowledge Assessments.
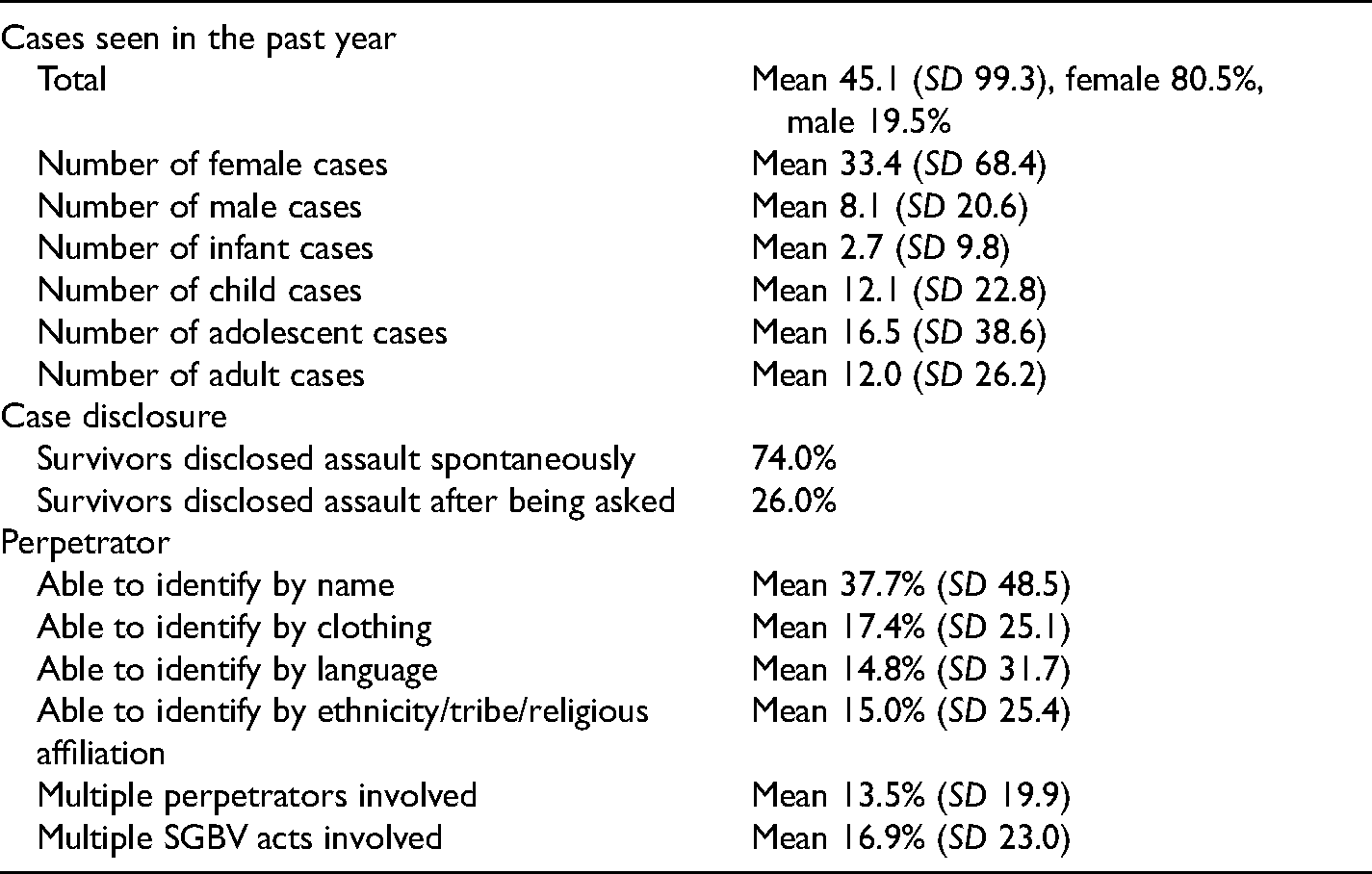
On average, training participants reported having been involved in 96.6 (SD 76.4) SGBV cases during their careers, with 66.5% (SD 65.2) of presenting survivors being female. Table 4 describes participant caseloads. When asked how likely is the destruction or loss of medical records or evidence related to a sexual violence case in their country, a plurality (41.9%) reported “somewhat likely,” while 16.2% reported “very unlikely,” 21.9% reported “somewhat unlikely,” and 20.0% reported “very likely.”
Sexual and Gender-based Violence (SGBV) Cases Seen by Training Participants in the Past Year, as Reported by Participants.
A comparison of pre- and posttraining knowledge assessments indicated an increase in participant knowledge with mean pre- and posttest knowledge assessment scores of 75.6% (SD 11.8) and 84.7% (SD 11.8), respectively. The result of a two-tailed paired t-test was significant (p < .001). When subcategorized by question topic, pre- and posttest scores increased in all question categories: SGBV terminology (means 87.8% and 96.9%, p < .001), survivor-centered care (means 82.6% and 89.8% p < .001), forensic evidence (means 65.6% and 72.2%, p = .004), evidence preservation (50.9% and 73.4%, p < .001), and professional attitudes (85.0% and 90.5%, p = .001).
Qualitative Results
In February 2018, 30 semistructured interviews were conducted among professionals who had completed one or more of the training workshops in the previous 12 months (Table 5). From these interviews, five common themes emerged. Illustrative quotations for each theme are presented in Table 6.
Distribution of Interviewees (n = 30) by Sector and Programmatic Area.
Themes and Illustrative Quotes.
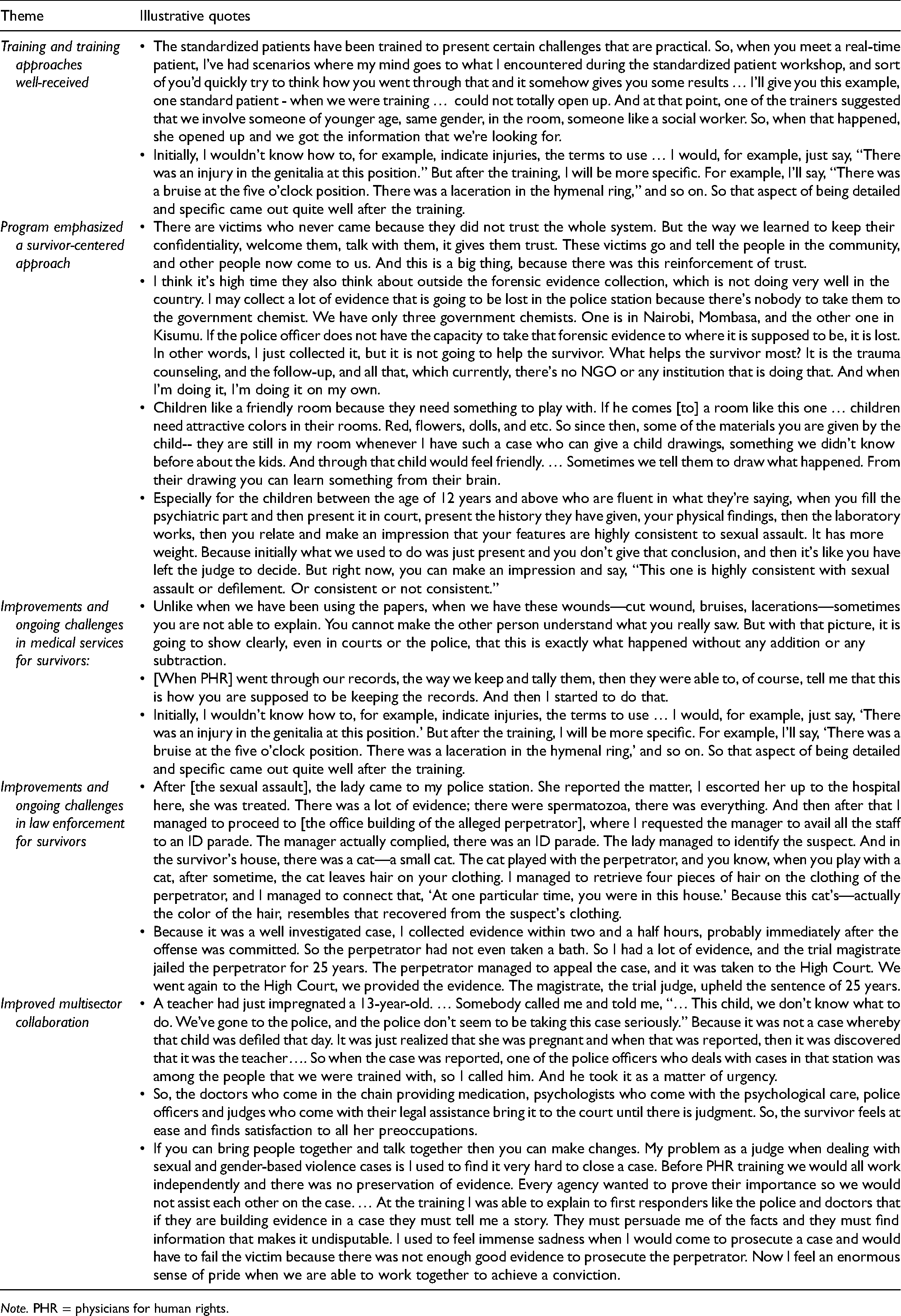
Note. PHR = physicians for human rights.
Training and Training Approaches Well Received
According to the participant interviews, the trainings facilitated improvements at two levels. First, the trainings improved the technical skills of individual participants. The training sessions featured the use of SPs as an andragogical method. Participants observed that the scenarios demonstrated by the SPs were fairly comprehensive, covered many of the situations encountered in practice, and were frequently recalled after the training when working with survivors. Second, the trainings improved the capacity for collaboration between individuals from the law enforcement, legal, medical, community health, civil society, and judicial sectors. Prior to the training, there was reportedly little trust or respect across these sectors of stakeholders, but this was directly addressed by the training. The training sessions used case studies to facilitate group discussions about current cross-sector challenges and propose solutions. The training sessions allowed the participants to forge new and trusting relationships that proved useful after the training.
The scope of this cross-sectoral impact, however, was limited by consistent turnover, especially among police officers and judges. After being trained, some professionals would be transferred to new posts in other counties while incoming professionals are unfamiliar with both the training's content and the larger concern with SGBV. Within sectors, knowledge dissemination occurred as some participants conducted their own trainings or mentoring sessions among their colleagues. Others described feeling they were unable to train their peers without additional time or resources to do so. These subsequent trainings were offered in a multitude of ways. For example, some respondents used time in regularly scheduled staff meetings to briefly share what they learned, while others would facilitate longer, more formalized sessions.
Trainees found the content to be important enough to be incorporated into conventional medical training to further expand forensic expertise in the region. They also recommended PHR work with the government to establish university-based laboratories to train clinical trainees such as medical students and obstetrics–gynecology residents.
Program Emphasized a Survivor-Centered Approach
The assumption that survivors are worthy of protection, rapid response, and access to justice was a central component of the training. Many respondents recognized that cases have been dismissed because of a lack of properly collected and stored forensic evidence. In these instances, the survivor did not receive any form of justice, which respondents said led to significant psychological harm for the survivor and perpetuated a culture of impunity for perpetrators.
Following the training, both medical and law enforcement professionals reported greater sensitivity to the stigma surrounding sexual assault and the potential for revictimization. This led them to establish private interview rooms with lockable doors—in both the medical facilities and police stations. This relatively minor action preserved the privacy and dignity of survivors while they underwent a forensic exam.
Legal sector trainees and other network members perceived that the training led to an increased conviction, and, in jurisdictions with more successful prosecutions, to more survivors reporting incidents to police.
To further improve survivor access to services, interview participants described a variety of activities their networks were pursuing. Some networks were highly focused on policy-change advocacy, including lobbying the government to reduce redundancies in sexual assault documentation, to implement various prison reforms, to use courthouse video links for child survivors of sexual violence, and to establish a centralized database to track case processing.
Consistent with a survivor-centered approach, one interviewee felt efforts should first improve survivors’ access to mental health services. In Kenya, mental health services are reportedly prohibitively expensive if survivors pay out of pocket, costing more than what many survivors earn in a month for one counseling session. Without affordable mental health services, healthcare providers—who were untrained in counseling—were attempting to provide this support but felt inadequate to meet the significant needs of survivors.
Following PHR's advanced pediatric evaluation training, perceived improvements in survivor-centeredness were also described for child survivors. A reportedly successful change was providers interacting more effectively with the child's caretaker or guardian. This was especially notable in situations where the caretaker was a potential perpetrator or when eliciting information on peer sexual contacts. Further, participants also noted that both their pediatric documentation and attentiveness to the psychological needs of child survivors improved as a result of the PHR training. Improvements were made to the physical spaces to make them more comfortable environments for children – providing toys, arts, and crafts to children during their visits. However, while interviewees felt progress had been made in improving the child-centeredness of health services, they regretted limited progress within the law enforcement and justice sectors.
Improvements and Ongoing Challenges in Medical Services for Survivors
Clinicians expressed greater confidence in conducting forensic examinations and documentation after training. Specifically, they shifted the focus of examinations away from relying solely on the characteristics of the hymen and toward greater documentation of the survivor's narrative statements and a fuller accounting of physical injuries on the body. Healthcare providers believed that, in response to these changes, the judiciary began receiving higher-quality evidence, survivor statements, physical examination documentation, and reliable laboratory tests as part of each case's evidence. Similarly, they believed that, as a result of these improvements, more perpetrators were held accountable in a court of law.
The interviews highlighted some operational challenges, including ongoing documentation issues. For example, some participants felt that completing both the Medical Examination Report and Post Rape Care form (both required by Kenyan law) was burdensome and that they did not have the expertise to properly complete the psychosocial section of the latter form. These issues often resulted in delays and in survivors sometimes waiting days to have both forms completed, becoming discouraged, and abandoning their pursuit of justice. Challenges with documentation also included limited space in the forms for diagramming survivor injuries. Participants described the ultimate goal of eliminating the requirement of the Medical Examination Form if the Post Rape Care Form is properly completed.
Medical professionals in Kenya reported system-wide structural deficiencies regarding the management of sexual violence cases. Respondents recommended PHR trainings be expanded to more medical and health facilities so survivors would be more likely to receive victim-centered care regardless of which facility or geographic region they present. Challenges to the potential impact of the trainings included frequent personnel transfers as well as a chronic shortage of equipment and supplies, including stockouts of basic antibiotics, laboratory reagents, and various testing kits.
Lastly, clinicians requested that greater attention be paid to vicarious trauma experienced by healthcare providers and recommended that additional support and time be allocated to personal recovery.
Improvements and Ongoing Challenges in Law Enforcement
Law enforcement respondents recognized that they enter the profession without forensic training and that, generally, the issue of sexual violence is deprioritized or not perceived as being effectively addressable. However, as a result of the PHR training, law enforcement participants described a stronger appreciation for appropriate forensic evidence collection, documentation, and processing.
Several training participants reported returning to their police precincts and training their colleagues following the workshops. This included accompanying colleagues into the field to collect evidence from crime scenes, modeling how to work with traumatized survivors, and reinforcing chain-of-custody procedures for secure evidence collection and transfer. Trainees perceived that sexual assault cases were being processed more successfully in the courts. In one example from the interviews, a police officer reported investigating 80 sexual violence cases using methods learned from his first PHR training five years earlier. Of those cases, 14 were pending, three were lost, and 63 resulted in imprisonment of perpetrators.
To further improve the reach and sustainability of the trainings within law enforcement, interviewees suggested PHR collaborate with the Kenyan Police College to introduce the content into the student curriculum.
Improved Multisector Collaboration
Participants believed that establishing professional networks of collaboration significantly increased cross-sectoral understanding, facilitated coordination, improved case processing, and strengthened the sectors’ ability to advocate to the government. One manner in which networking expedited cases was through newly established direct communication (e.g., phone calls and text messages) between law enforcement personnel conducting investigations and laboratory personnel analyzing the samples. Many networks established cross-sector WhatsApp groups to coordinate referrals and troubleshoot issues.
Integrating community-based organizations into the multisectoral networks further enhanced program impact, as these organizations were able to assist with public outreach and education campaigns, as well as to provide or facilitate psychosocial services for survivors. The networks also provided improved access to relatively high-level individuals across multiple sectors, including community leaders and judicial officers, who could help effect change. Relatedly, participants found having judicial sector participants present at the trainings was useful, as judges could provide feedback to physicians on best practices for evidence documentation.
Collaborations fostered in the trainings continued into the field in the form of improved coordination. For example, interviewees described PHR-trained law enforcement and legal professionals working side-by-side to conduct investigations of sexual assaults, including traveling together in the field to improve processes for medical evidence collection and transfer. Although some networks—including one of the Nairobi-based networks—were highly active with structured monthly meetings, lack of funding and a reliance on the voluntary efforts of network members were described as limiting potential collaboration.
Discussion
This initiative sought to improve services and outcomes for survivors of sexual violence in Kenya through training and network-building among healthcare, law enforcement, and legal professionals. The multisectoral trainings aimed at improving skills in forensic evidence collection, documentation, and preservation; pediatric forensic examination; mental health support for survivors; and training of peers.
The study's pre- and posttraining knowledge assessments showed a significant increase in knowledge among training participants across all sectors. Qualitative data from the interviews with participants were similarly encouraging and suggested the program made strong progress in establishing a multisectoral community and in deepening local forensic capacity to effectively document evidence of sexual violence using a survivor-centered approach. One of the more valued features of the program was its multisectoral focus which strengthened collaboration and communication across the medical, law enforcement, and legal communities. The networks facilitated improvement in the management and collection of forensic evidence for sexual assault survivors.
The results echo prior reporting about the benefits of this approach. The United Nations Population Fund concluded multisectoral approaches can help prevent revictimization, improve institutional and cultural perceptions of SGBV, and reinforce trust between the survivor and those providing services (Horga & Nicoara, 2015). A comparative study in Ethiopia and The Gambia concluded, despite its additional cost, that multisectoral efforts improved both forensic documentation and court processes for survivors of SGBV (Keesbury & Askew, 2010). Conversely, a study in Zambia found multidisciplinary coordination was not only more expensive and protracted but was, likewise, more challenging as a result of poor communication between nongovernmental and governmental institutions. A similar project in Uganda and Malawi by the same organization found multisectoral efforts unsustainable and requires constant reinforcement. Nevertheless, the authors also reported multisectoral models improved the quality of care as evidenced by an increase in referrals from police. In Kenya, a provincial hospital-based SGBV recovery center showed the effectiveness of closely integrating emergency care, mental health, paralegal, police, judiciary, and the community (Temmerman et al., 2019). Lastly, a study related to intimate-partner violence within one of Kenya's refugee camps identified the ineffectiveness of SGBV programming when it fails to engage community residents (Tappis et al., 2016).
Within the trainings themselves, the use of less didactic and more experiential teaching methods, such as SPs with OSCEs and case studies, were considered relatively innovative in this setting and effective in teaching participants critical interviewing and examination skills. In fact, several interviewees considered the SPs as the most valuable part of the training by solidifying learning objectives and aiding future recall. While commonly utilized in medical education in high-resource settings, the use of OSCEs and SPs is a relatively novel educational tool in sub-Saharan Africa (Daniels et al., 2017).
A significant focus in our initiative was also given to building local ownership and investment in training design and implementation to promote sustainability and ensure relevancy. The program used repeated engagement within and across sectors through training workshops, roundtable discussions, mentoring, and connections between local and international experts. Even greater sustainability and scale could be achieved by offering additional trainings coordinated by the government and by introducing training on SGBV into the preservice curricula of healthcare, law enforcement, and legal professionals.
Current efforts are focusing on addressing several of the barriers identified in the study. For example, improvements are being made in formalizing and providing additional supervisory support to trainees in subsequently training their peers. However, ongoing health system-level issues remain challenges to the program, including limited healthcare resources and mental health services for survivors.
There are limitations to this study. Although its participants were diverse in terms of age, experience, and professional sector and were from diverse communities in southern and western Kenya, the study findings may not be generalizable to communities beyond these regions or beyond Kenya. Nevertheless, the experiences reported by the participants appear consistent with those in the literature and in other countries in which PHR has been training. Secondly, as with any study involving self-report, there is the possibility of recall and social desirability biases. We attempted to mitigate social desirability bias by utilizing external evaluators and emphasizing the anonymous nature of the study and our desire to understand both the strengths and weaknesses of the program. Another limitation involves the fact that the evaluation was done at a point in time. At this moment there are no means of assessing the potential impact of the program (e.g., on practice and knowledge attainment) longitudinally, beyond the study period; it is possible that the positive effects will not be sustained in the long run. Lastly, despite the perceived positive outcomes reported by the participants, we did not assess the impact (actual or perceived) on survivors themselves, or on justice outcomes such as the number of successfully prosecuted SGBV cases involving the trained cohort compared to nontrained cohorts.
Conclusion
Scaling medical–legal training and strengthening multisectoral networks in areas with high rates of SGBV are promising strategies for increasing collaboration, enhancing the quality of services, and improving justice processes for survivors of SGBV.
Supplemental Material
sj-doc-1-vaw-10.1177_10778012221099984 - Supplemental material for Multiyear, Multisectoral Training Program in Kenya to Enhance Medical–Legal Processes in Response to Sexual and Gender-Based Violence
Supplemental material, sj-doc-1-vaw-10.1177_10778012221099984 for Multiyear, Multisectoral Training Program in Kenya to Enhance Medical–Legal Processes in Response to Sexual and Gender-Based Violence by Salma Albezreh, Mike Anastario, Billy J. Ulibarrí, Karen Naimer, Katy Johnson, Thomas McHale, Ranit Mishori, Wendy L. Macias-Konstantopoulos, Rose Olson and Brett D. Nelson in Violence Against Women
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The evaluation described was produced with funding from the UN Trust Fund to End Violence against Women; however, the views expressed, and content included does not imply official endorsement or acceptance by the United Nations.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.